Relationship between Fundamental Movement Skills and Physical Activity in Preschool-aged Children: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
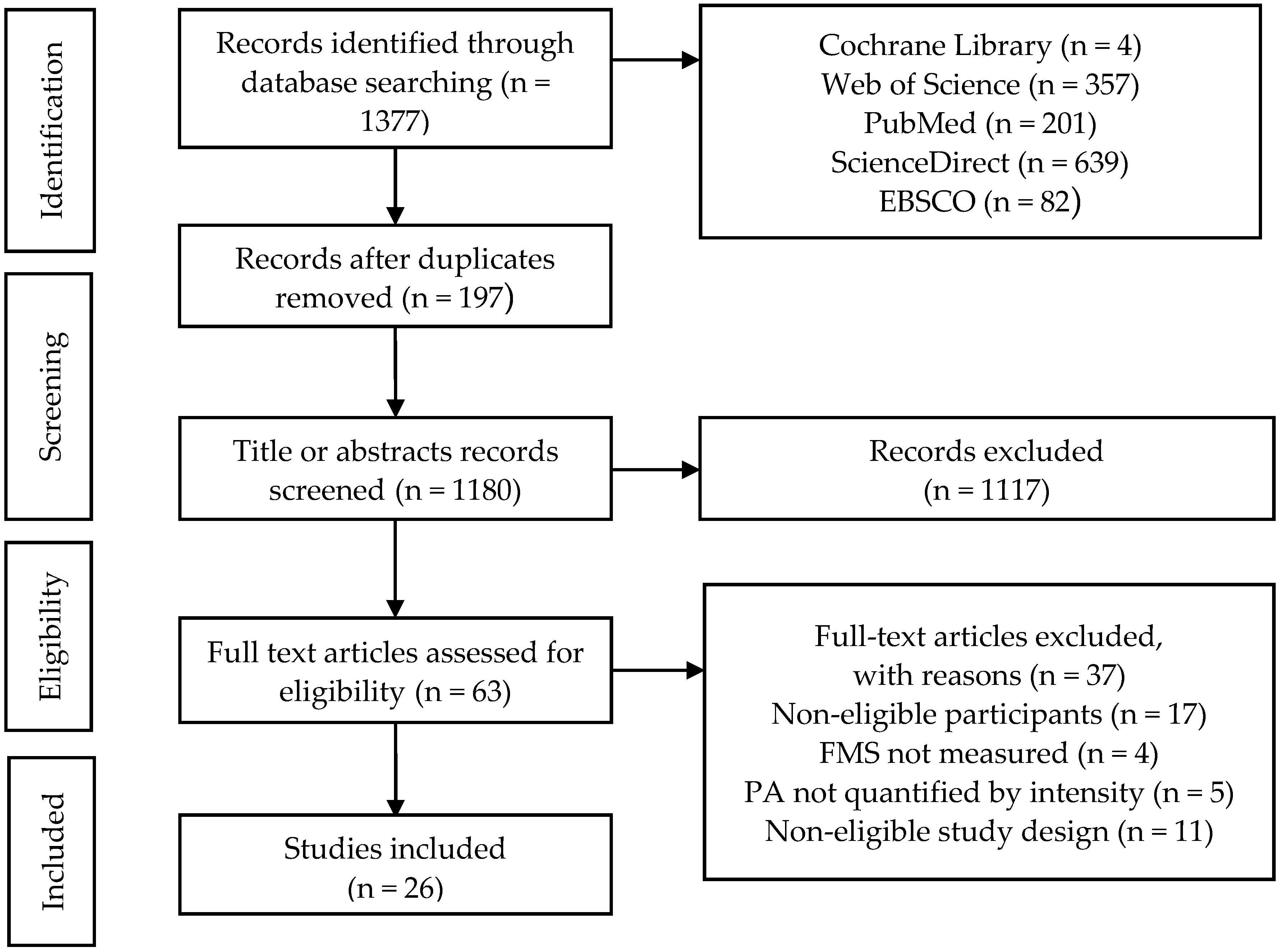
2.1. Search Strategy
2.2. Screen and Selection
2.3. Assessment of Methodological Quality
2.4. Data Extraction and Synthesis
3. Results
3.1. Study Identification and Characteristics
3.2. Methodological Quality of Studies
3.3. Assessment of FMS and PA
3.4. Relationship between FMS and PA
3.4.1. General Relationship between FMS and PA
3.4.2. Gender-Specific Aspects
3.4.3. Intensity-Specific PA and Total FMS
3.4.4. Intensity-Specific PA and Subdomain Skills
4. Discussion
5. Conclusions and Implication
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Vale, S.; Trost, S.G.; Rego, C.; Abreu, S.; Mota, J. Physical Activity, Obesity Status, and Blood Pressure in Preschool Children. J. Pediatr. 2015, 167, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Leppanen, M.H.; Henriksson, P.; Nystrom, C.D.; Henriksson, H.; Ortega, F.B.; Pomeroy, J.; Ruiz, J.R.; Cadenas-Sanchez, C.; Lof, M. Longitudinal Physical Activity, Body Composition, and Physical Fitness in Preschoolers. Med. Sci. Sports Exerc. 2017, 49, 2078–2085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leppanen, M.H.; Nystrom, C.D.; Henriksson, P.; Pomeroy, J.; Ruiz, J.R.; Ortega, F.B.; Cadenas-Sanchez, C.; Lof, M. Physical activity intensity, sedentary behavior, body composition and physical fitness in 4-year-old children: Results from the ministop trial. Int. J. Obes. 2016, 40, 1126–1133. [Google Scholar] [CrossRef] [PubMed]
- Carson, V.; Rahman, A.A.; Wiebe, S.A. Associations of subjectively and objectively measured sedentary behavior and physical activity with cognitive development in the early years. Ment. Health Phys. Act. 2017, 13, 1–8. [Google Scholar] [CrossRef]
- Webster, E.K.; Martin, C.K.; Staiano, A.E. Fundamental motor skills, screen-time, and physical activity in preschoolers. J. Sport Health Sci. 2019, 8, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Wadsworth, D.D.; Johnson, J.L.; Carroll, A.V.; Pangelinan, M.M.; Rudisill, M.E.; Sassi, J. Intervention Strategies to Elicit MVPA in Preschoolers during Outdoor Play. Int. J. Environ. Res. Public Health 2020, 17, 650. [Google Scholar] [CrossRef] [Green Version]
- Janssen, I.; LeBlanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. 2010, 7, 40. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children under 5 Years of Age. Available online: https://apps.who.int/iris/handle/10665/311664 (accessed on 7 May 2020).
- Strong, W.B.; Malina, R.M.; Blimkie, C.J.; Daniels, S.R.; Dishman, R.K.; Gutin, B.; Hergenroeder, A.C.; Must, A.; Nixon, P.A.; Pivarnik, J.M. Evidence based physical activity for school-age youth. J. Pediatr. 2005, 146, 732–737. [Google Scholar] [CrossRef]
- Pate, R.R.; O’Neill, J.R.; Brown, W.H.; Pfeiffer, K.A.; Addy, C.L. Prevalence of Compliance with a New Physical Activity Guideline for Preschool-Age Children. Child. Obes. 2015, 11, 415–420. [Google Scholar] [CrossRef]
- Andersen, E.; Borch-Jenssen, J.; Øvreås, S.; Ellingsen, H.; Jørgensen, K.A.; Moser, T. Objectively measured physical activity level and sedentary behavior in Norwegian children during a week in preschool. Prev. Med. Rep. 2017, 7, 130–135. [Google Scholar] [CrossRef]
