Large Gender Gap in Oral Hygiene Behavior and Its Impact on Gingival Health in Late Adolescence


Abstract
:1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Questionnaire
2.3. Statistical Analyses
2.4. Ethical Approval
3. Results
3.1. Gender Difference for the Frequency of Daily Brushing in Late Adolescents
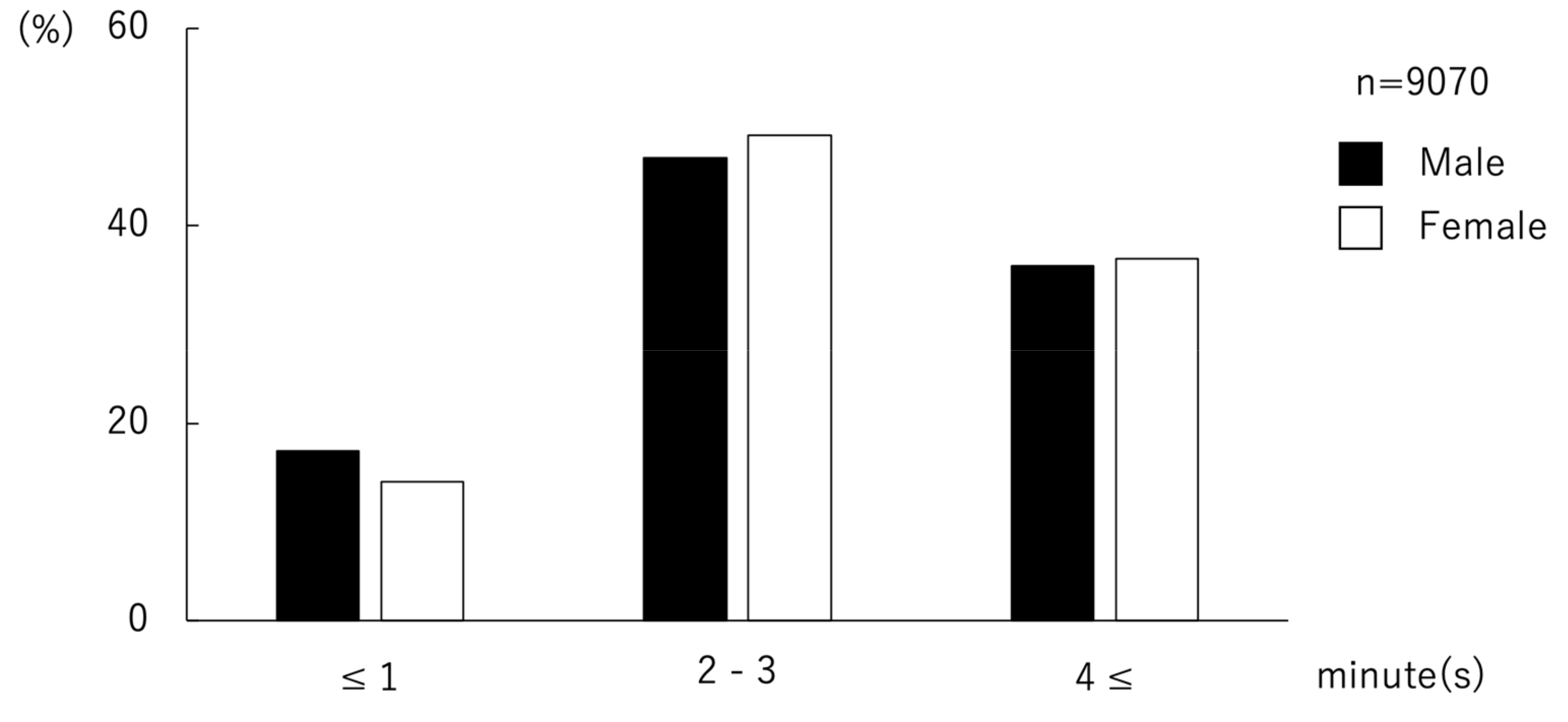
3.2. Gender Difference for the Duration of Brushing Each Time in Late Adolescents
3.3. The Association of Gingival Bleeding with Gender and Oral Hygiene Behavior
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Declarations
References
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef] [Green Version]
- Moreillon, P.; Que, Y.A. Infective endocarditis. Lancet 2004, 363, 139–149. [Google Scholar] [CrossRef]
- Kaur, S.; White, S.; Bartold, P.M. Periodontal disease and rheumatoid arthritis: A systematic review. J. Dent. Res. 2013, 92, 399–408. [Google Scholar] [CrossRef]
- Scannapieco, F.A.; Cantos, A. Oral inflammation and infection, and chronic medical diseases: Implications for the elderly. Periodontol. 2000 2016, 72, 153–175. [Google Scholar] [CrossRef] [PubMed]
- Lamster, I.B.; Pagan, M. Periodontal disease and the metabolic syndrome. Int. Dent. J. 2016, 67, 67–77. [Google Scholar] [CrossRef]
- Han, Y.W.; Wang, X. Mobile microbiome: Oral bacteria in extra-oral infections and inflammation. J. Dent. Res. 2013, 92, 485–491. [Google Scholar] [CrossRef] [Green Version]
- Abe, M.; Abe, T.; Mogi, R.; Kamimoto, H.; Hatano, N.; Taniguchi, A.; Saijo, H.; Hoshi, K.; Takato, T. Cervical necrotizing fasciitis of odontogenic origin in a healthy young patient without pre-systemic disorders. J. Oral Maxillofac. Surg. Med. Pathol. 2017, 29, 341–344. [Google Scholar] [CrossRef]
- Abe, M.; Mori, Y.; Inaki, R.; Ohata, Y.; Abe, T.; Saijo, H.; Ohkubo, K.; Hoshi, K.; Takato, T. A Case of Odontogenic Infection by Streptococcus constellatus Leading to Systemic Infection in a Cogan’s Syndrome Patient. Case Rep. Dent. 2014, 2014, 793174. [Google Scholar]
- Abe, M.; Mori, Y.; Saijo, H.; Hoshi, K.; Ohkubo, K.; Ono, T.; Takato, T. The efficacy of dental therapy for an adult case of Henoch-Schönlein Purpura. Oral Sci. Int. 2012, 9, 59–62. [Google Scholar] [CrossRef] [Green Version]
- Inagaki, Y.; Abe, M.; Inaki, R.; Zong, L.; Suenaga, H.; Abe, T.; Hoshi, K. A Case of Systemic Infection Caused by Streptococcus pyogenes Oral Infection in an Edentulous Patient. Diseases 2017, 5, 17. [Google Scholar] [CrossRef] [Green Version]
