1. Introduction
In late December 2019, an outbreak of an unexplained pneumonia occurred in Wuhan, Hubei Province, China, and subsequently evolved into a global pandemic. Presently, the pathogenic virus has been proven to be a novel coronavirus (COVID-19), which shares 79.5% sequence identity with SARS-CoV [
1]. A total of 2,314,621 laboratory-confirmed cases, including 157,847 deaths (6.8%) have been reported globally by 20 April 2020 [
2]. Common symptoms of COVID-19 infection include fever, fatigue, and dry cough. Some patients have experienced severe complications, including acute respiratory distress syndrome (ARDS), arrhythmia, and shock [
3]. According to one study, the mean incubation period is three days [
4]. Obviously, the COVID-19 epidemic can spread rapidly by human-to-human transmission, but the exact epidemiological characteristics and the specific modes of transmission remain partially unknown. The basic reproduction number (R0) was used to evaluate the transmission ability of COVID-19. Riou et al. estimated that the R0 of COVID-19 in January was about 2.2, suggesting the possibility for continuous human-to-human transmission [
5]. Zhou et al., obtained similar results with an R0 between 2.8 and 3.3 [
6]. Lipsitch et al. reported that severe acute respiratory syndrome-associated coronavirus (SARS-CoV) had an R0 value of approximately 2.2 to 3.6 [
7]. The transmission capacity of COVID-19 appeared to be similar or higher as compared with SARS-CoV. As a continuous unconventional public health event that can lead to economic recession and health damage, the government’s decision making should strike a balance among the prevention and control of the epidemic and the economy and people’s livelihood. After the occurrence of the epidemic peak, it is time to gradually implement the decision to resume work and production. Hence, it is of great importance to timely judge the peak of the epidemic and determine if it is possible to return to normal work and life. Faced with such a sudden outbreak of a new infectious disease, we have no history to learn from and little evidence to refer to. The traditional epidemic peak prediction models are highly sensitive to the pre-specified epidemiological parameters including R0, and the prediction results can be highly inconsistent due to different assumptions and data sources. One study obtained two results based on two different assumptions about R0. If R0 was assumed to be higher than 1 continuously, the number of infection cases would continue to rise by the end of February, in China. However, if it was assumed to decline gradually due to public health policies, then, the epidemic peak would occur in late February [
8]. Other researchers have used early epidemiological parameters to predict that the turning point of the COVID-19 epidemic, in China, would occur on 26 January [
9]. Another study used data as of 12 February to make a prediction. The result suggested that the number of newly confirmed cases in China (excluding Hubei Province) and in Hubei Province (excluding Wuhan City) would both peak approximately on 1 or 2 February [
10]. There are significant differences between the results of these studies, indicating the uncertainty of traditional peak prediction methods. The traditional models have proven to be most reliable only under ideal conditions.
To eliminate these limitations and build a practical index based on public reported data to timely evaluate the current epidemic situation, and then judge the epidemic peak robustly, we used the moving average of log-transformed daily new cases (LMA) to establish a specific index named “epidemic evaluation index” (EEI). The EEI was verified through previous SARS epidemic data in 2003, and then adopted to analyze the present COVID-19 epidemic based on its daily change.
2. Materials and Methods
We obtained the epidemic data in China available from 16 January to 20 April 2020 in the Chinese public domain [
11,
12], the data outside China from 27 January to 20 April 2020 on the WHO website [
2], and the data for the USA from 20 February to 19 April 2020 on the U.S. CDC website [
13]. On the basis of the publicly reported data, we calculated two indicators to timely judge the epidemic peak and to determine the time to resume production. Since the COVID-19 epidemic has not lasted a full year, it was difficult to judge whether the current season included the highest incidence. Therefore, the peaks we judged were all considered to be local epidemic peaks. All statistical analyses were carried out using SAS 9.4.