- Barnett, L.M.; Stodden, D.; Cohen, K.E.; Smith, J.J.; Lubans, D.R.; Lenoir, M.; Iivonen, S.; Miller, A.D.; Laukkanen, A.; Dudley, D. Fundamental Movement Skills: An Important Focus. J. Teach. Phys. Educ. 2016, 35, 219–225. [Google Scholar] [CrossRef]
- Barnett, L.M.; Van Beurden, E.; Morgan, P.J.; Brooks, L.O.; Beard, J.R. Childhood motor skill proficiency as a predictor of adolescent physical activity. J. Adolesc. Health 2009, 44, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D.; Davis, R.E.; Fu, Y.-C. Early motor skill competence as a mediator of child and adult physical activity. Prev. Med. Rep. 2015, 2, 833–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lloyd, M.; Saunders, T.J.; Bremer, E.; Tremblay, M.S. Long-term importance of fundamental motor skills: A 20-year follow-up study. Adapt. Phys. Act. Q. 2014, 31, 67–78. [Google Scholar] [CrossRef] [PubMed]
- Stodden, D.F.; Goodway, J.D.; Langendorfer, S.J.; Roberton, M.A.; Rudisill, M.E.; Garcia, C.; Garcia, L.E. A developmental perspective on the role of motor skill competence in physical activity: An emergent relationship. Quest 2008, 60, 290–306. [Google Scholar] [CrossRef]
- Barnett, L.; Hinkley, T.; Okely, A.D.; Salmon, J. Child, family and environmental correlates of children’s motor skill proficiency. J. Sci. Med. Sport 2013, 16, 332–336. [Google Scholar] [CrossRef] [Green Version]
- Stodden, D.; Goodway, J.D. The dynamic association between motor skill development and physical activity. JOPERD 2007, 78, 33–49. [Google Scholar] [CrossRef]
- Van Capelle, A.; Broderick, C.R.; van Doorn, N.; E Ward, R.; Parmenter, B.J. Interventions to improve fundamental motor skills in pre-school aged children: A systematic review and meta-analysis. J. Sci. Med. Sport 2017, 20, 658–666. [Google Scholar] [CrossRef]
- Wick, K.; Leeger-Aschmann, C.S.; Monn, N.D.; Radtke, T.; Ott, L.V.; Rebholz, C.E.; Cruz, S.; Gerber, N.; Schmutz, E.A.; Puder, J.J.; et al. Interventions to Promote Fundamental Movement Skills in Childcare and Kindergarten: A Systematic Review and Meta-Analysis. Sports Med. 2017, 47, 2045–2068. [Google Scholar] [CrossRef] [Green Version]
- Foweather, L.; Knowles, Z.; Ridgers, N.D.; O’Dwyer, M.V.; Foulkes, J.D.; Stratton, G. Fundamental movement skills in relation to weekday and weekend physical activity in preschool children. J. Sci. Med. Sport 2015, 18, 691–696. [Google Scholar] [CrossRef]
- Iivonen, K.; Sääkslahti, A.; Mehtälä, A.; Villberg, J.; Tammelin, T.; Kulmala, J.; Poskiparta, M. Relationship between fundamental motor skills and physical activity in 4-year-old preschool children. Percept. Motor Ski. 2013, 117, 627–646. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.E.; Metcalfe, J.S. The mountain of motor development: A metaphor. Mot. Dev. Res. Rev. 2002, 2, 163–190. [Google Scholar]
- Fisher, A.; Reilly, J.J.; Kelly, L.A.; Montgomery, C.; Williamson, A.; Paton, J.Y.; Grant, S. Fundamental movement skills and habitual physical activity in young children. Med. Sci. Sports Exerc. 2005, 37, 684–688. [Google Scholar] [CrossRef] [PubMed]
- Hall, C.; Eyre, E.; Oxford, S.; Duncan, M. Relationships between Motor Competence, Physical Activity, and Obesity in British Preschool Aged Children. J. Funct. Morphol. Kinesiol. 2018, 3, 57. [Google Scholar] [CrossRef] [Green Version]
