Air Quality Variation in Wuhan, Daegu, and Tokyo during the Explosive Outbreak of COVID-19 and Its Health Effects


Abstract
:1. Introduction
2. Methods
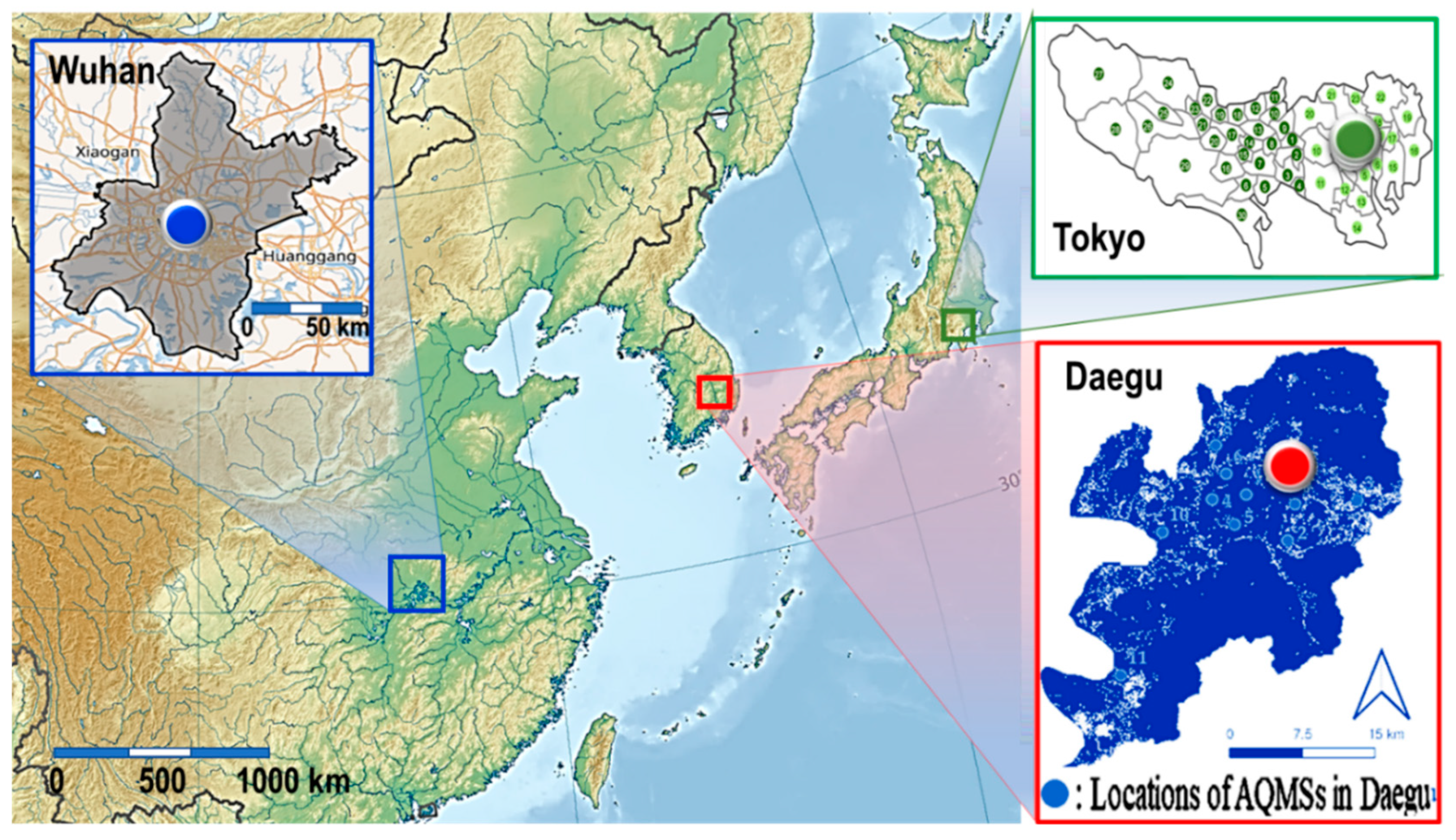
2.1. Sites Description
2.2. One-Hour Interval Measured Data and Those Sources
2.3. Data Handling
3. Results and Discussion