2.1. MovingAaverage of Log-Transformed Daily New Cases (LMA)
The pneumonia caused by COVID-19 has a median incubation period of 3.0 days [
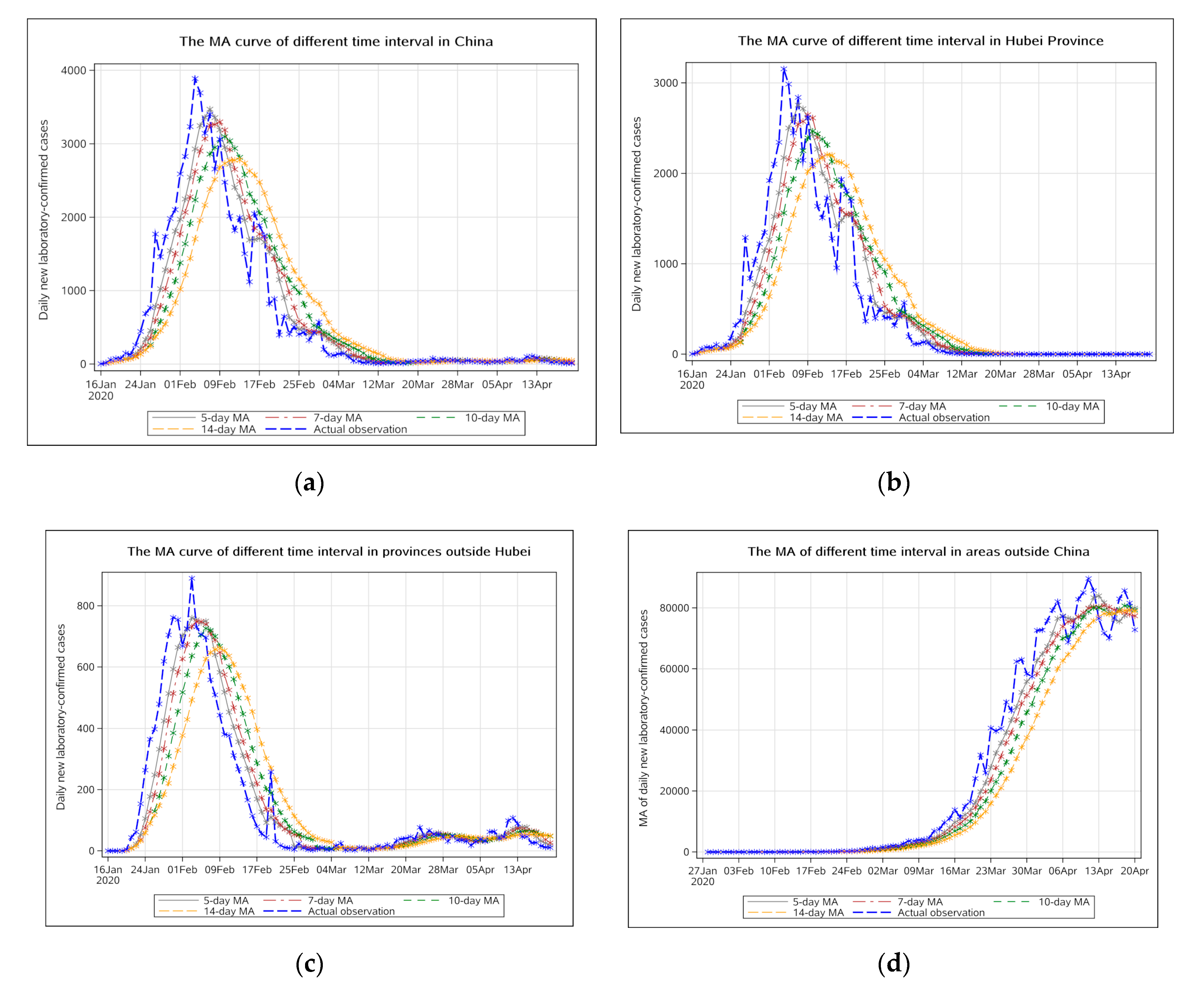
4]. According to the NHC (National Health Commission of the People’s Republic of China), the average time from onset to diagnosis was 4.95 days by 17 February 2020, therefore, the number of new cases per day could not accurately account for the epidemic situation. The choice of the LMA time interval can be changed based on the dynamics of the epidemic. Here, we mainly used the 7-day LMA, which could more effectively cover both the incubation period and the duration from the first symptoms to diagnosis. Other MAs (5 day, 10 day, and 14 day) were used for sensitivity analysis and auxiliary display was performed in
Appendix A.
