Effect of HIIT with Tabata Protocol on Serum Irisin, Physical Performance, and Body Composition in Men

 , , and
, , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Participants
2.2. Methods
2.2.1. Aerobic Performance
2.2.2. Anaerobic Performance
2.3. Biochemical Analysis
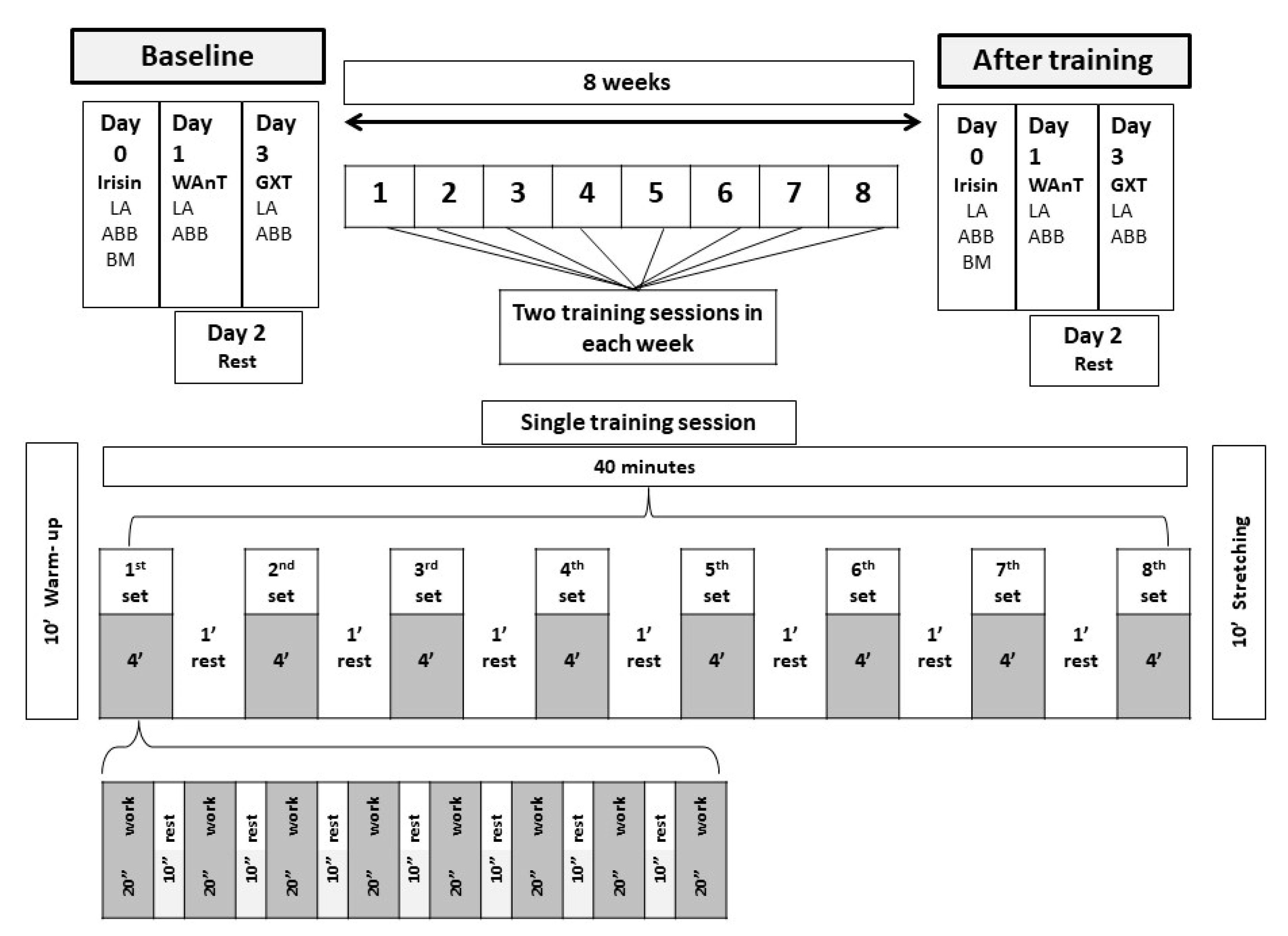
2.4. High Intensity Interval Training (HIIT) Training
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bartlett, J.D.; Close, G.L.; MacLaren, D.P.; Gregson, W.; Drust, B.; Morton, J.P. High-intensity interval running is perceived to be more enjoyable than moderate-intensity continuous exercise: Implications for exercise adherence. J. Sports Sci. 2011, 29, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Laursen, P.B.; Jenkins, D.G. The scientific basis for high-intensity interval training. Optimising training programmes and maximizing performance in highly trained endurance athletes. Sports Med. 2002, 32, 53–73. [Google Scholar] [CrossRef] [PubMed]
- Billat, L.V. Interval training for performance: A scientific and empirical practice. Special recommendations for middle- and long-distance running. Part I: Aerobic interval training. Sports Med. 2001, 31, 13–31. [Google Scholar] [CrossRef] [PubMed]
- Billat, L.V. Interval training for performance: A scientific and empirical practice. Special recommendations for middle- and long-distance running. Part II: Anaerobic interval training. Sports Med. 2001, 31, 75–90. [Google Scholar] [CrossRef] [PubMed]
- Kimm, S.Y.; Glynn, N.W.; McMahon, R.P.; Voorhees, C.C.; Striegel-Moore, R.H.; Daniels, S.R. Self-perceived barriers to activity participation among sedentary adolescent girls. Med. Sci. Sports Exerc. 2006, 38, 534–540. [Google Scholar] [CrossRef]
- Jung, M.E.; Bourne, J.E.; Little, J.P. Where does HIT fit? An examination of the affective response to high-intensity intervals in comparison to continuous moderate- and continuous vigorous-intensity exercise in the exercise intensity-affect continuum. PLoS ONE 2014, 9, e114541. [Google Scholar] [CrossRef] [Green Version]
- Gibala, M.J.; Gillen, J.B.; Percival, M.E. Physiological and health-related adaptations to low-volume interval training: Influences of nutrition and sex. Sports Med. 2014, 44 (Suppl. 2), 127–137. [Google Scholar] [CrossRef] [Green Version]
- Gillen, J.B.; Percival, M.E.; Skelly, L.E.; Martin, B.J.; Tan, R.B.; Tarnopolsky, M.A.; Gibala, M. Three minutes of all-out intermittent exercise per week increases skeletal muscle oxidative capacity and improves cardiometabolic health. PLoS ONE 2014, 9, e111489. [Google Scholar] [CrossRef]
- Skelly, L.E.; Andrews, P.C.; Gillen, J.B.; Martin, B.J.; Percival, M.E.; Gibala, M.J. High-intensity interval exercise induces 24-h energy expenditure similar to traditional endurance exercise despite reduced time commitment. Appl. Physiol. Nutr. Metab. 2014, 39, 1–4. [Google Scholar] [CrossRef]