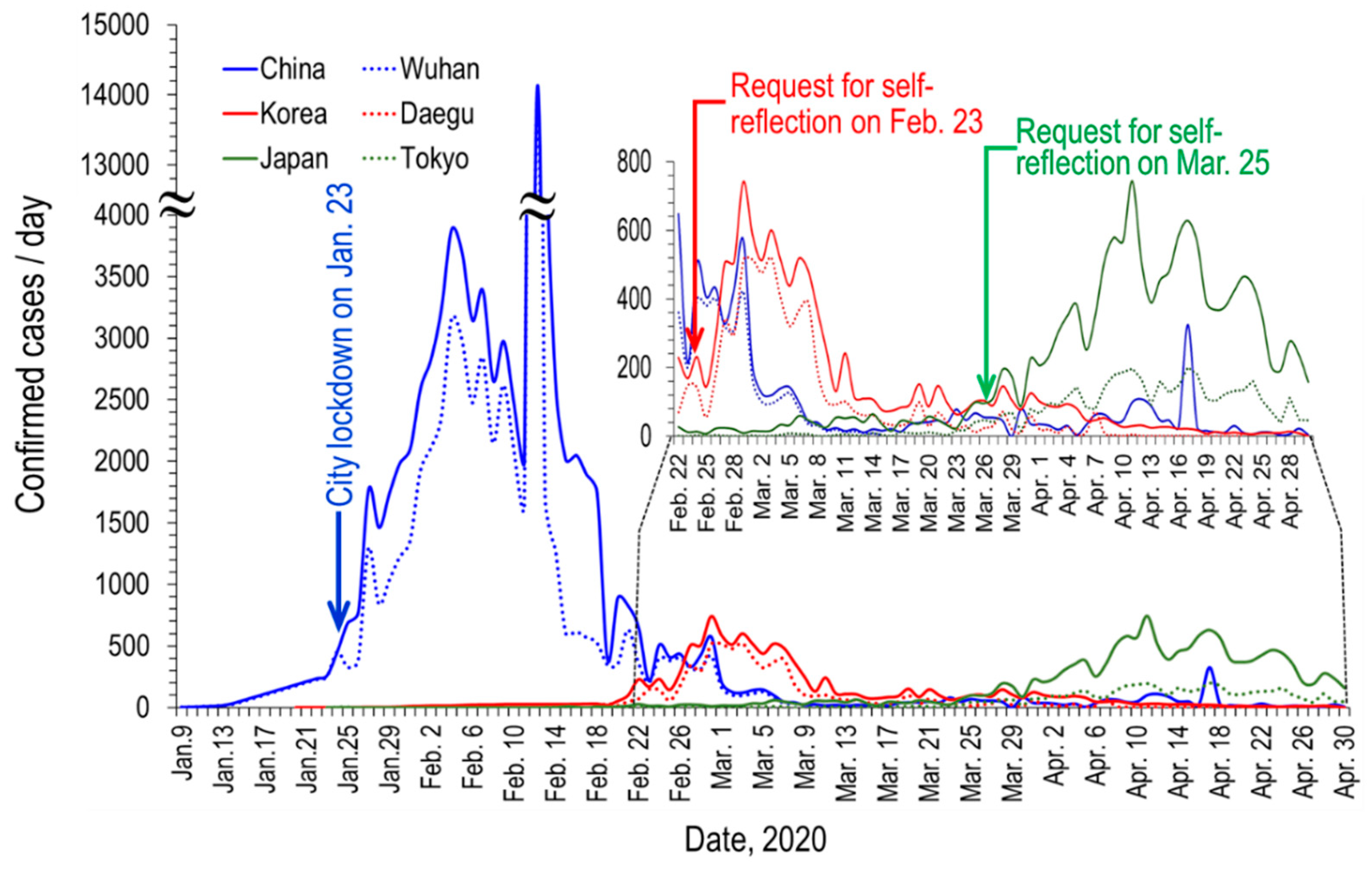
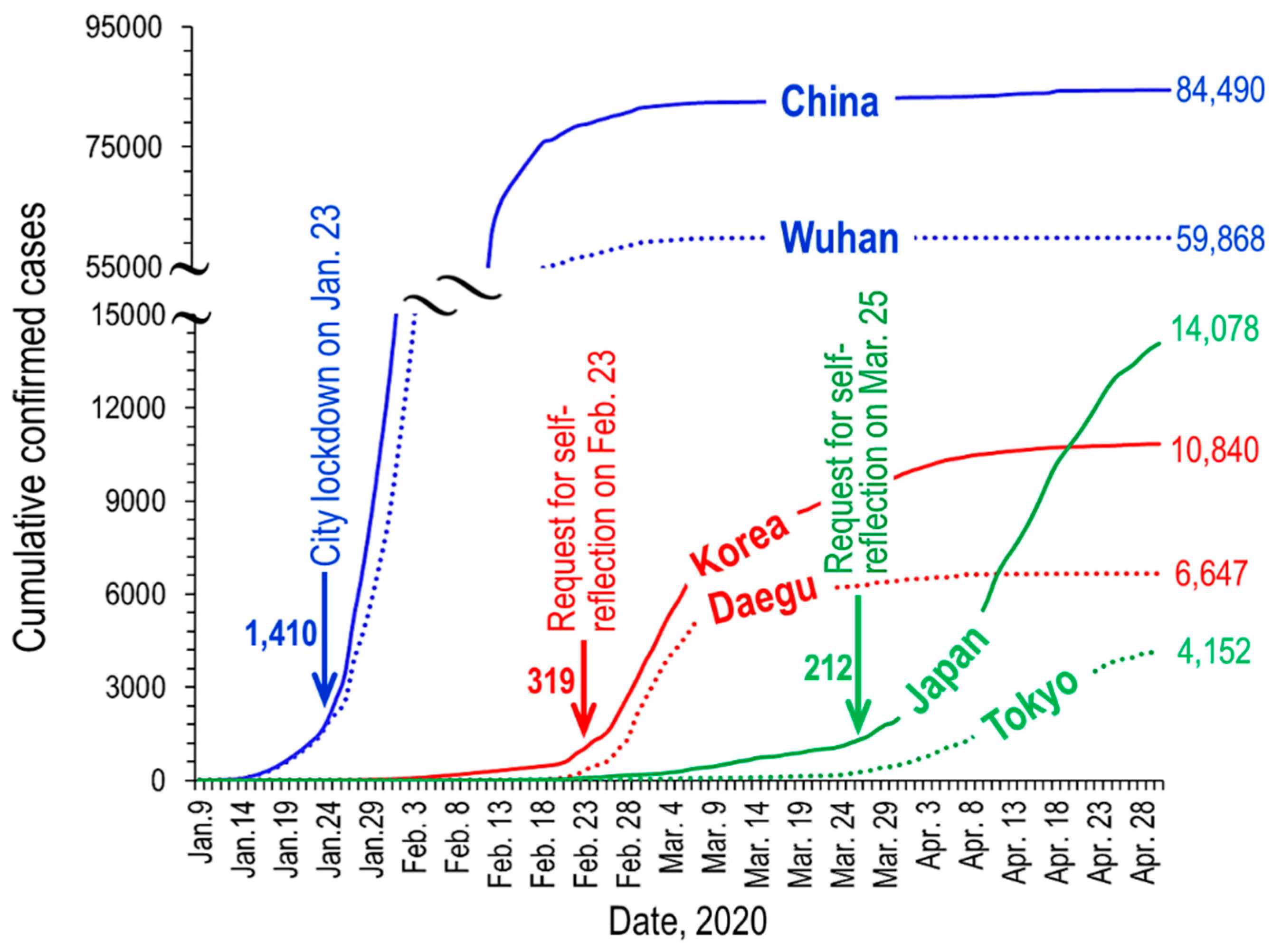
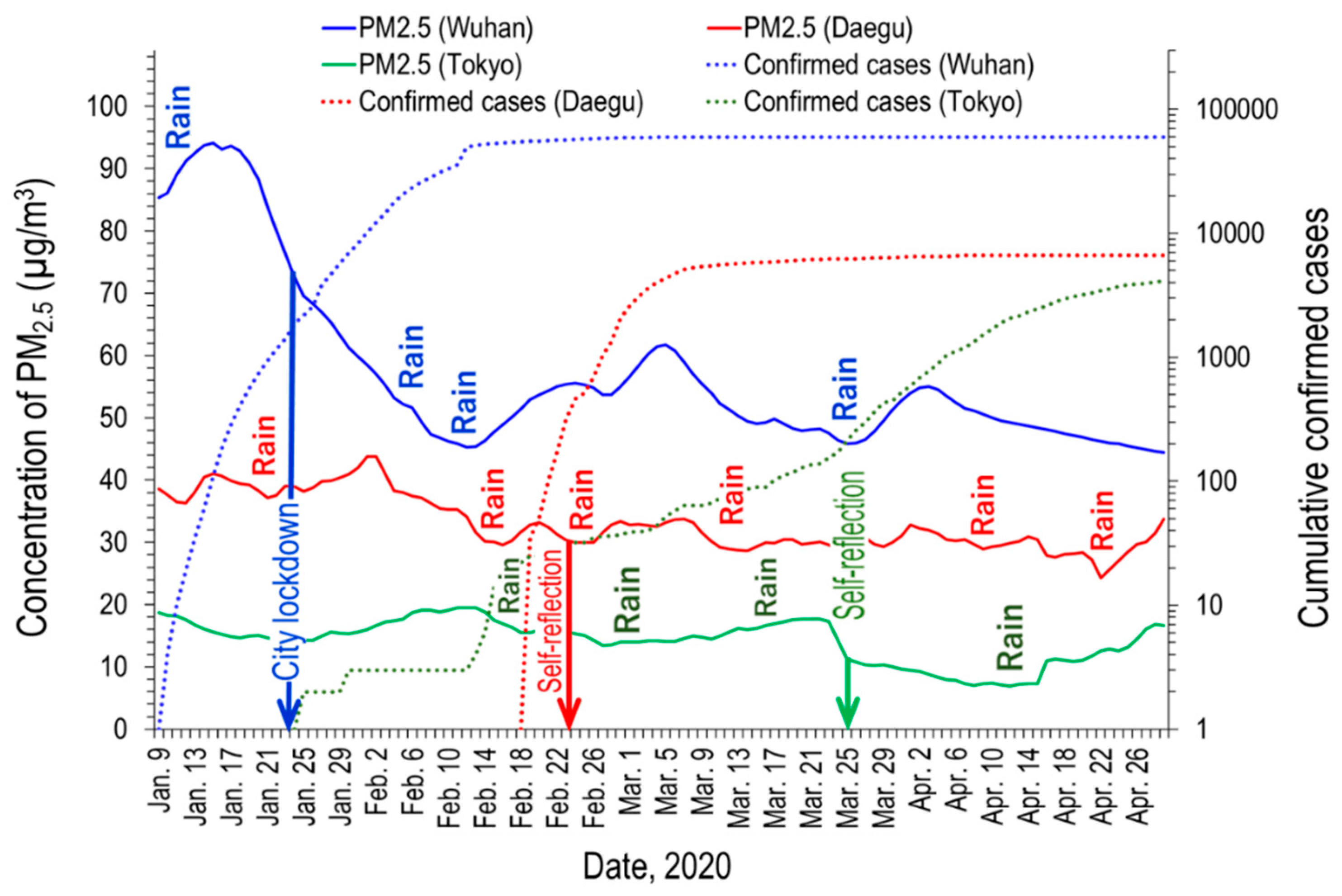
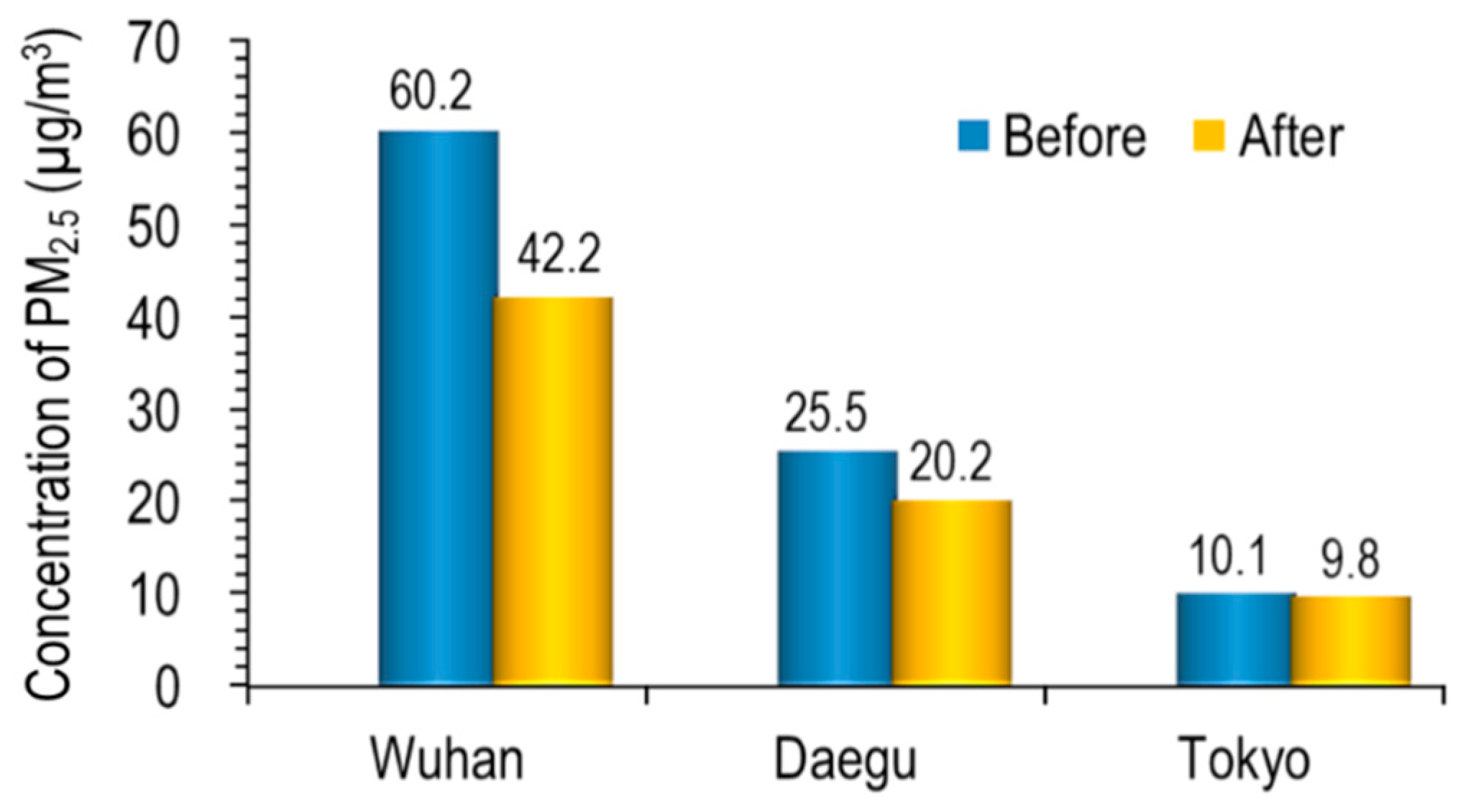
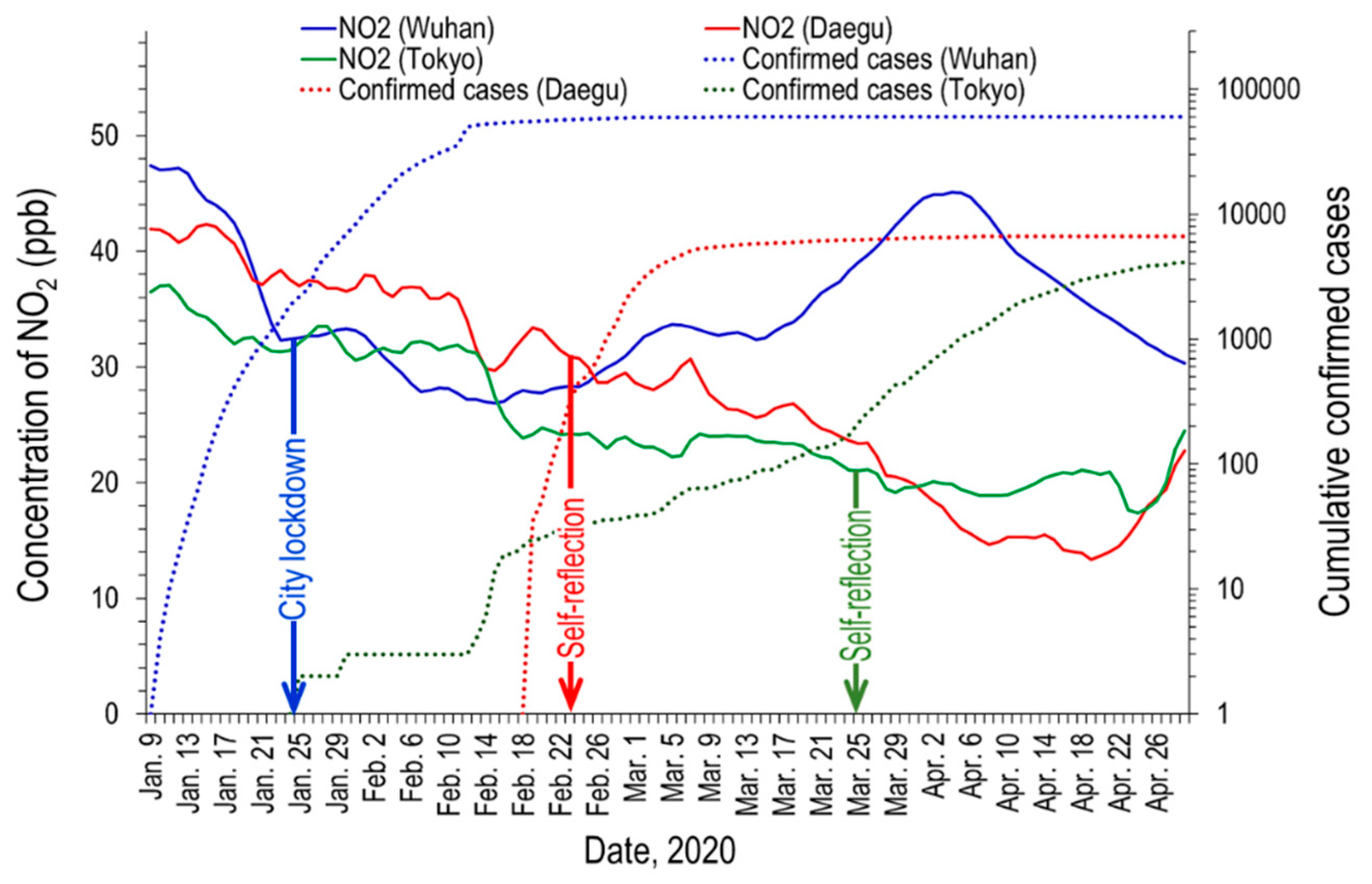