In order to make the LMA computable, first, we added 1 to the actual observation, and then performed a natural logarithmic transformation to make the proposed index, namely EEI, more tolerant of outliers. Moreover, the index after data transformation had better stability and the interval of the index limits had an appropriate width. After data transformation, we obtained the natural logarithm of actual observation as
LNj:
Thus, the LMA was read as the average of
LNj:
N1,
N2, …,
Nn indicates the daily new cases for the past n days (e.g., 7-day LMA on 7 February = (Sum of log-transformed daily new cases on 1 February to 7 February)/7)
When analyzing the epidemic situation day-by-day, actual observations were presented in logarithmic transformation form and the LMA curve is shown in the figures.
2.2. Epidemic Evaluation Index (EEI)
We predicted the COVID-19 epidemic trend in different districts of China based on the moving average and its prediction limits [
14]. Furthermore, we constructed a new time-varying index named “EEI” to more intuitively reflect the epidemic situation day-by-day which helped to judge the time of the epidemic peak. The definition of the EEI indicator itself is the ratio of the number of daily new cases on two consecutive days. It is defined by the following formula:
LNt and LNt−, respectively, represents the log-transformed value of daily new confirmed cases on day t and day t-1. However, the EEI itself only indicates the epidemic situation on a certain day but cannot reflect the changes in the epidemic situation over a period of time. Therefore, instead of using the EEI itself, we used the EEI(t) as the several days’ mean of EEIs on day t to depict the curve and judge the epidemic peak based on the incubation period and the duration from the initial symptoms to diagnosis (e.g., 7-day mean of EEIs for COVID-19).
The calculation of the mean and the variance of the EEIs involved a series of parameters. Taking the COVID-19 epidemic as an example, the selected time interval is 7 days. The specific meanings of the parameters involved in the following formulas are as follows:
LMAt indicates LMA on a certain day, namely day t (e.g., 8 April, 7-day LMA for COVID-19);
LMAt−1 indicates LMA for the previous day, namely day t−1 (e.g., 7 April, 7-day LMA for COVID-19);
Xt, LNt−6 to LNt, represents log-transformed values of daily new cases on day t−6 to day t (e.g., 2–8 April);
Xt−1, LNt−7 to LNt−1, represents log-transformed values of daily new cases on day t−7 to day t−1 (e.g., 1–7 April).
Through the above parameters, the mean and variance of the EEIs are calculated on the basis of Taylor expansion [
15] as:
Then, the upper and lower limits of the EEI on day t, which were used as auxiliary parameters to judge the epidemic peak, was calculated using the following formula. The formula evolved from the formula for calculating prediction limits of MA [
16] as:
A line chart of the EEI(t) over date indicates the epidemic situation. If the EEI(t) is higher than 1.0, it suggests that the epidemic is still developing, and the peak has not occurred. High level restriction measures should be maintained. If the EEI(t) drops below 1.0 for the first time, it can be judged that the epidemic has peaked and it is time to plan to phase out some stringent preventive and control measures. If the EEI(t) remains below 1.0 for more than 7 days (one of the time intervals of the LMA), it indicates that the epidemic has entered a stable remission period. It is possible to phase out highly stringent restrictions, and then resume production gradually. The upper and lower limits of the EEI on day t are auxiliary parameters for evaluating the epidemic situation and represent the worst and the best estimates of the epidemic situation, respectively. If the upper limit of the EEI on day t is maintained not far from 1.0 and at a relatively stable level, it indicates that the epidemic has stabilized. Moreover, if the upper limit of the EEI is less than 1, it indicates that under the worst circumstance, the EEI is also at a low level. It can be said with greater confidence that the epidemic would soon be completely eliminated. Likewise, if the lower limit of the EEI is above 1.0, this indicates that the epidemic is still in a severe period of progress. If there are very few daily new confirmed cases (<5), the EEI(t) would not be applicable. In this scenario, we should evaluate the epidemic situation based on suspected cases or other indicators.