- Kambas, A.; Michalopoulou, M.; Fatouros, I.G.; Christoforidis, C.; Manthou, E.; Giannakidou, D.; Venetsanou, F.; Haberer, E.; Chatzinikolaou, A.; Gourgoulis, V.; et al. The Relationship Between Motor Proficiency and Pedometer-Determined Physical Activity in Young Children. Pediatr. Exerc. Sci. 2012, 24, 34–44. [Google Scholar] [CrossRef]
- Temple, V.A.; Crane, J.R.; Brown, A.; Williams, B.L.; Bell, R.I. Recreational activities and motor skills of children in kindergarten. Phys. Educ. Sport Peda. 2016, 21, 268–280. [Google Scholar] [CrossRef]
- Williams, H.G.; Pfeiffer, K.A.; O’Neill, J.R.; Dowda, M.; McIver, K.L.; Brown, W.H.; Pate, R.R. Motor Skill Performance and Physical Activity in Preschool Children. Obesity 2008, 16, 1421–1426. [Google Scholar] [CrossRef]
- Lee, J.; Zhang, T.; Chu, T.L.; Gu, X. Effects of a Need-Supportive Motor Skill Intervention on Children’s Motor Skill Competence and Physical Activity. Children 2020, 7, 21. [Google Scholar] [CrossRef] [Green Version]
- Crane, J.R.; Naylor, P.J.; Cook, R.; Temple, V.A. Do Perceptions of Competence Mediate the Relationship Between Fundamental Motor Skill Proficiency and Physical Activity Levels of Children in Kindergarten? J. Phys. Act. Health 2015, 2, 954–961. [Google Scholar] [CrossRef]
- Nilsen, A.K.O.; Anderssen, S.A.; Loftesnes, J.M.; Johannessen, K.; Ylvisaaker, E.; Aadland, E. The multivariate physical activity signature associated with fundamental motor skills in preschoolers. J. Sports Sci. 2020, 38, 264–272. [Google Scholar] [CrossRef]
- Nilsen, A.K.O.; Anderssen, S.A.; Johannessen, K.; Aadland, K.N.; Ylvisaaker, E.; Loftesnes, J.M.; Aadland, E. Bi-directional prospective associations between objectively measured physical activity and fundamental motor skills in children: A two-year follow-up. Int. J. Behav. Nutr. Phys. 2020, 17, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.L. Fundamental motor skill, physical activity, and sedentary behavior in socioeconomically disadvantaged kindergarteners. Psychol. Health Med. 2016, 21, 871–881. [Google Scholar] [CrossRef] [PubMed]
- Cliff, D.P.; Okely, A.D.; Smith, L.M.; McKeen, K. Relationships between fundamental movement skills and objectively measured physical activity in preschool children. Pediatr. Exerc. Sci. 2009, 21, 436–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Logan, S.W.; Kipling Webster, E.; Getchell, N.; Pfeiffer, K.A.; Robinson, L.E. Relationship between fundamental motor skill competence and physical activity during childhood and adolescence: A systematic review. Kinesiol. Rev. 2015, 4, 416–426. [Google Scholar] [CrossRef]
- Figueroa, R.; An, R. Motor Skill Competence and Physical Activity in Preschoolers: A Review. Matern. Child Health J. 2017, 21, 1–11. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.G.; Stewart, L. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Rostom, A.; Dubé, C.; Cranney, A. Celiac Disease. Rockville (MD): Agency for Healthcare Research and Quality (US). September 2004; (Evidence Reports/Technology Assessments, No. 104.) Appendix, D. Quality Assessment Forms. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK35156/ (accessed on 7 May 2020).
