A Multiple Targeted Research Protocol for a Quasi-Experimental Trial in Primary School Children Based on an Active Break Intervention: The Imola Active Breaks (I-MOVE) Study

 , , ,
, , ,  , ,
, ,  ,
, 
Abstract
:1. Introduction
Aims of the I-MOVE Study
2. Materials and Methods
2.1. Study Design
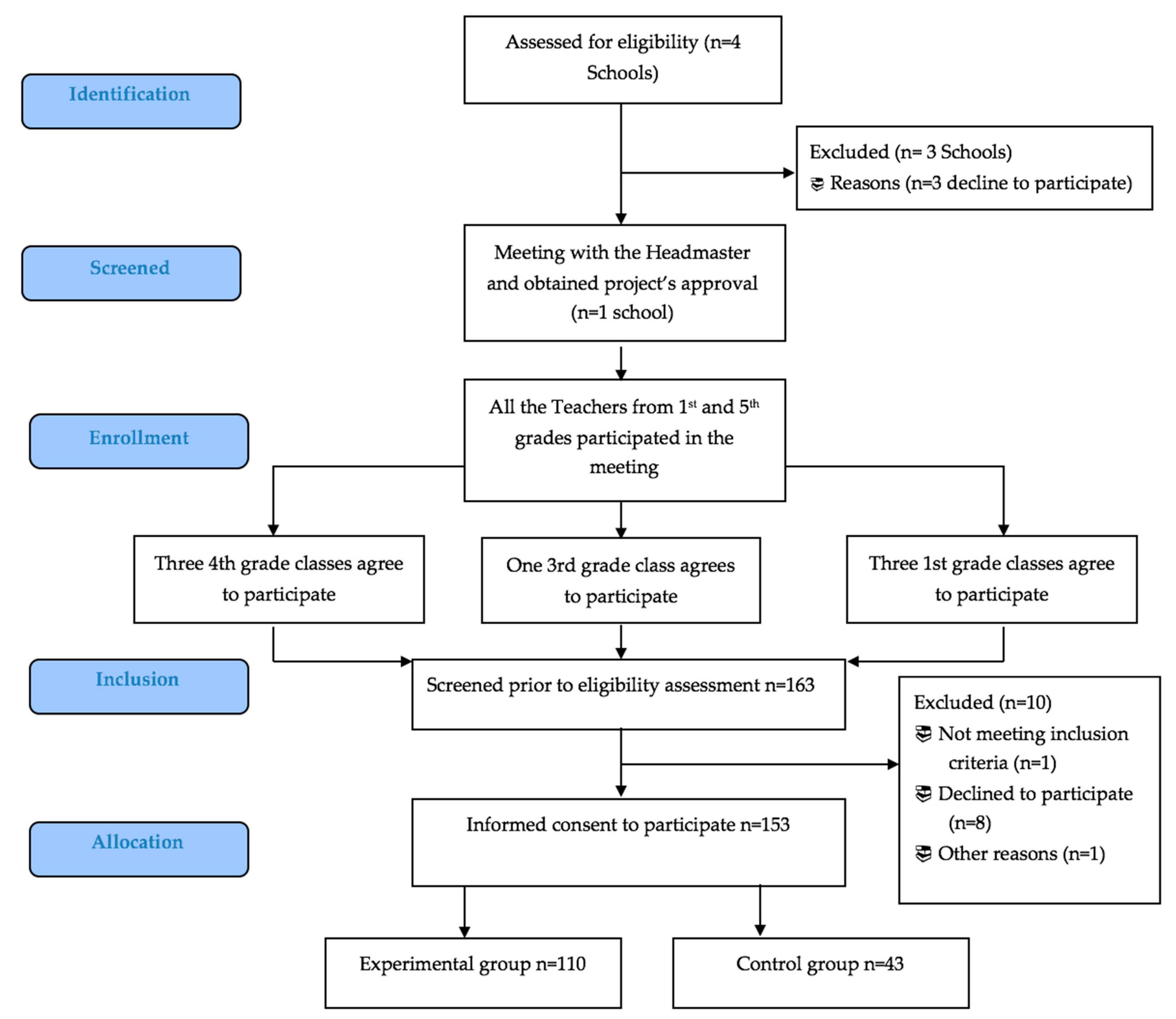
2.2. School and Participant Recruitment
2.3. Sample Size
2.4. Intervention
2.5. Data Collection and Outcome Measures
2.5.1. PA and Sedentary Behavior
2.5.2. Health-Related Fitness
2.5.3. Motor Control Development During Fine and Gross (Locomotor) Tasks
2.5.4. Dietary Patterns
2.5.5. Anthropometric Evaluation
2.5.6. Sociodemographic Determinants.
2.5.7. Cognitive Function
2.5.8. Time-On-Task Behavior
2.5.9. Quality of Life (HRQoL)
2.5.10. Process Evaluation of Children and Teachers
2.6. Data Analysis
2.6.1. Quantitative Analysis
2.6.2. Qualitative Analysis
2.7. Harmonization and Standardization
2.8. Dissemination of Project Findings
3. Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- Knowing their attitude concerning physical activity in general;
- Knowing their attitude in respect of the practice of active breaks;
- Knowing if something has changed in their attitude with respect to active breaks after having practiced them for all the intervention period.
- Factors related to us (barriers, limitations and points of strength. For example: a lack of personal skills, low trust and confidence in the proposed intervention);
- Factors related to children (such as difficulties in handling them and fear of accidents);
- Factors related to the environment (availability of space, inadequacy of space and not very stimulating exercises).
Appendix B
- Knowing their attitude concerning physical activity in general and sport practiced;
- Knowing their attitude in respect of the practice of active breaks;
- Knowing if something has changed in their attitude toward physical activity after having practiced active breaks for all the intervention period.
- Factors related to active breaks protocol (barriers, limitations and points of strength. For example: a lack of fun and uninvolving games);
- Factors related to themself (such as difficulties in interacting with other children and difficulties in managing the times of active breaks);
- Factors related to the environment (small classroom’s space and too much noise).
References
- Eime, R.M.; Young, J.A.; Harvey, J.T.; Charity, M.J.; Payne, W.R. A systematic review of the psychological and social benefits of participation in sport for children and adolescents: Informing development of a conceptual model of health through sport. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 135. [Google Scholar] [CrossRef] [Green Version]
- Longmuir, P.E.; Colley, R.C.; Wherley, V.A.; Tremblay, M.S. Canadian society for exercise physiology position stand: Benefit and risk for promoting childhood physical activity. Appl. Physiol. Nutr. Metab. 2014, 39, 1271–1279. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Recommendations on Physical Activity for Health. 2010. Available online: http://whqlibdoc.who.int/publications/2010/9789241599979_eng.pdf (accessed on 18 August 2020).