2.3. The Verification of EEI(t)
SARS epidemic data for Hong Kong in 2003 was used to verify the practicability of the EEI(t). The mean incubation period of SARS was 5 to 7 days [
17] and the average duration of onset of symptoms to hospital admission was 3.8 days [
18], therefore, we used the 10-day LMA and the corresponding ratio to verify that the result was consistent with the actual epidemic peak.
4. Discussion
A comparison with the EEI(t) curve shows that the actual observation curve always fluctuates greatly and makes it difficult to judge the epidemic peak. The decline in the log-transformed actual observation curve does not mean that the peak has occurred, as it can rise again. The EEI(t) can more accurately reflect the true situation of the epidemic. It aims to judge whether the epidemic peaks occurred or not, based on the combination of actual observations and LMA.
Traditional models, including Susceptible-Exposed-Infectious-Recovered (SEIR) and auto regressive integrated moving average (ARIMA) models, require preset application conditions. The new proposed EEI(t) avoids these limitations and is more intuitive and reliable with only officially released data. The EEI(t) aims to monitor and evaluate the epidemic in time, not to make predictions. It adopts another idea to provide timely decision support for epidemic prevention strategies. On the basis of the analysis of the epidemic situation, it can be seen that the EEI(t) has certain reliability for judging the epidemic peak.
Regarding the COVID-19 epidemic situation, it can be concluded that whether in Hubei Province or other districts, the epidemic entered a period of decline in late February due to many timely measures that were taken. In 2003, public health measures including individual isolation, quarantine, social distancing, and community containment played decisive roles in controlling the SARS epidemic [
24]. During the COVID-19 epidemic, the Chinese government learned lessons from the experience of the SARS epidemic and adopted emergency measures related to population prevention and clinical treatment after the outbreak. A comparison with the prevention and control of the previous SARS epidemic shows that significant progress has been made during the COVID-19 epidemic [
25]. On 20 January 2020, 43 days after the first unexplained pneumonia case occurred, traffic control was implemented in Wuhan. Three days later, on 23 January, Wuhan city was closed. Two days later, on 25 January, all provinces in China, except Tibet, triggered a level one public health emergency response. As can be seen from
Figure 2 and
Figure 3, the peak of daily new laboratory-confirmed cases in Hubei province was on 9 February, approximately 14 days (one quarantine observation period) after the public health emergency response, which indicates that the public health measures proved to be effective. The peak in other provinces appeared earlier, approximately on 5 February. A possible reason for this was that the epidemic outside Hubei Province was less serious and easier to control. We can see that the first-grade prevention policy (on 20 January) had not been carried out until 20 days after the outbreak (on 31 December). After the SARS epidemic in 2003, China’s public health system has received attention, but problems that emerged during the initial stage of the COVID-19 epidemic indicated that it still lacks the ability to respond quickly to unexpected infectious diseases and public health emergencies. There is still much room for improvement in the prevention and control system for major public health emergencies [
26].