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Non-Randomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 7 May 2020).
- Ioannidis, J.; Patsopoulos, N.; Rothstein, H. Reasons or excuses for avoiding meta-analysis in forest plots. BMJ 2008, 336, 1413–1415. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Sallis, J.F.; Prochaska, J.J.; Taylor, W.C. A review of correlates of physical activity of children and adolescents. Med. Sci. Sports Exerc. 2000, 32, 963–975. [Google Scholar] [CrossRef]
- Barnett, L.M.; Salmon, J.; Hesketh, K.D. More active pre-school children have better motor competence at school starting age: An observational cohort study. BMC Public Health 2016, 16, 1068. [Google Scholar] [CrossRef] [Green Version]
- Cook, C.J.; Howard, S.J.; Scerif, G.; Twine, R.; Kahn, K.; Norris, S.A.; Draper, C.E. Associations of physical activity and gross motor skills with executive function in preschool children from low-income South African settings. Dev. Sci. 2019, 22, e12820. [Google Scholar] [CrossRef]
- Gu, X.; Keller, M.J.; Weiller-Abels, K.H.; Zhang, T. The roles of physical activity and sedentary behavior on Hispanic children’s mental health: A motor skill perspective. Qual. Life Res. 2017, 27, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.X.; Schenkelberg, M.A.; O’Neill, J.R.; Dowda, M.; Pate, R.R. How Does the Relationship Between Motor Skill Performance and Body Mass Index Impact Physical Activity in Preschool Children? Pediatr. Exerc. Sci. 2018, 30, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Hall, C.J.S.; Eyre, E.L.J.; Oxford, S.W.; Duncan, M.J. Does Perception of Motor Competence Mediate Associations between Motor Competence and Physical Activity in Early Years Children? Sports 2019, 7, 77. [Google Scholar] [CrossRef] [PubMed]
- Iivonen, S.; Saakslahti, A.K.; Mehtala, A.; Villberg, J.J.; Soini, A.; Poskiparta, M. Directly observed physical activity and fundamental motor skills in four-year-old children in day care. Eur. Early Child. Educ. 2016, 24, 398–413. [Google Scholar] [CrossRef] [Green Version]
- Laukkanen, A.; Pesola, A.; Havu, M.; Sääkslahti, A.; Finni, T. Relationship between habitual physical activity and gross motor skills is multifaceted in 5-to 8-year-old children. Scand. J. Med. Sports 2014, 24, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Matarma, T.; Lagstrom, H.; Hurme, S.; Tammelin, T.H.; Kulmala, J.; Barnett, L.M.; Koski, P. Motor skills in association with physical activity, sedentary time, body fat, and day care attendance in 5–6-year-old children-The STEPS Study. Scand. J. Med. Sci. Sports 2018, 28, 2668–2676. [Google Scholar] [CrossRef]
- Robinson, L.E.; Wadsworth, D.D.; Peoples, C.M. Correlates of School-Day Physical Activity in Preschool Students. Res. Q. Exerc. Sport 2012, 83, 20–26. [Google Scholar] [CrossRef]
- Roscoe, C.M.P.; James, R.S.; Duncan, M.J. Accelerometer-based physical activity levels, fundamental movement skills and weight status in British preschool children from a deprived area. Eur. J. Pediatr. 2019, 178, 1043–1052. [Google Scholar] [CrossRef] [Green Version]
- Schmutz, E.A.; Leeger-Aschmann, C.S.; Kakebeeke, T.H.; Zysset, A.E.; Messerli-Bürgy, N.; Stülb, K.; Arhab, A.; Meyer, A.H.; Munsch, S.; Puder, J.J.; et al. Motor Competence and Physical Activity in Early Childhood: Stability and Relationship. Front. Public Health 2020, 8, 39. [Google Scholar] [CrossRef]
- Tsuda, E.; Goodway, J.D.; Famelia, R.; Brian, A. Relationship Between Fundamental Motor Skill Competence, Perceived Physical Competence and Free-Play Physical Activity in Children. Front. Psychol. 2020, 91, 55–63. [Google Scholar] [CrossRef]
- Welk, G.J. The youth physical activity promotion model: A conceptual bridge between theory and practice. Quest 1999, 51, 5–23. [Google Scholar] [CrossRef]
