The Northumberland Exercise Referral Scheme as a Universal Community Weight Management Programme: A Mixed Methods Exploration of Outcomes, Expectations and Experiences across a Social Gradient

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Design
2.2. Quantitative Sample
2.3. Quantitative Procedures
2.4. Qualitative Sample
2.5. Qualitative Procedures
2.6. Quantitative Analyses
2.7. Qualitative Analyses
3. Results
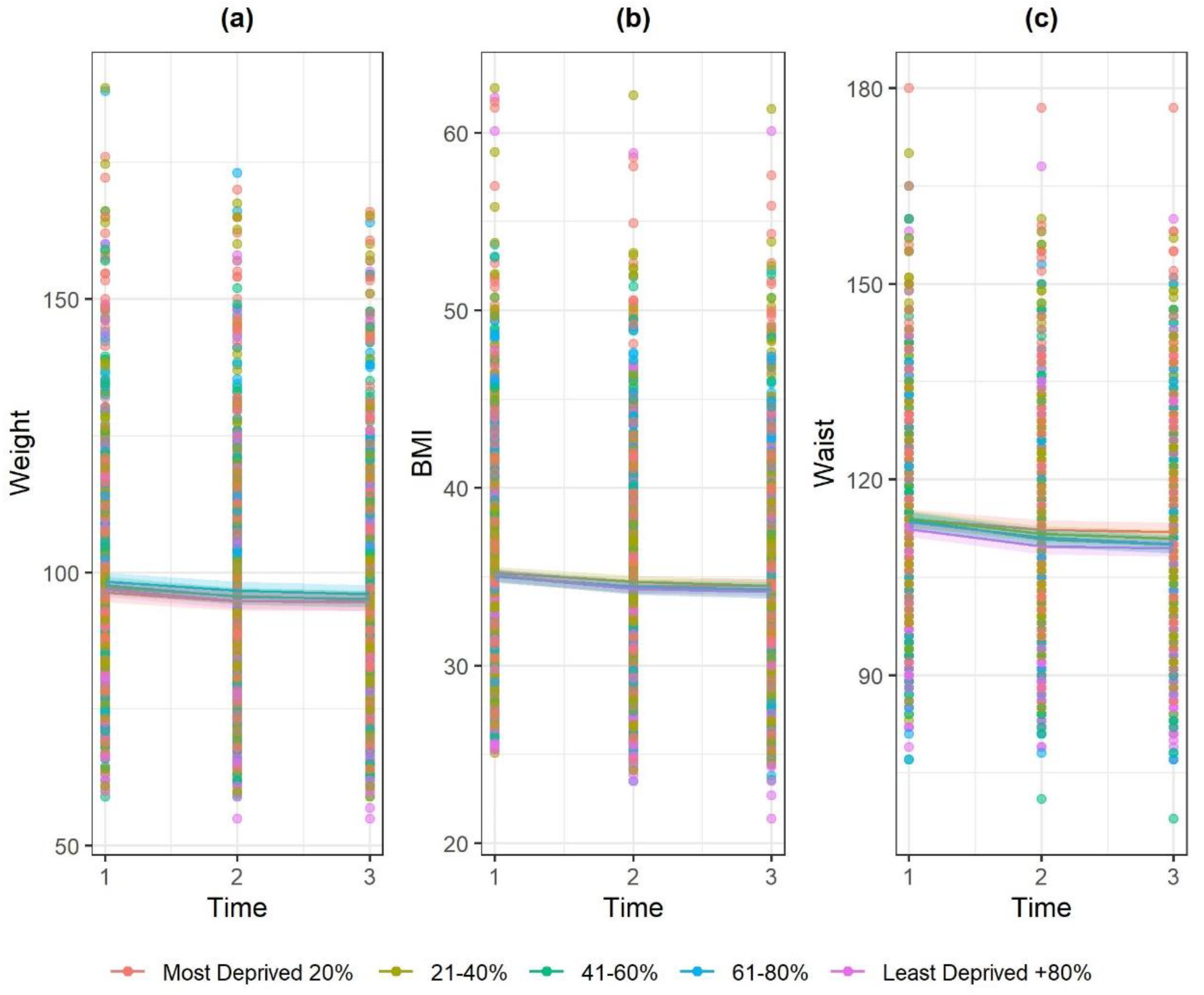
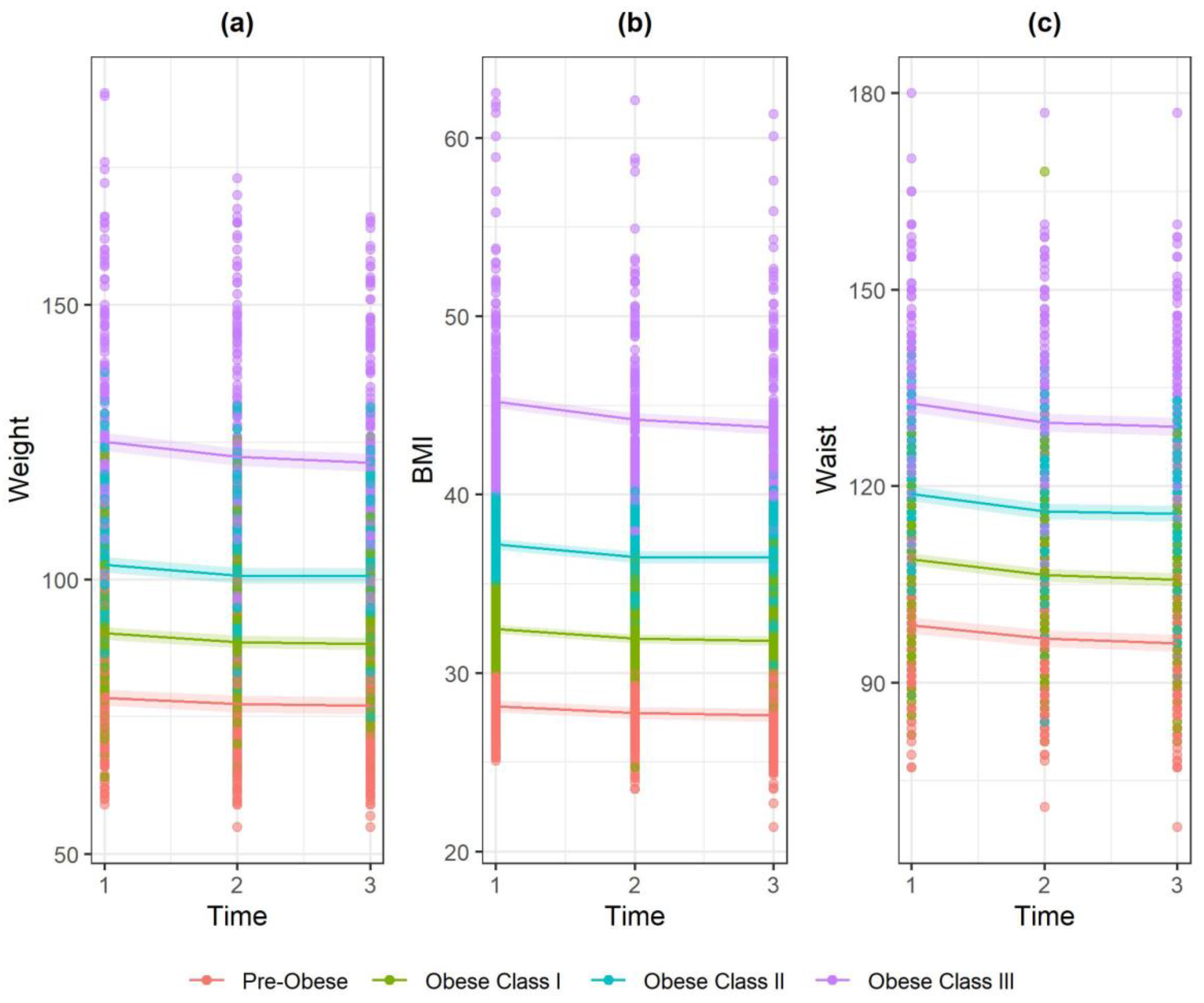
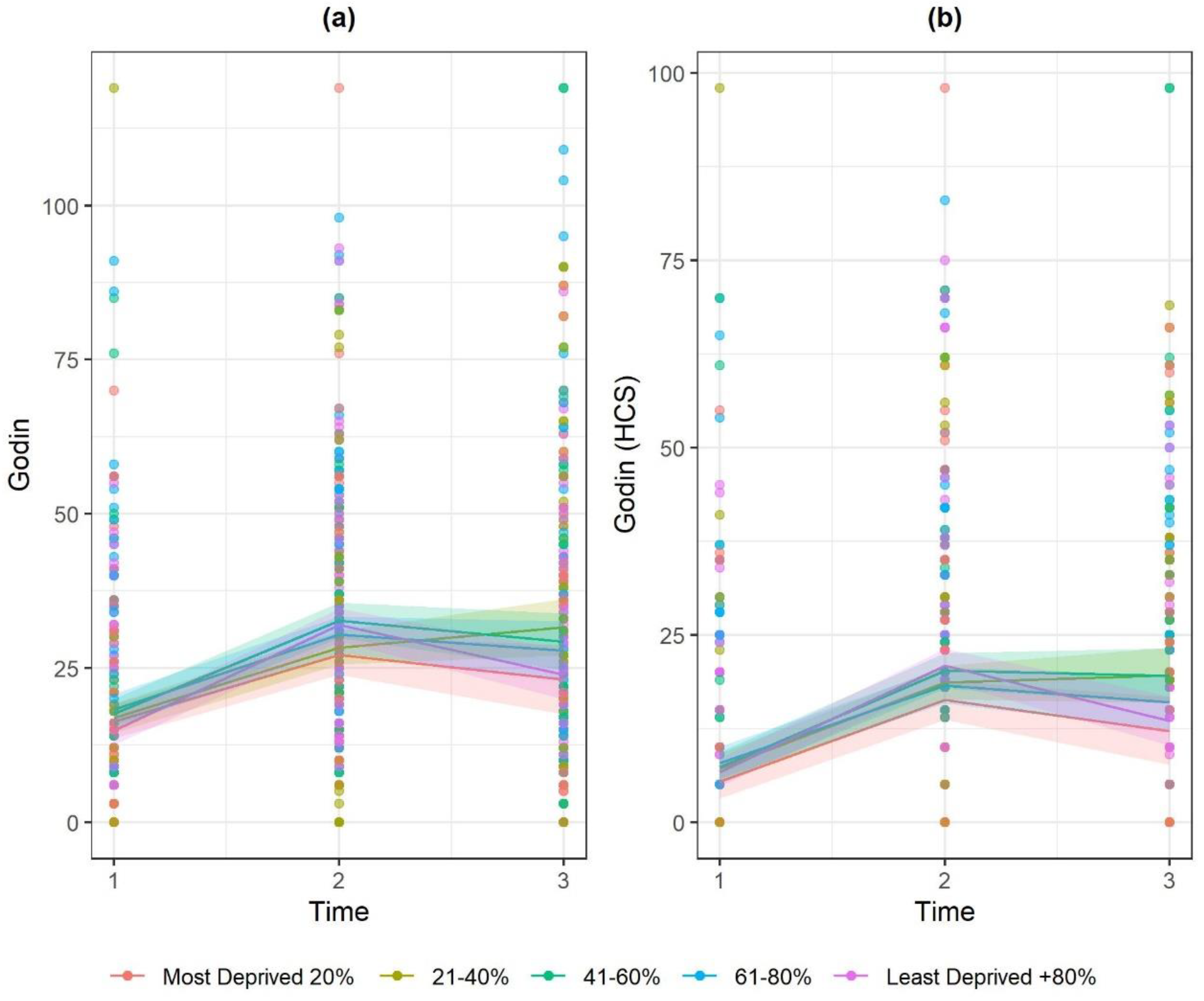
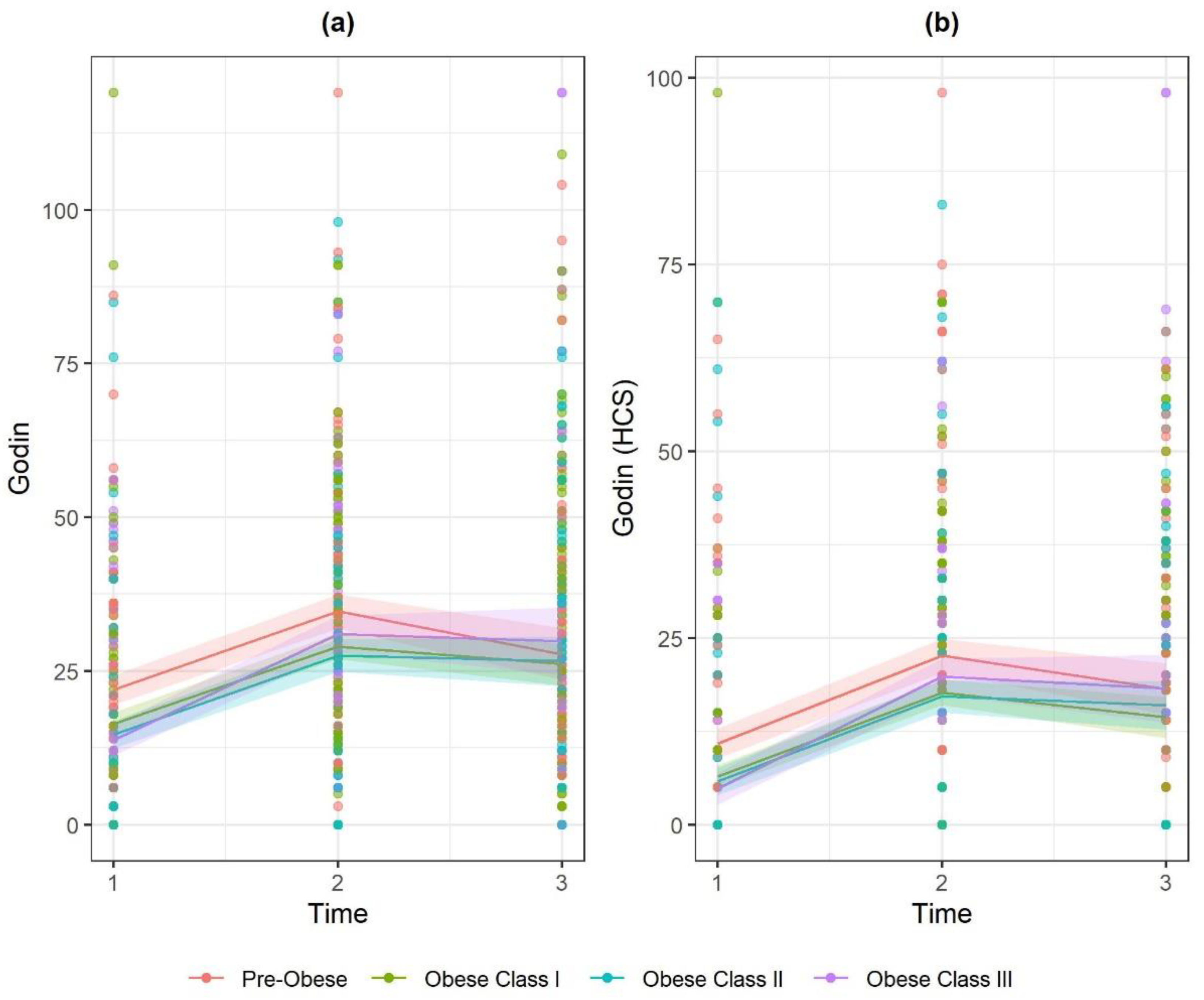
3.1. Quantitative Findings
Missing Data
3.2. Qualitative Findings
3.2.1. Support for Weight Loss in Primary Care
“I had already asked to be referred to a dietician but I never got a letter through for it... so I never got the referral... so she signed us up to this programme and that was basically it... what I could be offered in terms of weight loss...”(Amy, first interview)
3.2.2. Personal Circumstances and Weight Loss Strategies
“Well I’ve done Weight Watchers and that but I still haven’t lost... Well I did lose weight but then I did what they tell you what you are going to do... Diet, lose weight and then put it back on again”.(Julie, first interview)