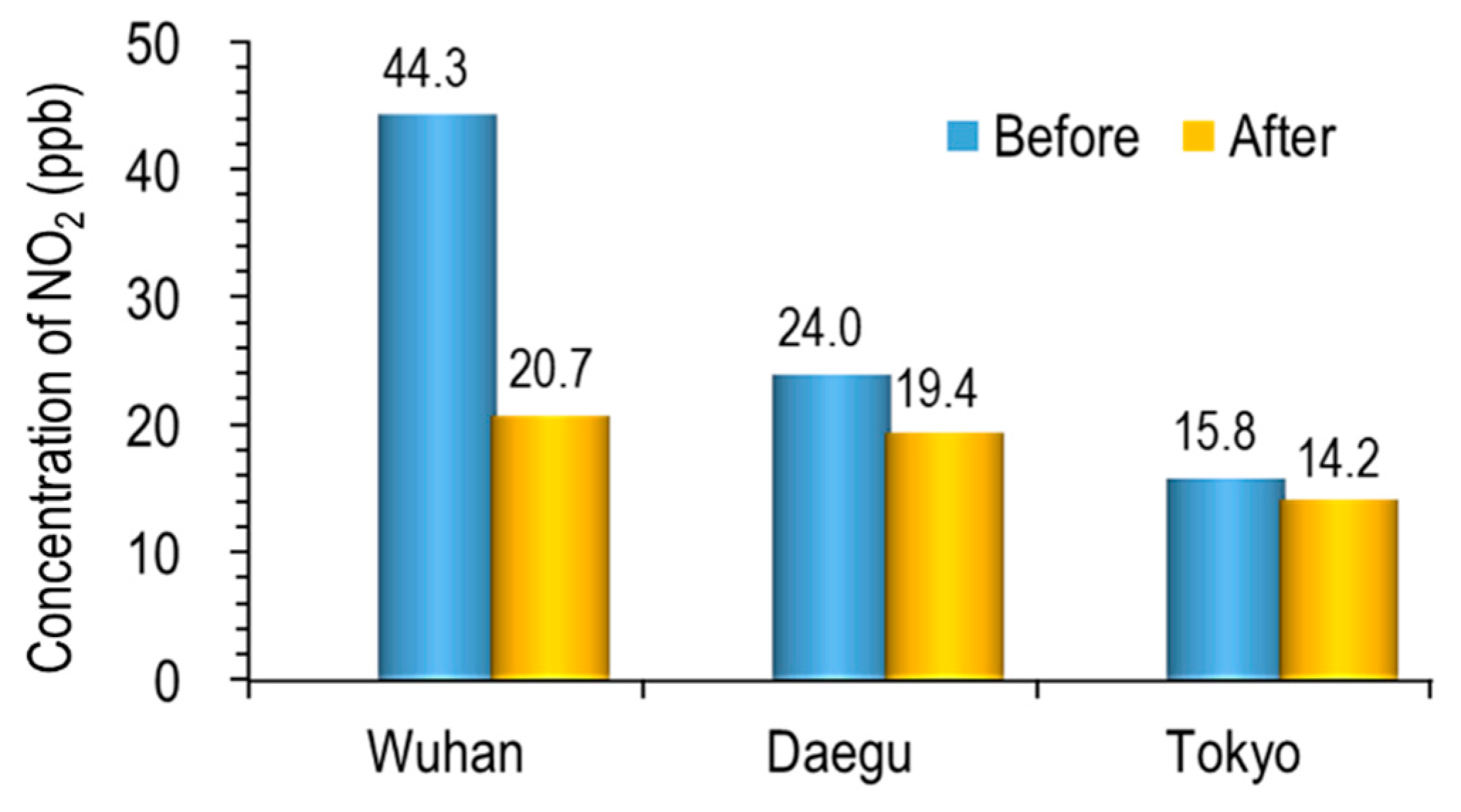
3.1. Variation of PM2.5 and NO2 Concentration with Confirmed Cases of COVID-19
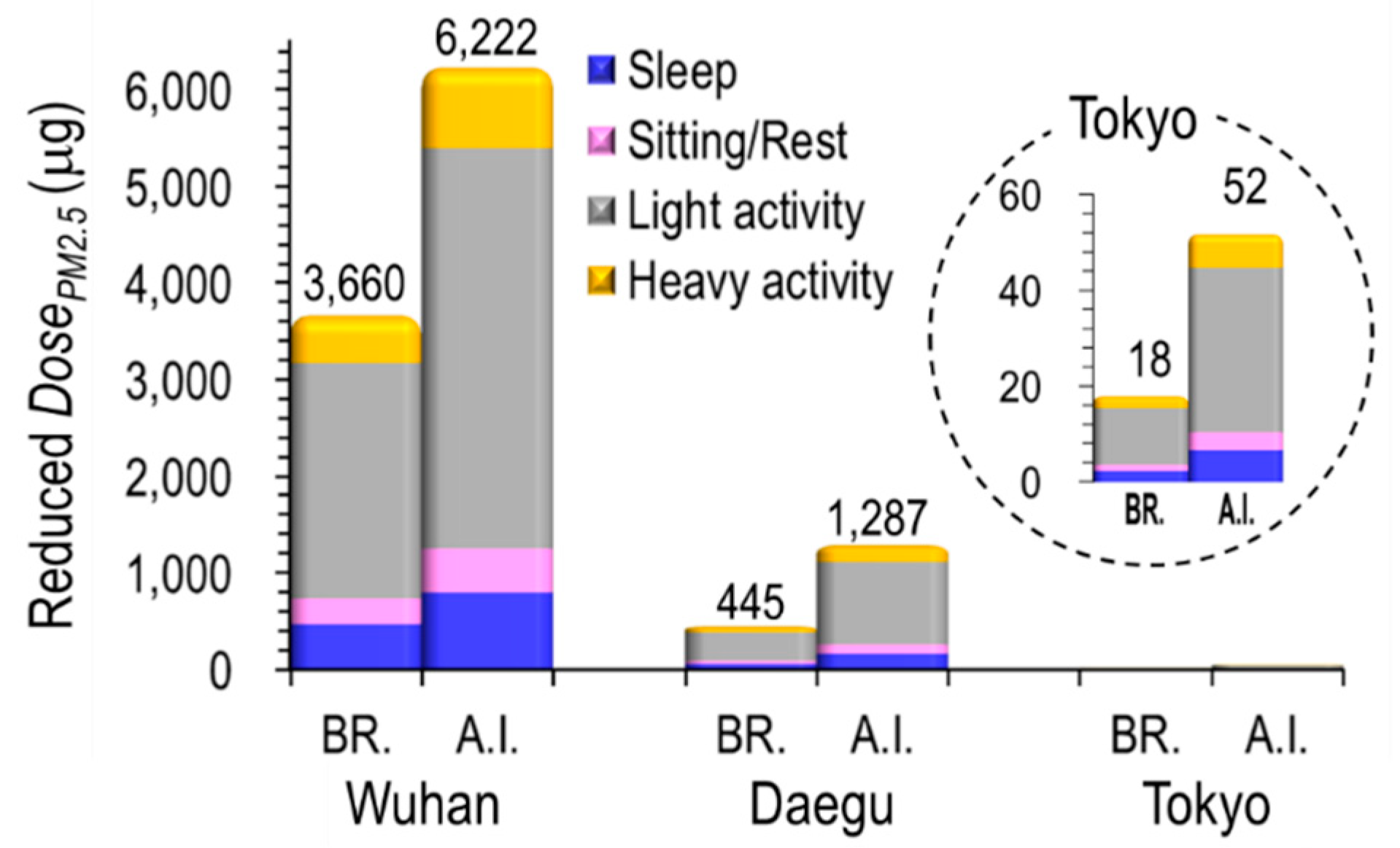