- Siahkouhian, M.K.D.; Shahmoradi, K. Effects of high-intensity interval training on aerobic and anaerobic indices: Comparison of physically active an inactive men. Sci. Sports 2013, 28, 119–125. [Google Scholar] [CrossRef]
- Boutcher, S.H. High-intensity intermittent exercise and fast loss. J. Obes. 2011, 868305. [Google Scholar] [CrossRef] [Green Version]
- Shehata, A.; Mohmoud, I. Effect of high intensity interval tranining (HIIT) on weight, body mass index and body fat percentage for adults. Sci. Mov. Health 2018, 18, 125–130. [Google Scholar]
- Ouerghi, N.; Ben-Fradj, K.; Bezrati, I.; Khammassi, M.; Feki, N.; Bouassida, A. Effects of high-intensity interval training on body composition, aerobic and anaerobic performance and plasma lipids in overweight/obese and normal-weight young men. Biol. Sport 2017, 34, 385–392. [Google Scholar] [CrossRef]
- Türk, Y.; Theel, W.; Kasteleyn, W.; Franssen, F.M.E.; Hiemstra, P.S.; Rudolphus, A. High intensity training in obesity: A meta-analysis. Obes. Sci. Pract. 2017. [Google Scholar] [CrossRef] [Green Version]
- Hood, M.S.; Little, J.P.; Tarnopolsky, M.A.; Myslik, F.; Gibala, M.J. Low-volume interval training improves muscle oxidative capacity in sedentary adults. Med. Sci. Sports Exerc. 2011, 43, 1849–1856. [Google Scholar] [CrossRef]
- Hoshino, D.; Kitaoka, Y.; Hatta, H. High-intensity interval training enhances oxidative capacity and substrate availability in skeletal muscle. J. Phys. Fitness Sports Med. 2016, 5, 13–23. [Google Scholar] [CrossRef] [Green Version]
- Rakobowchuk, M.; Tanguay, S.; Burgomaster, K.A.; Howarth, K.R.; Gibala, M.J.; MacDonald, M.J. Sprint interval and traditional endurance training induce similar improvements in peripheral arterial stiffness and flow-mediated dilation in healthy humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2008, 295, 236–242. [Google Scholar] [CrossRef]
- Stenman, M.; Pesola, A.; Laukkanen, A.; Haapala, E. Effects of two-week high-intensity interval training on cognition in adolescents—A randomized controlled pilot study. Hum. Mov. 2018, 18, 15–20. [Google Scholar] [CrossRef]
- Alahmadi, M.A. High-intensity interval training and obesity. J. Nov. Physiother. 2014, 4, 211. [Google Scholar] [CrossRef] [Green Version]
- Alkahtani, S.A.; King, N.A.; Hills, A.P.; Byrne, N.M. Effect of interval training intensity on fat oxidation, blood lactate and the rate of perceived exertion in obese men. SpringerPlus 2013, 2, 532. [Google Scholar] [CrossRef] [Green Version]
- Francois, M.E.; Little, J.P. Effectiveness and safety of high-intensity interval training in patients with type 2 diabetes. Diabetes Spectr. 2015, 28, 39–44. [Google Scholar] [CrossRef] [Green Version]
- Matos, M.A.; Vieira, D.V.; Pinhal, K.C.; Lopes, J.F.; Dias-Peixoto, M.F.; Pauli, J.R.; Magalhães, F.C.; Little, J.P.; Rocha-Vieira, E.; Amorim, F.T. High-intensity interval training improves markers of oxidative metabolism in skeletal muscle of individuals with obesity and insulin resistance. Front. Physiol. 2018, 31, doi. [Google Scholar] [CrossRef] [Green Version]