- Inaki, R.; Igarashi, M.; Abe, M.; Saijo, H.; Hoshi, K.; Takato, T. A case of infective endocarditis by Streptococcus mutans bacteremia induced by asymptomatic chronic dental caries in a wisdom tooth. Oral Sci. Jpn. 2014, 9, 95–96. [Google Scholar]
- Abe, M.; Mitani, A.; Yao, A.; Takeshima, H.; Zong, L.; Hoshi, K.; Yanagimoto, S. Close Associations of Gum Bleeding with Systemic Diseases in Late Adolescence. Int. J. Environ. Res. Public Health. 2020, 4290. [Google Scholar] [CrossRef]
- Shiau, H.J.; Reynolds, M.A. Sex differences in destructive periodontal disease: A systematic review. J. Periodontol. 2010, 81, 1379–1389. [Google Scholar] [CrossRef]
- Shiau, H.J.; Reynolds, M.A. Sex differences in destructive periodontal disease: Exploring the biologic basis. J. Periodontol. 2010, 81, 1505–1517. [Google Scholar] [CrossRef] [PubMed]
- Pawlaczyk-Kamienska, T.; Torlinska-Walkowiak, N.; Borysewicz-Lewicka, M. The relationship between oral hygiene level and gingivitis in children. Adv. Clin. Exp. Med. Off. Organ. Wroc. Med. Univ. 2018, 27, 1397–1401. [Google Scholar] [CrossRef]
- Olczak-Kowalczyk, D.; Gozdowski, D.; Kaczmarek, U. Oral Health in Polish Fifteen-year-old Adolescents. Oral Health Prev. Dent. 2019, 17, 139–146. [Google Scholar]
- Mizutani, S.; Ekuni, D.; Furuta, M.; Tomofuji, T.; Irie, K.; Azuma, T.; Kojima, A.; Nagase, J.; Iwasaki, Y.; Morita, M. Effects of self-efficacy on oral health behaviours and gingival health in university students aged 18- or 19-years-old. J. Clin. Periodontol. 2012, 39, 844–849. [Google Scholar] [CrossRef]
- Hikiji, H.; Koshikiya, N.; Fujihara, H.; Hatano, N.; Matsuzaki, M.; Matsuzaki, A.; Ohki, M.; Susami, T.; Takato, T.; Toyo-oka, T. Changes in the awareness of oral health among new students newly enrolled at the University of Tokyo over the past 15 years. Int. J. Dent. Hyg. 2005, 3, 137–144. [Google Scholar] [CrossRef]
- Zimmermann, H.; Zimmermann, N.; Hagenfeld, D.; Veile, A.; Kim, T.S.; Becher, H. Is frequency of tooth brushing a risk factor for periodontitis? A systematic review and meta-analysis. Community Dent. Oral Epidemiol. 2015, 43, 116–127. [Google Scholar] [CrossRef]
- Lertpimonchai, A.; Rattanasiri, S.; Arj-Ong Vallibhakara, S.; Attia, J.; Thakkinstian, A. The association between oral hygiene and periodontitis: A systematic review and meta-analysis. Int. Dent. J. 2017, 67, 332–343. [Google Scholar] [CrossRef] [Green Version]
