Cumulative Exposure to Adverse Childhood Experience: Depressive Symptoms, Suicide Intensions and Suicide Plans among Senior High School Students in Nanchang City of China

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Exposure Variable
2.3.1. Adverse Childhood Experiences
2.3.2. Covariates
2.4. Outcome Variable
2.4.1. Depressive Symptoms
2.4.2. Suicide Intensions
2.4.3. Suicide Plans
2.5. Analyses
2.6. Ethics Statement
3. Results
3.1. Describe Sociodemographic Characteristics and Adverse Childhood Experience of Sample
3.2. Describe the Incidence rate of Depressive Symptoms, Suicide Intentions and Suicide Plans
3.3. Associations of Adverse Childhood Experience and Depressive Symptoms, SUICIDE intensions, Suicide Plans
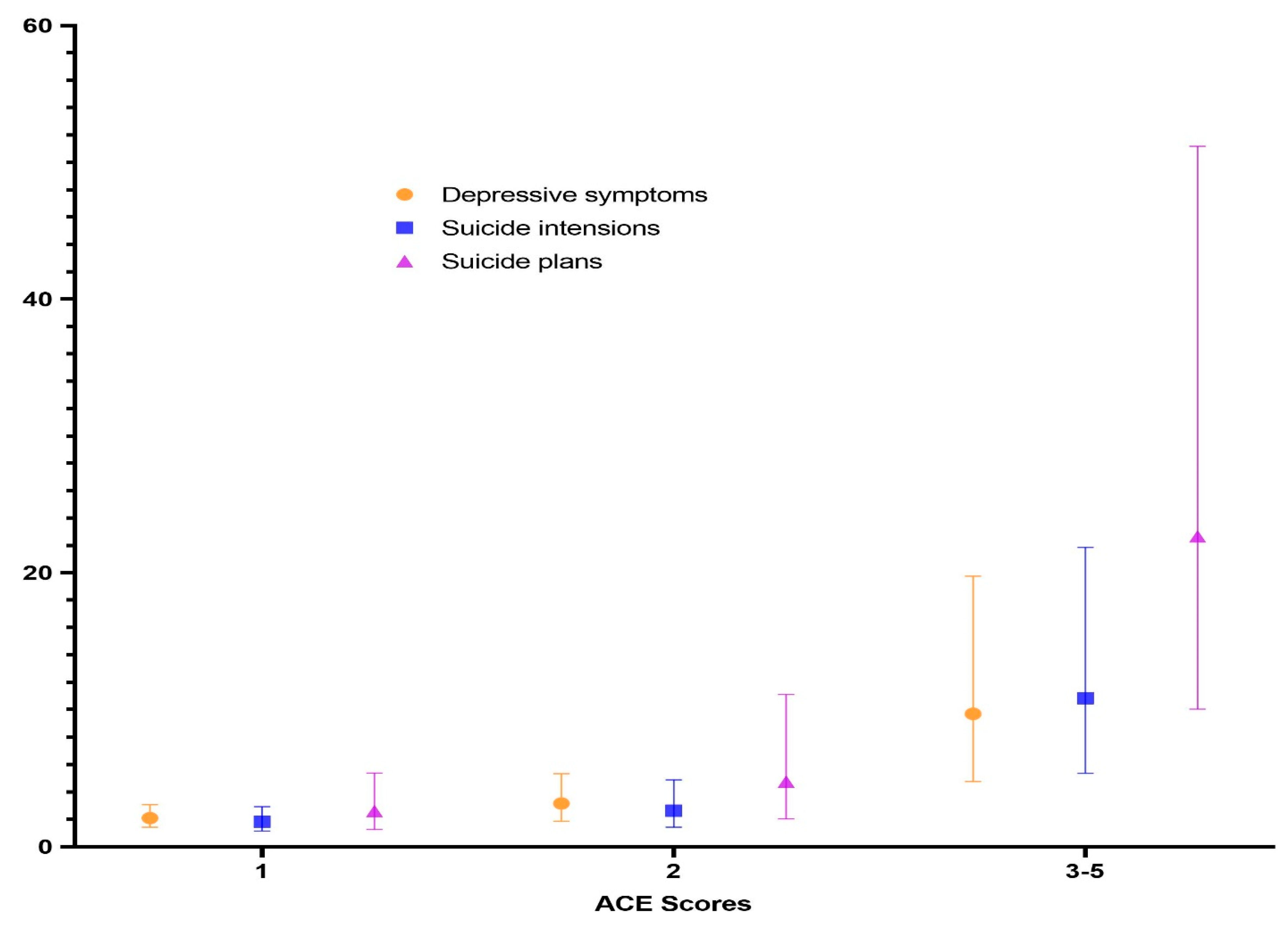
3.4. Associations of ACE Score and Depressive Symptoms, Suicide Intensions, Suicide Plans
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Boullier, M.; Blair, M. Adverse childhood experiences. Paediatr. Child Health 2018, 28, 132–137. [Google Scholar] [CrossRef]
- Turney, K. Adverse childhood experiences among children of incarcerated parents. Child. Youth Serv. Rev. 2018, 89, 218–225. [Google Scholar] [CrossRef]
- Vincent, J.; Felitti, R.F.A.; Nordenberg, D.; David, F.; Williamson, A.M.; Spitz, V.E.; Mary, P.; Koss, J.; Marks, S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults-the adverse childhood experiences (ace) study. Am. J. Prev. Med. 1998, 14, 13. [Google Scholar]
- Bjorkenstam, E.; Bjorkenstam, C.; Jablonska, B.; Kosidou, K. Cumulative exposure to childhood adversity, and treated attention deficit/hyperactivity disorder: A cohort study of 543,650 adolescents and young adults in sweden. Psychol. Med. 2018, 48, 498–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zatti, C.; Rosa, V.; Barros, A.; Valdivia, L.; Calegaro, V.C.; Freitas, L.H.; Cereser, K.M.M.; da Rocha, N.S.; Bastos, A.G.; Schuch, F.B. Childhood trauma and suicide attempt: A meta-analysis of longitudinal studies from the last decade. Psychiatry Res. 2017, 256, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Angst, J.; Hengartner, M.P.; Rogers, J.; Schnyder, U.; Steinhausen, H.C.; Ajdacic-Gross, V.; Rossler, W. Suicidality in the prospective zurich study: Prevalence, risk factors and gender. Eur. Arch. Psychiatry Clin. Neurosci. 2014, 264, 557–565. [Google Scholar] [CrossRef] [Green Version]
- Anda, R.F.; Croft, J.B.; Felitti, V.J.; Nordenberg, D.; Giles, W.H.; Williamson, D.F.; Giovino, G.A. Adverse childhood experiences and smoking during adolescence and adulthood. JAMA J. Am. Med. Assoc. 1999, 282, 1652–1658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, P.-Y.; Han, A.Z.; Wang, G.-F.; Wang, L.-H.; Zhang, G.-B.; Xu, N.; Xu, G. Is childhood maltreatment associated with murderous ideation and behaviors in adolescents in China? Psychiatry Res. 2018, 270, 467–473. [Google Scholar] [CrossRef]