- Khammassi, M.; Ouerghi, N.; Hadj-Taieb, S.; Feki, M.; Thivel, D.; Bouassida, A. Impact of a 12-week high-intensity interval training without caloric restriction on body composition and lipid profile in sedentary healthy overweight/obese youth. J. Exerc. Rehabil. 2018, 14, 118–125. [Google Scholar] [CrossRef] [Green Version]
- Feito, Y.; Brown, C.; Olmos, A. A content analysis of the high-intensity functional training literature: A look at the past and directions for the future. Hum. Mov. 2019, 20, 1–15. [Google Scholar] [CrossRef]
- Tabata, I.; Nishimura, K.; Kouzaki, M.; Hirai, Y.; Ogita, F.; Miyachi, M.; Yamamoto, K. Effects of moderate-intensity endurance and high-intensity intermittent training on anaerobic capacity and VO2max. Med. Sci. Sports Exerc. 1996, 28, 1327–1330. [Google Scholar] [CrossRef] [Green Version]
- Thompson, W. Worldwide survey of fitness trends for 2019. ACSM’s Health Fitness J. 2018, 22, 10–17. [Google Scholar] [CrossRef]
- Bostrom, P.; Wu, J.; Jedrychowski, M.P.; Korde, A.; Ye, L.; Lo, J.C.; Rasbach, K.A.; Boström, E.A.; Choi, J.H.; Long, J.Z.; et al. A PGC1-alpha-dependent myokine that drives brown-fat-like development of white fat and thermogenesis. Nature 2012, 481, 463–468. [Google Scholar] [CrossRef]
- Roca-Rivada, A.; Castelao, C.; Senin, L.L.; Landrove, M.O.; Baltar, J.; Crujeiras, A.; Seoane, L.M.; Casanueva, F.F.; Pardo, M. FNDC5/irisin is not only a myokine but also an adipokine. PLoS ONE 2013, 8, e60563. [Google Scholar] [CrossRef] [Green Version]
- Wrann, C.D.; White, J.P.; Salogiannnis, J.; Laznik-Bogoslavski, D.; Wu, J.; Ma, D.; Lin, J.D.; Greenberg, M.E.; Spiegelman, B.M. Exercise induces hippocampal BDNF through a PGC-1alpha/FNDC5 pathway. Cell Metab. 2013, 18, 649–659. [Google Scholar] [CrossRef] [Green Version]
- Mehrabian, S.; Taheri, E.; Karkhanenh, M.; Qorbani, M.; Hosseini, S. Association of circulating irisin levels with normal weight obesity; glycemic and lipid profile. J. Diabetes Metab. Disord. 2016, 15, 17. [Google Scholar] [CrossRef] [Green Version]
- Fukushima, Y.; Kurose, S.; Shinno, H.; Thi Thu, H.C.; Takao, N.; Tsutsumi, H.; Hasegawa, T.; Nakajima, T.; Kimura, Y. Effects of body weight reduction on serum irisin and metabolic parameters in obese subjects. Diabetes Metab. J. 2016, 40, 386–395. [Google Scholar] [CrossRef]
- Elsen, M.; Raschke, S.; Eckel, J. Browning of white fat: Does irisin play a role in humans? J. Endocrinol. 2014, 222, 25–38. [Google Scholar] [CrossRef] [Green Version]
- Dünnwald, T.; Melmer, A.; Gatterer, H.; Salzmann, K.; Ebenbichler, C.; Burtscher, M.; Schobersberger, W.; Grander, W. Supervised short-term high-intensity training on plasma irisin concentrations in type 2 diabetic patients. Int. J. Sports Med. 2019, 40, 158–164. [Google Scholar] [CrossRef]