- Rowlands, A.V. Physical activity, inactivity, and health during youth. Pediatr. Exerc. Sci. 2016, 28, 19–22. [Google Scholar] [CrossRef] [Green Version]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Hubbard, K.; Economos, C.D.; Bakun, P.; Boulos, R.; Chui, K.; Mueller, M.P.; Smith, K.; Sacheck, J. Disparities in moderate to vigorous physical activity among girls and overweight and obese schoolchildren during school and out of school time. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 39. [Google Scholar] [CrossRef] [Green Version]
- Konstabel, K.; Veidebaum, T.; Verbestel, V.; Moreno, L.A.; Bammann, K.; Tornaritis, M.; Eiben, G.; Molnár, D.; Siani, A.; Sprengeler, O.; et al. Objectively measured physical activity in European children: The IDEFICS study. Int. J. Obes. 2014, 38, S135–S143. [Google Scholar] [CrossRef] [Green Version]
- Pate, R.R.; O′Neill, J.R. Summary of the American Heart Association scientific statement: Promoting physical activity in children and youth: A leadership role for schools. J. Cardiovasc. Nurs. 2008, 23, 44–49. [Google Scholar] [CrossRef]
- Cassar, S.; Salmon, J.; Timperio, A.; Naylor, P.J.; Van Nassau, F.; Contardo Ayala, A.M.; Koorts, H. Adoption, implementation and sustainability of school-based physical activity and sedentary behaviour interventions in real-world settings: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Love, R.; Adams, J.; van Sluijs, E.M.F. Are school-based physical activity interventions effective and equitable? A meta-analysis of cluster randomized controlled trials with accelerometer-assessed activity. Obes. Rev. 2019, 20, 859–870. [Google Scholar] [CrossRef]
- Vitali, F.; Robazza, C.; Bortoli, L.; Bertinato, L.; Schena, F.; Lanza, M. Enhancing fitness, enjoyment, and physical self-efficacy in primary school children: A DEDIPAC naturalistic study. PeerJ 2019, 7, e6436. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. School health guidelines to promote healthy eating and physical activity. Morb. Mortal. Wkly. Rep. 2011, 60, 1–71. [Google Scholar]
- Grao-Cruces, A.; Sánchez-Oliva, D.; Padilla-Moledo, C.; Izquierdo-Gómez, R.; Cabanas-Sánchez, V.; Castro-Piñero, J. Changes in the school and non-school sedentary time in youth: The up&down longitudinal study. J. Sports Sci. 2020, 38, 780–786. [Google Scholar] [CrossRef]
- van Stralen, M.M.; Yıldırım, M.; Wulp, A.; Te Velde, S.J.; Verloigne, M.; Doessegger, A.; Chinapaw, M.J.M. Measured sedentary time and physical activity during the school day of European 10-to 12-year-old children: The energy project. J. Sci. Med. Sport 2014, 17, 201–206. [Google Scholar] [CrossRef]
- Murtagh, E.; Mulvihill, M.; Markey, O. Bizzy break! The effect of a classroom-based activity break on in-school physical activity levels of primary school children. Pediatr. Exerc. Sci. 2013, 25, 300–307. [Google Scholar] [CrossRef] [Green Version]
