Social Inequalities and Loneliness as Predictors of Ageing Well: A Trend Analysis Using Mixed Models


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Measures
2.3. Analyses
3. Results
3.1. Sample Characteristics
3.2. Predictors of Physical Functioning and Optimism
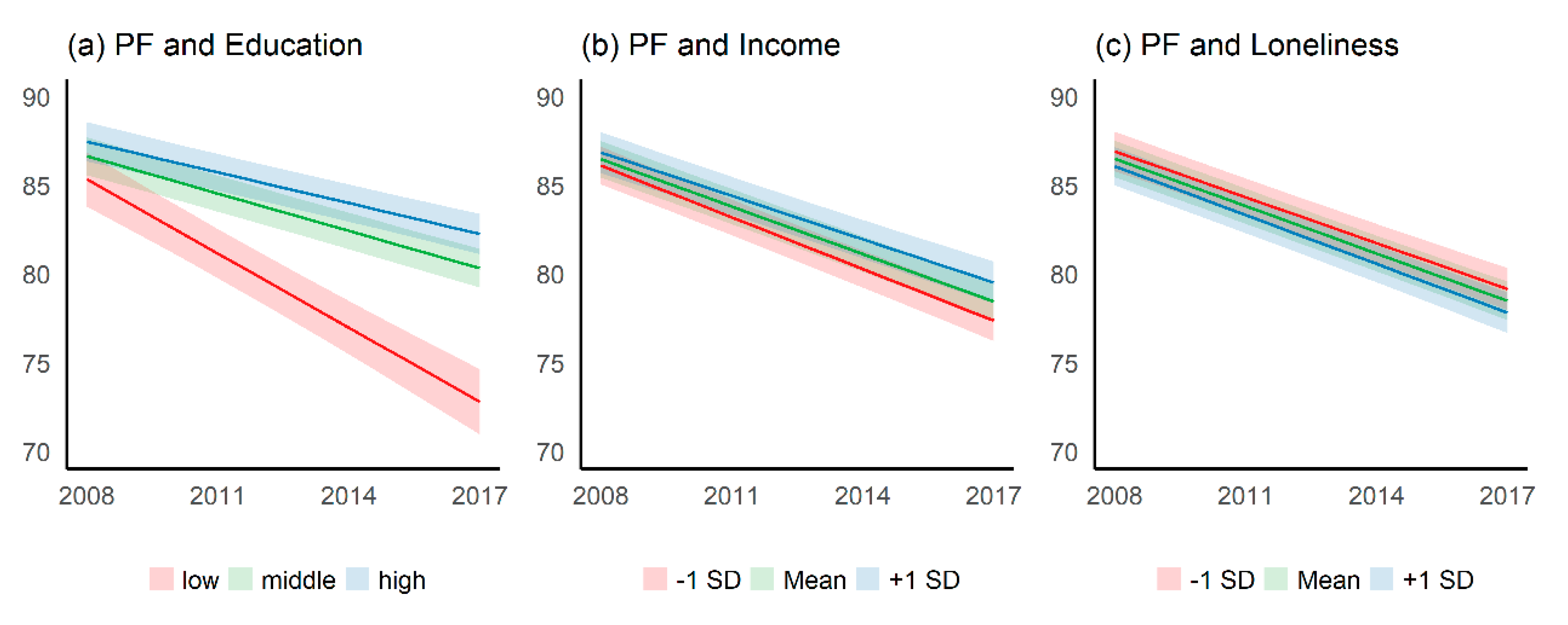
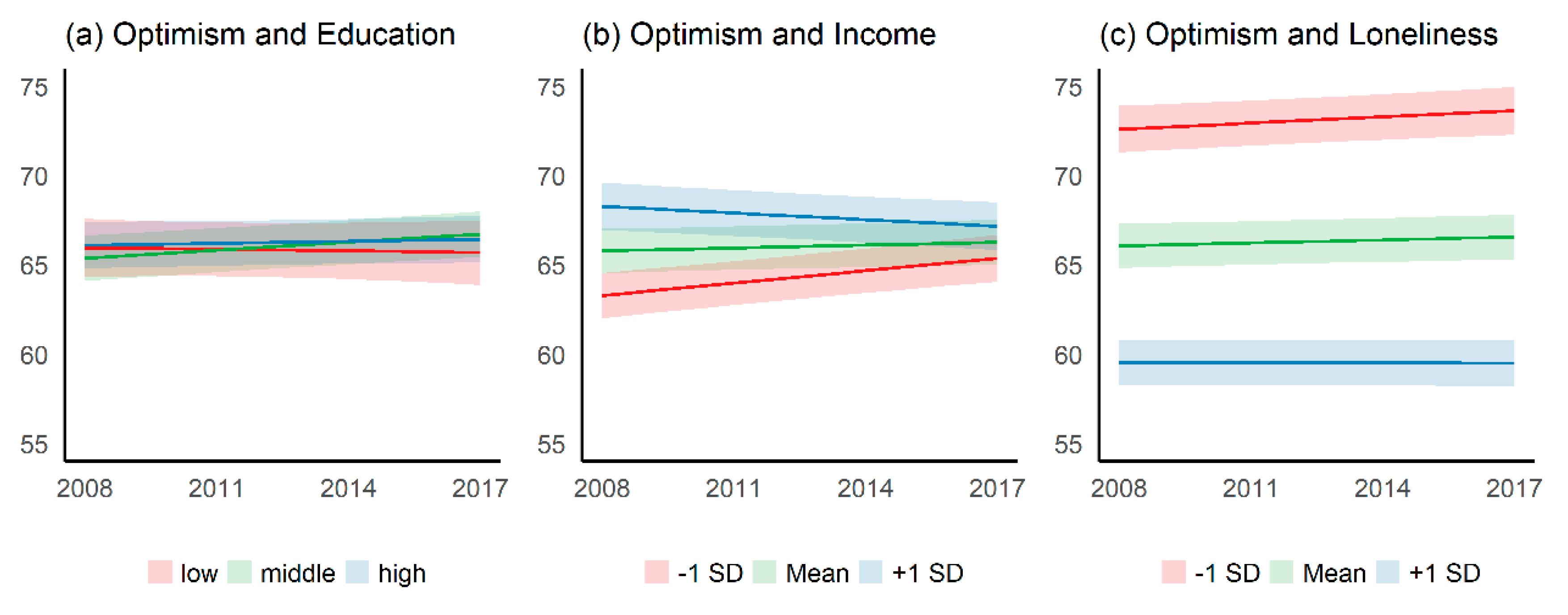
3.3. Time Trend of Physical Functioning and Optimism by Education, Income, and Loneliness
4. Discussion
4.1. Summary of the Main Findings
4.2. Comparison with Previous Research
4.3. Strengths
4.4. Limitations
4.5. Policy Implications
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Physical Functioning | Optimism | |||||
|---|---|---|---|---|---|---|
| Predictors | Estimates | 95% CI 2 | p | Estimates | 95% CI | p |
| (Intercept) | 88.17 | 86.26–90.08 | <0.001 | 64.13 | 62.21–66.05 | <0.001 |
| Wave | −4.18 | −4.81–(−3.55) | <0.001 | −0.07 | −0.62–0.47 | 0.791 |
| Between-Effects | ||||||
| Education, middle | −0.77 | −2.54–1.01 | 0.397 | −1.12 | −2.73–0.50 | 0.175 |
| Education, high | −0.32 | −2.23–1.59 | 0.742 | −0.05 | −1.78–1.69 | 0.957 |
| Income | 0.26 | −0.85–1.37 | 0.646 | 6.05 | 5.04–7.06 | <0.001 |
| Loneliness | −0.67 | −1.67–0.33 | 0.188 | −12.69 | −13.60–(−11.78) | <0.001 |
| Age | −9.50 | −10.10–(−8.90) | <0.001 | −3.86 | −4.40–(−3.31) | <0.001 |
| Female gender | −3.66 | −4.27–(−3.05) | <0.001 | −0.59 | −1.15–(−0.04) | 0.036 |
| Migration background | −0.33 | −1.63–0.98 | 0.625 | 1.08 | −0.11–2.27 | 0.074 |
| Partnership, same household | 1.72 | 1.04–2.40 | <0.001 | 0.62 | 0.01–1.23 | 0.048 |
| Partnership, different household | 0.32 | −0.83–1.48 | 0.581 | 0.67 | −0.36–1.70 | 0.201 |
| Voluntary work | 0.59 | 0.06–1.13 | 0.030 | 0.90 | 0.42–1.38 | <0.001 |
| Self-rated health | 22.47 | 21.86–23.07 | <0.001 | 10.71 | 10.16–11.25 | <0.001 |
| Within-Effects | ||||||
| Income | 0.36 | 0.05–0.67 | 0.022 | 0.43 | 0.16–0.70 | 0.002 |
| Loneliness | −0.30 | −0.60–0.00 | 0.051 | −3.48 | −3.74–(−3.21) | <0.001 |
| Self-rated health | 4.61 | 4.30–4.91 | <0.001 | 2.09 | 1.82–2.36 | <0.001 |
| Interaction Effects | ||||||
| Wave * Education, middle | 2.07 | 1.41–2.74 | <0.001 | 0.53 | −0.04–1.11 | 0.069 |
| Wave * Education, high | 2.45 | 1.75–3.14 | <0.001 | 0.19 | −0.41–0.80 | 0.529 |
| Wave * Income (between) | 0.47 | 0.10–0.85 | 0.013 | −1.06 | −1.39–(−0.74) | <0.001 |
| Wave * Loneliness (between) | −0.17 | −0.52–0.19 | 0.359 | −0.36 | −0.67–(−0.05) | 0.024 |
| ICC 3 | 0.45 | 0.51 | ||||