- Li, D.J.; Li, Y.H.; Yuan, H.B.; Qu, L.F.; Wang, P. The novel exercise-induced hormone irisin protects against neuronal injury via activation of the Akt and ERK1/2 signaling pathways and contributes to the neuroprotection of physical exercise in cerebral ischemia. Metabolism 2017, 68, 31–42. [Google Scholar] [CrossRef] [Green Version]
- Aydin, S.; Aydin, S.; Kuloglu, T.; Yilmaz, M.; Kalayci, M.; Sahin, I.; Cicek, D. Alterations of irisin concentrations in saliva and serum of obese and normal-weight subjects; before and after 45 min of a Turkish bath or running. Peptides 2013, 50, 13–18. [Google Scholar] [CrossRef]
- Norheim, F.; Langleite, T.M.; Hjorth, M.; Holen, T.; Kielland, A.; Stadheim, H.K.; Gulseth, H.L.; Birkeland, K.I.; Jensen, J.; Drevon, C.A.; et al. The effects of acute and chronic exercise on PGC-1alpha; irisin and browning of subcutaneous adipose tissue in humans. FEBS J. 2014, 281, 739–749. [Google Scholar] [CrossRef]
- Pekkala, S.; Wiklund, P.K.; Hulmi, J.J.; Ahtiainen, J.P.; Horttanainen, M.; Pöllänen, E.; Mäkelä, K.A.; Kainulainen, H.; Häkkinen, K.; Nyman, K.; et al. Are skeletal muscle FNDC5 gene expression and irisin release regulated by exercise and related to health? J. Physiol. 2013, 591, 5393–5400. [Google Scholar] [CrossRef]
- Kraemer, R.R.; Shockett, P.; Webb, N.D.; Shah, U.; Castracane, V.D. A transient elevated irisin blood concentration in response to prolonged; moderate aerobic exercise in young men and women. Horm. Metab. Res. 2014, 46, 150–1538. [Google Scholar] [CrossRef]
- Huh, J.Y.; Mougios, V.; Kabasakalis, A.; Fatouros, I.; Siopi, A.; Douroudos, I.I.; Filippaios, A.; Panagiotou, G.; Park, K.H.; Mantzoros, C.S. Exercise-induced irisin secretion is independent of age or fitness level and increased irisin may directly modulate muscle metabolism through AMPK activation. J. Clin. Endocrinol. Metab. 2014, 99, 2154–2161. [Google Scholar] [CrossRef] [Green Version]
- Khodadadi, H.; Rajabi, H.; Seyyed Reza Attarzadeh, S.R.; Abbasian, S. The efect of high intensity interval training (HIIT) and pilates on levels of irisin and insulin resistance in overweight women. Iran. J. Endocrinol. Metab. 2014, 16, 190–196. [Google Scholar]
- Archundia-Herrera, C.; Macias-Cervantes, M.; Ruiz-Muñoz, B.; Vargas-Ortiz, K.; Kornhauser, C.; PerezVazquez, V. Muscle irisin response to aerobic vs HIIT in overweight female adolescents. Diabetol. Metab. Syndr. 2017, 9, 165–172. [Google Scholar] [CrossRef] [Green Version]
- Jeukendrup, A.; Gleeson, M. Sport Nutrition; Human Kinetics: Champaign, IL, USA, 2019. [Google Scholar]
- Edvardsen, E.; Hem, E.; Anderssen, A.A. End criteria for reaching maximal oxygen uptake must be strict and adjusted to sex and age: A cross-sectional study. PLoS ONE 2014, 9, e85276. [Google Scholar] [CrossRef] [Green Version]
- Driss, T.; Vandewalle, H. The measurement of maximal (anaerobic) power output on a cycle ergometer: A critical review. BioMed Res. Int. 2013, 589361. [Google Scholar] [CrossRef] [Green Version]
