Caries Increment and Salivary Microbiome during University Life: A Prospective Cohort Study

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
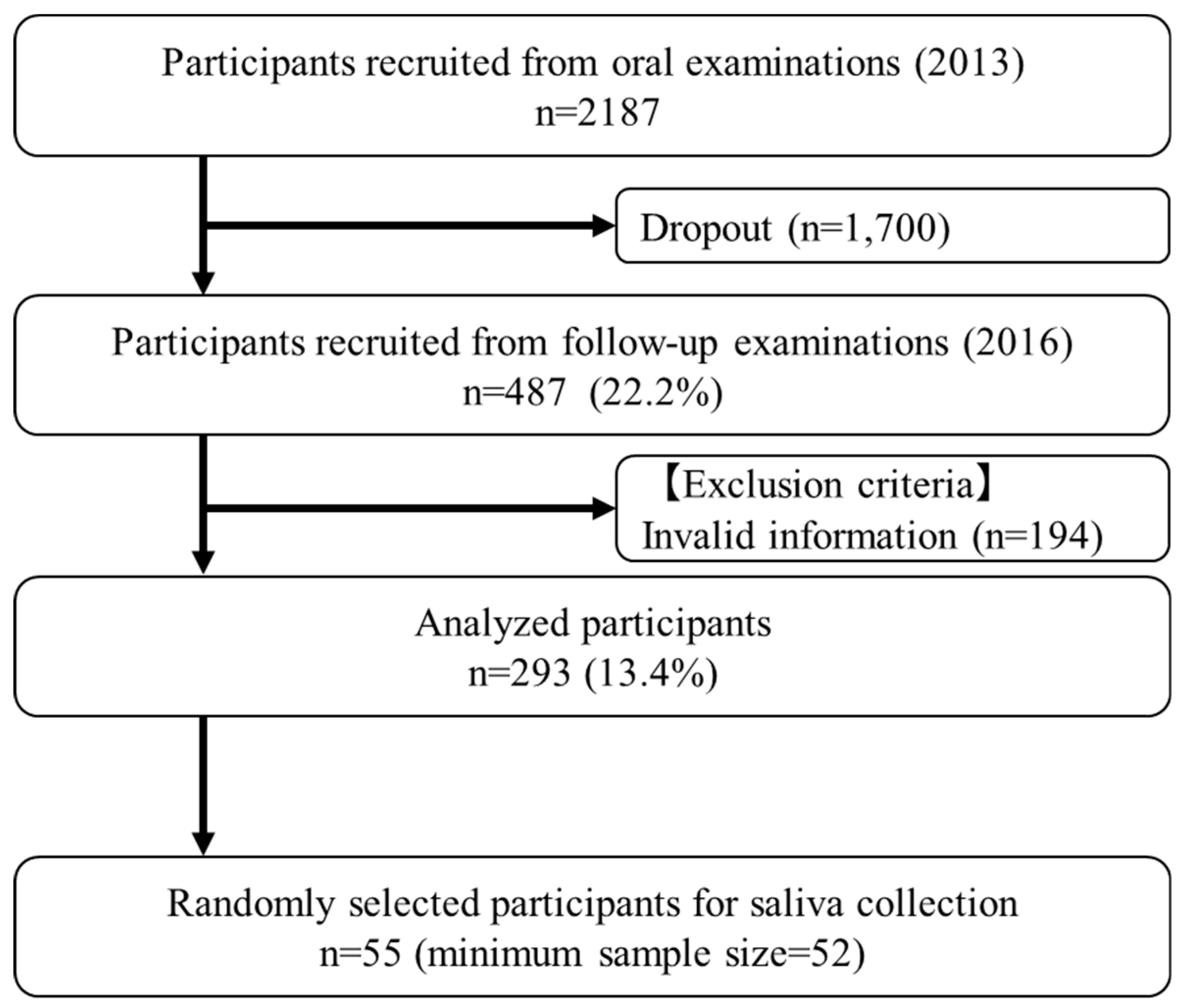
2.1. Study Population
2.2. Ethical Procedures and Informed Consent
2.3. Questionnaire
2.4. Oral Examination
2.5. DNA Extraction and NGS Analysis
2.6. Statistical Analyses
3. Results
3.1. Participant Characteristics
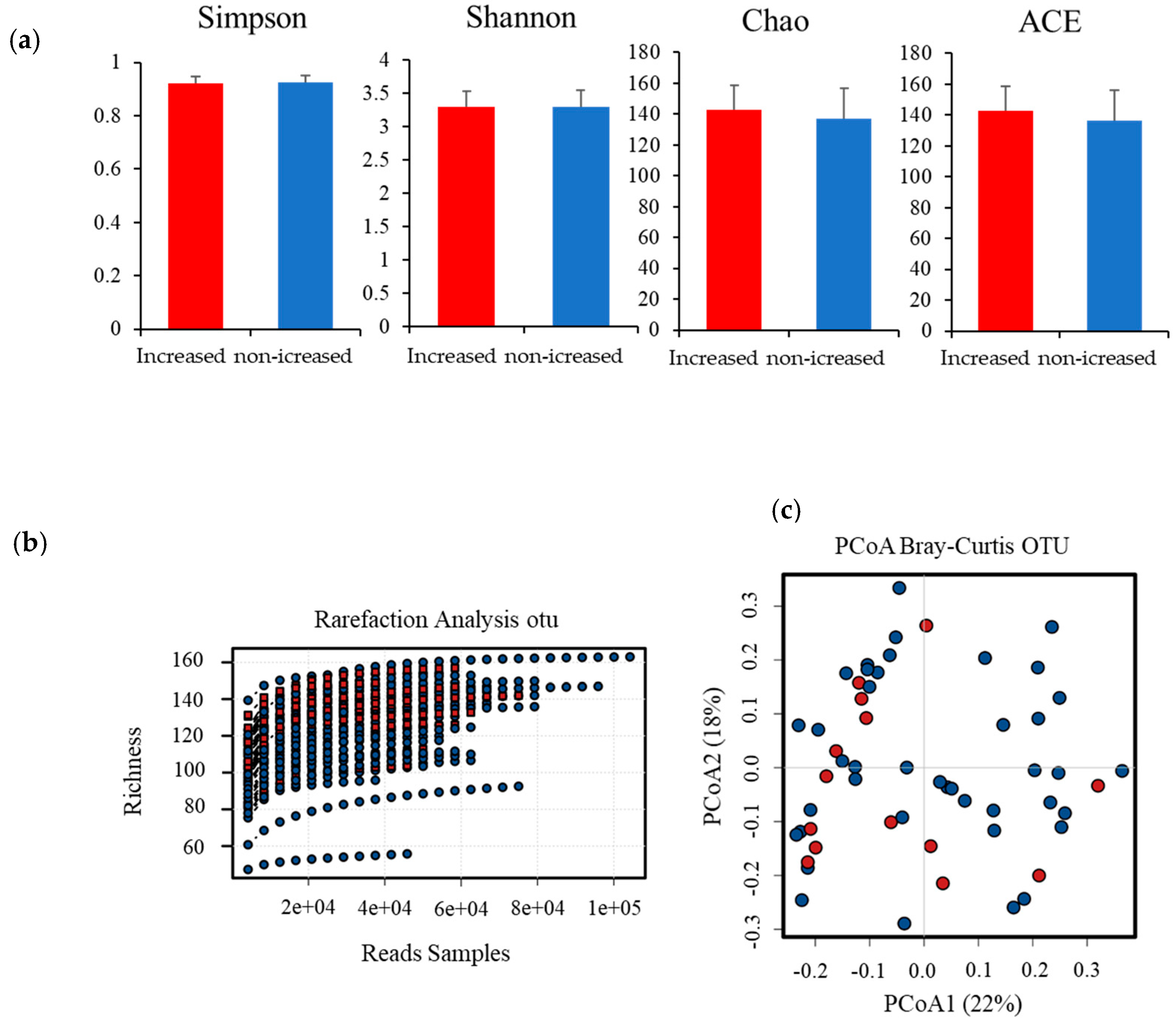
3.2. Salivary Microbiome Analysis
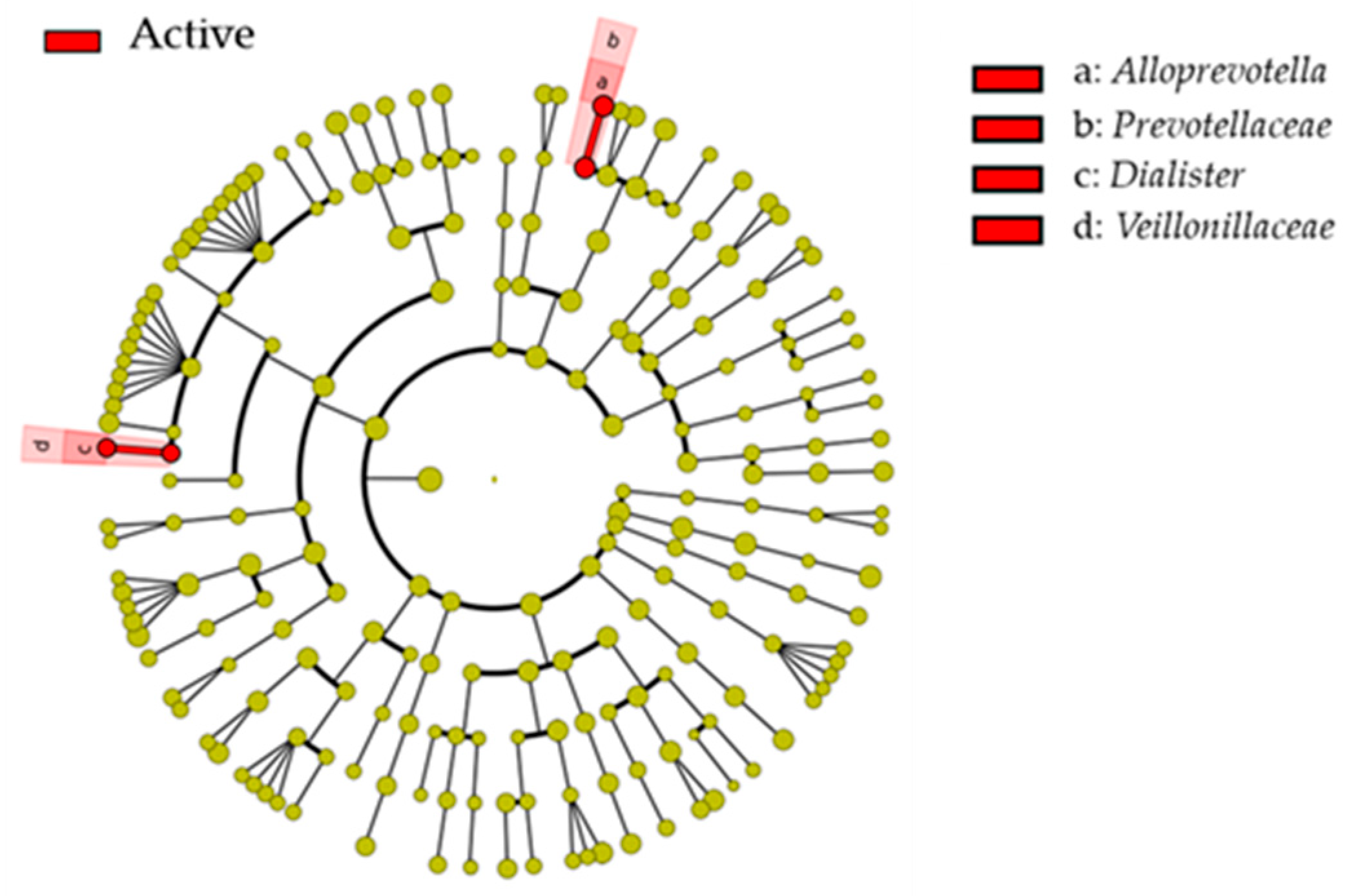
3.3. Microbial Composition
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kassebaum, N.; Smith, A.G.C.; Bernabé, E.; Fleming, T.D.; Reynolds, A.E.; Vos, T.; Murray, C.J.L.; Marcenes, W.; GBD 2015 Oral Health Collaborators. Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990–2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J. Dent. Res. 2017, 96, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef]
- Schulze-Schweifing, K.; Banerjee, A.; Wade, W.G. Comparison of bacterial culture and 16S rRNA community profiling by clonal analysis and pyrosequencing for the characterization of the dentine caries-associated microbiome. Front. Cell Infect. Microbiol. 2014, 12, 164. [Google Scholar] [CrossRef]
- Xu, L.; Chen, X.; Wang, Y.; Jiang, W.; Wang, S.; Ling, Z.; Chen, H. Dynamic alterations in salivary microbiota related to dental caries and age in preschool children with deciduous dentition: A 2-Year Follow-Up Study. Front. Physiol. 2018, 4, 342. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, N.; Nyvad, B. Ecological Hypothesis of Dentin and Root Caries. Caries Res. 2016, 50, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Aas, J.A.; Griffen, A.L.; Dardis, S.R.; Lee, A.M.; Olsen, I.; Dewhirst, F.E.; Leys, E.J.; Paster, B.J. Bacteria of dental caries in primary and permanent teeth in children and young adults. J. Clin. Microbiol. 2008, 46, 1407–1417. [Google Scholar] [CrossRef] [Green Version]