- Niemistö, D.; Finni, T.; Cantell, M.; Korhonen, E.; Sääkslahti, A. Individual, Family, and Environmental Correlates of Motor Competence in Young Children: Regression Model Analysis of Data Obtained from Two Motor Tests. Int. J. Environ. Res. Public Health 2020, 17, 2548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett, L.M.; Morgan, P.J.; Van, B.E.; Beard, J.R. Perceived sports competence mediates the relationship between childhood motor skill proficiency and adolescent physical activity and fitness: A longitudinal assessment. Int. J. Behav. Nutr. Phys. 2008, 5, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, T.; Lee, J.; Chu, T.L.A.; Chen, C.; Gu, X. Accessing Physical Activity and Health Disparities among Underserved Hispanic Children: The Role of Actual and Perceived Motor Competence. Int. J. Environ. Res. Public Health 2020, 17, 3013. [Google Scholar] [CrossRef] [PubMed]
- Harter, S. The Construction of the Self: Developmental and Sociocultural Foundations; Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- Tucker, P. The physical activity levels of preschool-aged children: A systematic review. Early Child Res. Q. 2008, 23, 547–558. [Google Scholar] [CrossRef]
- Niemistö, D.; Finni, T.; Haapala, E.A.; Cantell, M.; Korhonen, E.; Sääkslahti, A. Environmental Correlates of Motor Competence in Children—The Skilled Kids Study. Int. J. Environ. Res. Public Health 2019, 16, 1989. [Google Scholar] [CrossRef] [Green Version]
- Okely, A.D.; Wright, J. The Gender Bias in Fundamental Motor Skills Tests—A New Agenda Needed! In Proceedings of the Australian Association for Research in Education, Brisbane, Australia, 30 November–4 December 1997. [Google Scholar]
- Van Rheenen, D. A century of historical change in the game preferences of American children. J. Am. Folk. 2012, 125, 411–443. [Google Scholar] [CrossRef]
- Britton, U.; Issartel, J.; Symonds, J.; Belton, S. What Keeps Them Physically Active? Predicting Physical Activity, Motor Competence, Health-Related Fitness, and Perceived Competence in Irish Adolescents after the Transition from Primary to Second-Level School. Int. J. Environ. Res. Public Health 2020, 17, 2874. [Google Scholar] [CrossRef]
- Bornstein, D.B.; Beets, M.W.; Byun, W.; Welk, G.; Bottai, M.; Dowda, M.; Pate, R. Equating accelerometer estimates of moderate-to-vigorous physical activity: In search of the Rosetta Stone. J. Sci. Med. Sport 2011, 14, 404–410. [Google Scholar] [CrossRef] [Green Version]
- Logan, S.W.; Barnett, L.M.; Goodway, J.D.; Stodden, D.F. Comparison of performance on process-and product-oriented assessments of fundamental motor skills across childhood. J. Sport. Sci. 2017, 35, 634–641. [Google Scholar] [CrossRef]
- Ulrich, D. TGMD 2–Test of Gross Motor Development Examiner’s Manual; PRO-ED: Austin, TX, USA, 2000. [Google Scholar]
- Ulrich, D.A. The test of gross motor development−3 (TGMD−3): Administration, scoring, and international norms. Spor Bilimleri Derg. 2013, 24, 27–33. [Google Scholar]
- Herrmann, C.; Gerlach, E.; Seelig, H. Development and Validation of a Test Instrument for the Assessment of Basic Motor Competencies in Primary School. Meas. Phys. Educ. Exerc. Sci. 2015, 19, 80–90. [Google Scholar] [CrossRef]
- Sun, S.H.; Zhu, Y.C.; Shih, C.L.; Lin, C.H.; Wu, S.K. Development and initial validation of the Preschooler Gross Motor Quality Scale. Res. Dev. Disabil. 2010, 31, 1187–1196. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| First Author Year Country | Participant Details | Assessment | Study Findings | |
|---|---|---|---|---|
| PA | FMS | |||
| Barnett 2013 Australia [17] C | 76 (42 girls) 4.1 ± 0.68 y | Accelerometer (15 s) At least 4 days (3 weekdays and 1 weekend day) | TGMD−2 +- | Regressions: moderate–vigorous physical activity (MVPA) was a sig. predictor of object control skills (OCS), β = 0.37 *, but was not a sig. predictor of locomotor skills (LMS). |