“Well I’m looking forward to being thinner hopefully and a better shape so therefore just feeling healthier in myself. Also if I lose the weight that should prolong the time before I have to [have a knee operation]”.(Julie, first interview)
3.2.3. Weight Expectations versus Wellbeing Rewards
“At least two stone if not more… probably just the two stone because it is always hard work for me”.(Patricia, first interview)
“As long as I am losing something and I am feeling fitter then I will know that I am doing the right thing”.(Louise, first interview)
“I wouldn’t say so much with my weight but my overall health, it’s a lot better. I’ve lost half a stone so obviously I feel a bit down… not [disappointed] as much as I thought I would be because… I can actually get into my jeans and I have actually dropped a dress size as well…”(Amy, second interview)
4. Discussion
4.1. Physical Activity and Weight Loss
4.2. Sustainability, Adherence and Support Needs
4.3. Inequalities at Referral Point
4.4. Impact of ERS on Existing Inequalities
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kohl, H.W., 3rd; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S. The pandemic of physical inactivity: Global action for public health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef] [Green Version]
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; Van Mechelen, W.; Pratt, M. The economic burden of physical inactivity: A global analysis of major non-communicable diseases. Lancet 2016, 388, 1311–1324. [Google Scholar] [CrossRef]
- Martín-Borràs, C.; Giné-Garriga, M.; Puig-Ribera, A.; Martín, C.; Solà, M.; Cuesta-Vargas, A.I. A new model of exercise referral scheme in primary care: Is the effect on adherence to physical activity sustainable in the long term? A 15-month randomised controlled trial. BMJ Open 2018, 8, e017211. [Google Scholar] [CrossRef] [PubMed]
- Lawton, B.A.; Rose, S.B.; Elley, C.R.; Dowell, A.C.; Fenton, A.; Moyes, S.A. Exercise on prescription for women aged 40–74 recruited through primary care: Two year randomised controlled trial. BMJ 2008, 337, a2509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute for Health and Care Excellence. Exercise Referral Schemes to Promote Physical Activity. 2014, Volume 54. Available online: https://www.nice.org.uk/guidance/ph54 (accessed on 22 July 2020).