- Si, Y.; Fan, H.; Song, Y.; Zhou, X.; Zhang, J.; Wang, Z. Association between periodontitis and chronic obstructive pulmonary disease in a Chinese population. J. Periodontol. 2012, 83, 1288–1296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Aiuto, F.; Gkranias, N.; Bhowruth, D.; Khan, T.; Orlandi, M.; Suvan, J.; Masi, S.; Tsakos, G.; Hurel, S.; Hingorani, A.D.; et al. Systemic effects of periodontitis treatment in patients with type 2 diabetes: A 12 month, single-centre, investigator-masked, randomised trial. Lancet Diabetes Endocrinol. 2018, 6, 954–965. [Google Scholar] [CrossRef]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreno, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Watt, R.G.; Daly, B.; Allison, P.; Macpherson, L.M.D.; Venturelli, R.; Listl, S.; Weyant, R.J.; Mathur, M.R.; Guarnizo-Herreno, C.C.; Celeste, R.K.; et al. Ending the neglect of global oral health: Time for radical action. Lancet 2019, 394, 261–272. [Google Scholar] [CrossRef]
- Dubar, M.; Delatre, V.; Moutier, C.; Sy, K.; Agossa, K. Awareness and practices of general practitioners towards the oral-systemic disease relationship: A regionwide survey in France. J. Eval. Clin. Pract. in press. [CrossRef] [PubMed]
- Almas, K.; Al-Hawish, A.; Al-Khamis, W. Oral hygiene practices, smoking habit, and self-perceived oral malodor among dental students. J. Contemp Dent. Pr. 2003, 4, 77–90. [Google Scholar] [CrossRef]
- Górska, R.; Górski, B. Self-reported Oral Status and Habits Related to Oral Care in Adult Poles: A Questionnaire Study. Dent. Med. Probl. 2018, 55, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Abe, M.; Tsai, S.Y.; Jin, S.G.; Pfeifer, G.P.; Szabo, P.E. Sex-specific dynamics of global chromatin changes in fetal mouse germ cells. PLoS ONE 2011, 6, e23848. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.; Woo, H.G.; Park, J.; Lee, J.S.; Song, T.J. Improved oral hygiene care is associated with decreased risk of occurrence for atrial fibrillation and heart failure: A nationwide population-based cohort study. Eur. J. Prev. Cardiol. in press. [CrossRef]



{kind=link}
{kind=link}
| Frequency of Daily Brushing | All (n = 9072) | Male (n = 7294) | Female (n = 1778) | p |
|---|---|---|---|---|
| Time (s) | n (%) | n (%) | n (%) | |