- Holshausen, K.; Bowie, C.R.; Harkness, K.L. The relation of childhood maltreatment to psychotic symptoms in adolescents and young adults with depression. J. Clin. Child. Adolesc. Psychol. 2016, 45, 241–247. [Google Scholar] [CrossRef]
- Afifi, T.O.; Taillieu, T.; Zamorski, M.A.; Turner, S.; Cheung, K.; Sareen, J. Association of child abuse exposure with suicidal ideation, suicide plans, and suicide attempts in military personnel and the general population in Canada. JAMA Psychiatry 2016, 73, 229–238. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.J.; Tabet, M.; Elder, K.; Kiel, D.W.; Flick, L.H. Racial/ethnic differences in the correlates of mental health services use among pregnant women with depressive symptoms. Matern. Child Health J. 2016, 20, 1911–1922. [Google Scholar] [CrossRef] [PubMed]
- Davis, L.; Barnes, A.J.; Gross, A.C.; Ryder, J.R.; Shlafer, R.J. Adverse childhood experiences and weight status among adolescents. J. Pediatr. 2019, 78, 124–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, K.; Finkelhor, D. A meta-analysis of child physical abuse prevalence in china. Child Abus. Negl. 2015, 43, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Fang, X.M.; Fry, D.A.; Ji, K.; Finkelhor, D.; Chen, J.Q.; Lannen, P.; Dunne, M.P. The burden of child maltreatment in China: A systematic review. Bull. World Health Organ. 2015, 93, 176C–185C. [Google Scholar] [CrossRef]
- Laura Kann, T.M.; William, A.; Harris Shari, L.; Shanklin, K.H.; Flint, B.; Queen, R.L.; Chyen, D. Youth risk behavior surveillance—United States, 2017. Morb. Mortal. Wkly. Rep. 2018, 67, 6–26. [Google Scholar]
- Liu, J.B.; Fang, Y.M.; Gong, J.B.; Cui, X.L.; Meng, T.T.; Xiao, B.; He, Y.Q.; Shen, Y.M.; Luo, X.R. Associations between suicidal behavior and childhood abuse and neglect: A meta-analysis. J. Affect. Disord. 2017, 220, 147–155. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, K.A.; Sheridan, M.A. Beyond cumulative risk: A dimensional approach to childhood adversity. Curr. Dir. Psychol. 2016, 25, 239–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, G.W.; Li, D.; Whipple, S.S. Cumulative risk and child development. Psychol. Bull. 2013, 139, 1342. [Google Scholar] [CrossRef] [Green Version]
- Merrick, M.T.; Ford, D.C.; Ports, K.A.; Guinn, A.S. Prevalence of adverse childhood experiences from the 2011–2014 behavioral risk factor surveillance system in 23 states. JAMA Pediatr. 2018, 172, 1038–1044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, D.E.; Holtzman, D.; Bolen, J.; Stanwyck, C.A.; Mack, K.A. Reliability and validity of measures from the behavioral risk factor surveillance system (brfss). Sozial- und Praventivmedizin. 2001, 46, S3–S42. [Google Scholar]