- British Heart Foundation National Centre for Physical Activity and Health. A Tool Kit for the Design, Implementation & Evaluation of Exercise Referral Schemes. Available online: http://www.ncsem-em.org.uk/resources/exercise-referral-toolkit/ (accessed on 8 July 2020).
- Wade, M.; Mann, S.; Copeland, R.J.; Steele, J. Effect of exercise referral schemes upon health and well-being: Initial observational insights using individual patient data meta-analysis from the National Referral Database. J. Epidemiol. Community Health 2020, 74, 32. [Google Scholar] [CrossRef] [Green Version]
- Oliver, E.J.; Hanson, C.L.; Lindsay, I.; Dodd-Reynolds, C.J. Exercise on referral: Evidence and complexity at the nexus of public health and sport policy. Int. J. Sport Policy Politics 2016, 8, 731–736. [Google Scholar] [CrossRef] [Green Version]
- Campbell, F.; Holmes, M.; Everson-Hock, E.; Davis, S.; Buckley Woods, H.; Anokye, N.; Tappenden, P.; Kaltenthaler, E. A systematic review and economic evaluation of exercise referral schemes in primary care: A short report. Health Technol. Assess. 2015, 19, 1–87. [Google Scholar] [CrossRef]
- Pavey, T.G.; Anokye, N.; Taylor, A.; Trueman, P.; Moxham, T.; Fox, K.; Hillsdon, M.; Green, C.; Campbell, J.; Foster, C. The clinical effectiveness and cost-effectiveness of exercise referral schemes: A systematic review and economic evaluation. Health Technol. Assess. 2011, 15, 1–254. [Google Scholar] [CrossRef] [Green Version]
- Kelly, M.C.; Rae, G.C.; Walker, D.; Partington, S.; Dodd-Reynolds, C.J.; Caplan, N. Retrospective cohort study of the South Tyneside Exercise Referral Scheme 2009–14: Predictors of dropout and barriers to adherence. J. Public Health 2017, 39, e257–e264. [Google Scholar] [CrossRef] [Green Version]
- Hanson, C.L.; Allin, L.J.; Ellis, J.G.; Dodd-Reynolds, C.J. An evaluation of the efficacy of the exercise on referral scheme in Northumberland, UK: Association with physical activity and predictors of engagement. A naturalistic observation study. BMJ Open 2013, 3, e002849. [Google Scholar] [CrossRef] [Green Version]
- Bagnall, A.-M.; Radley, D.; Jones, R.; Gately, P.; Nobles, J.; Van Dijk, M.; Blackshaw, J.; Montel, S.; Sahota, P. Whole systems approaches to obesity and other complex public health challenges: A systematic review. (Report). BMC Public Health 2019, 19, 8. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.M.; Edwards, R.T.; Williams, N.; Raisanen, L.; Moore, G.; Linck, P.; Hounsome, N.; Din, N.U.; Moore, L. An evaluation of the effectiveness and cost effectiveness of the National Exercise Referral Scheme in Wales, UK: A randomised controlled trial of a public health policy initiative. J. Epidemiol. Community Health 2012, 66, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Pavey, T.G.; Taylor, A.; Hillsdon, M.; Fox, K.; Campbell, J.; Foster, C.; Moxham, T.; Mutrie, N.; Searle, J.; Taylor, R. Levels and predictors of exercise referral scheme uptake and adherence: A systematic review. J. Epidemiol. Community Health 2012, 66, 737–744. [Google Scholar] [CrossRef]
- National Obesity Observatory. Standard Evaluation Framework for Physical Activity Interventions; National Obesity Observatory: London, UK, 2012; p. 39. [Google Scholar]
- Rowley, N.; Mann, S.; Steele, J.; Horton, E.; Jimenez, A. The effects of exercise referral schemes in the United Kingdom in those with cardiovascular, mental health, and musculoskeletal disorders: A preliminary systematic review. BMC Public Health 2018, 18, 949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavey, T.G.; Taylor, A.H.; Fox, K.R.; Hillsdon, M.; Anokye, N.; Campbell, J.L.; Foster, C.; Green, C.; Moxham, T.; Mutrie, N.; et al. Republished research: Effect of exercise referral schemes in primary care on physical activity and improving health outcomes: Systematic review and meta-analysis. Br. J. Sports Med. 2013, 47, 526. [Google Scholar] [CrossRef] [PubMed]
- Morgan, F.; Battersby, A.; Weightman, A.L.; Searchfield, L.; Turley, R.; Morgan, H.; Jagroo, J.; Ellis, S. Adherence to exercise referral schemes by participants—What do providers and commissioners need to know? A systematic review of barriers and facilitators. BMC Public Health 2016, 16, 1–11. [Google Scholar] [CrossRef]
- Steele, J.; Wade, M.; Polley, M.; Copeland, R.J.; Stokes, S.; Mann, S. The National Referral Database: An initial overview. SportRxiv 2019. [Google Scholar] [CrossRef] [Green Version]
- Hanson, C.L.; Oliver, E.J.; Dodd-Reynolds, C.J.; Allin, L.J. How do participant experiences and characteristics influence engagement in exercise referral? A qualitative longitudinal study of a scheme in Northumberland, UK. BMJ Open 2019, 9, e024370. [Google Scholar] [CrossRef] [Green Version]
- Parretti, H.M.; Bartington, S.E.; Badcock, T.; Hughes, L.; Duda, J.L.; Jolly, K. Impact of primary care exercise referral schemes on the health of patients with obesity. Pragmat. Obs. Res. 2017, 8, 189–201. [Google Scholar] [CrossRef] [Green Version]
- Birtwistle, S.B.; Ashcroft, G.; Murphy, R.; Gee, I.; Poole, H.; Watson, P.M. Factors influencing patient uptake of an exercise referral scheme: A qualitative study. Health Educ. Res. 2019, 34, 113–127. [Google Scholar] [CrossRef]
- Bambra, C.L.; Hillier, F.C.; Cairns, J.M.; Kasim, A.; Moore, H.J.; Summerbell, C.S. How effective are interventions at reducing socioeconomic inequalities in obesity among children and adults? Two systematic reviews. Public Health Res. 2015. [Google Scholar] [CrossRef] [Green Version]
- Loring, B.; Roberston, A. Obesity and Inequities Guidance for Addressing Inequities in Overweight and Obesity; World Health Oganisation: Geneva, Switzerland, 2014. [Google Scholar]
- Friel, S.; Chopra, M.; Satcher, D. Unequal weight: Equity oriented policy responses to the global obesity epidemic. BMJ 2007, 335, 1241–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Backholer, K.; Sarink, D.; Beauchamp, A.; Keating, C.; Loh, V.; Ball, K.; Martin, J.; Peeters, A. The impact of a tax on sugar-sweetened beverages according to socio-economic position: A systematic review of the evidence. Public Health Nutr. 2016, 19, 3070–3084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahern, A.L.; Aveyard, P.; Boyland, E.J.; Halford, J.C.; Jebb, S.A. Inequalities in the uptake of weight management interventions in a pragmatic trial: An observational study in primary care. Br. J. Gen. Pract. 2016, 66, e258–e263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Logue, J.; Allardice, G.; Gillies, M.; Forde, L.; Morrison, D.S. Outcomes of a specialist weight management programme in the UK National Health Service: Prospective study of 1838 patients. BMJ Open 2014, 4, e003747. [Google Scholar] [CrossRef] [PubMed]
- Lebrun, L.A.; Chowdhury, J.; Sripipatana, A.; Nair, S.; Tomoyasu, N.; Ngo-Metzger, Q. Overweight/obesity and weight-related treatment among patients in U.S. federally supported health centers. Obes. Res. Clin. Pract. 2013, 7, e377. [Google Scholar] [CrossRef]
- Dodd-Reynolds, C.J.; Nevens, L.; Oliver, E.J.; Finch, T.; Lake, A.A.; Hanson, C.L. Prototyping for public health in a local context: A streamlined evaluation of a community-based weight management programme (Momenta), Northumberland, UK. BMJ Open 2019, 9, e029718. [Google Scholar] [CrossRef] [Green Version]
- Boelsen-Robinson, T.; Peeters, A.; Beauchamp, A.; Chung, A.; Gearon, E.; Backholer, K. A systematic review of the effectiveness of whole-of-community interventions by socioeconomic position. Obes. Rev. 2015, 16, 806–816. [Google Scholar] [CrossRef]
- Beauchamp, A.; Backholer, K.; Magliano, D.; Peeters, A. The effect of obesity prevention interventions according to socioeconomic position: A systematic review. Obes. Rev. 2014, 15, 541–554. [Google Scholar] [CrossRef]
- Hillier-Brown, F.C.; Bambra, C.L.; Cairns, J.M.; Kasim, A.; Moore, H.J.; Summerbell, C.D. A systematic review of the effectiveness of individual, community and societal-level interventions at reducing socio-economic inequalities in obesity among adults. Int. J. Obes. 2014, 38, 1483–1490. [Google Scholar] [CrossRef] [Green Version]
- Marmot, M.G. Fair Society, Healthy Lives: The Marmot Review; Department of Health: London, UK, 2010. [Google Scholar]
- Althoff, T.; Sosic, R.; Hicks, J.L.; King, A.C.; Delp, S.L.; Leskovec, J. Large-scale physical activity data reveal worldwide activity inequality. Nature 2017, 547, 336–339. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. Identifying What Works for Local Physical Inactivity Interventions. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/374560/Whatworksv1_2.pdf (accessed on 8 July 2020).
- Public Health England Work. Worklessness and Health: Local Infographic Tool. Available online: https://www.gov.uk/government/publications/work-worklessness-and-health-local-infographic-tool (accessed on 12 June 2020).
- Public Health England Local Authority Health Profiles. Available online: https://fingertips.phe.org.uk/profile/health-profiles/data#page/0/gid/1938132701/pat/6/par/E12000001/ati/102/are/E06000057/iid/10101/age/169/sex/4/cid/4/page-options/ovw-do-0 (accessed on 10 June 2020).
- Creswell, J.W.; Plano Clark, V.L. Key decisions in choosing a mixed methods design. In Designing and Conducting Mixed Methods Research, 2nd ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2011; pp. 63–68. [Google Scholar]
- Godin, G.; Shepard, R.J. A simple method to assess exercise behavior in the community. Can. J. Appl. Sports Sci. 1985, 10, 141–146. [Google Scholar]
- Motl, R.W.; Bollaert, R.E.; Sandroff, B.M. Validation of the Godin Leisure-Time Exercise Questionnaire Classification Coding System Using Accelerometry in Multiple Sclerosis. Rehabil. Psych. 2018, 63, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Godin, G. The Godin-Shephard leisure-time physical activity questionnaire. Health Fitness J. Can. 2011, 4, 18–22. [Google Scholar]
- Amireault, S.; Godin, G. The Godin-Shephard leisure-time physical activity questionnaire: Validity evidence supporting its use for classifying healthy adults into active and insufficiently active categories. Percept. Mot. Ski. 2015, 120, 604. [Google Scholar] [CrossRef] [PubMed]
- Patton, M.Q. Qualitative Research & Evaluation Methods: Integrating Theory and Practice, 4th ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2015. [Google Scholar]
- Prevention CfDCa. Defining Adult Overweight and Obesity. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/obesity/adult/defining.html (accessed on 16 July 2020).