- Drummy, C.; Murtagh, E.M.; McKee, D.P.; Breslin, G.; Davison, G.W.; Murphy, M.H. The effect of a classroom activity break on physical activity levels and adiposity in primary school children. J. Paediatr. Child Health 2016, 52, 745–749. [Google Scholar] [CrossRef]
- Masini, A.; Marini, S.; Gori, D.; Leoni, E.; Rochira, A.; Dallolio, L. Evaluation of school-based interventions of active breaks in primary schools: A systematic review and meta-analysis. J. Sci. Med. Sport 2020, 23, 377–384. [Google Scholar] [CrossRef]
- Erwin, H.E.; Beighle, A.; Morgan, C.F.; Noland, M. Effect of a low-cost, teacher-directed classroom 16 intervention on elementary students′ physical activity. J. Sch. Health 2011, 81, 455–461. [Google Scholar] [CrossRef]
- Calella, P.; Mancusi, C.; Pecoraro, P.; Sensi, S.; Sorrentino, C.; Imoletti, M.; Franzese, A.; Gallè, F.; Liguori, G.; Valerio, G. Classroom active breaks: A feasibility study in Southern Italy. Health Promot. Int. 2019, 35, 373–380. [Google Scholar] [CrossRef]
- Cook, T.D.; Campbell, O.T. Quasi-Experimentation; Rand McNally: Chigaco, IL, USA, 1979. [Google Scholar]
- Masini, A.; Marini, S.; Leoni, E.; Lorusso, G.; Toselli, S.; Tessari, A.; Ceciliani, A.; Dallolio, L. Active breaks: A pilot and feasibility study to evaluate the effectiveness of physical activity levels in a school based intervention in an Italian primary school. Int. J. Environ. Res. Public Health 2020, 17, 4351. [Google Scholar] [CrossRef]
- Watson, A.J.L.; Timperio, A.; Brown, H.; Best, K.; Hesketh, K.D. Effect of classroom-based physical activity interventions on academic and physical activity outcomes: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 114. [Google Scholar] [CrossRef] [Green Version]
- Mavilidi, M.F.; Drew, R.; Morgan, P.J.; Lubans, R.D.; Schmidt, M.; Riley, N. Effects of different types of classroom physical activity breaks on children′s on-task behavior, academic achievement and cognition. Acta Paediatr. 2019, 109, 158–165. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, J.; Ottoboni, G.; Tessari, A.; Setti, A. One bout of open skill exercise improves cross-modal perception and immediate memory in healthy older adults who habitually exercise. PLoS ONE 2017, 12, e0178739. [Google Scholar] [CrossRef] [Green Version]
- Pesce, C.; Crova, C.; Cereatti, L.; Casella, R.; Bellucci, M. Physical activity and mental performance in preadolescents: Effects of acute exercise on free-recall memory. Ment. Health Phys. Act. 2009, 2, 16–22. [Google Scholar] [CrossRef]
- Roig, M.; Nordbrandt, S.; Geertsen, S.S.; Nielsen, J.B. The effects of cardiovascular exercise on human memory: A review with meta-analysis. Neurosci. Biobehav. Rev. 2013, 37, 1645–1666. [Google Scholar] [CrossRef]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle-Nyström, C.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer data collection and processing criteria to assess physical activity and other outcomes: A systematic review and practical considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Masse, L.C.; Tilert, T. McDowell, M. Physical activity in the United States measured by accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef]