| Observations | 21,632 | 21,676 | ||||
| Marginal R2/Conditional R2 | 0.45/0.70 | 0.34/0.67 | ||||
| Predictor | Physical functioning | Optimism | |||
|---|---|---|---|---|---|
| EMM 1 | 95% CI | EMM 1 | 95% CI | ||
| Wave | Education | ||||
| 1 | low | 85.2 | 83.7–86.7 | 65.7 | 64.1–67.4 |
| 2 | 81.0 | 79.6–82.4 | 65.7 | 64.2–67.2 | |
| 3 | 76.8 | 75.3–78.3 | 65.6 | 65.0–67.1 | |
| 4 | 72.7 | 70.8–74.5 | 65.5 | 64.7–67.3 | |
| 1 | middle | 86.5 | 85.4–87.6 | 65.2 | 63.9–66.4 |
| 2 | 84.4 | 83.4–85.4 | 65.6 | 64.4–66.8 | |
| 3 | 82.3 | 81.3–83.3 | 66.1 | 64.8–67.3 | |
| 4 | 80.2 | 79.1–81.3 | 66.5 | 65.2–67.8 | |
| 1 | high | 87.3 | 86.2–88.4 | 65.9 | 64.6–67.2 |
| 2 | 85.6 | 84.6–86.6 | 66.0 | 64.8–67.2 | |
| 3 | 83.9 | 82.8–84.9 | 66.1 | 64.9–67.4 | |
| 4 | 82.1 | 81.0–83.2 | 66.2 | 64.9–67.5 | |
| Income | |||||
| 1 | −1 SD | 86.0 | 84.9–87.0 | 63.1 | 61.8–64.3 |
| 2 | 83.1 | 82.1–84.0 | 63.8 | 62.6–65.0 | |
| 3 | 80.1 | 79.1–81.2 | 64.5 | 63.2–65.7 | |
| 4 | 77.2 | 76.1–78.4 | 65.2 | 63.9–66.5 | |
| 1 | Mean | 86.3 | 85.3–87.3 | 65.6 | 64.3–66.8 |
| 2 | 83.7 | 82.7–84.6 | 65.7 | 64.5–66.9 | |
| 3 | 81.0 | 80.0–82.0 | 65.9 | 64.7–67.1 | |
| 4 | 78.3 | 77.2–79.4 | 66.1 | 64.8–67.3 | |
| 1 | +1 SD | 86.7 | 85.6–87.9 | 68.1 | 66.7–69.4 |
| 2 | 84.3 | 83.2–85.3 | 67.7 | 66.4–69.0 | |
| 3 | 81.8 | 80.7–82.9 | 67.3 | 66.0–68.6 | |
| 4 | 79.4 | 78.2–80.6 | 67.0 | 65.6–68.3 | |
| Loneliness | |||||
| 1 | −1 SD | 86.8 | 85.7–87.9 | 72.4 | 71.1–73.7 |
| 2 | 84.2 | 83.1–85.2 | 72.7 | 71.5–74.0 | |
| 3 | 81.6 | 80.5–82.7 | 73.1 | 71.8–74.3 | |
| 4 | 79.0 | 77.8–80.2 | 73.4 | 72.1–74.7 | |
| 1 | Mean | 86.4 | 85.3–87.4 | 65.9 | 64.6–67.1 |
| 2 | 83.7 | 82.7–84.7 | 66.0 | 64.8–67.2 | |
| 3 | 81.0 | 80.0–82.0 | 66.2 | 65.0–67.4 | |
| 4 | 78.3 | 77.3–79.4 | 66.3 | 65.1–67.6 | |
| 1 | +1 SD | 85.9 | 84.9–87.0 | 59.3 | 58.1–60.0 |
| 2 | 83.2 | 82.2–84.2 | 59.3 | 58.1–60.5 | |
| 3 | 80.4 | 79.4–81.5 | 59.3 | 58.1–60.5 | |
| 4 | 77.7 | 76.6–78.8 | 59.3 | 58.0–60.6 | |
References
- Beard, J.R.; Bloom, D.E. Towards a comprehensive public health response to population ageing. Lancet 2014, 385, 658–661. [Google Scholar] [CrossRef] [Green Version]
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2017; United Nations: New York, NY, USA, 2017. [Google Scholar]
- Rowe, J.W.; Kahn, R.L. Successful Aging. Gerontologist 1997, 37, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Depp, C.A.; Vahia, I.V.; Jeste, D. Successful Aging: Focus on Cognitive and Emotional Health. Annu. Rev. Clin. Psychol. 2010, 6, 527–550. [Google Scholar] [CrossRef] [PubMed]