| Barnett 2016 Australia [43] C,L | 127 (68 girls) 5.0 ± 0.1 y 118 (65 girls) 3.5 ± 0.2 y | Accelerometer (15 s) At least 4 days (3 weekdays and 1 weekend) | TGMD−2 + | Regressions: MVPA at 3.5 years was a predictor of LMS at age 5 years, β = 0.073*. MVPA at 5 years was not associated with LMS. MVPA was not associated with OCS fundamental movement skills (FMS) at any age. |
| Cliff 2009 Australia [34] C | 46 (21 girls) 4.3 ± 0.7 y | Accelerometer (60 s) At least 3 days | TGMD−2 + | Correlations for boys: MVPA and total FMS r = 0.48 *, & OCS r = 0.48 *, & LMS, not sig.; for girls: MVPA & GMQ r = −0.46 *, & LMS r = −0.50 *, & OCS not sig. Regressions for boys: OCS explained 16.9% and 13.7% of var. in MVPA and total physical activity (TPA), respectively; for girls: LMS explained 19.2% of var. in MVPA. |
| Cook 2019 South Africa [44] C | 129 (68 girls) 4.2 y | Accelerometer (15 s) At least 3 days | TGMD−2 + | Correlations: LMS & MVPA r = 0.18, & TPA r = 0.14; OCS & MVPA r = 0.25, & TPA r = 0.20; FMS & MVPA r = 0.24, & TPA r = 0.15. |
| Crane 2015 Canada [30] C | 116 (49 girls) 5.6 y | Accelerometer (15 s) At least 4 days (3 weekdays and 1 weekend day) | TGMD−2 + | Regressions: OCS were sig. predictors of MVPA, β = 0.281 **, LMS were not a sig. predictor of MVPA. MVPA explained 10.4% of var. in OCS, but MVPA was not a sig. predictor of LMS. |
| Fisher 2005 UK [24] C | 394 (185 girls) 4.2 ± 0.5 y | Accelerometer (60 s) 6 days | MABC - | Correlations: total FMS & TPA r = 0.10 * & MVPA r = 0.18 **; & LPA not sig. |
| Foweather 2015 UK [21] C | 99 (47 girls) 4.6 ± 0.5 y | Accelerometer (5 s) 7 days | TGMD−2 + | Correlations: FMS & MVPA r = 0.114 **, & TPA r = 0.102 **. |
| Gu 2016 USA [33] C | 256 (127 girls) 5.37 ± 0.48 y | Accelerometer (60 s) 5 school days | PE Metrics + | Correlations: LMS & LPA r = −0.18 **, MVPA r = 0.21 **; OCS & LPA r = −0.18 **, MVPA r = 0.21 **; total FMS & LPA r = −0.23 **, MVPA r = 0.26 **. Regressions: LMS was a sig. predictor of LPA, β = −0.19, and MVPA, β = 0.20; OCS was not a sig. predictor of MVPA. |
| Gu 2017 USA [45] C | 141 (69 girls) 5.37 ± 0.48 y | Accelerometer (60 s) 5 school days | PE Metrics + | Correlations: LMS & MVPA r = 0.24 **; OCS & MVPA r = 0.24 **; FMS & MVPA r = 0.28**. |
| Guo 2018 China [46] C | 227 (116 girls) 4.15 ± 0.63 y | Accelerometer (15 s) At least 3 days | CMSP + | Correlations: TPA & LMS r = 0.14 *, & OCS r = 0.16 *; & total FMS r = 0.17 *. Regressions: LMS was a sig. predictor of TPA β = 0.04 *, while OCS and total FMS were not sig. predictors of TPA. |
| Hall 2018 UK [25] C | 166 (75 girls) 4.28 ± 0.74 y (3–5 y) | Accelerometer (1 s) 4 days (2 weekdays and 2 weekend days) | TGMD−2 + | Correlations: total FMS & MVPA r = 0.376 **, & TPA r = 0.402 **; OCS & MVPA r = 0.367 **, & TPA r = 0.386 **; LMS & MVPA, & TPA not sig. |
| Hall 2019 UK [47] C | 38 (14 girls) 5.37 ± 0.79 y (4–6 y) | Accelerometer (60 s) 4 days (2 weekdays & 2 weekend days) | TGMD−2 + | Regressions: FMS (total FMS, LMS, OCS) were not sig. predictors of physical activity (PA) (MVPA, TPA) and vice versa. |
| Iivonen 2013 Finland [22] C | 37 (20 girls) 4.1 ± 0.34 y | Accelerometer (5 s) 5 days (at least 2 weekdays and 1 weekend day) | APM - | Regressions: total FMS was a predictor of MVPA, β = 0.49 **, and TPA, β = 0.49 **; OCS was a sig. predictor of MVPA, β = 0.49 **, and TPA, β = 0.47 **; LMS was a sig. predictor of MVPA, β = 0.35 **, but not a sig. predictor of TPA; stability skills were not sig. predictors of MVPA and TPA. |
| Iivonen 2016 Finland [48] C | 53 (29 girls) 4.07 ± 0.32 y | OSRAC–P | APM - | Regressions: LPA and MVPA were not sig. predictors of total FMS. |
| Kambas 2012 Greece [26] C | 232 (114 girls) 5.37 ± 0.28 y | Pedometer 7 days | BOTMP - | Correlations: TPA & LMS r = 0.31–0.39 *, & OCS r = 0.30–0.35 *, & SS r = 0.401 *, & FMS r = 0.368 |