- Colley, R.; Gorber, S.C.; Tremblay, M.S. Quality control and data reduction procedures for accelerometry-derived measures of physical activity. Health Rep. 2010, 21, 63–69. [Google Scholar]
- Ortega, F.B.; Konstabel, K.; Pasquali, E.; Ruiz, J.R.; Hurtig-Wennlof, A.; Maestu, J.; Lof, M.; Harro, J.; Bellocco, R.; Labayen, I.; et al. Objectively measured physical activity and sedentary time during childhood, adolescence and young adulthood: A cohort study. PLoS ONE 2013, 8, e60871. [Google Scholar] [CrossRef] [Green Version]
- Rich, C.; Geraci, M.; Griffiths, L.; Sera, F.; Dezateux, C.; Cortina-Borja, M. quality control methods in accelerometer data processing: Identifying extreme counts. PLoS ONE 2014, 9, e85134. [Google Scholar] [CrossRef]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef]
- Gobbi, E.; Ferri, I.; Carraro, A. A contribution to the Italian validation of the Physical Activity Questionnaire for Children (PAQ-C). Sport Sci. Health 2012, 8, 63. [Google Scholar] [CrossRef] [Green Version]
- Ayan, C.; Cancela, M.J.; Romero, S.; Alonso, S. Reliability of two field-based tests for Measuring cardiorespiratory fitness in preschool children. J. Strength Cond. Res. 2015, 29, 2874–2880. [Google Scholar] [CrossRef] [PubMed]
- Bolonchuk, W.W. The Accuracy of the Six Minute Run Test to Measure Cardiorespiratory Fitness; North Dakota University: Grand Forks, ND, USA, 1975. [Google Scholar]
- American Thoracic Society. American thoracic society statement: guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Geiger, R.; Strasak, A.; Treml, B.; Gasser, K.; Leinsasser, A.; Fischer, V.; Geiger, H.; Loeckinger, A.; Stein, J.I. Six-minute walk test in children and adolescent. J. Pediatr. 2007, 150, 395–399. [Google Scholar] [CrossRef]
- Lammers, A.E.; Hislop, A.A.; Flynn, Y.; Haworth, S.G. The 6-minuts walk test: Normal values for children o 4–11 years of age. Arch. Dis. Child. 2008, 93, 464–468. [Google Scholar] [CrossRef]
- Secchia, J.D.; Magister, G.G.C.; España-Romeroc, V.; Castro-Piñero, J. Physical fitness and future cardiovascular risk in argentine children and adolescents: An introduction to the ALPHA test battery. Arch. Argent. Pediatr. 2014, 112, 132–140. [Google Scholar] [CrossRef]
- Castro-Piñero, J.; Ortega, F.B.; Artero, E.G.; Girela-Rejón, M.J.; Mora, J.; Sjöström, M.; Ruiz, J.R. Assessing muscular strength in youth: Usefulness of standing long jump as a general index of muscular fitness. J. Strength Cond. Res. 2010, 24, 1810–1817. [Google Scholar] [CrossRef] [PubMed]
- Harre, D. The Principles of Sports Training: Introduction to the Theory and Methods of Training; Sportverlag: Berlin, Germany, 1982. [Google Scholar]
- Bonaccorsi, A. Manuale di standardizzazione dei test. In Osservatorio Nazionale Capacità Motorie; CONI: Roma, Italy, 2001. [Google Scholar]
- Chiodera, P.; Volta, E.; Gobbi, G.; Milioli, M.A.; Mirandola, P.; Bonetti, A.; Delsignore, R.; Bernasconi, S.; Anedda, A.; Vitale, M. Specifically designed physical exercise programs improve children’s motor abilities. Scand. J. Med. Sci. Sport 2008, 18, 179–187. [Google Scholar] [CrossRef]