- Nelson, D.E.; Powell-Griner, E.; Town, M.; Kovar, M.G. A comparison of national estimates from the national health interview survey and the behavioral risk factor surveillance system. Am. J. Public Health 2003, 93, 1335–1341. [Google Scholar] [CrossRef] [PubMed]
- Vink, R.M.; van Dommelen, P.; van der Pal, S.M.; Eekhout, I.; Pannebakker, F.D.; Klein Velderman, M.; Haagmans, M.; Mulder, T.; Dekker, M. Self-Reported adverse childhood experiences and quality of life among children in the two last grades of dutch elementary education. Child Abus. Negl. 2019, 95, 104051. [Google Scholar] [CrossRef] [PubMed]
- Afifi, T.O.; Ford, D.; Gershoff, E.T.; Merrick, M.; Grogan-Kaylor, A.; Ports, K.A.; MacMillan, H.L.; Holden, G.W.; Taylor, C.A.; Lee, S.J.; et al. Spanking and adult mental health impairment: The case for the designation of spanking as an adverse childhood experience. Child Abus. Negl. 2017, 71, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.F.; Tang, S.Q.; Ren, Z.H.; Wong, D.F.K. Prevalence of depressive symptoms among adolescents in secondary school in mainland china: A systematic review and meta-analysis. J. Affect. Disord. 2019, 245, 498–507. [Google Scholar] [CrossRef]
- Bond, L.; Toumbourou, J.W.; Thomas, L.; Catalano, R.F.; Patton, G. Individual, family, school, and community risk and protective factors for depressive symptoms in adolescents: A comparison of risk profiles for substance use and depressive symptoms. Prev. Sci. 2005, 6, 73–88. [Google Scholar] [CrossRef]
- Murshid, N.S. Parents, friends, and depression: A multi-country study of adolescents in south Asia. Child. Youth Serv. Rev. 2017, 79, 160–165. [Google Scholar] [CrossRef]
- Liu, Y.; Lu, Z. Chinese high school students’ academic stress and depressive symptoms: Gender and school climate as moderators. Stress Health 2012, 28, 340–346. [Google Scholar] [CrossRef]
- Tepper, P.; Liu, X.; Guo, C.; Zhai, J.; Liu, T.; Li, C. Depressive symptoms in Chinese children and adolescents: Parent, teacher, and self reports. J. Affect. Disord. 2008, 111, 291–298. [Google Scholar] [CrossRef]
- Kinchin, I.; Doran, C.M. The cost of youth suicide in Australia. Int. J. Environ. Res. Public Health 2018, 15, 672. [Google Scholar] [CrossRef] [Green Version]
- Kyron, M.J.; Carrington-Jones, P.; Page, A.C.; Bartlett, J.; Lawrence, D. Factors differentiating adolescents who consider suicide and those who attempt: Results from a national survey of Australian adolescents. Aust. J. Psychol. 2020, 72, 145–155. [Google Scholar] [CrossRef]
- Dong, Y.H.; Liu, Y.; Liu, L.; He, W.; Peng, G.H.; Yin, Y.Z.; Chen, T.; Mo, X.Q. Reported rate of suicide-related behaviors among Chinese adolescents: A meta-analysis. Chin. J. Sch. Health 2014, 35, 532–536. [Google Scholar]