- Cosco, T.D.; Prina, A.M.; Perales, J.; Stephan, B.C.M.; Brayne, C. Operational definitions of successful aging: A systematic review. Int. Psychogeriatr. 2013, 26, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Kok, A.A.L.; Aartsen, M.J.; Deeg, D.J.H.; Huisman, M. Capturing the Diversity of Successful Aging: An Operational Definition Based on 16-Year Trajectories of Functioning. Gerontologist 2015, 57, 240–251. [Google Scholar] [CrossRef] [Green Version]
- Kendig, H.; Browning, C.J.; Thomas, S.A.; Wells, Y. Health, Lifestyle, and Gender Influences on Aging Well: An Australian Longitudinal Analysis to Guide Health Promotion. Front. Public Health 2014, 2, 70. [Google Scholar] [CrossRef]
- Cosco, T.D.; Prina, A.M.; Perales, J.; Stephan, B.C.M.; Brayne, C. Lay perspectives of successful ageing: A systematic review and meta-ethnography. BMJ Open 2013, 3, e002710. [Google Scholar] [CrossRef]
- Foster, L.; Walker, A. Active and successful aging: A European policy perspective. Gerontologist 2015, 55, 83–90. [Google Scholar] [CrossRef]
- Glymour, M.M.; Avendano, M.; Kawachi, I. Socioeconomic Status and Health. In Social Epidemiology; Berkman, L.F., Kawachi, I., Glymour, M.M., Eds.; Oxford University Press: New York, NY, USA, 2014; pp. 17–62. [Google Scholar]
- Marmot, M. Fair Society, Healthy Lives: The Marmot Review—Executive Summary; Marmot Review: London, UK, 2010. [Google Scholar]
- Huisman, M.; Kunst, A.E.; MacKenbach, J.P. Socioeconomic inequalities in morbidity among the elderly; a European overview. Soc. Sci. Med. 2003, 57, 861–873. [Google Scholar] [CrossRef]
- Huisman, M.; Kunst, A.E.; Bopp, M.; Borgan, J.-K.; Borrell, C.; Costa, G.; Deboosere, P.; Gadeyne, S.; Glickman, M.; Marinacci, C.; et al. Educational inequalities in cause-specific mortality in middle-aged and older men and women in eight western European populations. Lancet 2005, 365, 493–500. [Google Scholar] [CrossRef]
- Von dem Knesebeck, O.; Vonneilich, N.; Lüdecke, D. Income and functional limitations among the aged in Europe: A trend analysis in 16 countries. J. Epidemiol. Community Health 2017, 71, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.P. Health Inequalities: Europe in Profile. An Independent Expert Report Commissioned by UK Presidency of the EU; Department of Health: London, UK, 2006. [Google Scholar]