- Jiang, W.; Ling, Z.; Lin, X.; Chen, Y.; Zhang, J.; Yu, J.; Xiang, C.; Chen, H. Pyrosequencing analysis of oral microbiota shifting in various caries states in childhood. Microb. Ecol. 2014, 67, 962–969. [Google Scholar] [CrossRef]
- Jiang, S.; Gao, X.; Jin, L.; Lo, E.C.M. Salivary Microbiome Diversity in Caries-Free and Caries-Affected Children. Int. J. Mol. Sci. 2016, 17, 1978. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Hao, W.; Zhou, Q.; Wang, W.; Xia, Z.; Liu, C.; Chen, X.; Qin, M.; Chen, F. Plaque bacterial microbiome diversity in children younger than 30 months with or without caries prior to eruption of second primary molars. PLoS ONE 2014, 28, e89269. [Google Scholar] [CrossRef]
- Xu, H.; Tian, J.; Hao, W.; Zhang, Q.; Zhou, Q.; Shi, W.; Qin, M.; He, X.; Chen, F. Oral Microbiome Shifts from Caries-Free to Caries-Affected Status in 3-Year-Old Chinese Children: A Longitudinal Study. Front. Microbiol. 2018, 28, 2009. [Google Scholar] [CrossRef]
- Survey of Dental Disease in Japan. 2016. Available online: https://www.mhlw.go.jp/toukei/list/62-17c.html (accessed on 1 February 2019).
- Mizutani, S.; Ekuni, D.; Tomofuji, T.; Irie, K.; Azuma, T.; Iwasaki, Y.; Morita, M. Self-efficacy and progression of periodontal disease: A prospective cohort study. J. Clin. Periodontol. 2015, 42, 1083–1089. [Google Scholar] [CrossRef] [PubMed]
- Greene, J.C.; Vermillion, J.R. The simplified oral hygiene index. J. Am. Dent. Assoc. 1964, 68, 7–13. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Oral Health Survey. Basic Methods, 4th ed.; World Health Organization: Geneva, Switzerland, 1997. [Google Scholar]
- Mohamed, R.; Campbell LCooper-White, J.; Dimeski, G.; Punyadeera, C. The impact of saliva collection and processing methods on CRP, IgE, and Myoglobin immunoassays. Clin. Transl. Med. 2012, 1, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Principe, S.; Hui, A.B.; Bruce, J.; Sinha, A.; Liu, F.F.; Kislinger, T. Tumor-derived exosomes and microvesicles in head and neck cancer: Implications for tumor biology and biomarker discovery. Proteomics 2013, 13, 1608–1623. [Google Scholar] [CrossRef]