- Duan, C.R.; Lv, L.D.; Guo, J.; Wang, Z.P. Survival and development of left-behind children in rural china: Based on the analysis of sixth census data. Popul. J. 2013, 199, 37–49. [Google Scholar]
- Ge, Y.; Song, L.; Clancy, R.F.; Qin, Y.L. Studies on left-behind children in China: Reviewing paradigm shifts. In Child and Adolescent Development in China; Liu, Y., Grigorenko, E.L., Eds.; Wiley Periodicals: San Francisco, CA, USA, 2019; Volume 163, pp. 115–135. [Google Scholar]
- Fellmeth, G.; Rose-Clarke, K.; Zhao, C.Y.; Busert, L.K.; Zheng, Y.T.; Massazza, A.; Sonmez, H.; Eder, B.; Blewitt, A.; Lertgrai, W.; et al. Health impacts of parental migration on left-behind children and adolescents: A systematic review and meta-analysis. Lancet 2018, 392, 2567–2582. [Google Scholar] [CrossRef] [Green Version]
- Lu, R.; Zhou, Y.; Wu, Q.; Peng, X.; Dong, J.; Zhu, Z.; Xu, W. The effects of mindfulness training on suicide ideation among left-behind children in China: A randomized controlled trial. Child Care Health Dev. 2019, 45, 371–379. [Google Scholar] [CrossRef]
- Mark, A.; Bellis, K.H.; Leckenby, N.; Perkins, C.; Lowey, H. National household survey of adverse childhood experiences and their relationship with resilience to health-harming behaviors in England. BMC Med. 2014, 12, 72. [Google Scholar]
- Kerker, B.D.; Zhang, J.; Nadeem, E.; Stein, R.E.; Hurlburt, M.S.; Heneghan, A.; Landsverk, J.; McCue Horwitz, S. Adverse childhood experiences and mental health, chronic medical conditions, and development in young children. Acad. Pediatr. 2015, 15, 510–517. [Google Scholar] [CrossRef] [Green Version]
- Hunt, T.K.A.; Slack, K.S.; Berger, L.M. Adverse childhood experiences and behavioral problems in middle childhood. Child Abus. Negl. 2017, 67, 391–402. [Google Scholar] [CrossRef] [Green Version]
- Loria, H.; Caughy, M. Prevalence of adverse childhood experiences in low-income Latino immigrant and nonimmigrant children. J. Pediatr. 2018, 192, 209–215. [Google Scholar] [CrossRef]
- Garcia-Moreno, C. Violence against women—International perspectives. Am. J. Prev. Med. 2000, 19, 330–333. [Google Scholar] [CrossRef]
- Kremer, I.; Orbach, I.; Rosenbloom, T. Mental pain and suicidal tendencies in sexual and physical abuse victims. Arch. Suicide Res. 2017, 21, 307–321. [Google Scholar] [CrossRef]
- Adams, J.; Mrug, S.; Knight, D.C. Characteristics of child physical and sexual abuse as predictors of psychopathology. Child Abus. Negl. 2018, 86, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Nolen-Hoeksema, S. The role of rumination in depressive disorders and mixed anxiety/depressive symptoms. J.J Abnorm Psychol. 2000, 109, 504–511. [Google Scholar] [CrossRef]