- Kok, A.A.L.; Aartsen, M.J.; Deeg, D.J.H.; Huisman, M. Socioeconomic inequalities in a 16-year longitudinal measurement of successful ageing. J. Epidemiol. Community Health 2016, 70, 1106–1113. [Google Scholar] [CrossRef] [PubMed]
- Britton, A.; Shipley, M.; Singh-Manoux, A.; Marmot, M. Successful aging: The contribution of early-life and midlife risk factors. J. Am. Geriatr. Soc. 2008, 56, 1098–1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peeters, G.; Beard, J.; Deeg, D.J.H.; Tooth, L.; Brown, W.J.; Dobson, A.J. Longitudinal associations between lifestyle, socio-economic position and physical functioning in women at different life stages. Eur. J. Ageing 2018, 16, 167–179. [Google Scholar] [CrossRef]
- Depp, C.A.; Jeste, D.V. Definitions and Predictors of Successful Aging: A Comprehensive Review of Larger Quantitative Studies. Am. J. Geriatr. Psychiatry 2006, 14, 6–20. [Google Scholar] [CrossRef]
- O’rand, A. Age and Inequality: Diverse Pathways Through Later Life; Westview Press: Boulder, CO, USA, 1999. [Google Scholar]
- Schöllgen, I.; Huxhold, O.; Tesch-Römer, C. Socioeconomic status and health in the second half of life: Findings from the German Ageing Survey. Eur. J. Ageing 2010, 7, 17–28. [Google Scholar] [CrossRef] [Green Version]
- Leopold, L.; Engelhardt, H. Education and physical health trajectories in old age. Evidence from the Survey of Health, Ageing and Retirement in Europe (SHARE). Int. J. Public Health 2013, 58, 23–31. [Google Scholar] [CrossRef] [Green Version]
- Koster, A.; Bosma, H.; Broese van Groenou, M.I.; Kempen, G.I.J.M.; Penninx, B.W.J.H.; van Eijk, J.T.M.; Deeg, D.J.H. Explanations of socioeconomic differences in changes in physical function in older adults: Results from the Longitudinal Aging Study Amsterdam. BMC Public Health 2006, 6, 244. [Google Scholar] [CrossRef] [Green Version]
- Boehm, J.K.; Chen, Y.; Williams, D.R.; Ryff, C.; Kubzansky, L.D. Unequally Distributed Psychological Assets: Are There Social Disparities in Optimism, Life Satisfaction, and Positive Affect? PLoS ONE 2015, 10, e0118066. [Google Scholar] [CrossRef] [Green Version]
- Robb, K.A.; Simon, A.E.; Wardle, J. Socioeconomic Disparities in Optimism and Pessimism. Int. J. Behav. Med. 2009, 16, 331–338. [Google Scholar] [CrossRef]