- Murawska-Cialowicz, E.; Wojna, J.; Zuwala-Jagiello, J. CrossFit training changes brain-derived neurotrophic factor and irisin levels at rest, after Wingate and progressive tests and improves aerobic capacity and body composition of young physically active men and women. J. Physiol. Pharm. 2015, 66, 811–825. [Google Scholar]
- Stengel, A.; Hofmann, T.; Goebel-Stengel, M.; Elbelt, U.; Kobelt, P.; Klapp, B.F. Circulating levels of irisin in patients with anorexia nervosa and different stages of obesity correlation with body mass index. Peptides 2013, 39, 125–130. [Google Scholar] [CrossRef]
- Timmons, J.A.; Baar, K.; Davidsen, P.K.; Atherton, P.J. Is irisin a human exercise gene? Nature 2012, 488, E9–E10. [Google Scholar] [CrossRef]
- Kurdiova, T.; Balaz, M.; Vician, M.; Maderova, D.; Vlcek, M.; Valkovic, L. Effects of obesity; diabetes and exercise on Fndc5 gene expression and irisin release in human skeletal muscle and adipose tissue: In vivo and in vitro studies. J. Physiol. 2014, 592, 1091–1107. [Google Scholar] [CrossRef]
- Daskalopoulou, S.S.; Cooke, A.B.; Gomez, Y.H.; Mutter, A.F.; Filippaios, A.; Mesfum, E.T. Plasma irisin levels progressively increase in response to increasing exercise workloads in young; healthy; active subjects. Eur. J. Endocrinol. 2014, 171, 343–352. [Google Scholar] [CrossRef]
- Kerstholt, N.; Ewert, R.; Nauck, M.; Spielhagen, T.; Bollmann, T.; Stubbe, B. Association of circulating irisin and cardiopulmonary exercise capacity in healthy volunteers: Results of the Study of Health in Pomerania. BMC Pulm. Med. 2015, 15, 41. [Google Scholar] [CrossRef] [Green Version]
- Foster, C.; Farland, C.V.; Guidotti, F.; Harbin, M.; Roberts, B.; Schuette, J. The effects of high intensity interval training vs steady state training on aerobic and anaerobic capacity. J. Sports Sci. Med. 2015, 14, 747–755. [Google Scholar]
- Burgomaster, K.A.; Howarth, K.R.; Phillips, S.M.; Rakobowchuk, M.; MacDonald, M.J.; McGee, S.L. Similar metabolic adaptations during exercise after low volume sprint interval and traditional endurance training in humans. J. Physiol. 2008, 586, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Trapp, E.G.; Chisholm, D.J.; Freund, J.; Boutcher, S.H. The effects of high-intensity intermittent exercise training on fat loss and fasting insulin levels of young women. Int. J. Obes. (Lond.) 2008, 32, 684–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talanian, J.L.; Galloway, S.D.; Heigenhauser, G.J.; Bonen, A.; Spriet, L.L. Two weeks of high-intensity aerobic interval training increases the capacity for fat oxidation during exercise in women. J. Appl. Physiol. 2007, 102, 1439–1447. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, K.H.J.; Sue, D.Y.; Stringer, W.W.; Whipp, B.J. Principles of Exercise Testing and Interpretation: Including Pathophysiology and Clinical Applications; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Little, J.P.; Safdar, A.; Wilkin, G.P.; Tarnopolsky, M.A.; Gibala, M.J. A practical model of low-volume high-intensity interval training induces mitochondrial biogenesis in human skeletal muscle: Potential mechanisms. J. Physiol. 2010, 588, 1011–1022. [Google Scholar] [CrossRef]