- Amireault, S.; Godin, G.; Lacombe, J.; Sabiston, C. Validation of the Godin-Shephard Leisure-Time Physical Activity Questionnaire classification coding system using accelerometer assessment among breast cancer survivors. J. Cancer Surviv. 2015, 9, 532–540. [Google Scholar] [CrossRef]
- Verbeke, G.; Molenberghs, G. Linear Mixed Models for Longitudinal Data; Springer: New York, NY, USA, 2000. [Google Scholar]
- Hosmer, D.W., Jr. Applied Logistic Regression, 3rd ed.; Hosmer, D.W., Jr., Lemeshow, S., Sturdivant, R.X., Eds.; Wiley: Hoboken, NJ, USA, 2013. [Google Scholar]
- White, I.R.; Daniel, R.; Royston, P. Avoiding bias due to perfect prediction in multiple imputation of incomplete categorical variables. Comput. Stat. Data Anal. 2010, 54, 2267–2275. [Google Scholar] [CrossRef] [Green Version]
- Morris, T.P.; White, I.R.; Royston, P. Tuning multiple imputation by predictive mean matching and local residual draws. BMC Med. Res. Methodol. 2014, 14, 75. [Google Scholar] [CrossRef] [Green Version]
- White, I.R.; Royston, P.; Wood, A.M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef]
- Little, R.J.A. Statistical Analysis with Missing Data, 2nd ed.; Wiley-Interscience: Hoboken, NJ, USA, 2002. [Google Scholar]
- Spencer, L.; Ritchie, J.; Lewis, J.; Dillon, L. Quality in Qualitative Evaluation: A Framework for Assessing Research Evidence; Cabinet Office and National Centre for Social Research: London, UK, 2003. [Google Scholar]
- Rowley, N.; Steele, J.; Wade, M.; Copeland, R.J.; Mann, S.; Liguori, G.; Horton, E.; Jimenez, A. Are Exercise Referral Schemes Associated With an Increase in Physical Activity? Observational Findings Using Individual Patient Data Meta-Analysis from the National Referral Database. J. Phys. Act. Health 2020, 17, 621–631. [Google Scholar]
- Pentecost, C.; Taket, A. Understanding exercise uptake and adherence for people with chronic conditions: A new model demonstrating the importance of exercise identity, benefits of attending and support. Health Educ. Res. 2011, 26, 908–922. [Google Scholar] [CrossRef] [PubMed]
- Eynon, M.; Foad, J.; Downey, J.; Bowmer, Y.; Mills, H. Assessing the psychosocial factors associated with adherence to exercise referral schemes: A systematic review. Scand. J. Med. Sci. Sports 2019, 29, 638–650. [Google Scholar] [CrossRef] [PubMed]
- Swift, D.L.; Johannsen, N.M.; Lavie, C.J.; Earnest, C.P.; Church, T.S. The Role of Exercise and Physical Activity in Weight Loss and Maintenance. Prog. Cardiovasc. Dis. 2014, 56, 441–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Health and Social Care. Physical Activity Guidelines: UK Chief Medical Officers’ Report; Department of Health and Social Care: London, UK, 2019.
- Prior, F.; Coffey, M.; Robins, A.; Cook, P. Long-Term Health Outcomes Associated With an Exercise Referral Scheme: An Observational Longitudinal Follow-Up Study. J. Phys. Act. Health 2019, 16, 288–293. [Google Scholar] [CrossRef]
- Brown, I.; Gould, J. Decisions about weight management: A synthesis of qualitative studies of obesity. Clin. Obes. 2011, 1, 99–109. [Google Scholar] [CrossRef]
- Buckley, B.J.R.; Thijssen, D.H.J.; Murphy, R.C.; Graves, L.E.F.; Whyte, G.; Gillison, F.B.; Crone, D.; Wilson, P.M.; Watson, P.M. Making a move in exercise referral: Co-development of a physical activity referral scheme. J. Public Health 2018, 40, e586–e593. [Google Scholar] [CrossRef]
- Conolly, A.; Craig, S. Health Survey for England 2018 Overweight and Obesity in Adults and Children; NatCen Social Resrearch, Health and Social Care Information Centre: London, UK, 2019. [Google Scholar]
- Aboueid, S.; Jasinska, M.; Bourgeault, I.; Giroux, I. Current Weight Management Approaches Used by Primary Care Providers in Six Multidisciplinary Healthcare Settings in Ontario. Can. J. Nurs Res. 2018, 50, 169–178. [Google Scholar] [CrossRef]
- Sport England. Active Lives Adult Survey November 2018/19 Report. Available online: https://www.sportengland.org/know-your-audience/data/active-lives (accessed on 22 July 2020).
- Sowden, S.; Breeze, E.; Barber, J.; Raine, R. Do general practices provide equitable access to physical activity interventions? Br. J. Gen. Pract. 2008, 58, e1–e8. [Google Scholar] [CrossRef] [Green Version]
- Smith, B. Generalizability in qualitative research: Misunderstandings, opportunities and recommendations for the sport and exercise sciences. Qual. Res. Sport Exerc. Health 2018, 10, 137–149. [Google Scholar] [CrossRef]
- Yin, R.K. Qualitative Research from Start to Finish; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Morse, J.M. Sampling in Grounded Theory. In The SAGE Handbook of Grounded Theory; Byrant, A., Charmaz, K., Eds.; SAGE Publications Ltd.: London, UK, 2007; pp. 229–244. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | At Point of Referral * | At Point of Completion | ||
|---|---|---|---|---|
| Frequency | % | Frequency | % | |
| Gender | 3585 | 100 | 1056 | 100 |
| Male | 1098 | 30.6 | 351 | 33.2 |
| Female | 2487 | 69.4 | 705 | 66.8 |
| IMD Quintile | 3595 | 100 | 1060 | 100 |
| 20% Most Deprived | 766 | 21.3 | 182 | 17.2 |
| 21–40% | 852 | 23.7 | 237 | 22.4 |
| 41–60% | 709 | 19.7 | 211 | 19.9 |
| 61–80% | 574 | 16.0 | 188 | 17.7 |
| 81–100% Least Deprived | 694 | 19.3 | 242 | 22.8 |
| Employment Status | 3291 | 100 | 999 | 100 |
| Retired | 866 | 26.3 | 455 | 45.6 |
| Claiming Benefits | 549 | 16.7 | 108 | 10.8 |
| Employed or FTE | 1183 | 36.0 | 246 | 24.6 |
| Other/not Stated | 693 | 21.1 | 190 | 19 |
| Profession of Referrer | 3576 | 100 | 1058 | 100 |
| GP | 2340 | 65.4 | 653 | 61.7 |
| Practice Nurse | 983 | 27.5 | 326 | 30.8 |
| Other/not Stated | 253 | 7.1 | 79 | 7.5 |
| BMI Category | 2687 | 100 | 1045 | 100 |
| Pre-obese (25–29.9) | 451 | 16.8 | 217 | 20.8 |
| Obese class I (30–34.9) | 894 | 33.3 | 386 | 36.9 |
| Obese class II (35–39.9) | 685 | 25.5 | 244 | 23.4 |
| Obese class III (40+) | 657 | 24.5 | 198 | 19 |
| Variable | Observations at Baseline | Observations at 12 Weeks | Observations at 24 Weeks |
|---|---|---|---|
| Weight | 1046 | 945 | 1052 |
| BMI | 1045 | 940 | 1050 |
| Waist | 1038 | 940 | 1044 |
| Observations at Baseline | Observations at 24 Weeks | Observations at 52 Weeks | |
| Godin | 1020 | 950 | 437 |
| Godin (HCS) | 1023 | 955 | 462 |
| Main Effects | Weight | BMI | Waist | Godin | Godin (HCS) |
|---|---|---|---|---|---|
| 12 Weeks (Godin: 24 Weeks) | −1.429 (−2.083; −0.776) | −0.513 (−0.756; −0.271) | −2.138 (−3.042; −1.234) | 16.299 (12.205; 20.392) | 13.963 (10.545; 17.381) |
| 24 Weeks (Godin: 52 Weeks) | −1.721 (−2.518; −0.924) | −0.673 (−1.005; −0.341) | −2.567 (−3.518; −1.616) | 4.325 (−1.054; 9.703) | 4.881 (0.506; 9.256) |
| Baseline | Ref | Ref | Ref | Ref | Ref |
| Obese class I | 11.722 (9.838; 13.606) | 4.335 (3.916; 4.753) | 10.108 (8.540; 11.676) | −5.467 (−8.488; −2.447) | −4.384 (−6.871; −1.898) |
| Obese class II | 24.227 (22.154; 26.300) | 9.080 (8.620; 9.541) | 20.127 (18.405; 21.850) | −7.271 (−10.573; −3.969) | −5.058 (−7.779; −2.337) |
| Obese class III | 46.566 (44.296; 48.836) | 17.071 (16.567; 17.574) | 33.954 (32.061; 35.847) | −8.127 (−11.720; −4.533) | −6.032 (−8.992; −3.071) |
| Pre-obese | Ref | Ref | Ref | Ref | Ref |
| Practice Nurse | −0.544 (−2.023; 0.935) | −0.457 (−0.779; −0.136) | −1.203 (−2.403; −0.002) | 1.702 (−0.304; 3.708) | 1.553 (−0.068; 3.174) |
| Other/Not Stated | 3.987 (1.398; 6.576) | 0.204 (−0.358; 0.767) | 2.875 (0.774; 4.975) | 2.814 (−0.669; 6.296) | 1.505 (−1.307; 4.316) |
| General Practitioner | Ref | Ref | Ref | Ref | Ref |
| Retired | −1.631 (−3.620; 0.358) | −0.069 (−0.501; 0.363) | 0.426 (−1.189; 2.040) | 0.034 (−2.663; 2.730) | −0.184 (−2.365; 1.996) |
| Benefits | 0.599 (−1.925; 3.124) | −0.093 (−0.642; 0.455) | 2.346 (0.298; 4.393) | −2.527 (−5.962; 0.908) | −3.201 (−5.987; −0.415) |
| Other/Not Stated | −2.178 (−4.238; −0.117) | 0.011 (−0.437; 0.459) | 0.923 (−0.749; 2.595) | −0.146 (−2.945; 2.653) | 0.058 (−2.208; 2.325) |
| Employed/FTE | Ref | Ref | Ref | Ref | Ref |
| Male | 16.325 (14.883; 17.767) | 0.077 (−0.237; 0.390) | 8.580 (7.410; 9.751) | 2.255 (0.301; 4.209) | 2.372 (0.793; 3.952) |
| Female | Ref | Ref | Ref | Ref | Ref |
| Age | −0.121 (−0.188; −0.054) | −0.014 (−0.029; 0.001) | 0.012 (−0.043; 0.066) | −0.209 (−0.300; −0.118) | −0.212 (−0.286; −0.138) |
| Quintile 1: Most Deprived (0–20%) | −0.633 (−2.956; 1.691) | −0.074 (−0.589; 0.441) | 1.569 (−0.361; 3.499) | 1.447 (−2.220; 5.114) | −1.216 (−4.230; 1.799) |
| Quintile 2: (21–40%) | 0.309 (−1.791; 2.409) | 0.132 (−0.334; 0.598) | 1.597 (−0.150; 3.344) | 1.984 (−1.374; 5.342) | 0.555 (−2.213; 3.322) |
| Quintile 3: (41–60%) | 0.774 (−1.328; 2.876) | −0.057 (−0.524; 0.410) | 1.440 (−0.312; 3.193) | 2.698 (−0.655; 6.052) | 0.692 (−2.073; 3.457) |
| Quintile 4: (61–80%) | 1.395 (−0.754; 3.545) | −0.077 (−0.555; 0.400) | 1.082 (−0.713; 2.878) | 3.336 (−0.106; 6.779) | 1.264 (−1.574; 4.101) |