- Easton, S.D.; Kong, J.; Gregas, M.C.; Shen, C.; Shafer, K. Child sexual abuse and depression in late life for men: A population-based, longitudinal analysis. J. Gerontol. B Psychol. Sci. Soc. Sci. 2019, 74, 842–852. [Google Scholar] [CrossRef]
- Stoltenborgh, M.; Bakermans-Kranenburg, M.J.; Alink, L.R.A.; van Ijzendoorn, M.H. The prevalence of child maltreatment across the globe: Review of a series of meta-analyses. Child Abus. Rev. 2015, 24, 37–50. [Google Scholar] [CrossRef]
- Anda, R.F.; Butchart, A.; Felitti, V.J.; Brown, D.W. Building a framework for global surveillance of the public health implications of adverse childhood experiences. Am. J. Prev. Med. 2010, 39, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Danese, A.; McEwen, B.S. Adverse childhood experiences, allostasis, allostatic load, and age-related disease. Physiol. Behav. 2012, 106, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Cicchetti, D. Annual research review: Resilient functioning in maltreated children—Past, present, and future perspectives. J. Child Psychol. Psychiatry 2013, 54, 402–422. [Google Scholar] [CrossRef]
- Bellis, M.A.; Lowey, H.; Leckenby, N.; Hughes, K.; Harrison, D. Adverse childhood experiences: Retrospective study to determine their impact on adult health behaviours and health outcomes in a UK population. J. Public Health 2014, 36, 81–91. [Google Scholar] [CrossRef] [Green Version]
- Gomis-Pomares, A.; Villanueva, L. The effect of adverse childhood experiences on deviant and altruistic behavior during emerging adulthood. Psicothema 2020, 32, 33–39. [Google Scholar]
- Merricka, M.T.; Ports, K.A.; Ford, D.C.; Afifi, T.O.; Gershoff, E.T.; Grogan-Kaylor, A. Unpacking the impact of adverse childhood experiences on adult mental health. Child Abus. Negl. 2017, 10, 19. [Google Scholar] [CrossRef]
- Krug, E.G.; Dahlberg, L.L.; Mercy, J.A.; Zwi, A.B. World Report on Violence and Health; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Haahr-Pedersen, I.; Perera, C.; Hyland, P.; Vallieres, F.; Murphy, D.; Hansen, M.; Spitz, P.; Hansen, P.; Cloitre, M. Females have more complex patterns of childhood adversity: Implications for mental, social, and emotional outcomes in adulthood. Eur. J. Psychotraumatol. 2020, 11, 1708618. [Google Scholar] [CrossRef]
- Meinck, F.; Cosma, A.P.; Mikton, C.; Baban, A. Psychometric properties of the adverse childhood experiences abuse short form (ace-asf) among romanian high school students. Child Abus. Negl. 2017, 72, 326–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finkelhor, D.; Shattuck, A.; Turner, H.; Hamby, S. Improving the adverse childhood experiences study scale. JAMA Pediatr. 2013, 167, 70–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balistreri, K.S. Adverse childhood experiences, the medical home, and child well-being. Matern. Child Health J. 2015, 19, 2492–2500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anda, R.F.; Whitfield, C.L.; Felitti, V.J.; Chapman, D.; Edwards, V.J.; Dube, S.R.; Williamson, D.F. Adverse, childhood experiences, alcoholic parents, an later risk of alcoholism and depression. Psychiatr. Serv. 2002, 53, 1001–1009. [Google Scholar] [CrossRef] [PubMed]