| ≤1 | 1868 (20.6) | 1669 (22.9) | 199 (11.2) | <0.001 * |
| 2 | 5971 (65.8) | 4741 (65.0) | 1230 (69.2) | |
| 3≤ | 1233 (13.6) | 884 (12.1) | 349 (19.6) |
| Duration of Brushing | All (n = 9070) | Male (n = 7293) | Female (n = 1777) | p |
|---|---|---|---|---|
| min | n (%) | n (%) | n (%) | |
| ≤1 | 1508 (16.6) | 1258 (17.2) | 250 (14.1) | 0.005 * |
| 2–3 | 4291 (47.3) | 3417 (46.9) | 874 (49.2) | |
| 4≤ | 3271 (36.1) | 2618 (35.9) | 653 (36.7) |
| n | Gingival Bleeding | p | ||
|---|---|---|---|---|
| Presence | Absence | |||
| n (%) | n (%) | |||
| All | 9098 | 3321 (36.5) | 5777 (63.5) | |
| Gender | ||||
| Male | 7316 | 2780 (38.0) | 4536 (62.0) | <0.001 * |
| Female | 1782 | 541 (30.4) | 1241 (69.6) | |
| Frequency of daily brushing (times) | ||||
| ≤1 | 1868 | 881 (47.2) | 987 (52.8) | <0.001 * |
| 2 | 5971 | 2108 (35.3) | 3863 (64.7) | |
| 3≤ | 1233 | 331 (26.8) | 902 (73.2) | |
| Duration of brushing (min) | ||||
| ≤1 | 1508 | 653 (43.3) | 855 (56.7) | <0.001 * |
| 2–3 | 4291 | 1593 (37.1) | 2698 (62.9) | |
| 4≤ | 3271 | 1073 (32.8) | 2198 (67.2) | |
| Odds Ratio (95% CI) | p | |
|---|---|---|
| Gender | ||
| Male | 1.29 (1.15–1.44) | <0.001 * |
| Female | 1 | – |
| Frequency of daily brushing (times) | ||
| ≤1 | 2.36 (2.02–2.76) | <0.001 * |
| 2 | 1.45 (1.27–1.67) | <0.001 * |
| 3≤ | 1 | – |
| Duration of brushing (min) | ||
| ≤1 | 1.57 (1.39–1.78) | <0.001 * |
| 2–3 | 1.26 (1.14–1.39) | <0.001 * |
| 4≤ | 1 | – |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abe, M.; Mitani, A.; Hoshi, K.; Yanagimoto, S. Large Gender Gap in Oral Hygiene Behavior and Its Impact on Gingival Health in Late Adolescence. Int. J. Environ. Res. Public Health 2020, 17, 4394. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124394
Abe M, Mitani A, Hoshi K, Yanagimoto S. Large Gender Gap in Oral Hygiene Behavior and Its Impact on Gingival Health in Late Adolescence. International Journal of Environmental Research and Public Health. 2020; 17(12):4394. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124394
Chicago/Turabian StyleAbe, Masanobu, Akihisa Mitani, Kazuto Hoshi, and Shintaro Yanagimoto. 2020. "Large Gender Gap in Oral Hygiene Behavior and Its Impact on Gingival Health in Late Adolescence" International Journal of Environmental Research and Public Health 17, no. 12: 4394. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17124394