Patterning in Patient Referral to and Uptake of a National Exercise Referral Scheme (NERS) in Wales from 2008 to 2017: A Data Linkage Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Participants
2.2. NERS Intervention
2.3. Study Data
2.4. Statistical Analysis
2.5. Ethics
3. Results
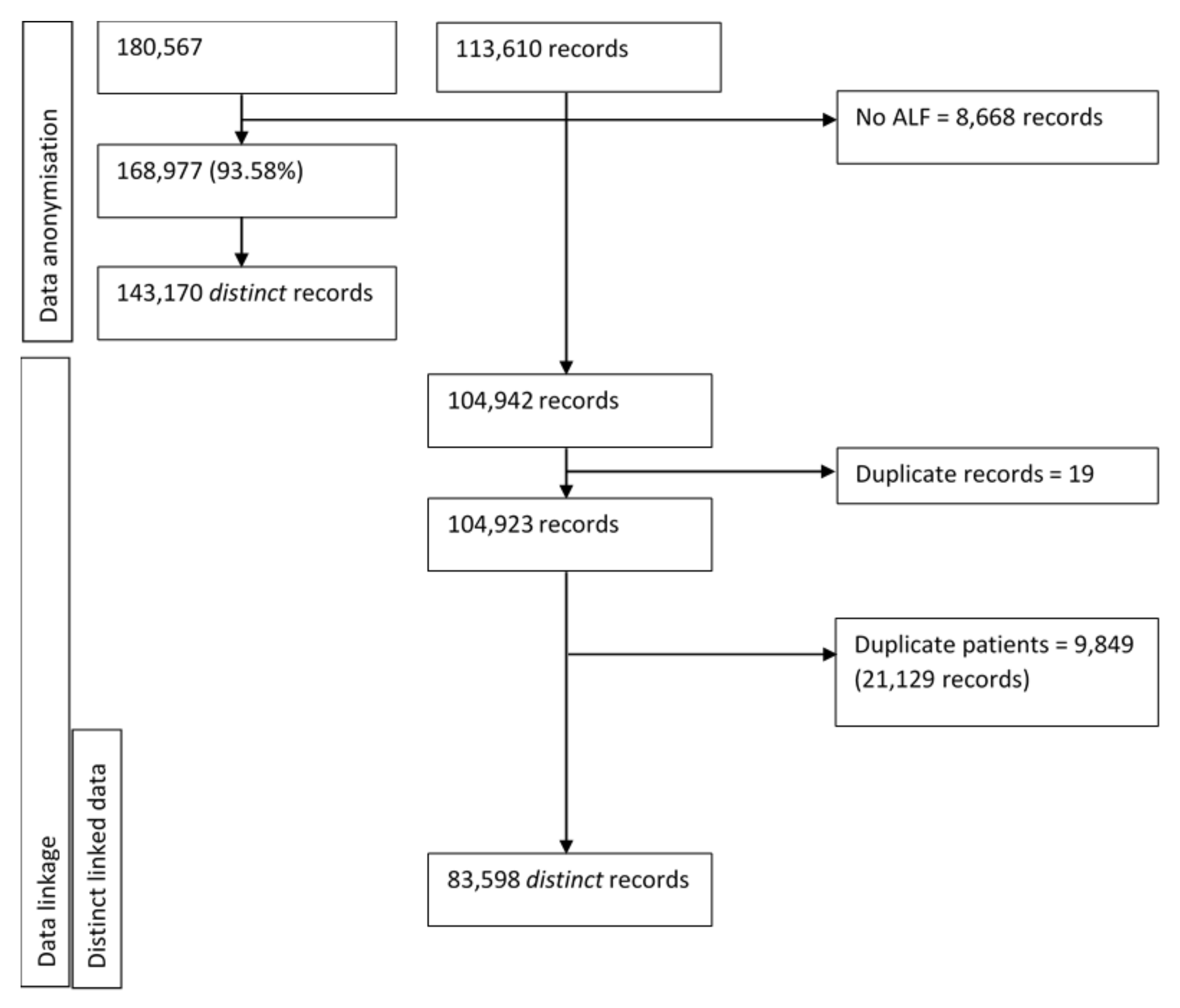
3.1. Data Linkage
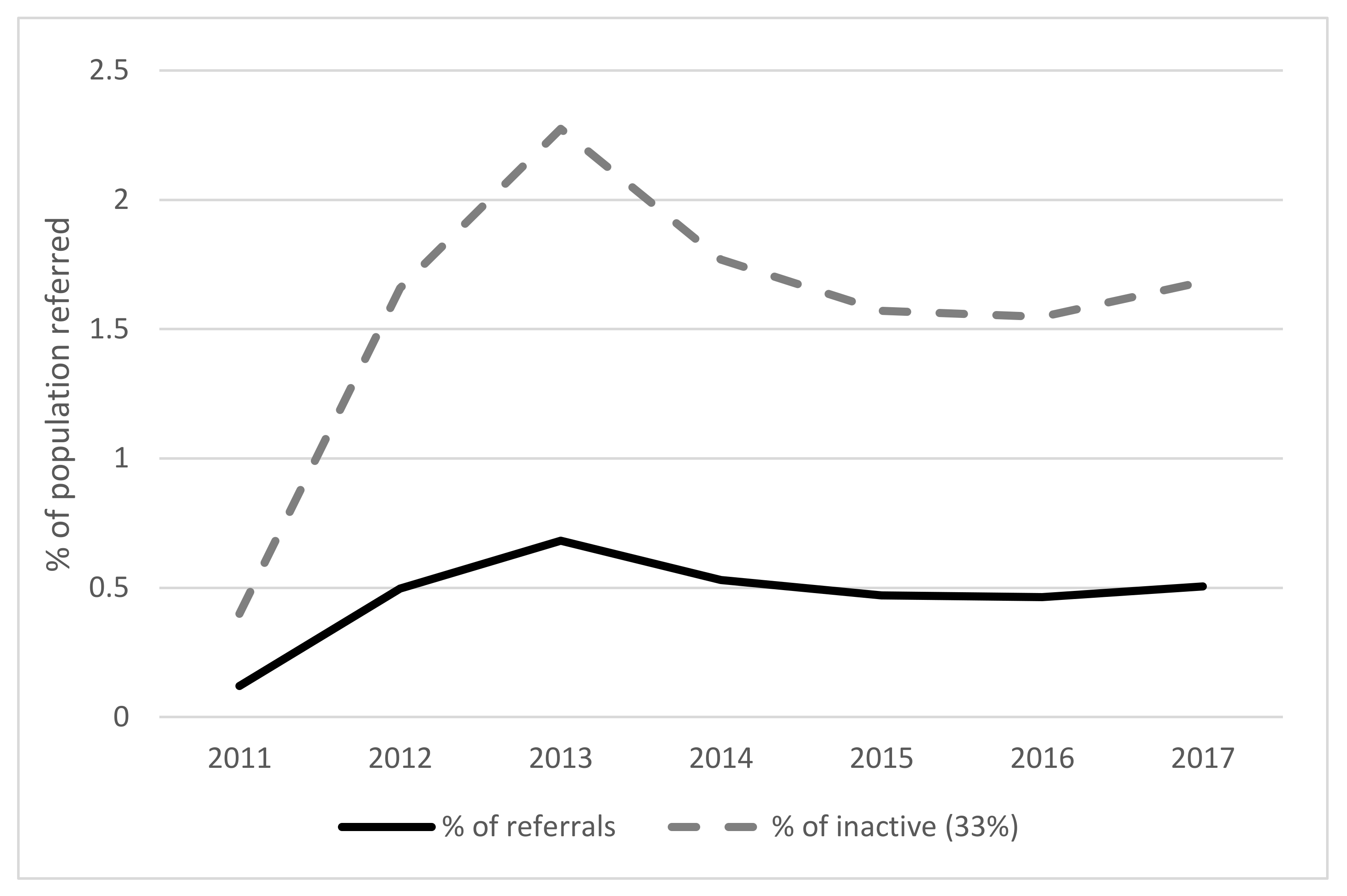
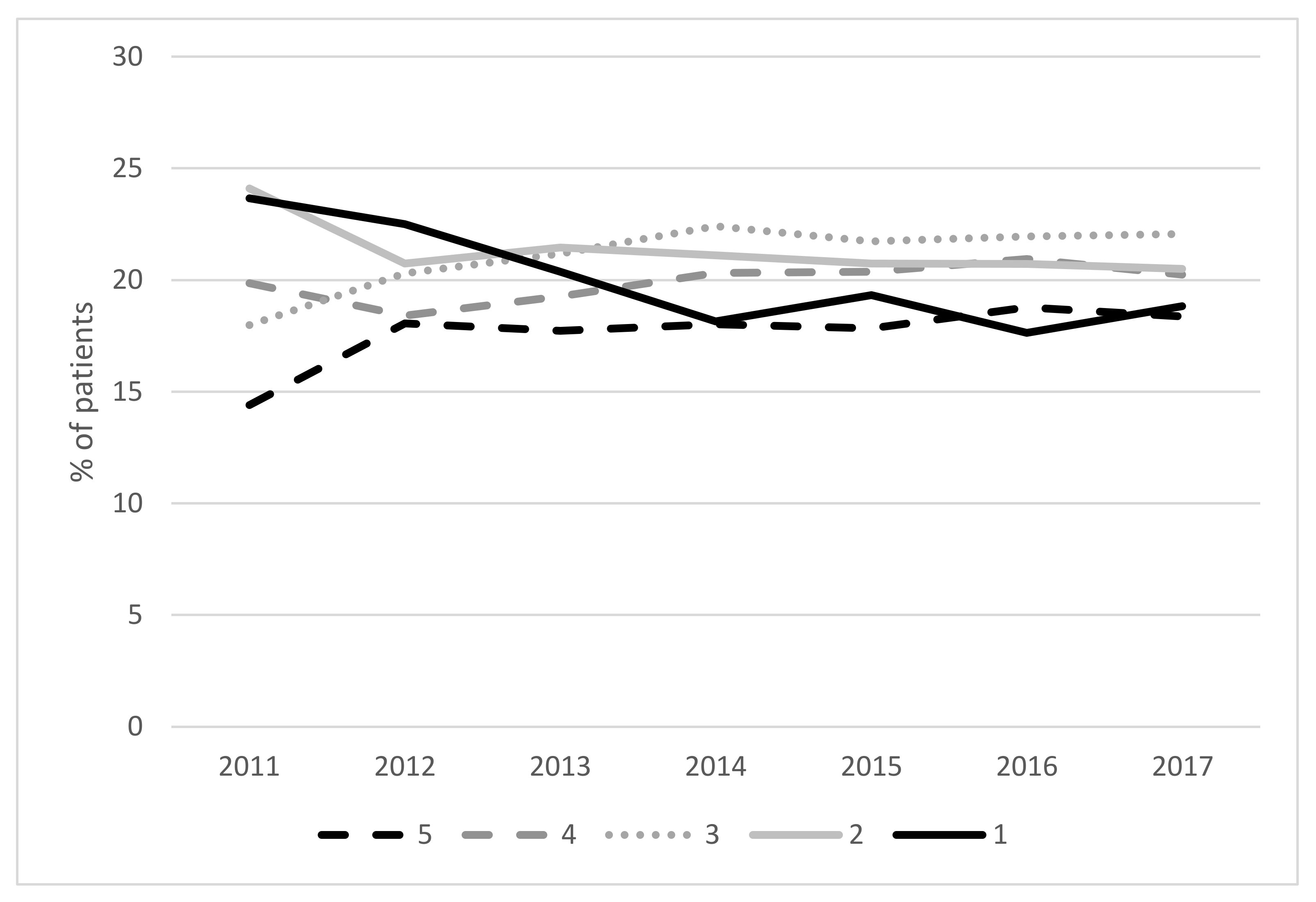
3.2. Scheme Referral
3.3. Scheme Uptake
3.4. Predictors of Scheme Uptake
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Haskell, W.; Lee, I.-M.; Pate, R.; Powell, K.; Blair, S.; Franklin, B.; Macera, C.; Heath, G.; Thompson, P.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. J. Circ. 2007, 16, 1081–1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. Global Recommendations on Physical Activity for Health; World Health Organisation: Geneva, Switzerland, 2010. [Google Scholar]
- World Health Organisation. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organisation: Geneva, Switzerland, 2018. [Google Scholar]
- National Institute for Health and Clinical Excellence. A Rapid Review of the Effectiveness of Exercise Referral Schemes to Promote Physical Activity in Adults; National Institute for Health and Clinical Excellence: London, UK, 2006. [Google Scholar]
- Pavey, T.G.; Taylor, A.H.; Fox, K.R.; Hillsdon, M.; Anokye, N.; Campbell, J.L.; Foster, C.; Green, C.; Moxham, T.; Mutrie, N.; et al. Effect of exercise referral schemes in primary care on physical activity and improving health outcomes: Systematic review and meta-analysis. BMJ 2011, 343, d6462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wadem, M.; Mann, S.; Copeland, R.J.; Steele, J. Effect of exercise referral schemes upon health and well-being: Initial observational insights using individual patient data meta-analysis from the National Referral Database. J. Epidemiol. Commun. Health 2020, 74, 32–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rowley, N.; Mann, S.; Steele, J.; Horton, E.; Jimenez, A. The effects of exercise referral schemes in the United Kingdom in those with cardiovascular, mental health, and musculoskeletal disorders: A preliminary systematic review. BM Public Health 2018, 18, 949. [Google Scholar] [CrossRef] [Green Version]
- Glasgow, R.E.; Lichtenstein, E.; Marcus, A.C. Why don’t we see more translation of health promotion research to practice? Rethinking the efficacy-to-effectiveness transition. Am. J. Public Health 2003, 93, 1261–1267. [Google Scholar] [CrossRef]
- Chaudoir, S.R.; Dugan, A.G.; Barr, C.H. Measuring factors affecting implementation of health innovations: A systematic review of structural, organizational, provider, patient, and innovation level measures. Implement Sci. 2013, 8, 22. [Google Scholar] [CrossRef] [Green Version]
- Bumbarger, B.; Perkins, D. After randomised trials: Issues related to dissemination of evidence-based interventions. J. Child. Serv. 2008, 3, 55–64. [Google Scholar] [CrossRef]
- Department of Health. Exercise Referral Systems: A National Quality Assurance Framework; Department of Health: London, UK, 2001.
- Iliffe, S.T.S.; Gould, M.; Thorogood, M.; Hillsdon, M. Prescribing exercise in general practice. BMJ 1994, 309, 494–495. [Google Scholar] [CrossRef]
- Hillsdon, M.T.M. A systematic review of physical activity promotion strategies. Br. J. Sports Med. 1996, 30, 84–89. [Google Scholar] [CrossRef] [Green Version]
- Pavey, T.G.; Anokye, N.; Taylor, A.H.; Trueman, P.; Moxham, T.; Fox, K.R.; Hillsdon, M.; Green, C.; Campbell, J.L.; Foster, C.; et al. The clinical effectiveness and cost-effectiveness of exercise referral schemes: A systematic review and economic evaluation. Health Technol Assess. 2011, 15, 1–254. [Google Scholar] [CrossRef] [Green Version]
- Williams, N.H.; Hendry, M.; France, B.; Lewis, R.; Wilkinson, C. Effectiveness of exercise-referral schemes to promote physical activity in adults: Systematic review. Br. J. Gener. Pract. J. R. Coll. Gener. Pract. 2007, 57, 979–986. [Google Scholar] [CrossRef]
- Gidlow, C.; Johnston, L.H.; Crone, D.; James, D. Attendance of exercise referral schemes in the UK: A systematic review. Health Educ. J. 2005, 64, 168–186. [Google Scholar] [CrossRef]
- Stevens, W.; Hillsdon, M.; Thorogood, M.; McArdle, D. Cost-effectiveness of a primary care based physical activity intervention in 45–74 year old men and women: A randomised controlled trial. Br. J. Sports Med. 1998, 32, 236–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, S.M.; Edwards, R.T.; Williams, N.; Raisanen, L.; Moore, G.; Linck, P.; Hounsome, N.; Din, N.; Moore, L. An evaluation of the effectiveness and cost effectiveness of the National Exercise Referral Scheme in Wales, UK: A randomised controlled trial of a public health policy initiative. J. Epidemiol. Commun. Health 2012, 66, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Kennedy-Martin, T.; Curtis, S.; Faries, D.; Robinson, S.; Johnston, J. A literature review on the representativeness of randomized controlled trial samples and implications for the external validity of trial results. Trials 2015, 16, 495. [Google Scholar] [CrossRef] [Green Version]