3.2. Exposure Assessment
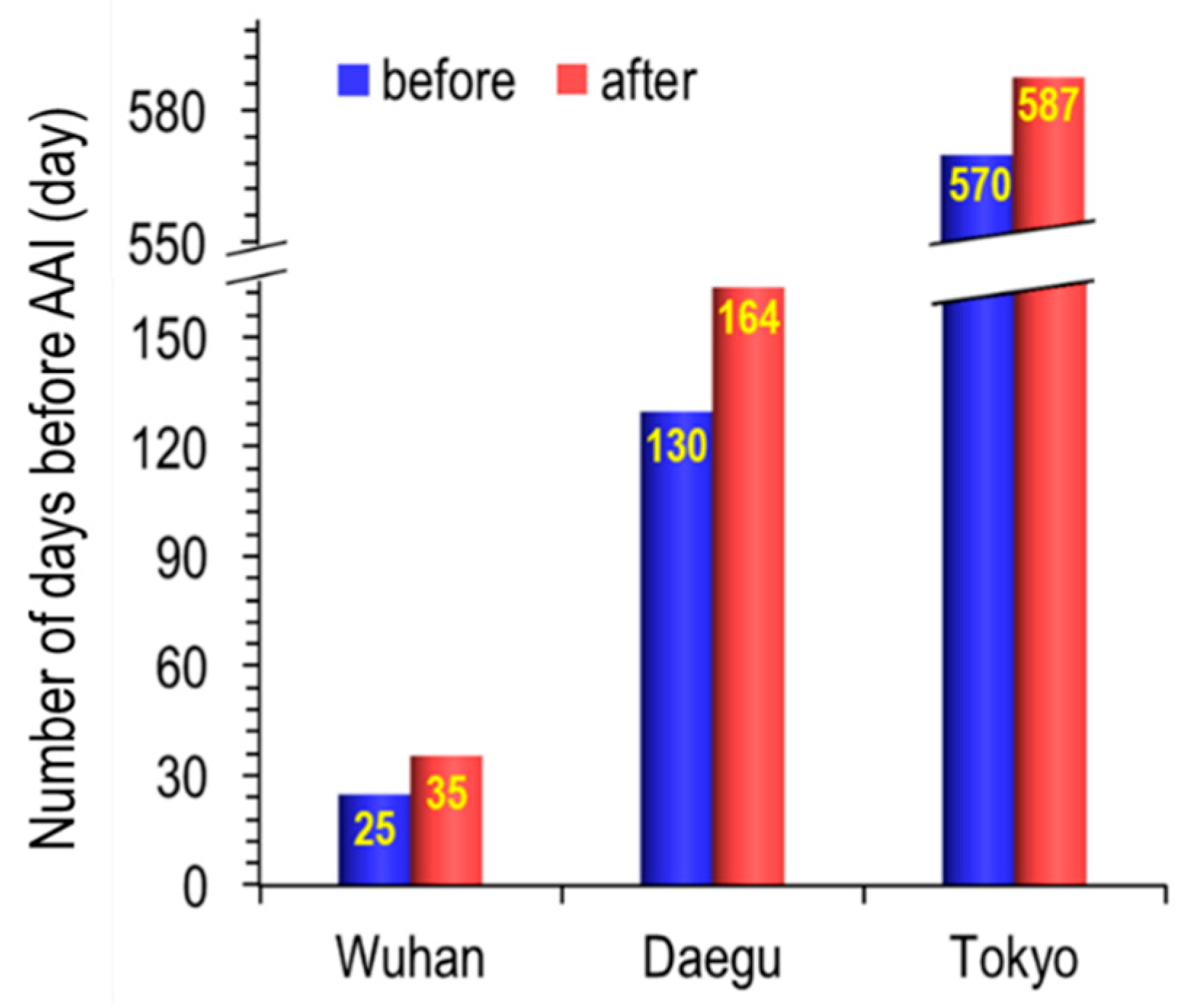
3.3. Airway Inflammation Delay Effect
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- COVID-19 Coronavirus/Death Toll: National Health Commission (NHC) of the People’s Republic of China. Available online: http://www.nhc.gov.cn/ (accessed on 11 May 2020).