| Laukkanen 2014 Finland [49] C | 53 (28 girls) 5.94 y | Accelerometer (15 s) 6 days (at least 2 weekdays and 1 weekend day) | KTK & APM manipulative skill test - | Correlations for boys: total FMS & TPA r = 0.448 *;for Girls: total FMS & TPA r = 0.138. |
| Matarma 2018 Finland [50] C | 111 (66 girls) 5.57 ± 0.4 y | Accelerometer (15 s) 7 days (at least 3 weekdays and 1 weekend day) | BOT−2 - | Regressions: total FMS was not a sig. predictor of MVPA. |
| Nilsen 2020 Norway [31] C | 1081 (526 girls) 4.7 ± 0.9 y | Accelerometer (1 s) At least 4 days (3 weekdays and 1 weekend day) | TGMD−3 + PGMQ + | Correlations: LPA & LMS, & OCS, & SS, not sig; MVPA & LMS, r = 0.26, & OCS r = 0.16, & SS not sig.; TPA & LMS, r = 0.23, & OCS r = 0.16, & SS not sig. |
| Nilsen 2020 Norway [32] L | 230 (110 girls) 4.7 ± 0.9 y | Accelerometer (1 s) At least 4 days | TGMD−3 + PGMQ (SS) + | Regressions: MVPA at baseline was sig. predictor of LMS, β = 0.26 **, OCS, β = 0.18, and SS, β = 0.19 at follow up; TPA at baseline was a sig. predictor of LMS, β = 0.23 **, OCS, β = 0.22, and SS, β = 0.17 at follow up; LPA was not a sig. predictor of FMS. FMS at baseline was not a sig. predictor of PA at follow up. |
| Robinson 2012 USA [51] C | 34 (22 girls) 4.75 ± 0.53 y | Pedometer 3 school days | TGMD−2 + | Correlations: LMS & TPA r = 0.461 *, OCS & TPA r = 0.435 *. Regressions: LMS explained 21.3% of the var. in TPA;OCS was not a sig. predictor of TPA. |
| Roscoe 2019 UK [52] C | 185 (86 girls) 3.4 ± 0.5 y | Accelerometer (10 s) 4 days (2 weekdays and 2 weekend days) | Adapted TGMD−2 + | Correlations: No sig. corr. between FMS (total FMS, LMS, OCS) and MVPA. |
| Schmutz 2020 Switzerland [53] C | 550 (292 girls) 3.9 ± 0.7 y | Accelerometer (15 s) At least 3 days (including 1 weekend day) | ZNA | Correlations: FMS & MVPA r = 0.23, & TPA r = 0.24 |
| Temple 2016 Canada [27] C | 74 (33 girls) 5.92 ± 0.33 y | CAPE | Stork stand - TGMD−2 + | Correlations: TPA & LMS r = 0.24 *, & OCS, & SS not sig.; for boys: TPA & LMS r = 0.41 **, & OCS r = 0.40 *, & SS r = 0.33 *; for girls: TPA & LMS, & OCS, & SS not sig. |
| Tsuda 2019 USA [54] C | 72 (33 girls) 4.38 ± 0.85 y | Accelerometer (15 s) 3 school days | TGMD−2 + | Correlations: LMS & MVPA r = 0.53 **; OCS & MVPA r = 0.46 **. Regressions: LMS and OCS explained 19% of var. in MVPA. |
| Webster 2018 USA [5] C | 126(68 girls) 3.4 ± 0.5 y | Accelerometer (15 s) 7 days (at least 3 days) | TGMD−3 + | Regressions: FMS (total FMS, LMS, OCS) were not sig. predictors of PA (MVPA, TPA). |
| Williams 2008 USA [28] C | 198 (98 girls) 4.2 ± 0.5 y | Accelerometer (15 s) 8–10 days | CMSP + | Correlations: FMS & LPA not sig, & MVPA r = 0.20 **; LMS & LPA not sig, & MVPA r = 0.16 *; OCS & LPA not sig, & MVPA r = 0.19 *. |
| Study | Criteria | Total Score | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I | II | III | IV | V | VI | VII | VIII | IX | X | XI | ||
| Barnett 2013 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 9 |
| Cliff 2009 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 9 |
| Cook 2019 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 9 |
| Crane 2015 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 8 |
| Fisher 2005 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 9 |
| Foweather 2015 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 9 |
| Gu 2016 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 10 |
| Gu 2018 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 7 |
| Guo 2018 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 7 |
| Hall 2018 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 9 |
| Hall 2019 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 9 |
| Iivonen 2013 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 8 |
| Iivonen 2016 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 5 |