- Čillík, I.; Kollár, R.; Kremnický, J.; Pivovarniček, P.; Mandzáková, M. The level of general physical performance and physical development of 7 and 10-year-old boys and girls. J. Hum. Sport Exerc. 2015, 10. [Google Scholar] [CrossRef] [Green Version]
- Bisi, M.C.; Tamburini, P.; Panebianco, G.P.; Stagni, R. Nonlinear analysis of human movement dynamics offers new insights in the development of motor control during childhood. J. Biomech. Eng. 2018. [Google Scholar] [CrossRef]
- Bisi, M.C.; Tamburini, P.; Stagni, R.A. ‘Fingerprint’ of locomotor maturation: Motor development descriptors, reference development bands and data-set. Gait Posture 2019, 68, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Leversen, J.S.; Haga, M.; Sigmundsson, H. From children to adults: Motor performance across the life-span. PLoS ONE 2012, 7, e38830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roccaldo, R.; Censi, L.; D′Addezio, L.; Toti, E.; Martone, D.; D’Addesa, D.; Cernigliaro, A. ZOOM8 study group adherence to the mediterranean diet in Italian school children (The ZOOM8 Study). Int. J. Food. Sci. Nutr. 2014, 65, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Willet, W. Food-frequency methods. In Nutritional Epidemiology, 2nd ed.; Oxford University Press: New York, NY, USA, 1998. [Google Scholar]
- Martone, D.; Roccaldo, R.; Censi, L.; Toti, E.; Catasta, G.; D’Addesa, D.; Carletti, C. ZOOM8 Study group. food consumption and nutrient intake in Italian school children: Results of the ZOOM8 study. Int. J. Food Sci. Nutr. 2013, 64, 700–705. [Google Scholar] [CrossRef]
- Weiner, J.S.; Lourie, J.A. Practical Human Biology; Academic Press: Cambridge, MA, USA, 1981; ISBN 0127419608. [Google Scholar]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champain, IL, USA, 1998. [Google Scholar]
- Frisancho, A.R. Anthropometric Standards: An Interactive Nutritional Reference of Body Size and Body Composition for Children and Adults; University of Michigan Press: Ann Arbor, MI, USA, 2008; ISBN 9780472115914. [Google Scholar]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- Cole, T.J.; Flegal, K.M.; Nicholls, D.; Jackson, A.A. Body mass index cut offs to define thinness in children and adolescents: International survey. Br. Med. J. 2007, 335, 194–197. [Google Scholar] [CrossRef] [Green Version]
- Ashwell, M.; Hsieh, S.D. Six reasons why the waist-to-height ratio is a rapid and effective global indicator for health risks of obesity and how its use could simplify the international public health message on obesity. Int. J. Food Sci. Nutr. 2005, 56, 303–307. [Google Scholar] [CrossRef]
- Maffeis, C.; Banzato, C.; Talamini, G. Waist-to-height ratio, a useful index to identify high metabolic risk in overweight children. J. Pediatr. 2008, 152, 207–213. [Google Scholar] [CrossRef]