- Katz, S.; Calasanti, T. Critical Perspectives on Successful Aging: Does It “Appeal More Than It Illuminates”? Gerontologist 2014, 55, 26–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ong, A.D.; Uchino, B.N.; Wethington, E. Loneliness and health in older adults: A mini-review and synthesis. Gerontology 2016, 62, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Shankar, A.; McMunn, A.; Demakakos, P.; Hamer, M.; Steptoe, A. Social isolation and loneliness: Prospective associations with functional status in older adults. Health Psychol 2017, 36, 179–187. [Google Scholar] [CrossRef] [Green Version]
- Perissinotto, C.M.; Stijacic Cenzer, I.; Covinsky, K.E. Loneliness in older persons: A predictor of functional decline and death. Arch. Intern. Med. 2012, 172, 1078–1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, S.S.; Fierloos, I.N.; Zhang, X.; Koppelaar, E.; Alhambra-Borras, T.; Rentoumis, T.; Williams, G.; Rukavina, T.; Van Staveren, R.; Ferrer, J.G.; et al. The Association between Loneliness and Health Related Quality of Life (HR-QoL) among Community-Dwelling Older Citizens. Int. J. Environ. Res. Public Health 2020, 17, 600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Jong Gierveld, J.; Van Tilburg, T. The De Jong Gierveld short scales for emotional and social loneliness: Tested on data from 7 countries in the UN generations and gender surveys. Eur. J. Ageing 2010, 7, 121–130. [Google Scholar] [CrossRef] [Green Version]
- De Jong-Gierveld, J.; Kamphuis, F. The development of a Rasch-type loneliness scale. Appl. Psychol. Meas. 1985, 9, 289–299. [Google Scholar] [CrossRef]
- Van Bavel, J.J.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N.; et al. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef]
- Douglas, H.; Georgiou, A.; Westbrook, J. Social participation as an indicator of successful aging: An overview of concepts and their associations with health. Aust. Health Rev. 2017, 41, 455–462. [Google Scholar] [CrossRef] [Green Version]
- Strawbridge, W.J.; Cohen, R.D.; Shema, S.J.; Kaplan, G.A. Successful Aging: Predictors and Associated Activities. Am. J. Epidemiol. 1996, 144, 135–141. [Google Scholar] [CrossRef]
- Engstler, H.; Hameister, N.; Schwichtenberg-Hilmert, B. German Ageing Survey (DEAS): User Manual SUF DEAS2017, Version 1.1. Available online: http://0-doi-org.brum.beds.ac.uk/10.5156/DEAS.2017.M.002 (accessed on 14 July 2020).
- Vogel, C.; Wettstein, M.; Tesch-Römer, C. Frauen und Männer in Der Zweiten Lebenshälfte: Älterwerden im Sozialen Wandel; Springer: Wiesbaden, Germany, 2019. [Google Scholar]
- Klaus, D.; Engstler, H. Daten und Methoden des Deutschen Alterssurveys. In Altern im Wandel: Zwei Jahrzehnte Deutscher Alterssurvey (DEAS); Mahne, K., Wolff, J.K., Simonson, J., Tesch-Römer, C., Eds.; Springer: Wiesbaden, Germany, 2017; pp. 29–45. [Google Scholar]