| Kambas 2012 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 7 |
| Laukkanen 2014 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 7 |
| Matarma 2018 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 8 |
| Nilsen 2020 b | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 7 |
| Robinson 2012 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 5 |
| Roscoe 2019 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 6 |
| Schmutz 2020 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 |
| Temple 2016 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 6 |
| Tsuda 2019 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 6 |
| Webster 2018 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 8 |
| Williams 2008 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 10 |
| Study | Criteria | Total Score | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1a | 1b | 1c | 1d | 2a | 2b | 3a | 3b | 3c | ||
| Barnett 2016 | * | * | * | * | * | * | * | * | 8 | |
| Nilsen 2016 | * | * | * | * | * | * | * | * | * | 9 |
| Not Sig | Low Level | Moderate Level | Strong Level | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Boys | Girls | Total | Boys | Girls | Total | Boys | Girls | Total | Boys | Girls | Total | |
| FMS-LPA | [21,24,28,48] | [33] − | ||||||||||
| LMS-LPA | [21,28,31,32] | [33] − | ||||||||||
| OCS-LPA | [28,31,32] | [33] − | ||||||||||
| SS-LPA | [31,32] | |||||||||||
| FMS-MVPA | [5,43,47,48,52] | [21,24,28,33,44,45,53] | [34] | [34]- | [22,25,54] | |||||||
| LMS-MVPA | [34] | [34] | [5,17,25,30,43,47,52] | [28,31,32,33,44,45] | [22,34] | [54] | ||||||
| OCS-MVPA | [34] | [5,33,43,47,52] | [28,30,31,32,33,44,45] | [34] | [17,22,25,30,34,54] | |||||||
| SS-MVPA | [22,31] | [32] | ||||||||||
| FMS-TPA | [5,46,47,50] | [49] | [21,24,44,46,53] | [49] | [22,25,26] | |||||||
| LMS-TPA | [27] | [5,22,25,47] | [27,31,44,46] | [27] | [26,51] | |||||||
| OCS-TPA | [27] | [5,27,46,47,51] | [31,44,46] | [27] | [22,25,26,34,51] | |||||||
| SS-TPA | [27] | [22,27,31] | [27] | [26] | ||||||||
| Bivariate | Not Sig. | Sig. (n) | Summary Coding | |
|---|---|---|---|---|
| n/N (%) | Association (+, −, 0, ?) | |||
| FMS-LPA | [21,24,28,48] | [33] − | 1/5 (20%) | + |
| LMS-LPA | [21,28,31,32] | [33] − | 1/5 (20%) | + |
| OCS-LPA | [28,31,32] | [33] − | 1/4 (25%) | ? |
| SS-LPA | [31,32] | / | 0 | ? |
| FMS-MVPA | [5,43,47,48,52] | [21,22,24,25,28,33,34,44,45,53,54] | 11/16 (69%) | + |
| LMS-MVPA | [5,17,25,30,43,47,52] | [22,28,31,32,33,34,44,45,54] | 9/16 (56%) | ? |
| OCS-MVPA | [5,34,43,47,52] | [17,22,25,28,30,31,32,33,34,44,45,54] | 12/17 (71%) | + |
| SS-MVPA | [22,31] | [32] | 1/3 (33%) | ? |
| FMS-TPA | [5,47,50] | [21,22,24,25,26,44,46,49,53] | 9/12 (75%) | + |
| LMS-TPA | [5,22,25,47] | [26,27,31,44,46,51] | 6/10 (60%) | + |
| OCS-TPA | [5,47] | [22,25,26,27,31,34,44,46,51] | 9/11 (82%) | + |
| SS-TPA | [22,31] | [26,27] | 2/4 (50%) | ? |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xin, F.; Chen, S.-T.; Clark, C.; Hong, J.-T.; Liu, Y.; Cai, Y.-J. Relationship between Fundamental Movement Skills and Physical Activity in Preschool-aged Children: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 3566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103566
Xin F, Chen S-T, Clark C, Hong J-T, Liu Y, Cai Y-J. Relationship between Fundamental Movement Skills and Physical Activity in Preschool-aged Children: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(10):3566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103566
Chicago/Turabian StyleXin, Fei, Si-Tong Chen, Cain Clark, Jin-Tao Hong, Yang Liu, and Yu-Jun Cai. 2020. "Relationship between Fundamental Movement Skills and Physical Activity in Preschool-aged Children: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 10: 3566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103566