- Yakob, M.; Fuentes, L.; Wang, M.B.; Abemayor, E.; Wong, D.T. Salivary biomarkers for detection of oral squamous cell carcinoma—current state and recent advances. Curr. Oral. Health Rep. 2014, 1, 133–141. [Google Scholar] [CrossRef] [Green Version]
- Kunitomo, M.; Ekuni, D.; Mizutani, S.; Tomofuji, T.; Irie, K.; Azuma, T.; Yamane, M.; Kataoka, K.; Taniguchi-Tabata, A.; Mizuno, H.; et al. Association between Knowledge about Comprehensive Food Education and Increase in Dental Caries in Japanese University Students: A Prospective Cohort Study. Nutrients 2016, 8, 114. [Google Scholar] [CrossRef] [Green Version]
- Johansson, I.; Witkowska, E.; Kaveh, B.; Lif Holgerson, P.; Tanner, A.C. The Microbiome in Populations with a Low and High Prevalence of Caries. J. Dent. Res. 2016, 95, 80–86. [Google Scholar] [CrossRef]
- Eriksson, L.; Lif Holgerson, P.; Johansson, I. Saliva and tooth biofilm bacterial microbiota in adolescents in a low caries community. Sci. Rep. 2017, 7, 5861. [Google Scholar] [CrossRef] [Green Version]
- Belstrom, D.; Fiehn, N.E.; Nielsen, C.H.; Holmstrup, P.; Kirkby, N.; Klepac-Ceraj, V.; Paster, B.J.; Twetman, S. Altered bacterial profiles in saliva from adults with caries lesions: A case-cohort study. Caries Res. 2014, 48, 368–375. [Google Scholar] [CrossRef]
- Kim, B.S.; Han, D.H.; Lee, H.; Oh, B. Association of Salivary Microbiota with Dental Caries Incidence with Dentine Involvement after 4 Years. J. Microbiol. Biotechnol. 2018, 28, 454–464. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Q.; Liu, J.; Chen, L.; Gan, N.; Yang, D. The oral microbiome in the elderly with dental caries and health. Front. Cell Infect. Microbiol. 2018, 4, 442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chhour, K.L.; Nadkarni, M.A.; Byun, R.; Martin, F.E.; Jacques, N.A.; Hunter, N. Molecular analysis of microbial diversity in advanced caries. J. Clin. Microbiol. 