- Schiel, S.; Marcos, J.R.; Dickmann, C.; Aust, F.; Middendorf, L. Methodenbericht Deutscher Alterssurvey (DEAS): Durchführung Der 6. Erhebungswelle 2017; Deutsches Zentrum für Altersfragen (DZA): Berlin, Germany, 2019. [Google Scholar]
- World Medical Association. World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Brandtstädter, J.; Wentura, D. Changes in time perspectives and attitudes toward the future during the transition to later adulthood: Developmental psychology and differential aspects. Z. Entwickl. Pädagogische Psychol. 1994, 26, 2–21. [Google Scholar]
- International Standard Classification of Education. ISCED 1997; UNESCO: Paris, France, 1997. [Google Scholar]
- Hagenaars, A. Poverty Statistics in the Late 1980s. Research Based on Micro-Data; Office for Official Publications of the European Communities: Luxembourg, 1994. [Google Scholar]
- De Jong Gierveld, J.; van Tilburg, T. A 6-item scale for overall, emotional, and social loneliness: Confirmatory tests on survey data. Res. Aging 2006, 28, 582–598. [Google Scholar] [CrossRef]
- Carle, A.C. Fitting multilevel models in complex survey data with design weights: Recommendations. BMC Med. Res. Methodol. 2009, 9, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, G.; Witten, D.; Hastie, T.; Tibshirani, R. An Introduction to Statistical Learning: With Applications in R; Springer: New York, NY, USA, 2013. [Google Scholar]
- Gelman, A. Scaling regression inputs by dividing by two standard deviations. Stat. Med. 2008, 27, 2865–2873. [Google Scholar] [CrossRef]
- Bell, A.; Jones, K. Explaining Fixed Effects: Random Effects Modeling of Time-Series Cross-Sectional and Panel Data. Political Sci. Res. Methods 2014, 3, 133–153. [Google Scholar] [CrossRef] [Green Version]
- Mundlak, Y. On the Pooling of Time Series and Cross Section Data. Econometrica 1978, 46, 69. [Google Scholar] [CrossRef]
- Bell, A.; Fairbrother, M.; Jones, K. Fixed and random effects models: Making an informed choice. Qual. Quant. 2018, 53, 1051–1074. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Lüdecke, D. Ggeffects: Tidy Data Frames of Marginal Effects from Regression Models. JOSS 2018, 3, 772. [Google Scholar] [CrossRef] [Green Version]
- Lüdecke, D.; Makowski, D.; Waggoner, P.; Patil, I. Performance: Assessment of Regression Models Performance. Available online: https://easystats.github.io/performance/ (accessed on 14 July 2020).
- Ben-Zur, H. Loneliness, Optimism, and Well-Being Among Married, Divorced, and Widowed Individuals. J. Psychol. 2012, 146, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Snijders, T.A.B.; Bosker, R.J. Multilevel Analysis: An Introduction to Basic and Advanced Multilevel Modeling, 2nd ed.; Sage Publications: London, UK, 2012. [Google Scholar]
- Marmot, M.; Allen, J.; Bell, R.; Bloomer, E.; Goldblatt, P. Consortium for the European Review of Social Determinants of Health and the Health Divide. WHO European review of social determinants of health and the health divide. Lancet 2012, 380, 1011–1029. [Google Scholar] [CrossRef]
- Morley, J.E.; Flaherty, J.H. It’s never too late: Health promotion and illness prevention in older persons. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, 338–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dean, K.; Holstein, B.E. Health Promotion Among the Elderly. WHO Reg. Publ. Eur. Ser. 1991, 37, 341. [Google Scholar]
- Duplaga, M.; Grysztar, M.; Rodzinka, M.; Kopec, A. Scoping review of health promotion and disease prevention interventions addressed to elderly people. BMC Health Serv. Res. 2016, 16, 278. [Google Scholar] [CrossRef] [Green Version]
- Harmell, A.L.; Jeste, D.; Depp, C. Strategies for Successful Aging: A Research Update. Curr. Psychiatry Rep. 2014, 16, 476. [Google Scholar] [CrossRef] [Green Version]
- Hart, J.T. The inverse care law. Lancet 1971, 1, 405–412. [Google Scholar] [CrossRef] [Green Version]
- Masi, C.M.; Chen, H.-Y.; Hawkley, L.C.; Cacioppo, J.T. A Meta-Analysis of Interventions to Reduce Loneliness. Pers. Soc. Psychol. Rev. 2010, 15, 219–266. [Google Scholar] [CrossRef] [Green Version]
- Domènech-Abella, J.; Lara, E.; Rubio-Valera, M.; Olaya, B.; Moneta, M.V.; Rico-Uribe, L.A.; Ayuso-Mateos, J.L.; Mundó, J.; Haro, J.M. Loneliness and depression in the elderly: The role of social network. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 381–390. [Google Scholar] [CrossRef]
- WHO. World Report on Ageing and Health. 2015. Available online: https://www.who.int/ageing/events/world-report-2015-launch/en/ (accessed on 14 July 2020).


| Characteristic | 2008 (n = 6072) | 2011 (n = 3990) | 2014 (n = 7923) | 2017 (n = 5587) | Total (N = 23,572) |
|---|---|---|---|---|---|
| Physical functioning (mean, SD 1), (range 0–100) | 86.3 (20.7) | 84.2 (21.7) | 83.6 (22.0) | 83.2 (22.1) | 84.3 (21.7) |
| Optimism (mean, SD), (range 0–100) | 64.0 (19.5) | 64.6 (18.5) | 66.1 (18.5) | 66.4 (18.4) | 65.3 (18.8) |
| Education (low), % | 10.9 | 10.1 | 8.0 | 7.2 | 8.9 |
| Education (middle), % | 53.7 | 52.2 | 52.9 | 51.3 | 52.6 |
| Education (high), % | 35.4 | 37.7 | 39.1 | 41.5 | 38.5 |
| Income 2 (mean, SD) | 1632.8 (933.5) | 1776.3 (979.3) | 1897.0 (1043.0) | 2068.7 (1045.3) | 1852.2 (1018.3) |
| Loneliness (mean, SD), (range 1–4) | 1.8 (0.6) | 1.8 (0.5) | 1.8 (0.6) | 1.8 (0.5) | 1.8 (0.5) |
| Age (mean, SD) | 67.8 (11.9) | 67.7 (11.3) | 63.5 (11.9) | 63.3 (11.4) | 65.3 (11.9) |