- McCarthy, H.D.; Ashwell, M. A study of central fatness using waist-to-height ratios in UK children and adolescents over two decades supports the simple message ‘Keep your waist circumference to less than half your height’. Int. J. Obes. 2006, 30, 988–992. [Google Scholar] [CrossRef] [Green Version]
- Slaughter, M.H.; Lohman, T.G.; Boileau, R.A.; Horswill, C.A.; Stillman, R.J.; Van Loan, M.D.; Bemben, D.A. Skinfold equations for estimation of body fatness in children and youth. Hum. Biol. 1988, 60, 709–723. [Google Scholar]
- Laurson, K.R.; Eisenmann, J.C.; Welk, G.J. Body fat percentile curves for US children and adolescents. Am. J. Prev. Med. 2011, 41, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Grizzle, R. Wechsler intelligence scale for children fourth edition. In Encyclopedia of Child Behavior and Development; Goldstein, S., Naglieri, J.A., Eds.; Springer: Boston, MA, USA, 2011; pp. 1553–1555. [Google Scholar] [CrossRef]
- Shams, L.; Kamitani, Y.; Shimojo, S. What you see is what you hear. Nature 2000, 408, 788. [Google Scholar] [CrossRef] [PubMed]
- Shams, L.; Kamitani, Y.; Shimojo, S. A visual illusion induced by sound. Cogn. Brain Res. 2002, 14, 147–152. [Google Scholar] [CrossRef]
- Innes-Brown, H.; Barutchu, A.; Shivdasani, M.N.; Crewther, D.P.; Grayden, D.B.; Paolini, A.G. Susceptibility to the flash-beep illusion is increased in children compared to adults. Dev. Sci. 2011, 14, 1089–1099. [Google Scholar] [CrossRef] [PubMed]
- Nava, E.; Pavani, F. Changes insensory dominance during childhood: Converging evidence from the colavita effect and the sound-induced flash illusion. Child Dev. 2013, 84, 604–616. [Google Scholar] [CrossRef]
- Tremblay, C.; Champoux, F.; Voss, P.; Bacon, B.A.; Lepore, F.; Théoret, H. Speech and non-speech audio-visual illusions: A developmental study. PLoS ONE 2007, 2, e742. [Google Scholar] [CrossRef] [Green Version]
- Varni, J.W.; Seid, M.; Kurtin, P.S. PedsQL 4.0: Reliability and validity of the pediatric quality of life inventory version 4.0 generic core scales in healthy and patient populations. Med. Care 2001, 39, 800–812. [Google Scholar] [CrossRef]
- Sandelowski, M. Using qualitative research. Qual. Health Res. 2004, 14, 1366–1386. [Google Scholar] [CrossRef]
- Huston, P.; Rowan, M. Qualitative studies: Their role in medical research. Can. Fam. Physician 1998, 44, 2453–2458. [Google Scholar]
- Glaser, B.G.; Strauss, A.L. The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine: Chicago, IL, USA, 1967. [Google Scholar]
- Ministero della Salute, Direzione Generale della Prevenzione sSanitaria. Linee Di Indirizzo Sull’attività Fisica per Le Differenti Fasce D’età E Con Riferimento a Situazioni Fisiologiche E Fisiopatologiche E a Sottogruppi Specifici Di Popolazione; Ministero Della Salute: Rome, Italy, 2019. Available online: http://www.salute.gov.it/imgs/C_17_ pubblicazioni_2828_allegato.pdf (accessed on 18 August 2020).
- Nardone, P.; Spinelli, A.; Buoncristiano, M.; Lauria, L.; Pierannunzio, D.; Galeone, D. Il Sistema di sorveglianza OKkio alla SALUTE: Risultati 2016. 2018. Available online: https://www.epicentro.iss.it/okkioallasalute/pdf/ONLINE_OKKIO_ALLA_SALUTE.pdf (accessed on 18 August 2020).