- Gibala, M.J.; Little, J.P.; MacDonald, M.J.; Hawley, J.A. Physiological adaptations to low-volume; high-intensity interval training in health and disease. J. Physiol. 2012, 590, 1077–1084. [Google Scholar] [CrossRef]
- Nalbandian, M.; Takeda, M. Lactate as a signaling molecule that regulates exercise-induced adaptations. Biology 2016, 5, 38. [Google Scholar] [CrossRef] [Green Version]
- Castro, F.; Aquino, R.; Júnior, J.; Gonçalves, L.; Puggina, E. Strength training with vascular occlusion: A review of possible adaptive mechanisms. Hum. Mov. 2017, 18, 3–14. [Google Scholar] [CrossRef]
- Clanton, T.L.; Klawitter, P.F. Physiological and genomic consequences of intermittent hypoxia invited review: Adaptive responses of skeletal muscle to intermittent hypoxia: The known and the unknown. J. Appl. Physiol. 2001, 90, 2476–2487. [Google Scholar] [CrossRef] [Green Version]
- Summermatter, S.; Santos, G.; Perez-Schindler, J.; Handschin, C. Skeletal muscle PGC-1alpha controls whole-body lactate homeostasis through estrogen-related receptor alpha-dependent activation of LDH B and repression of LDH A. Proc. Natl. Acad. Sci. USA 2013, 110, 8738–8743. [Google Scholar] [CrossRef] [Green Version]
- Perry, C.G.; Heigenhauser, G.J.; Bonen, A.; Spriet, L.L. High-intensity aerobic interval training increases fat and carbohydrate metabolic capacities in human skeletal muscle. Appl. Physiol. Nutr. Metab. 2008, 33, 1112–1123. [Google Scholar] [CrossRef]
- McNulty, C.R.; Robergs, R.A. Repeat trial and breath averaging: Recommendations for research of VO2 kinetics of exercise transitions to steady-state. Mov. Sport Sci./Sci. Mot. 2019, 106, 37–44. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | HT | Sedentary | HT vs. Sedentary | |||||
|---|---|---|---|---|---|---|---|---|
| Variable | Baseline | 8 Weeks | p | Baseline | 8 Weeks | p | Baseline | 8 Weeks |
| Body mass (kg) | 81.01 ± 12.44 | 79.05 ± 9.19 | 0.032 | 79.03 ± 12.05 | 79.70 ± 9.69 | 0.243 | 0.342 | 0.346 |
| LBM (kg) | 64.37 ± 9.58 | 68.62 ± 9.50 | 0.047 | 67.34 ± 8.36 | 67.72 ± 8.69 | 0.156 | 0.254 | 0.432 |
| FAT (kg) | 11.64 ± 4.05 | 10.43 ± 3.61 | 0.043 | 10.92 ± 3.42 | 11.32 ± 3.72 | 0.046 | 0.044 | 0.087 |
| % FAT | 14.44 ± 3.33 | 13.61 ± 3.16 | 0.018 | 12.44 ± 3.97 | 13.00 ± 4.21 | 0.096 | 0.009 | 0.324 |
| % LBM | 84.56 ± 3.37 | 86.39 ± 3.95 | 0.028 | 87.55 ± 6.79 | 72.34 ± 8.5 | 0.047 | 0.010 | 0.012 |
| LBM/FAT (kg) | 1.53 ± 0.70 | 1.85 ± 0.81 | 0.041 | 1.66 ± 0.60 | 1.59 ± 0.57 | 0.213 | 0.432 | 0.047 |
| VO2max (mL/min) | 3658.10 ± 487.04 | 3982.07 ± 575.95 | 0.028 | 3962.00 ± 568.19 | 4001.23 ± 695.33 | 0.102 | 0.021 | 0.134 |
| VO2max (mL/kg/min) | 44.86 ± 5.74 | 50.16 ± 5.80 | 0.005 | 47.16 ± 5.01 | 47.73 ± 5.07 | 0.231 | 0.432 | 0.059 |