| Quintile 5: Least Deprived (+80%) | Ref | Ref | Ref | Ref | Ref |
| Constant | 80.495 (76.266; 84.723) | 29.087 (28.164; 30.010) | 93.679 (90.230; 97.127) | 30.782 (24.792; 36.772) | 21.653 (16.789; 26.518) |
| Interactions | Weight | BMI | Waist | Godin | Godin (HCS) |
| Time = 2 × Obese class I | −0.402 (−1.060; 0.255) | −0.171 (−0.415; 0.073) | −0.440 (−1.349; 0.469) | −0.198 (−4.256; 3.861) | −0.548 (−3.945; 2.849) |
| Time = 2 × Obese class II | −0.855 (−1.573; −0.137) | −0.342 (−0.608; −0.075) | −0.697 (−1.687; 0.292) | 0.098 (−4.358; 4.554) | −0.355 (−4.090; 3.380) |
| Time = 2 × Obese class III | −1.585 (−2.353; −0.817) | −0.630 (−0.915; −0.345) | −0.960 (−2.032; 0.111) | 4.484 (−0.238; 9.205) | 3.231 (−0.730; 7.193) |
| Time = 2 × Pre-obese | Ref | Ref | Ref | Ref | Ref |
| Time = 3 × Obese class I | −0.466 (−1.256; 0.325) | −0.187 (−0.516; 0.143) | −0.410 (−1.355; 0.535) | 3.852 (−1.793; 9.497) | 0.540 (−4.038; 5.118) |
| Time = 3 × Obese class II | −0.620 (−1.487; 0.248) | −0.237 (−0.598; 0.125) | −0.378 (−1.413; 0.658) | 6.146 (0.060; 12.231) | 2.824 (−2.132; 7.781) |
| Time = 3 × Obese class III | −2.316 (−3.242; −1.390) | −0.942 (−1.328; −0.556) | −0.920 (−2.035; 0.196) | 10.234 (3.044; 17.424) | 6.070 (0.152; 11.989) |
| Time = 3 × Pre-obese | Ref | Ref | Ref | Ref | Ref |
| Time = 2 × Quintile 1: (0–20%) | 0.515 (−0.276; 1.305) | 0.192 (−0.100; 0.485) | 0.937 (−0.157; 2.031) | −6.321 (−11.108; −1.533) | −3.403 (−7.411; 0.605) |
| Time = 2 × Quintile 2: (21–40%) | 0.551 (−0.169; 1.271) | 0.260 (−0.007; 0.527) | 0.274 (−0.722; 1.270) | −5.633 (−10.101; −1.165) | −2.858 (−6.590; 0.874) |
| Time = 2 × Quintile 3: (41–60%) | −0.090 (−0.815; 0.634) | 0.052 (−0.217; 0.321) | −0.362 (−1.364; 0.640) | −1.940 (−6.475; 2.595) | −1.402 (−5.197; 2.393) |
| Time = 2 × Quintile 4: (61–80%) | 0.423 (−0.326; 1.172) | 0.206 (−0.073; 0.484) | 0.235 (−0.802; 1.272) | −4.872 (−9.520; −0.223) | −3.941 (−7.831; −0.052) |
| Time = 2 × Quintile 5: (+80%) | Ref | Ref | Ref | Ref | Ref |
| Time = 3 × Quintile 1: (0–20%) | 0.898 (−0.033; 1.830) | 0.460 (0.071; 0.848) | 0.923 (−0.192; 2.039) | −2.283 (−9.400; 4.835) | −0.107 (−5.943; 5.728) |
| Time = 3 × Quintile 2: (21–40%) | 0.317 (−0.551; 1.185) | 0.206 (−0.156; 0.567) | −0.111 (−1.150; 0.927) | 5.711 (−0.591; 12.014) | 5.561 (0.363; 10.758) |
| Time = 3 × Quintile 3: (41–60%) | −0.055 (−0.939; 0.829) | 0.086 (−0.283; 0.455) | −0.910 (−1.971; 0.151) | 2.607 (−3.705; 8.919) | 5.327 (0.170; 10.485) |
| Time = 3 × Quintile 4: (61–80%) | 0.208 (−0.699; 1.115) | 0.240 (−0.139; 0.618) | −0.447 (−1.536; 0.643) | 0.540 (−5.861; 6.942) | 1.211 (−3.971; 6.392) |
| Time = 3 × Quintile 5: (+80%) | Ref | Ref | Ref | Ref | Ref |
| Participant Pseudonym | Age Group (Years) | Gender | Employment Status | Index of Multiple Deprivation Quintile | Number of Interviews Completed | Participation Status * | Self-Reported Weight Loss |
|---|---|---|---|---|---|---|---|
| Amy | 20–29 | Female | Home-maker | 21–40% most deprived | 2 | Adherer | 3.2 kg |
| Julie | 50–59 | Female | Employed | 20% least deprived | 2 | Adherer | 3.6 kg |
| Patricia | 60–69 | Female | Retired | 40–60% most deprived | 2 | Adherer | 3.2 kg |
| Paul | 50–59 | Male | Disability benefit | 20% most deprived | 2 | Medically excluded | No weight loss |
| Jackie | 40–49 | Female | Carer | 20% most deprived | 2 | Non-attender | No weight loss |
| Vicky | 40–49 | Female | Unemployed | 20% most deprived | 1 | Dropout | Unknown |
| Louise | 40–49 | Female | Employed | 20% most deprived | 1 | Dropout | Unknown |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dodd-Reynolds, C.J.; Vallis, D.; Kasim, A.; Akhter, N.; Hanson, C.L. The Northumberland Exercise Referral Scheme as a Universal Community Weight Management Programme: A Mixed Methods Exploration of Outcomes, Expectations and Experiences across a Social Gradient. Int. J. Environ. Res. Public Health 2020, 17, 5297. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155297
Dodd-Reynolds CJ, Vallis D, Kasim A, Akhter N, Hanson CL. The Northumberland Exercise Referral Scheme as a Universal Community Weight Management Programme: A Mixed Methods Exploration of Outcomes, Expectations and Experiences across a Social Gradient. International Journal of Environmental Research and Public Health. 2020; 17(15):5297. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155297
Chicago/Turabian StyleDodd-Reynolds, Caroline J., Dimitris Vallis, Adetayo Kasim, Nasima Akhter, and Coral L. Hanson. 2020. "The Northumberland Exercise Referral Scheme as a Universal Community Weight Management Programme: A Mixed Methods Exploration of Outcomes, Expectations and Experiences across a Social Gradient" International Journal of Environmental Research and Public Health 17, no. 15: 5297. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155297