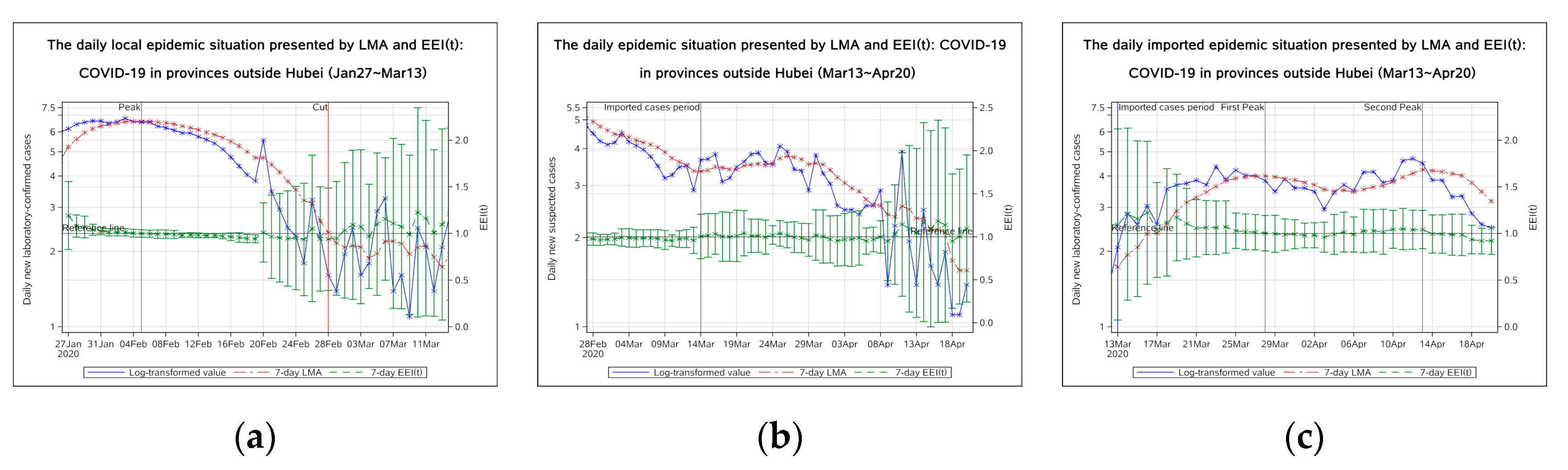
The EEI(t) in China has fallen below 1.0. In order to avoid excessive economic and social burden caused by the epidemic restriction measures, localities should take actions according to current epidemic situation. In Hubei Province, as the initial district of the epidemic outbreak, the EEI(t) has risen to slightly more than 1.0 twice. It suggests that after the epidemic peak, Hubei Province had to go through a long transition period before entering the final end phase. The local government planned to restore production of some enterprises and planned to normalize residents’ travel and public transportation after the peak (9 February 2020). After 17 February, the government reduced the restriction level and gradually restored urban traffic. In provinces outside Hubei, the EEI(t) of daily new laboratory-confirmed cases experienced two brief increases, one of which was caused by the prison epidemic. The upper limit of the index had been below 1.0 for several consecutive days which indicated that the speed of the epidemic to the end in areas outside Hubei was faster than in Hubei Province. However, resumption of work and return trips could lead to an increase in new cases. For example, on 26 February the index temporarily rose above 1.0. Local governments, in these districts, could gradually withdraw highly tight restrictions and public health emergency response based on the low-risk level of epidemic after 13 February. At the same time, public places and enterprises should continue to monitor body temperature. If public places such as department stores and restaurants are to be opened, disinfection measures should be emphasized. On 14 March, a new epidemic period caused by imported cases began. Due to the development of the epidemic worldwide, the direction of domestic epidemic prevention must be changed to prevent the spread of imported cases.
Outside of China, the EEI(t) fell below 1.0 on 14 April 2020, indicating that the global epidemic had been controlled to a certain extent. The epidemic outside China peaked on 14 April. Countries with a rapidly increasing number of confirmed cases can learn from China’s prevention and control experience and integrate it with their own economic situation and sociocultural background. Governments of the countries which have experienced epidemic peaks can begin to resume production, while continuing to focus on disinfection measures and maintain social distance, in order to accelerate the end of the global epidemic.