- Sacchetti, R.; Ceciliani, A.; Garulli, A.; Masotti, A.; Poletti, G.; Beltrami, P.; Leoni, E. Physical fitness of primary school children in relation to overweight prevalence and physical activity habits. J. Sports Sci. 2012, 30, 633–640. [Google Scholar] [CrossRef]
- Sacchetti, R.; Ceciliani, A.; Garulli, A.; Dallolio, L.; Beltrami, P.; Leoni, E. Effects of a 2-year school-based intervention of enhanced physical education in the primary school. J. Sch. Health 2013, 83, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Dallolio, L.; Ceciliani, A.; Sanna, T.; Garulli, A.; Leoni, E. Proposal for an enhanced physical education program in the primary school: evaluation of feasibility and effectiveness in improving physical skills and fitness. J. Phys. Act. Health 2016, 13, 1025–1034. [Google Scholar] [CrossRef] [PubMed]
- Wassenaar, T.M.; Williamson, W.; Johansen-Berg, H.; Dawes, H.; Roberts, N.; Foster, C.; Sexton, C.E. A critical evaluation of systematic reviews assessing the effect of chronic physical activity on academic achievement, cognition and the brain in children and adolescents: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 79. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Phase | Aim | Examples of the Type of Exercises | Duration |
|---|---|---|---|
| Warm-up | Cardiorespiratory and mobility exercises | “The chair march”: The children all stand up and move their chairs sideways, waiting for the teacher’s commands. They begin to march, raising their knees well and resting their toes on the chair, without pushing upwards. Progressively, they also combine the movement of the legs with the alternating movement of the arms. | 2 min |
| Tone-up | High-intensity interval training (HIIT) exercises | HIIT Animal jumps: Children scattered around the classroom have to jump like frogs for 40 s then rest for 20 s and repeat the exercise 2 times, then they jump like kangaroos for 40 s with 20 s break to be performed 2 times. | 5 min |
| Cool-down | Breath and relaxation exercises | The imaginary balloon: Children must inflate an imaginary balloon by inhaling and exhaling, mimicking the progressive expansion of the balloon with the widening of their arms. We ask for a very slow and long exhalation twice as long as the inspiration. | 3 min |
| Outcome Measures | Baseline October 2019 (T0) | Mid-Intervention October 2020 (T1) | End of Intervention June 2021 (T2) | 6 Months After End of Intervention December 2021 (T3) |
|---|---|---|---|---|
| Personal information (Age, Country) | √ | √ | ||
| PA and sedentary behavior (accelerometer) | √ | √ | √ | |
| Total reported physical activity Questionnaire | √ | √ | √ | |
| Health related fitness | √ | √ | √ | |
| Motor control development | √ | √ | √ | |
| Dietary patterns | √ | √ | √ | |
| Anthropometric evaluation | √ | √ | √ | |
| Sociodemographic and early determinants | √ | √ | ||
| Cognitive Function | √ | √ | √ | |
| Time-on-task behavior (Teachers and children self-administrated questionnaire) | √ | √ | ||
| Quality of Life | √ | √ | √ | |
| Process evaluation focus group with children | √ | |||
| Process evaluation: focus group with teachers | √ |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masini, A.; Lanari, M.; Marini, S.; Tessari, A.; Toselli, S.; Stagni, R.; Bisi, M.C.; Bragonzoni, L.; Gori, D.; Sansavini, A.; et al. A Multiple Targeted Research Protocol for a Quasi-Experimental Trial in Primary School Children Based on an Active Break Intervention: The Imola Active Breaks (I-MOVE) Study. Int. J. Environ. Res. Public Health 2020, 17, 6123. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176123
Masini A, Lanari M, Marini S, Tessari A, Toselli S, Stagni R, Bisi MC, Bragonzoni L, Gori D, Sansavini A, et al. A Multiple Targeted Research Protocol for a Quasi-Experimental Trial in Primary School Children Based on an Active Break Intervention: The Imola Active Breaks (I-MOVE) Study. International Journal of Environmental Research and Public Health. 2020; 17(17):6123. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176123
Chicago/Turabian StyleMasini, Alice, Marcello Lanari, Sofia Marini, Alessia Tessari, Stefania Toselli, Rita Stagni, Maria Cristina Bisi, Laura Bragonzoni, Davide Gori, Alessandra Sansavini, and et al. 2020. "A Multiple Targeted Research Protocol for a Quasi-Experimental Trial in Primary School Children Based on an Active Break Intervention: The Imola Active Breaks (I-MOVE) