1. Introduction
The development of children’s dietary habits involves many interacting factors within different domains. During the life course, the home environment is acknowledged as an important setting in shaping children’s diets [
1,
2]. The home environment can be characterized by sociodemographic, behavioral and physical domains. A large cross-European (Belgium, Bulgaria, Germany, Greece, Poland and Spain) study of pre-schoolers (3.3–5.5 years old) and their mothers that examined differences in dietary quality among pre-schoolers according to gender, weight status and mothers’ socioeconomic status (SES) provided evidence that SES, predominantly determined by mothers’ education, is positively correlated with children’s higher diet quality scores [
3]. The study authors hypothesized that higher education level in mothers positively influences their beliefs, knowledge and motivations around their child’s diet [
3].
Parental behavioral characteristics such as feeding practices also play an important role in the development of children’s food preferences, eating habits and body weight [
4,
5]. Feeding practices are defined as the behavioral strategies that parents use to influence their children’s food intake [
6]. These include monitoring food intake, restrictive or controlled feeding, pressurizing the child to eat and instrumental and emotional feeding [
4,
5,
7,
8,
9]. For example, controlled or restrictive feeding practices have been shown to have a strong positive association with high child BMI in several cross-sectional studies [
10,
11,
12,
13,
14,
15]. In contrast, putting pressure on a child to eat has been associated with lower BMI [
12,
16,
17,
18,
19,
20] and child appetite characteristics such as food fussiness and slow eating [
21,
22]. Suboptimal feeding practices may disrupt children’s self-regulation of hunger and satiety, which may contribute to the development of overweight and obesity in young children [
23].
In the case of dietary habits, feeding experience in early childhood can shape children’s subsequent dietary intake [
24]. Studies have demonstrated that breastfeeding duration is positively associated with better quality of diet, with higher intakes of fruits and vegetables among pre-school children observed [
25]. In contrast, early introduction of complementary foods (e.g., <17 weeks) has been associated with poor dietary quality, overweight and obesity in children [
26]. In later childhood, parents may also shape their children’s eating behavior not only by the food choices they make for their family but by their own eating habits [
27,
28,
29]. Several studies show the positive impact of parental role modelling on children’s eating habits, mainly on their consumption of fruits and vegetables [
2,
30,
31,
32]. Family mealtimes are also an excellent opportunity to establish healthy eating habits in early childhood. During meals, parents can make healthy options available, give children autonomy and the opportunity for food choice and exploration, and also encourage a positive family dynamic and environment [
33,
34]. For example, negative interactions between parents and children, such as restriction of foods or negative statements about a child’s food intake, are associated with higher weight status in children [
35,
36], while eating family meals while watching television is associated with consumption of unhealthy foods [
37,
38,
39,
40]. Conversely, interpersonal dynamics such as warmth and group enjoyment during the family meal are associated with lower risk of child overweight or obesity, higher fruit and vegetable intakes and increased frequency of family meals [
34,
41].
The contribution of the physical domain of the home environment on children’s dietary habits and weight status has also been examined [
42]. For example, a recent cross-sectional study demonstrated a positive association between the availability and accessibility of vegetables in the home and higher frequency of vegetable consumption among three–five-year-old children [
43]. A recent systematic review of older children (aged 6–12 years old) also reported consistent evidence of children’s intake of fruits and vegetables in the home being positively related to availability and accessibility of these foods. The authors highlighted the importance of both factors (accessibility and availability) as children may not consume fruits and vegetables that are inaccessible, even if available, especially if unhealthy foods are also available or accessible [
44].