- Baglivio, M.T.; Epps, N. The interrelatedness of adverse childhood experiences among high-risk juvenile offenders. Youth Violence Juv. Justice 2015, 14, 179–198. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total (N = 884) | Depressive Symptoms n (%) | Suicide Intensions n (%) | Suicide Plans n (%) | p-Value |
|---|---|---|---|---|---|
| Sex | |||||
| Female | 475 (53.73) | 110 (23.16) | 70 (14.74) | 26 (5.47) | |
| Male | 409 (46.27) | 89 (21.76) | 55 (13.45) | 29 (7.09) | |
| Age (year) | |||||
| ≤15 | 128 (14.48) | 23 (17.97) | 13 (10.16) | 8 (6.25) | |
| 16 | 385 (43.55) | 93 (24.16) | 61 (15.84) | 21 (5.45) | |
| ≥17 | 371 (41.97) | 83 (22.37) | 51 (13.75) | 26 (7.01) | |
| School | |||||
| Key senior high school | 382 (43.21) | 100 (26.18) | 62 (16.23) | 30 (7.85) | A1 |
| General senior high school | 392 (44.35) | 72 (18.37) | 45 (11.48) | 16 (4.08) | |
| Art senior high school | 110 (12.44) | 27 (24.55) | 18 (16.36) | 9 (8.18) | |
| Sexual abuse | A2 B1 C3 | ||||
| No | 834 (94.34) | 179 (21.46) | 112 (13.43) | 43 (5.16) | |
| Yes | 50 (5.66) | 20 (40.00) | 37 (74.00) | 12 (24.00) | |
| Physical abuse | A3 B3 C3 | ||||
| No | 792 (89.59) | 155 (19.57) | 94 (11.87) | 35 (4.42) | |
| Yes | 92 (10.41) | 44 (47.83) | 31 (33.70) | 20 (21.74) | |
| Household domestic violence | A3 B3 C2 | ||||
| No | 694 (78.51) | 133 (19.16) | 83 (11.96) | 35 (5.04) | |
| Yes | 190 (21.49) | 66 (34.74) | 42 (22.11) | 20 (10.53) | |
| Household mental illness | A3 B3 C3 | ||||
| No | 788 (89.14) | 153 (19.42) | 91 (11.55) | 32 (4.06) | |
| Yes | 96 (10.86) | 46 (47.92) | 34 (35.42) | 23 (23.96) | |
| Household substance use/abuse | A3 B3 C3 | ||||
| No | 842 (95.25) | 180 (21.38) | 111 (13.18) | 43 (5.11) | |
| Yes | 42 (4.75) | 19 (45.24) | 14 (33.33) | 12 (28.57) | |
| ACE Score | A3 B3 C3 | ||||
| 0 | 582 (65.84) | 93 (15.98) | 57 (9.79) | 17 (2.92) | |
| 1 | 193 (21.83) | 55 (28.50) | 32 (16.58) | 14 (7.25) | |
| 2 | 72 (8.14) | 27 (37.50) | 16 (22.22) | 9 (12.50) | |
| 3–5 | 37 (4.19) | 24 (64.86) | 20 (54.05) | 15 (40.54) | |
| Total | 884 (100.00) | 199 (22.51) | 125 (14.14) | 55 (6.22) | – |
| Variables | Depressive Symptoms | Suicide Intensions | Suicide Plans | p-Value |
|---|---|---|---|---|
| Sex | ||||
| Female (ref) | 1 | 1 | 1 | |
| Male | 0.779 (0.553,1.097) | 0.743 (0.491,1.122) | 0.920 (0.493,1.715) | |
| Age | ||||
| ≤15 year (ref) | 1 | 1 | 1 | |
| 16 year | 1.607 (0.936,2.759) | 1.941 (0.989,3.807) | 0.956 (0.387,2.360) | |