| VEmax (L/min) | 139.52 ± 23.58 | 146.70 ± 24.68 | 0.048 | 151.50 ± 22.35 | 153.04 ± 25.31 | 0.212 | 0.040 | 0.062 |
| HRmax (b/min) | 185.30 ± 8.14 | 186.33 ± 6.89 | 0.193 | 190.11 ± 9.65 | 190.78 ± 7.81 | 0.342 | 0.254 | 0.102 |
| VT (L/min) | 2.86 ± 0.55 | 2.97 ± 0.69 | 0.124 | 2.87 ± 0.71 | 2.72 ± 0.57 | 0.143 | 0.110 | 0.231 |
| Vmax (km/h) | 16.60 ± 2.32 | 17.11 ± 1.76 | 0.049 | 17.71 ± 1.38 | 17.95 ± 1.65 | 0.219 | 0.231 | 0.232 |
| Time to exhaustion (min) | 16.40 ± 2.94 | 17.31 ± 2.79 | 0.005 | 17.34 ± 1.60 | 16.90 ± 1.69 | 0.025 | 0.097 | 0.058 |
| Groups | HT | Sedentary | HT vs. Sedentary | |||||
|---|---|---|---|---|---|---|---|---|
| Variables | Baseline | 8 Weeks | p | Baseline | 8 Weeks | p | Baseline | 8 Weeks |
| Pmax (W) | 794.2 ± 125.9 | 825.6 ± 127.4 | 0.046 | 840.3 ± 67.9 | 836.4 ± 68.8 | 0.043 | 0.031 | 0.437 |
| Pmax (W/kg) | 10.23 ± 0.64 | 11.87 ± 0.67 | 0.032 | 10.56 ± 0.66 | 10.46 ± 0.42 | 0.324 | 0.543 | 0.032 |
| T1 (s) | 4.84 ± 1.62 | 3.79 ± 0.93 | 0.037 | 4.71 ± 1.47 | 4.11 ± 0.65 | 0.049 | 0.231 | 0.031 |
| T2 (s) | 3.45 ± 1.90 | 3.09 ± 1.12 | 0.143 | 3.41 ± 1.77 | 2.96 ± 0.75 | 0.132 | 0.432 | 0.237 |
| Pend (W/kg) | 6.51 ± 0.59 | 6.35 ± 1.55 | 0.212 | 6.41 ± 0.55 | 6.43 ± 0.62 | 0.345 | 0.453 | 0.543 |
| Pmean (W/kg) | 8.07 ± 0.69 | 8.09 ± 1.55 | 0.103 | 8.33 ± 0.48 | 8.28 ± 0.43 | 0.372 | 0.076 | 0.067 |
| IF (%) | 24.03 ± 4.85 | 24.12 ± 3.90 | 0.324 | 22.72 ± 5.14 | 23.63 ± 2.17 | 0.105 | 0.003 | 0.049 |
| TW (kJ) | 19.03 ± 2.53 | 18.86 ± 2.64 | 0.097 | 19.91 ± 19.54 | 19.54 ± 1.66 | 0.432 | 0.231 | 0.067 |
| TW (J/kg) | 240.14 ± 13.08 | 240.72 ± 17.08 | 0.342 | 252.85 ± 14.64 | 242.76 ± 16.50 | 0.041 | 0.040 | 0.342 |
| LA (mmol/L) | 11.5 ± 1.5 | 10.11 ± 1.7 | 0.022 | 9.3 ± 2.2 | 9.2 ± 2.0 | 0.436 | 0.032 | 0.012 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murawska-Cialowicz, E.; Wolanski, P.; Zuwala-Jagiello, J.; Feito, Y.; Petr, M.; Kokstejn, J.; Stastny, P.; Goliński, D. Effect of HIIT with Tabata Protocol on Serum Irisin, Physical Performance, and Body Composition in Men. Int. J. Environ. Res. Public Health 2020, 17, 3589. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103589
Murawska-Cialowicz E, Wolanski P, Zuwala-Jagiello J, Feito Y, Petr M, Kokstejn J, Stastny P, Goliński D. Effect of HIIT with Tabata Protocol on Serum Irisin, Physical Performance, and Body Composition in Men. International Journal of Environmental Research and Public Health. 2020; 17(10):3589. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103589
Chicago/Turabian StyleMurawska-Cialowicz, Eugenia, Pawel Wolanski, Jolanta Zuwala-Jagiello, Yuri Feito, Miroslav Petr, Jakub Kokstejn, Petr Stastny, and Dawid Goliński. 2020. "Effect of HIIT with Tabata Protocol on Serum Irisin, Physical Performance, and Body Composition in Men" International Journal of Environmental Research and Public Health 17, no. 10: 3589. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103589