- Wilder-Smith, A.; Freedman, D.O. Isolation, quarantine, social distancing and community containment: Pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J. Travel Med. 2020, 27, taaa020. [Google Scholar] [CrossRef] [PubMed]
- Kazuki OGIWARA: Toyo Keizai Online: Coronavirus Disease (COVID-19) Situation Report in Japan. Available online: https://toyokeizai.net/sp/visual/tko/covid19 /en.html. (accessed on 6 May 2020).
- NASA: Airborne Nitrogen Dioxide Plummets over China. Available online: https://earthobservatory.nasa.gov/images/146362/airborne-nitrogen-dioxide-plummets-over-china (accessed on 11 May 2020).
- Guterres, A. Air Pollution Kills 600,000 Children Each Year According to WHO, 2018. Available online: https://www.france24.com/en/20181029 (accessed on 10 May 2020).
- Brauer, M. How Much, How Long, What, and Where: Air Pollution Exposure Assessment for Epidemiologic Studies of Respiratory Disease. Proc. Am. Thorac. Soc. 2010, 7, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, C.; Linares, C.; Carmona, R.; Diaz, J. Evaluation of short-term mortality attributable to particulate matter pollution in Spain. Environ. Pollut. 2017, 224, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Barnes, N.M.; Ng, T.W.; Ma, K.K.; Lai, K.M. In-Cabin Air Quality during Driving and Engine Idling in Air-Conditioned Private Vehicles in Hong Kong. Int. J. Environ. Res. Public Heal. 2018, 15, 611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, A.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef] [Green Version]
- Song, J.; Guang, W.; Li, L.; Xiang, R.-B. Assessment of Air Quality Status in Wuhan, China. Atmosphere 2016, 7, 56. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Zhu, X.; Guo, W.; She, B.; Yue, H.; Li, M. Exploring the Weekly Travel Patterns of Private Vehicles Using Automatic Vehicle Identification Data: A Case Study of Wuhan, China. Sustainability 2019, 11, 6152. [Google Scholar] [CrossRef] [Green Version]
- Institute of Health and Environment of Daegu Metropolitan City. Report on the Results of Air Quality Analysis in March 2020. p. 2. Available online: http://air.daegu.go.kr/open_content/ko/page.do?mnu_uid=251& (accessed on 9 May 2020). (In Korean).
- Statistics Bureau: Ministry of Internal Affairs and Communications, 2020. Available online: https://www.stat.go. jp/data/jinsui/new.html (accessed on 9 May 2020).
- Automobiles Registered: Automobile Inspection & Registration Information Association, 2019. Available online: https://stats-japan.com/t/kiji/10786 (accessed on 14 May 2020).
- Ministry of Environmental Protection (MEP) in China, 2002. Available online: http://106. 37.208.233:20035. (accessed on 6 May 2020).
- Gong, W.; Zhang, T.; Zhu, Z.; Ma, Y.; Ma, X.; Wang, W. Characteristics of PM1.0, PM2.5, and PM10, and their relation to clack carbon in Wuhan, central China. Atmosphere 2015, 6, 1377–1387. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.; Wang, Y.; He, S.; Wu, Z. PM2.5/PM10 ratio prediction based on a long short-term memory neural network in Wuhan, China. Geosci. Model. Dev. 2020, 13, 1499–1511. [Google Scholar] [CrossRef] [Green Version]
- Xu, K.; Cui, K.; Young, L.-H.; Hsieh, Y.-K.; Wang, Y.-F.; Zhang, J.; Wan, S. Impact of the COVID-19 Event on Air Quality in Central China. Aerosol Air Qual. Res. 2020, 20, 915–929. [Google Scholar] [CrossRef] [Green Version]
- Dutheil, F.; Baker, J.S.; Navel, V. COVID-19 as a factor influencing air pollution? Environ. Pollut. 2020, 263, 114466. [Google Scholar] [CrossRef] [PubMed]
- Wagner, J.G.; Morishita, M.; Keeler, G.J.; Harkema, J.R. Divergent effects of urban particulate air pollution on allergic airway responses in experimental asthma: A comparison of field exposure studies. Environ. Health 2012, 11, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gauderman, W.J.; Avol, E.; Gilliland, F.; Vora, H.; Thomas, D.; Berhane, K.; McConnell, R.; Künzli, N.; Lurmann, F.; Rappaport, E.; et al. The Effect of Air Pollution on Lung Development from 10 to 18 Years of Age. N. Engl. J. Med. 2004, 351, 1057–1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, G.; Huang, J.; Xu, G.-Z.; Pan, X.; Qian, X.; Xu, J.; Zhao, Y.; Zhang, T.; Liu, Q.; Guo, X.; et al. The short term burden of ambient fine particulate matter on chronic obstructive pulmonary disease in Ningbo, China. Environ. Health 2017, 16, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, C.; Smallwood, M.D. All About Allergies, KidsHealth, 2016. Available online: https://kidshealth. org/en/parents/allergy.html (accessed on 2 May 2020).
- Löndahl, J.; Massling, A.; Pagels, J.; Swietlicki, E.; Vaclavik, E.; Loft, S. Size-Resolved Respiratory-Tract Deposition of Fine and Ultrafine Hydrophobic and Hygroscopic Aerosol Particles During Rest and Exercise. Inhal. Toxicol. 2007, 19, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Choi, D.H.; Kang, D.H. Indoor/Outdoor Relationships of Airborne Particles under Controlled Pressure Difference across the Building Envelope in Korean Multifamily Apartments. Sustainability 2018, 10, 4074. [Google Scholar] [CrossRef] [Green Version]
- Hu, J.; Li, N.; Yoshino, H.; Yanagi, U. Field Investigation of PM 2.5 in Schoolchildren’s Houses and Classrooms in Changsha, China. Procedia Eng. 2017, 205, 1433–1438. [Google Scholar] [CrossRef]
- Kagi, N. Situations and countermeasure for indoor PM2.5, 2014. Available online: www.kinki-shasej.org/upload/pdf/sinpo.pdf (accessed on 7 May 2020).