| ≥17 year | 1.380 (0.798,2.386) | 1.489 (0.752,2.950) | 1.036 (0.425,2.522) | |
| School | ||||
| Key senior high school (ref) | 1 | 1 | 1 | |
| General senior high school | 0.719 (0.501,1.031) | 0.779 (0.504,1.202) | 0.607 (0.311,1.186) | |
| Art senior high school | 0.969 (0.574,1.637) | 1.065 (0.577,1.968) | 1.061 (0.448,2.516) | |
| Sexual abuse | ||||
| No (ref) | 1 | 1 | 1 | |
| Yes | 1.565 (0.802,3.054) | 1.334 (0.623,2.858) | 2.894 (1.210,6.924) | C1 |
| Physical abuse | ||||
| No (ref) | 1 | 1 | 1 | |
| Yes | 2.621 (1.603,4.285) | 2.723 (1.581,4.689) | 3.189 (1.549,6.567) | A3 B3 C2 |
| Household domestic violence | ||||
| No (ref) | 1 | 1 | 1 | |
| Yes | 1.530 (1.034,2.262) | 1.347 (0.849,2.136) | 0.974 (0.489,1.938) | A1 |
| Household mental illness | ||||
| No (ref) | 1 | 1 | 1 | |
| Yes | 2.789 (1.703,4.567) | 3.153 (1.839,5.404) | 4.288 (2.097,8.766) | A3 B3 C2 |
| Household substance use/abuse | ||||
| No (ref) | 1 | 1 | 1 | |
| Yes | 1.202 (0.570,2.536) | 1.231 (0.551,2.754) | 1.975 (0.761,5.125) |
| ACE Score | Depressive Symptoms | Suicide Intensions | Suicide Plans | |||
|---|---|---|---|---|---|---|
| AOR (95% CI) | p-Value | AOR (95% CI) | p-Value | AOR (95% CI) | p-Value | |
| 0 (ref) | 1 | – | 1 | – | 1 | – |
| 1 | 2.096 (1.429, 3.074) | <0.001 | 1.831 (1.147,2.922) | 0.011 | 2.599 (1.256,5.378) | 0.010 |
| 2 | 3.155 (1.864, 5.339) | <0.001 | 2.632 (1.417,4.888) | 0.002 | 4.748 (2.032,11.096) | <0.001 |
| 3–5 | 9.707 (4.770,19.753) | <0.001 | 10.836 (5.370,21.864) | <0.001 | 22.660 (10.035,51.170) | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jia, Z.; Wen, X.; Chen, F.; Zhu, H.; Li, C.; Lin, Y.; Xie, X.; Yuan, Z. Cumulative Exposure to Adverse Childhood Experience: Depressive Symptoms, Suicide Intensions and Suicide Plans among Senior High School Students in Nanchang City of China. Int. J. Environ. Res. Public Health 2020, 17, 4718. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134718
Jia Z, Wen X, Chen F, Zhu H, Li C, Lin Y, Xie X, Yuan Z. Cumulative Exposure to Adverse Childhood Experience: Depressive Symptoms, Suicide Intensions and Suicide Plans among Senior High School Students in Nanchang City of China. International Journal of Environmental Research and Public Health. 2020; 17(13):4718. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134718
Chicago/Turabian StyleJia, Zhihui, Xiaotong Wen, Feiyu Chen, Hui Zhu, Can Li, Yixiang Lin, Xiaoxu Xie, and Zhaokang Yuan. 2020. "Cumulative Exposure to Adverse Childhood Experience: Depressive Symptoms, Suicide Intensions and Suicide Plans among Senior High School Students in Nanchang City of China" International Journal of Environmental Research and Public Health 17, no. 13: 4718. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17134718