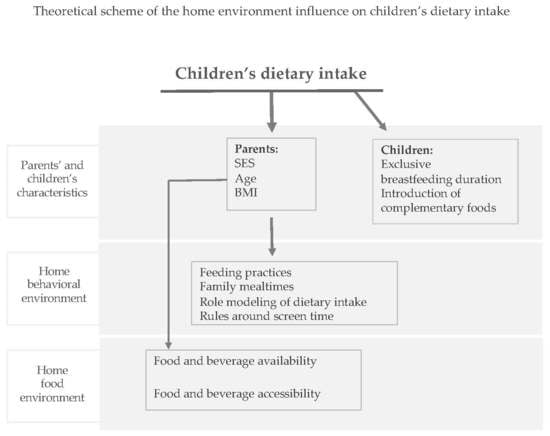
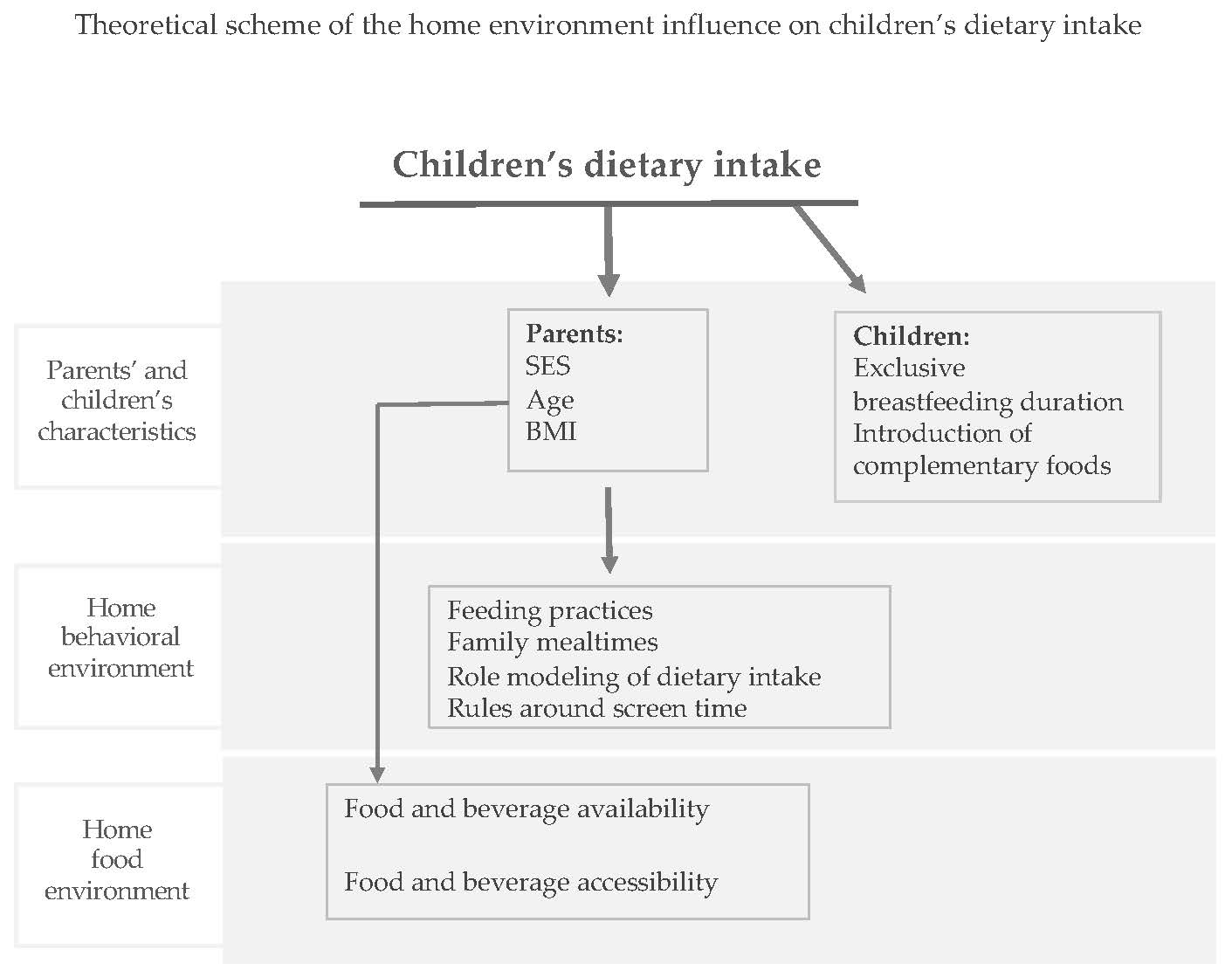
To date in Ireland, there is little research using an ecological approach to understand the influence of the home environment and parental feeding practices on pre-school children’s dietary behaviors. In this context, the present study increases our knowledge of the influence of important home environmental factors (parents’ attitudes towards children’s diet, parents’ own dietary intakes, family mealtimes, parents’ rules and polices around children’s screen time and home foods availability/accessibility) on pre-school children’s dietary intakes. Such knowledge will inform public health interventions and provide health professionals with accurate information that will allow them to effectively advise how healthier home environment for this age group can be created. Developing effective interventions to promote healthier patterns throughout the life course requires an understanding of the dietary behaviors of young children and the mediating influences of parenting practices and home environmental factors that influence early health behaviors [
45]. Therefore, this study aimed to examine the associations between home environmental characteristics, including parental control feeding practices and children’s intakes of fruit, vegetables and confectionary/sugar-sweetened beverages (SSBs).
4. Discussion
This study examined the home environmental characteristics associated with children’s fruit, vegetable and confectionary/SSB intakes. The data demonstrated that children consumed almost twice as much fresh fruit (excluding fruit juice, canned or dried fruits) than vegetables. Such a pattern of fruit and vegetable consumption among infants and pre-schoolers has previously been observed in national and international studies [
57,
58]. Consumption of biscuits, chocolates, muffins, sweets and SSBs on a weekly basis was common practice for over 70% of pre-schoolers in this study. This figure may be influenced by the offer of “treat” foods to children, which has been shown to be a habitual practice in Ireland [
59,
60]. A recent Irish study of adult treat-giving behaviors to children reported that unhealthy foods such as sweets and chocolates were the most common “treats” offered (57.8%). For 57.2% of adults, treats were offered to children routinely, between one–four times per week [
59]. It is important to consider that intake of individual food items cannot fully represent the habitual diet. However, the role of fresh fruit and vegetables in a healthy diet is clear and, moreover, has been shown to be a good marker for a heathy diet [
49]. Furthermore, excessive consumption of foods and drinks high in fat and sugar increase the risk of childhood obesity and other diet-related conditions such as dental caries and weight-related comorbidities [
61].
Parental characteristics such as education level and BMI were consistently associated with children’s consumption of fruits, vegetables and confectionery/SSBs. Higher level of parental education was associated with higher intake of fruits and vegetables and lower intakes of confectionary/SSBs in children. Our findings are supported by recently published data from a European study involving 10 countries, which associated parents’ education with fruit and vegetable consumption in 11-year-old children [
50]. The children of more highly educated parents had higher fruit intakes in five out of 10 countries, while the association between higher parental education and higher daily vegetable consumption in children was reported in seven out of 10 countries. Associations between confectionary/SSB intakes were not investigated in this international study [
50]. However, in another study, parents with lower education had children with a higher intake of snack foods, SSBs and lower quality diet in childhood and adolescence [
62]. Education may reflect parents’ capacity to access, interpret and put into practice health information. For instance, parents with higher education have been shown to make healthy options more available and accessible to children [
63]. Parents’ BMI is an indicator of environmental and sociocultural factors and is associated with children’s dietary intake and weight status in previous studies [
64,
65]. In our study, children whose parents were overweight/obese were less likely to consume fruit and vegetables, and more likely to have confectionary/SSBs one or more times per week, compared to children whose parents were normal weight. The results of the study by Wardle et al. concur with our results; this study demonstrated that children aged 4–5 years old with overweight/obese parents were less likely to consume vegetables compared to children with normal weight parents [
66].
Our study demonstrated that earlier introduction of complementary foods (<17 weeks) was positively associated with higher confectionary/SSB intakes in the unadjusted and adjusted models. An association between the timing of introduction of complementary foods was established and children’s dietary patterns and overweight/obesity has been examined in several studies with contradictory findings [
67,
68]. Results from a cross-sectional study which looked at dietary risk among children aged one–five years, breastfeeding duration and age of introduction to solids, demonstrated that poor diet quality at five years was related to shorter duration of breastfeeding, but failed to find an association with age of introduction of solids. Earlier introduction of complementary foods has been positively associated with poor dietary quality in children, with higher consumption of foods high in fat and SSBs in two previous studies [
69,
70]. In addition, a nationally representative longitudinal study ‘Growing up in Ireland’ reported that 3-year-old children who had been introduced to complementary foods after 17 weeks were less likely to be overweight or obese [
71].
In pre-school aged children, dietary habits are heavily influenced by observational learning; consequently, parents’ diets are likely to impact on their children’s dietary habits [
72,
73]. Our study found that not all foods from parents’ and children’s diets were positively associated. The most consistent findings we observed were for parent-child vegetable intakes. International studies which investigated dietary intakes in parent-child dyads have shown mixed results, with weak associations and variation by nutrient, food and parent-child dyad (such as mother-daughter or parent-offspring) [
72]. A meta-analysis by Wang et al. established that similarities between parents’ and children’s dietary intakes focused on total energy and dietary fat and concluded that the associations were weak [
74]. Overall, mixed results in this field might be explained by the fact that parents may influence their children’s eating habits not only by their own eating habits but also by providing a food environment that encourages healthy or unhealthy eating habits [
75].
The parental control feeding practice, ‘pressure to eat’ was positively associated with children’s lower fruit intake. Pressure to eat is normally used to encourage children’s food consumption [
76]. It has been hypothesized that pressure to eat is associated with food preferences, fussy eating, less healthy diet and lower BMI [
8]. Indeed, a review of the literature concluded that children whose mothers put more pressure on them to eat had lower consumption of fruits and vegetables and higher overall fat intake; these associations were observed independently of family socioeconomic status [
77]. A systematic review of the literature supports the association between parental pressure to eat and children’s lower BMI in 11 cross-sectional studies, one longitudinal study and one randomized control trial (RCT). The authors attempted to explain their findings by stating that pressure to eat may have been applied in response to children’s lower BMI and that it may not be the cause of the lower BMI [
18]. In the longitudinal study, the authors assessed the directionality in relation to fussy eating and pressure to eat. The study findings showed a positive bi-directional relationship; pre-schoolers’ fussy eating predicted parental pressure to eat at four years of age. Parental pressure to eat at four years of age predicted children’s eating fussiness at six years [
78].
The present study showed a strong association between watching more than one hour of television daily and lower vegetable consumption and higher confectionary/SSB intakes in children. International studies have identified associations between children’s television viewing, diet quality and overweight/obesity [
37,
79,
80]. Television may influence what children eat through advertisement of energy-dense foods and promotion of mindless eating during viewing, which, in turn, may lead to overeating and overweight/obesity [
39]. Indeed, a recent systematic review, which included 19 observational studies, reported that all studies found a significant positive correlation between television viewing and/or total screen time and unhealthy dietary behaviors such as lower fruit and vegetable intakes and greater consumption of foods higher in fat and sugar [
81]. Such findings are in line with the present study in which children who eat snacks while watching television were over 70% less likely to eat vegetables daily. Based on these findings, and taking into consideration that in pre-school aged children, the family environment remains a major contributor to the development of children’s eating behavior, it is advised that parents offer healthier snacks, such as fruit bowls or vegetable platters in an attractive way to children while watching television and to restrict television viewing during meal and snack times [
81].
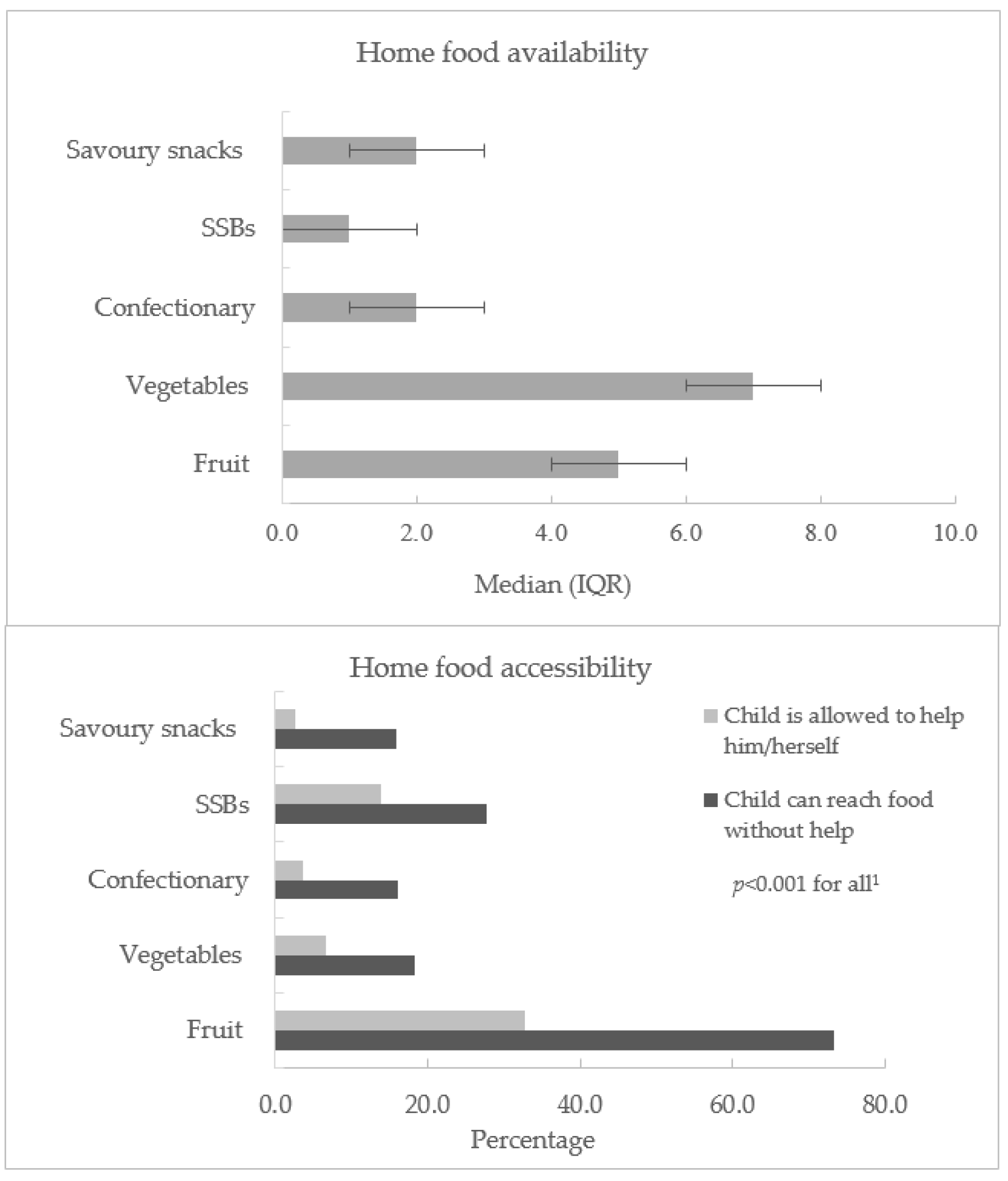
Home food availability and accessibility are among the determinants that are most consistently associated with dietary intake in children and adolescents [
82,
83,
84]. In the present study, the adjusted model showed that the availability of fruits, vegetables and SSBs in the home were associated with higher children’s fruit and confectionary/SSB intakes. Such findings are consistent with a cross-sectional study which examined the home food environment and quality of diet in parent–child dyads in which greater availability of healthful foods was associated with a higher diet quality score [
85]. Another international study with pre-schoolers reported that having foods high in sugar in the home was associated with unhealthy dietary patterns, even when fruit and vegetables were also available [
82]. A literature review and meta-analysis supported the view that the availability of food items was consistently associated with healthy or unhealthy food consumption in children [
83]. The authors hypothesized that it is possible that food availability might increase consumption by children since they tend to eat whatever is available to them [
83].
Home food accessibility is determined by whether foods are available in a form and location that facilitates their consumption; for instance, if a food item is located in a visible place such as the kitchen counter [
86]. In the present study, food accessibility was measured through food visibility—the food being easy for children to reach without adult help, and whether parents allowed children to serve themselves without asking permission. The number of parents that allowed children to take foods without permission was very low, thus, making it difficult to conduct a statistical analysis with adequate power. This is probably due to the age of the study population, since children under five years are usually not allowed to take food without their parents’ or caregivers’ permission. Thus, in the present study, the only food accessibility variable that showed a relationship with children’s dietary intake was related to food visibility. A previous study with pre-school children, which examined fruit and vegetable storage in a ready-to-eat form and children’s fruit and vegetable consumption, demonstrated that parents were more likely to feed their pre-school children with foods that are more accessible [
2]. Overall, healthy and/or unhealthy food availability and accessibility alone or in combination have been associated with children’s intake of such foods. This is, therefore, an important issue that must be taken into consideration in the development of interventions that could provide home environments favorable to healthy eating [
1,
84,
87].
Before drawing conclusions, the strengths and limitations of this study must be considered. This is one of the first studies in Ireland to provide insights into the relationship between home environmental characteristics and pre-school children’s dietary intakes. As home environment and children’s diet have been found to be related to socioeconomic status, an important strength of this study is the representation (over 45%) of parents of lower education, particularly as such parents have been under-represented in previous studies [
43]. A further strength of our study is the use of validated instruments, which allows for direct comparison with previous studies in the same age group.
The limitations of this study must also be considered. The study design is cross-sectional, hence, it can only demonstrate associations between the variables investigated but cannot demonstrate cause and effect. Furthermore, although the response rate in this study was over 50%, the results are not nationally representative. Moreover, the assessment of diet is known to be challenging and parents’ ability to recall their children’s diet may be a limiting factor. Administration of the self-completion questionnaires used in this study may have introduced positive response bias. The measurement of the home environment is complex with many dynamic influences; therefore, it is also possible that important family environment variables have been involuntarily excluded or poorly characterized.




{kind=link}
{kind=link}