2005, 43, 843–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, F.; Zeng, X.; Ning, K.; Liu, K.L.; Lo, C.C.; Wang, W.; Chen, J.; Wang, D.; Huang, R.; Chang, X.; et al. Saliva microbiomes distinguish caries-active from healthy human populations. ISME J. 2012, 6, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, N.; Nyvad, B. The role of bacteria in the caries process: Ecological perspectives. J. Dent. Res. 2011, 90, 294–303. [Google Scholar] [CrossRef] [PubMed]
- Gross, E.; Leys, E.; Gasparovich, S.; Firestone, N.; Schwartzbaum, J.; Janies, D.; Asnani, K.; Griffen, A. Bacterial 16S sequence analysis of severe caries in young permanent teeth. J. Clin. Microbiol. 2010, 48, 4121–4128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foxman, B.; Luo, T.; Srinivasan, U.; Ramadugu, K.; Wen, A.; Goldberg, D.; Shedden, K.; Crout, R.; McNeil, D.W.; Weyant, R.; et al. The effects of family, dentition, and dental caries on the salivary microbiome. Ann. Epidemiol. 2016, 26, 348–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Söderström, U.; Johansson, I.; Sunnegårdh-Grönberg, K. A retrospective analysis of caries treatment and development in relation to assessed caries risk in an adult population in Sweden. BMC Oral. Health 2014, 17, 126. [Google Scholar] [CrossRef] [Green Version]
- Tafere, Y.; Chanie, S.; Dessie, T.; Gedamu, H. Assessment of prevalence of dental caries and the associated factors among patients attending dental clinic in Debre Tabor general hospital: A hospital-based cross-sectional study. BMC Oral. Health 2018, 18, 119. [Google Scholar] [CrossRef] [Green Version]
- Van Houte, J. Role of micro-organisms in caries etiology. J. Dent. Res. 1994, 73, 672–681. [Google Scholar] [CrossRef]
- Inquimbert, C.; Bourgeois, D.; Bravo, M.; Viennot, S.; Tramini, P.; Llodra, J.C.; Molinari, N.; Dussart, C.; Giraudeau, N.; Carrouel, F. The oral bacterial microbiome of interdental surfaces in adolescents according to carious risk. Microorganisms 2019, 7, 319. [Google Scholar] [CrossRef] [Green Version]
- Takeshita, T.; Kageyama, S.; Furuta, M.; Tsuboi, H.; Takeuchi, K.; Shibata, Y.; Shimazaki, Y.; Akifusa, S.; Ninomiya, T.; Kiyohara, Y.; et al. Bacterial diversity in saliva and oral health-related conditions: The Hisayama Study. Sci. Rep. 2016, 24, 22164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chattopadhyay, I.; Verma, M.; Panda, M. Role of Oral Microbiome Signatures in Diagnosis and Prognosis of Oral Cancer. Technol. Cancer Res. Treat. 2019, 18, 1533033819867354. [Google Scholar] [CrossRef] [Green Version]
- Patil, P.B.; Patil, B.R. Saliva: A diagnostic biomarker of periodontal diseases. J. Indian Soc. Periodontol. 2011, 15, 310–317. [Google Scholar] [CrossRef]
- Lorenzo-Pouso, A.I.; Pérez-Sayáns, M.; Bravo, S.B.; López-Jornet, P.; García-Vence, M.; Alonso-Sampedro, M.; Carballo, J.; García-García, A. Protein-Based Salivary Profiles as Novel Biomarkers for Oral Diseases. Dis. Markers 2018, 7, 6141845. [Google Scholar] [CrossRef] [PubMed]
- Fisher-Owens, S.A.; Gansky, S.A.; Platt, L.J.; Weintraub, J.A.; Soobader, M.J.; Bramlett, M.D.; Newacheck, P.W. Influences on children’s oral health: A conceptual model. Pediatrics 2007, 120, 510–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furuta, M.; Ekuni, D.; Takao, S.; Suzuki, E.; Morita, M.; Kawachi, I. Social capital and self-rated oral health among young people. Community Dent. Oral. Epidemiol. 2012, 40, 97–104. [Google Scholar] [CrossRef]
- Slade, G.D. Epidemiology of dental pain and dental caries among children and adolescents. Community Dent. Health 2001, 18, 219–227. [Google Scholar]
- Belstrøm, D.; Holmstrup, P.; Bardow, A.; Kokaras, A.; Fiehn, N.E.; Paster, B.J. Comparative analysis of bacterial profiles in unstimulated and stimulated saliva samples. J. Oral. Microbiol. 2016, 16, 30112. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total Participants | Selected Participants | p-Value 3 | ||
|---|---|---|---|---|---|
| (n = 293) | (n = 55) | ||||
| Baseline | Gender | Male/Female | 149/144 (50.9/49.1) 1 | 17/38 (30.9/69.1) | 0.006 |
| Age (year) | 18.22 ± 0.76 2 | 18.24 ± 0.47 | 0.378 | ||
| Number of teeth present | 28.49 ± 1.43 | 28.42 ± 1.49 | 0.699 | ||
| DMFT score | 1.00 ± 2.01 | 1.44 ± 2.79 | 0.459 | ||
| DI-S | 0.41 ± 0.37 | 0.33 ± 0.32 | 0.363 | ||
| Daily frequency of tooth brushing | 1 | 55 (18.8) | 9 (16.4) | 0.914 | |
| 2 | 212 (72.4) | 41 (74.5) | |||
| 3 | 26 (8.9) | 5 (9.1) | |||
| Use of dental floss | yes | 20 (6.8) | 5 (9.1) | 0.551 | |
| Regular dental check-ups | yes | 36 (12.3) | 13 (23.6) | 0.034 | |
| Follow-up | Number of teeth present | 29.2 ± 1.77 | 28.9 ± 1.78 | 0.353 | |
| DMFT score | 1.70 ± 2.99 | 1.82 ± 2.97 | 0.477 | ||
| DI-S | 0.81 ± 2.49 | 0.31 ± 0.36 | 0.037 | ||
| Daily frequency of tooth brushing | 1 | 45 (15.4) | 8 (14.5) | 0.323 | |
| 2 | 220 (75.1) | 38 (69.1) | |||
| 3 | 28 (9.6) | 9 (16.4) | |||
| Use of dental floss | yes | 45 (15.4) | 12 (21.8) | 0.237 | |
| Regular dental check-ups | yes | 41 (14.0) | 11 (20.0) | 0.301 | |
| Current smoker | yes | 9 (3.07) | 2 (3.36) | ||
| Use of fluoride containing paste | yes | 155 (52.9) | 28 (50.9) | 0.883 | |
| Knowledge of the effectiveness of fluoride | yes | 250 (85.3) | 46 (83.6) | 0.686 | |
| Frequency of sweet intake (daily) | 0 | 53 (18.1) | 8 (14.5) | 0.295 | |
| 1 | 163 (55.6) | 37 (67.3) | |||
| 2 | 56 (19.1) | 9 (16.4) | |||
| 3 | 21 (7.2) | 1 (1.8) | |||
| Variable | Total Participants(n = 293) | Selected Participants(n = 55) | ||||||
|---|---|---|---|---|---|---|---|---|
| Non-Increased | Increased | p-Value 3 | Non-Increased | Increased | p-Value | |||
| (n = 220) | (n = 73) | (n = 41) | (n = 14) | |||||
| Baseline | Number of teeth present | 28.37 ± 0.37 1 | 28.82 ± 1.65 | 0.017 | 28.27 ± 1.28 | 28.86 ± 1.95 | 0.127 | |
| DMFT score | 0.78 ± 0.12 | 1.68 ± 2.35 | <0.001 | 1.32 ± 2.64 | 1.79 ± 3.28 | 0.71 | ||
| DI-S | 0.38 ± 0.35 | 0.52 ± 0.42 | 0.008 | 0.33 ± 0.29 | 0.43 ± 0.41 | 0.619 | ||
| Daily frequency of tooth brushing | 1 | 38 (17.3) 2 | 17 (23.3) | 0.452 | 8 (19.5) | 1 (7.1) | 0.504 | |
| 2 | 161 (73.2) | 51 (69.9) | 29 (65.9) | 12 (85.7) | ||||
| 3 | 21 (9.5) | 5 (6.8) | 4 (9.8) | 1 (7.1) | ||||
| Use of dental floss | yes | 15 (6.8) | 5 (6.8) | 0.993 | 2 (4.9) | 3 (21.4) | 0.063 | |
| Regular dental check-ups | yes | 23 (10.5) | 13 (17.8) | 0.097 | 9 (22) | 4 (28.6) | 0.615 | |
| Follow-up | Number of teeth present | 29.22 ± 1.77 | 29.36 ± 1.82 | 0.323 | 28.78 ± 1.74 | 29.29 ± 1.93 | 0.371 | |
| DMFT score | 0.78 ± 0.12 | 4.26 ± 3.98 | <0.001 | 1.32 ± 2.64 | 3.28 ± 3.49 | <0.001 | ||
| DI-S | 0.94 ± 2.87 | 0.43 ± 0.42 | 0.932 | 0.33 ± 0.37 | 0.27 ± 0.37 | 0.372 | ||
| Daily frequency of tooth brushing | 1 | 12 (15.4) | 34 (15.4) | 0.522 | 7 (17.8) | 1 (7.1) | 0.522 | |
| 2 | 61 (78.2) | 164 (73.9) | 27 (65.9) | 11 (78.6) | ||||
| 3 | 5 (6.4) | 24 (10.8) | 7 (17.1) | 2 (14.3) | ||||
| Use of dental floss | yes | 30 (13.6) | 15 (20.5) | 0.156 | 8 (19.5) | 4 (28.6) | 0.479 | |
| Regular dental check-ups | yes | 29 (13.2) | 12 (16.4) | 0.487 | 8 (19.5) | 3 (21.4) | 0.877 | |
| Current smoker | yes | 7 (3.2) | 2 (2.7) | 0.982 | 1 (2.4) | 1 (7.1) | 0.448 | |
| Use of fluoride containing paste | yes | 116 (52.7) | 39 (53.4) | 0.918 | 18 (43.9) | 10 (71.4) | 0.075 | |
| Knowledge of the effectiveness of fluoride | yes | 182 (82.7) | 68 (93.2) | 0.029 | 34 (82.9) | 12 (85.7) | 0.808 | |
| Frequency of sweet intake (daily) | 0 | 41 (18.6) | 12 (16.4) | 0.769 | 7 (17.1) | 1 (7.1) | 0.693 | |
| 1 | 124 (56.4) | 39 (53.4) | 29 (63.4) | 11 (78.6) | ||||
| 2 | 39 (17.7) | 17 (23.3) | 7 (17.1) | 2 (14.3) | ||||
| 3 | 16 (7.3) | 5 (6.8) | 1 (2.4) | 0 (0.0) | ||||
| Taxonomy Level | Non-Increased | Increased | p-Value 2 | |
|---|---|---|---|---|
| (n = 41) | (n = 14) | |||
| Phylum | Proteobacteria | 10.5 ±7.8 1 | 12.2 ± 4.3 | 0.029 |
| Family | Prevotellaceae | 1.6 ± 1.6 | 2.6 ± 2 | 0.007 |
| Genera | Alloprevotella | 1.6 ± 1.6 | 2.6 ± 2 | 0.007 |
| Dialister | 0.2 ± 0.3 | 0.3 ± 0.5 | 0.039 | |
| Actinobaculum | 0.1 ± 0.1 | 0.1 ± 0.1 | 0.008 | |
| Species | Neisseria sicca; n. mucosa | 2.3 ± 2.8 | 3 ± 2.5 | 0.042 |
| Alloprevotella sp. | 1.1 ± 1.3 | 1.7 ± 1.7 | 0.009 | |
| Dialister invisus | 0.1 ± 0.3 | 0.3 ± 0.5 | 0.037 | |
| Cardiobacterium hominis | 0.3 ± 0.7 | 0.4 ± 0.6 | 0.037 | |
| Acinetobacter sp. | 0.3 ± 0.5 | 0.5 ± 0.5 | 0.001 | |
| GN02 [G-1] | 0.1 ± 0.3 | 0.2 ± 0.3 | 0.031 | |
| Neisseria elongata | 0.4 ± 0.8 | 0.7 ± 1 | 0.034 | |
| Actinomyces graevenitzii | 0.1 ± 0.1 | 0.1 ± 0.2 | 0.024 | |
| Anaerolineae [G-1] | 0.1 ± 0.1 | 0.2 ± 0.2 | 0.032 | |
| Dialister pneumosintes | 0.1 ± 0.1 | 0.1 ± 0.2 | 0.015 | |
| Haemophilus haemolyticus | 0.1 ± 0.2 | 0.2 ± 0.4 | 0.019 | |
| Actinobaculum sp. | 0.1 ± 0.1 | 0.1 ± 0.1 | 0.008 | |
| Corynebacterium matruchotii | 0.1 ± 0.1 | 0.1 ± 0.1 | 0.042 | |
| Prevotella pleuritidis | 0.1 ± 0.1 | 0.1 ± 0.2 | 0.014 | |
| Neisseria sp. | 0.1 ± 0.1 | 0.1 ± 0.1 | 0.021 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uchida-Fukuhara, Y.; Ekuni, D.; Islam, M.M.; Kataoka, K.; Taniguchi-Tabata, A.; Fukuhara, D.; Toyama, N.; Kobayashi, T.; Fujimori, K.; Sawada, N.; et al. Caries Increment and Salivary Microbiome during University Life: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 3713. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103713
Uchida-Fukuhara Y, Ekuni D, Islam MM, Kataoka K, Taniguchi-Tabata A, Fukuhara D, Toyama N, Kobayashi T, Fujimori K, Sawada N, et al. Caries Increment and Salivary Microbiome during University Life: A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(10):3713. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103713
Chicago/Turabian StyleUchida-Fukuhara, Yoko, Daisuke Ekuni, Md Monirul Islam, Kota Kataoka, Ayano Taniguchi-Tabata, Daiki Fukuhara, Naoki Toyama, Terumasa Kobayashi, Kohei Fujimori, Nanami Sawada, and et al. 2020. "Caries Increment and Salivary Microbiome during University Life: A Prospective Cohort Study" International Journal of Environmental Research and Public Health 17, no. 10: 3713. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17103713