- Yamada, Y.; Fukutsu, K.; Kurihara, O.; Momose, T.; Miyabe, K.; Akashi, M. Influences of biometrical parameters on aerosol deposition in the ICRP 66 human respiratory tract model: Japanese and Caucasians. Aarozoru Kenkyu 2007, 22, 236–243. (in Japanese). [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Feng, G.; Du, Q.; Jin, X.; Du, X.-R. Fine particulate matter aggravates allergic airway inflammation through thymic stromal lymphopoietin activation in mice. Mol. Med. Rep. 2017, 16, 4201–4207. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.B.; Jacob, S. A simple practice guide for dose conversion between animals and human. J. Basic Clin. Pharm. 2016, 7, 27–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kouno, T.; Katsumata, N.; Mukai, H.; Ando, M.; Watanabe, T. Standardization of the body surface area (BSA) formula to calculate the dose of anticancer agents in Japan. Jpn. J. Clin. Oncol. 2003, 33, 309–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.-Y.; Choi, J.-W.; Kim, H. Determination of hand surface area by sex and body shape using alginate. J. Physiol. Anthr. 2007, 26, 475–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, C.-Y.; Lin, C.-H.; Yang, Y.-H. Human body surface area database and estimation formula. Burn. 2010, 36, 616–629. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Behavioral Patterns of 10- Year-Old Children in the Day | Activity Time (h) | Total Exposure Period (Texp., Day) | CPM2.5 (μg/m3) Reduced in 2020 | I/O Ratio | Fdep. | Rbre. (m3/h) | ||
|---|---|---|---|---|---|---|---|---|
| Br. | A.I. | |||||||
| Wuhan | Sleep | 9 | 60 | 18 | 0.94 | 0.209 | 0.355 | 0.246 |
| Sitting/Rest | 4 | 60 | 18 | 0.94 | 0.218 | 0.370 | 0.301 | |
| Light activity | 10 | 60 | 18 | 0.94 | 0.270 | 0.459 | 0.888 | |
| Heavy activity | 1 | 60 | 18 | 0.94 | 0.300 | 0.510 | 1.610 | |
| Daegu | Sleep | 9 | 60 | 5.3 | 0.66 | 0.123 | 0.355 | 0.246 |
| Sitting/Rest | 4 | 60 | 5.3 | 0.66 | 0.128 | 0.370 | 0.301 | |
| Light activity | 10 | 60 | 5.3 | 0.66 | 0.159 | 0.459 | 0.888 | |
| Heavy activity | 1 | 60 | 5.3 | 0.66 | 0.176 | 0.510 | 1.610 | |
| Tokyo | Sleep | 9 | 60 | 0.36 | 0.39 | 0.123 | 0.355 | 0.246 |
| Sitting/Rest | 4 | 60 | 0.36 | 0.39 | 0.128 | 0.370 | 0.301 | |
| Light activity | 10 | 60 | 0.36 | 0.39 | 0.159 | 0.459 | 0.888 | |
| Heavy activity | 1 | 60 | 0.36 | 0.39 | 0.176 | 0.510 | 1.610 | |
| Behavioral Patterns of 10- Year-Old Children in the Day | Activity Time (h) | Reduced DosePM2.5 (μg) at Br. | Reduced DosePM2.5 (μg) at A.I. | |||
|---|---|---|---|---|---|---|
| 1 Day | 2-Month | 1 Day | 2-Month | |||
| Wuhan | Sleep | 9 | 7.82 | 469 | 13 | 798 |
| Sitting/Rest | 4 | 4.43 | 266 | 8 | 452 | |
| Light activity | 10 | 40.57 | 2434 | 69 | 4138 | |
| Heavy activity | 1 | 8.17 | 490 | 14 | 834 | |
| Total reduced DosePM2.5 (μg) | 61 | 3660 | 104 | 6222 | ||
| Daegu | Sleep | 9 | 0.95 | 57 | 3 | 165 |
| Sitting/Rest | 4 | 0.54 | 32 | 2 | 93 | |
| Light activity | 10 | 4.93 | 296 | 14 | 855 | |
| Heavy activity | 1 | 0.99 | 60 | 3 | 172 | |
| Total reduced DosePM2.5 (μg) | 7 | 445 | 21 | 1286 | ||
| Tokyo | Sleep | 9 | 0.04 | 2.3 | 0.1 | 7 |
| Sitting/Rest | 4 | 0.02 | 1.3 | 0.1 | 4 | |
| Light activity | 10 | 0.20 | 11.9 | 0.6 | 34 | |
| Heavy activity | 1 | 0.04 | 2.4 | 0.1 | 7 | |
| Total reduced DosePM2.5 (μg) | 0.30 | 17.9 | 0.9 | 52 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, C.-J.; Kang, G.-U. Air Quality Variation in Wuhan, Daegu, and Tokyo during the Explosive Outbreak of COVID-19 and Its Health Effects. Int. J. Environ. Res. Public Health 2020, 17, 4119. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114119
Ma C-J, Kang G-U. Air Quality Variation in Wuhan, Daegu, and Tokyo during the Explosive Outbreak of COVID-19 and Its Health Effects. International Journal of Environmental Research and Public Health. 2020; 17(11):4119. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114119
Chicago/Turabian StyleMa, Chang-Jin, and Gong-Unn Kang. 2020. "Air Quality Variation in Wuhan, Daegu, and Tokyo during the Explosive Outbreak of COVID-19 and Its Health Effects" International Journal of Environmental Research and Public Health 17, no. 11: 4119. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17114119