| Age (range) | 49–104 | 49–104 | 43–98 | 43–97 | 43–104 |
| Gender (female), % | 51.6 | 53.2 | 52.1 | 51.4 | 52.0 |
| Migrant background, % | 5.5 | 4.3 | 5.5 | 4.5 | 5.0 |
| No partner, % | 19.9 | 19.2 | 20.4 | 21.8 | 20.4 |
| Partnership (same household), % | 75.8 | 75.8 | 74.9 | 73.7 | 75.0 |
| Partnership (different household), % | 4.4 | 5.0 | 4.7 | 4.4 | 4.6 |
| Voluntary work, % | 19.6 | 24.7 | 28.0 | 27.4 | 25.1 |
| Self-rated health (mean, SD), (range 1–5) | 3.6 (0.8) | 3.5 (0.8) | 3.5 (0.8) | 3.5 (0.8) | 3.6 (0.8) |
| Physical Functioning | Optimism | |||||
|---|---|---|---|---|---|---|
| Predictors | Estimates | 95% CI 2 | p | Estimates | 95% CI | p |
| (Intercept) | 84.10 | 82.62–85.57 | <0.001 | 63.24 | 61.67–64.82 | <0.001 |
| Wave | −2.12 | −2.30–(−1.94) | <0.001 | 0.27 | 0.12–0.43 | 0.001 |
| Between-Effects | ||||||
| Education (middle) | 3.35 | 2.21–4.49 | <0.001 | 0.15 | −0.90–1.20 | 0.783 |
| Education (high) | 4.69 | 3.46–5.92 | <0.001 | 0.41 | −0.72–1.54 | 0.481 |
| Income | 1.43 | 0.78–2.09 | <0.001 | 3.39 | 2.79–4.00 | <0.001 |
| Loneliness | −1.07 | −1.67–(−0.47) | <0.001 | −13.49 | −14.04–(−12.95) | <0.001 |
| Age | −9.47 | −10.07–(−8.88) | <0.001 | −3.88 | −4.42–(−3.33) | <0.001 |
| Gender (female) | −3.64 | −4.25–(−3.04) | <0.001 | −0.58 | −1.13–(−0.02) | 0.042 |
| Migrant background | −0.31 | −1.61–1.00 | 0.645 | 1.00 | −0.19–2.19 | 0.100 |
| Partnership (same household) | 1.74 | 1.06–2.42 | <0.001 | 0.58 | −0.03–1.20 | 0.062 |
| Partnership (different household) | 0.29 | −0.86–1.45 | 0.620 | 0.72 | −0.31–1.75 | 0.170 |
| Voluntary work | 0.60 | 0.07–1.14 | 0.028 | 0.89 | 0.41–1.36 | <0.001 |
| Self-rated health | 22.46 | 21.86–23.06 | <0.001 | 10.71 | 10.16–11.26 | <0.001 |
| Within-Effects | ||||||
| Income | 0.42 | 0.11–0.73 | 0.008 | 0.39 | 0.11–0.66 | 0.005 |
| Loneliness | −0.31 | −0.61–(−0.01) | 0.045 | −3.48 | −3.74–(−3.21) | <0.001 |
| Self-rated health | 4.61 | 4.30–4.92 | <0.001 | 2.10 | 1.83–2.37 | <0.001 |
| ICC 3 | 0.45 | 0.51 | ||||
| Observations (N) | 21,632 | 21,676 | ||||
| Marginal R2/Conditional R2 | 0.44/0.69 | 0.34/0.67 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klein, J.; von dem Knesebeck, O.; Lüdecke, D. Social Inequalities and Loneliness as Predictors of Ageing Well: A Trend Analysis Using Mixed Models. Int. J. Environ. Res. Public Health 2020, 17, 5314. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155314
Klein J, von dem Knesebeck O, Lüdecke D. Social Inequalities and Loneliness as Predictors of Ageing Well: A Trend Analysis Using Mixed Models. International Journal of Environmental Research and Public Health. 2020; 17(15):5314. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155314
Chicago/Turabian StyleKlein, Jens, Olaf von dem Knesebeck, and Daniel Lüdecke. 2020. "Social Inequalities and Loneliness as Predictors of Ageing Well: A Trend Analysis Using Mixed Models" International Journal of Environmental Research and Public Health 17, no. 15: 5314. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17155314