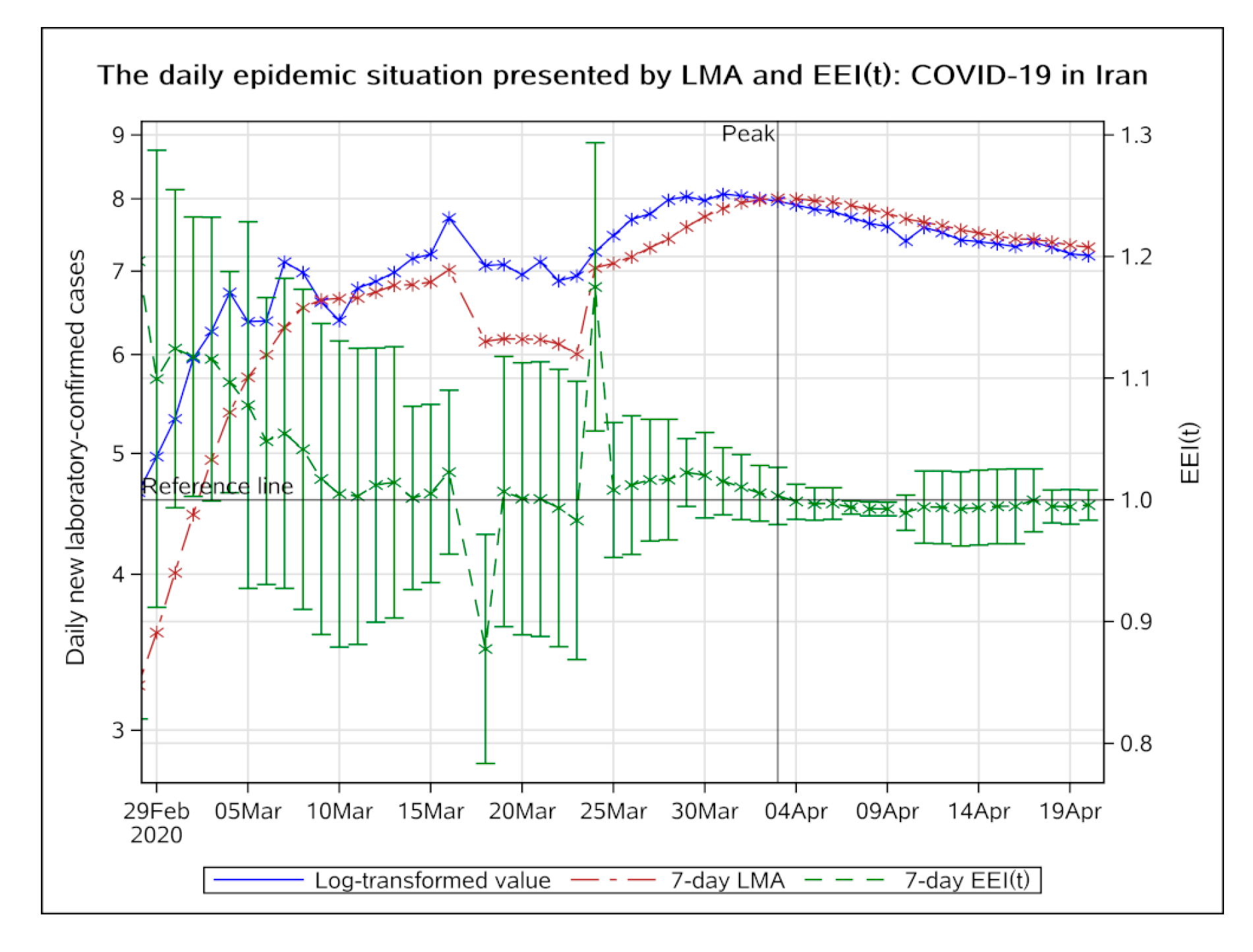
Measures taken by the Republic of Korea, Italy, Germany, and Iran to control the epidemic have shown effectiveness according to the EEI(t). On 23 February 2020, the Republic of Korea raised the level of COVID-19 epidemic warning to the highest level. Ten days later, on 4 March, the epidemic reached its peak. On 10 March, Italy closed the whole country and 18 days later, on 28 March, the epidemic reached its peak. The epidemic, in Germany and Iran, has experienced a long period before the occurrence of the peaks. In all these four countries, the epidemic has reached a stable remission period, and therefore some of the isolation measures could be withdrawn. However, on 20 March, the EEI(t) in the Republic of Korea rose above 1.0 due to imported cases, indicating that unless the epidemic in all countries is alleviated, no country can alone avoid the potential threat of the epidemic. In Singapore, the EEI(t) has not dropped below 1.0, and in the USA, the EEI(t) was still unstable and has not been continuously below 1.0. Further efforts are needed to eventually control the epidemic. Another issue worthy of attention is that the EEI(t) dropped below 1.0 twice, but then quickly returned to above 1.0 in the USA. This phenomenon suggests that a confirmation period of two to three days could be required to finalize the epidemic peak through the EEI(t). Local governments should combine the theoretical basis and the actual situation.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}