- Shore, C.B.; Hubbard, G.; Gorely, T.; Polson, R.; Hunter, A.; Galloway, S.D. Insufficient reporting of factors associated with exercise referral scheme uptake, attendance, and adherence: A systematic review of reviews. J. Phys. Act. Health 2019, 16, 667. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the public health impact of health promotion interventions: The RE-AIM framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef] [Green Version]
- Pavey, T.; Taylor, A.; Hillsdon, M.; Fox, K.; Campbell, J.; Foster, C.; Moxham, T.; Mutrie, N.; Searle, J.; Taylor, R. Levels and predictors of exercise referral scheme uptake and adherence: A systematic review. J. Epidemiol. Commun. Health 2012, 66, 737–744. [Google Scholar] [CrossRef]
- Harrison, R.A.; McNair, F.; Dugdill, L. Access to exercise referral schemes—A population based analysis. J. Public Health 2005, 27, 326–330. [Google Scholar] [CrossRef]
- Gidlow, C.; Johnston, L.H.; Crone, D.; Morris, C.; Smith, A.; Foster, C.; James, D. Socio-demographic patterning of referral, uptake and attendance in Physical Activity Referral Schemes. J. Public Health 2007, 29, 107–113. [Google Scholar] [CrossRef] [Green Version]
- Isaacs, A.J.; Critchley, J.A.; Tai, S.S.; Buckingham, K.; Westley, D.; Harridge, S.D.; Smith, C.; Gottlieb, J. Exercise Evaluation Randomised Trial (EXERT): A randomised trial comparing GP referral for leisure centre-based exercise, community-based walking and advice only. Health Technol. Assess 2007, 11, 1–165. [Google Scholar] [CrossRef] [Green Version]
- Damush, T.M.; Stump, T.E.; Saporito, A.; Clark, D.O. Predictors of older primary care patients’ participation in a submaximal exercise test and a supervised, low-impact exercise class. Prevent. Med. 2001, 33, 485–494. [Google Scholar] [CrossRef] [PubMed]
- Birtwistle, S.B.; Ashcroft, G.; Murphy, R.; Gee, I.; Poole, H.; Watson, P.M. Factors influencing patient uptake of an exercise referral scheme: A qualitative study. Health Educ. Res. 2018, 34, 113–127. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Physical Activity: Exercise Referral Schemes. Public Health Guideline [PH54]. 2014. Available online: https://www.nice.org.uk/guidance/ph54 (accessed on 24 September 2014).
- Steele, J.; Wade, M.; Polley, M.; Copeland, R.J.; Stokes, S.; Mann, S. The National Referral Database: An Initial Overview. 2019. Available online: https://0-doi-org.brum.beds.ac.uk/10.31236/osf.io/rgywq (accessed on 21 March 2020).
- Jones, K.; Ford, D.V.; Thompson, S.; Lyons, R.A. A profile of the SAIL databank on the UK secure research platform. Int. J. Popu. Data Sci. 2019, 4, 3. [Google Scholar] [CrossRef] [Green Version]
- Jones, K.H.; Ford, D.V.; Jones, C.; Dsilva, R.; Thompson, S.; Brooks, C.J.; Heaven, M.L.; Thayer, D.S.; McNerney, C.L.; Lyons, R.A. A case study of the Secure Anonymous Information Linkage (SAIL) Gateway: A privacy-protecting remote access system for health-related research and evaluation. J. Biomed. Inform. 2014, 50, 196–204. [Google Scholar] [CrossRef] [Green Version]
- Welsh Government. Welsh Index of Multiple Deprivation 2014. Executive Summary; 2014. Available online: https://gov.wales/sites/default/files/statistics-and-research/2019-05/welsh-index-of-multiple-deprivation-wimd-2014-executive-summary.pdf (accessed on 9 August 2018).
- Statistics for Wales. National Survey for Wales 2018-19: Adult Lifestyle. 2019. Available online: https://gov.wales/sites/default/files/statistics-and-research/2019-06/national-survey-for-wales-april-2018-to-march-2019-adult-lifestyle-534.pdf (accessed on 16 July 2019).
- Lehmann, B.A.; Lindert, L.; Ohlmeier, S.; Schlomann, L.; Pfaff, H.; Choi, K.-E. “And then he got into the wrong group”: A qualitative study exploring the effects of randomization in recruitment to a randomized controlled trial. Int. J. Environ. Res. Public Health 2020, 17, 1886. [Google Scholar] [CrossRef] [Green Version]
- Din, N.U.; Moore, G.F.; Murphy, S.; Wilkinson, C.; Williams, N.H. Health professionals’ perspectives on exercise referral and physical activity promotion in primary care: Findings from a process evaluation of the National Exercise Referral Scheme in Wales. Health Educ. J. 2015, 74, 743–757. [Google Scholar] [CrossRef] [Green Version]
- NICE. Physical Activity: Brief Advice for Adults in Primary Care; NICE: London, UK, 2013. [Google Scholar]
- Hansen, D.; Rovelo Ruiz, G.; Doherty, P.; Iliou, M.C.; Vromen, T.; Hinton, S.; Frederix, I.; Wilhelm, M.; Schmid, J.; Abreu, A.; et al. Do clinicians prescribe exercise similarly in patients with different cardiovascular diseases? Findings from the EAPC EXPERT working group survey. Eur. J. Prevent. Cardiol. 2018, 25, 682–691. [Google Scholar] [CrossRef]
- Yarborough, B.J.H.; Stumbo, S.P.; Cavese, J.A.; Yarborough, M.T.; Green, C.A. Patient perspectives on how living with a mental illness affects making and maintaining healthy lifestyle changes. Patient Educ. Counsel. 2019, 102, 346–351. [Google Scholar] [CrossRef]
- Sowden, S.L.; Breeze, E.; Barber, J.; Raine, R. Do general practices provide equitable access to physical activity interventions? Br. J. Gener. Pract. 2008, 58, e1–e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dugdill, L.; Graham, R.C.; McNair, F. Exercise referral: The public health panacea for physical activity promotion? A critical perspective of exercise referral schemes; their development and evaluation. Ergonomics 2005, 48, 1390–1410. [Google Scholar] [CrossRef] [PubMed]
- Duda, J.L.; Williams, G.C.; Ntoumanis, N.; Daley, A.; Eves, F.F.; Mutrie, N.; Rouse, P.; Lodhia, R.; Blamey, R.; Jolly, K. Effects of a standard provision versus an autonomy supportive exercise referral programme on physical activity, quality of life and well-being indicators: A cluster randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 10. [Google Scholar] [CrossRef] [Green Version]
- Rouse, P.C.; Ntoumanis, N.; Duda, J.L.; Jolly, K.; Williams, G.C. In the beginning: Role of autonomy support on the motivation, mental health and intentions of participants entering an exercise referral scheme. Psychol. Health 2011, 26, 729–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalder, M.; Wiles, N.J.; Campbell, J.; Hollinghurst, S.P.; Haase, A.M.; Taylor, A.H.; Fox, K.; Costelloe, C.; Searle, A.; Baxter, H.; et al. Facilitated physical activity as a treatment for depressed adults: Randomised controlled trial. BMJ Br. Med. J. 2012, 344, e2758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glowacki, K.; Arbour-Nicitopoulos, K.; Burrows, M.; Chesick, L.; Heinemann, L.; Irving, S.; Lam, R.; Macridis, S.; Michalak, E.; Scott, A.; et al. It’s more than just a referral: Development of an evidence-informed exercise and depression toolkit. Mental Health Phys. Acti. 2019, 17, 100297. [Google Scholar] [CrossRef]
- Crone, D.; Johnston, L.H.; Gidlow, C.; Henley, C.; James, D.V. Uptake and participation in physical activity referral schemes in the UK: An investigation of patients referred with mental health problems. Issues Ment. Health Nurs. 2008, 29, 1088–1097. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. NICE Impact Mental Health; NICE: London, UK, 2019. [Google Scholar]
- Department of Health. Annual Report of the Chief Medical Officer 2013, Public Mental Health Priorities: Investing in the Evidence. 2014. Available online: Gov.uk/government/publications/chief-medical-officer-cmoannual-report-public-mental-health (accessed on 19 February 2016).
- Yang, L.; Zhao, Y.; Wang, Y.; Liu, L.; Zhang, X.; Li, B.; Cui, R. The effects of psychological stress on depression. Curr. Neuropharmacol. 2015, 13, 494–504. [Google Scholar] [CrossRef] [Green Version]
- Marmot, M.W.R. Social Determinants of Health., 2nd ed.; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- Tudor Hart, J. The inverse care law. Lancet 1971, 297, 405–412. [Google Scholar] [CrossRef] [Green Version]
- Mercer, S.W.; Watt, G.C. The inverse care law: Clinical primary care encounters in deprived and affluent areas of Scotland. Anna. Fam. Med. 2007, 5, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Dayan, M. Are Parts of England ’Left Behind’ by the NHS? Nuffield Trust Comment. 2018. Available online: https://www.nuffieldtrust.org.uk/news-item/are-parts-of-england-left-behind-by-the-nhs (accessed on 11 May 2019).
- MacRae, K. Commentary: Socioeconomic deprivation and health and the ecological fallacy. BMJ 1994, 309, 1478–1479. [Google Scholar] [CrossRef] [PubMed]
- Age Discrimination Info. Age Discrimination Statistics. 2020. Available online: http://www.agediscrimination.info/statistics (accessed on 22 January 2020).
- National Assembly for Wales Finance Committee. The Cost of Caring for an Ageing Population. National Assembly for Wales Commission. 2018. Available online: https://www.assembly.wales/laid%20documents/cr-ld11773/cr-ld11773-e.pdf (accessed on 22 January 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Overall | N | % |
|---|---|---|---|
| 83,598 | |||
| Sex | 83,487 | ||
| Male | 32,027 | 38.36 | |
| Female | 51,460 | 61.64 | |
| Unknown | 111 | 0.13 | |
| Age (years) | 83,598 | ||
| <16 | 72 | 0.09 | |
| 16–44 | 25,846 | 30.92 | |
| 45–59 | 24,890 | 29.77 | |
| 60+ | 32,790 | 39.22 | |
| LSOA quintile | 76,628 | ||
| 5 (Least deprived) | 13,748 | 17.94 | |
| 4 | 15,208 | 19.85 | |
| 3 | 16,428 | 21.44 | |
| 2 | 16,147 | 21.07 | |
| 1 (Most deprived) | 15,097 | 19.70 | |
| Reason for referral | 83,569 | ||
| CHD only | 17,622 | 21.09 | |
| Mental health only | 9724 | 11.64 | |
| Musculoskeletal | 42,137 | 50.42 | |
| Level 4 | 7424 | 8.88 | |
| CHD and mental health | 6662 | 7.97 | |
| Referrer type | 83,598 | ||
| GP | 48,304 | 57.78 | |
| Physiotherapist | 26,194 | 31.33 | |
| Other | 9100 | 10.89 |
| Characteristic | Overall | N | % | Uptake | Did Not Take Up |
|---|---|---|---|---|---|
| 75,470 | 50,800 | 24,670 | |||
| Sex | 75,470 | ||||
| Male | 28,873 | 38.26 | 19,229 (66.60) | 9644 (33.40) | |
| Female | 46,527 | 61.65 | 31,524 (67.75) | 15,003 (32.25) | |
| Unknown | 70 | 0.09 | 47 (67.14) | 23 (32.86) | |
| Age (years) | 75,470 | ||||
| 16–44 | 23,117 | 30.63 | 12,959 (56.06) | 10,158 (43.94) | |
| 45–59 | 22,494 | 29.81 | 15,028 (66.81) | 7466 (33.19) | |
| 60+ | 29,859 | 39.56 | 22,813 (76.40) | 7046 (23.60) | |
| LSOA quintile | 69,316 | ||||
| 5 (Least deprived) | 12,605 | 18.18 | 9129 (72.42) | 3476 (27.58) | |
| 4 | 13,721 | 19.79 | 9594 (69.92) | 4127 (30.08) | |
| 3 | 14,776 | 21.32 | 10,165 (68.79) | 4611 (31.21) | |
| 2 | 14,573 | 21.02 | 9503 (65.21) | 5070 (34.79) | |
| 1 (Most deprived) | 13,641 | 19.68 | 8300 (60.85) | 5341 (39.15) | |
| Reason for referral | 75,442 | ||||
| CHD only | 15,800 | 20.94 | 10,699 (67.72) | 5101 (32.28) | |
| Mental health only | 9603 | 12.73 | 4677 (54.36) | 3926 (45.64) | |
| Musculoskeletal | 38,121 | 50.53 | 26,301 (68.99) | 11,820 (31.01) | |
| Level 4 | 6889 | 9.13 | 5370 (77.95) | 1519 (22.05) | |
| CHD and mental health | 6029 | 7.99 | 3730 (61.87) | 2299 (38.13) | |
| Referrer type | 75,470 | ||||
| GP | 43,742 | 57.96 | 29,449 (67.32) | 14,293 (32.68) | |
| Physiotherapist | 23,633 | 31.31 | 16,170 (68.42) | 7463 (31.58) | |
| Other | 8095 | 10.73 | 5181 (64.00) | 2914 (36.00) | |
| Year of referral ^ | 75,470 | ||||
| 2008 | <10 | 5 | <5 | ||
| 2009 | <100 | 51 | <36 | ||
| 2010 | <500 | 397 | <36 | ||
| 2011 | 2703 | 3.58 | 2171 (80.32) | 532 (19.68) | |
| 2012 | 11,814 | 15.65 | 7975 (67.50) | 3839 (32.50) | |
| 2013 | 16,417 | 21.75 | 10,438 (63.58) | 5979 (36.42) | |
| 2014 | 12,311 | 16.31 | 8086 (65.68) | 4225 (34.32) | |
| 2015 | 10,910 | 14.46 | 7349 (67.36) | 3561 (32.64) | |
| 2016 | 10,573 | 14.01 | 7206 (68.15) | 3367 (31.85) | |
| 2017 | 10,246 | 13.58 | 7122 (69.51) | 3124 (30.49) | |
| Trial area | 75,470 | ||||
| Yes | 42,796 | 56.71 | 29,486 (68.90) | 13,310 (31.10) | |
| No | 32,674 | 43.29 | 21,314 (65.23) | 11,360 (34.77) |
| Characteristic | OR | p | 95% Confidence Interval | |
|---|---|---|---|---|
| Lower | Upper | |||
| Gender (Female) | ||||
| Male | 0.90 | <0.001 | 0.87 | 0.94 |
| Age (16–44 years) | ||||
| 45–59 | 1.50 | <0.001 | 1.44 | 1.56 |
| 60+ | 2.37 | <0.001 | 2.27 | 2.47 |
| Deprivation quintile (5-least deprived) | ||||
| 4 | 0.86 | <0.001 | 0.81 | 0.91 |
| 3 | 0.86 | <0.001 | 0.81 | 0.91 |
| 2 | 0.76 | <0.001 | 0.72 | 0.81 |
| 1 (most deprived) | 0.70 | <0.001 | 0.66 | 0.74 |
| Reason for referral (CHD only) | ||||
| Mental health only | 0.79 | <0.001 | 0.74 | 0.84 |
| Musculoskeletal | 1.15 | <0.001 | 1.09 | 1.20 |
| Level 4 | 1.90 | <0.001 | 1.76 | 2.05 |
| CHD and mental health | 0.93 | 0.055 | 0.87 | 1.00 |
| Referrer (GP) | ||||
| Physiotherapist | 0.88 | <0.001 | 0.85 | 0.92 |
| Other | 0.84 | <0.001 | 0.80 | 0.89 |
| Referral year (2017) | ||||
| 2008 | 2.48 | 0.425 | 0.27 | 22.99 |
| 2009 | 3.15 | 0.006 | 1.39 | 7.14 |
| 2010 | 5.18 | <0.001 | 3.59 | 7.47 |
| 2011 | 1.96 | <0.001 | 1.74 | 2.20 |
| 2012 | 1.06 | 0.092 | 0.99 | 1.13 |
| 2013 | 0.87 | <0.001 | 0.82 | 0.92 |
| 2014 | 0.86 | <0.001 | 0.81 | 0.92 |
| 2015 | 0.94 | 0.061 | 0.88 | 1.00 |
| 2016 | 0.93 | 0.024 | 0.87 | 0.99 |
| Trial area (Yes) | 1.34 | 0.267 | 0.80 | 2.26 |
| Area deprivation | 1.00 | 0.59 | 0.98 | 1.01 |
| ICC—constant only | 0.10 | |||
| ICC—level 1 variables | 0.11 | |||
| ICC—level 1 & 2 variables | 0.10 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morgan, K.; Rahman, M.; Moore, G. Patterning in Patient Referral to and Uptake of a National Exercise Referral Scheme (NERS) in Wales from 2008 to 2017: A Data Linkage Study. Int. J. Environ. Res. Public Health 2020, 17, 3942. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113942
Morgan K, Rahman M, Moore G. Patterning in Patient Referral to and Uptake of a National Exercise Referral Scheme (NERS) in Wales from 2008 to 2017: A Data Linkage Study. International Journal of Environmental Research and Public Health. 2020; 17(11):3942. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113942
Chicago/Turabian StyleMorgan, Kelly, Muhammad Rahman, and Graham Moore. 2020. "Patterning in Patient Referral to and Uptake of a National Exercise Referral Scheme (NERS) in Wales from 2008 to 2017: A Data Linkage Study" International Journal of Environmental Research and Public Health 17, no. 11: 3942. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17113942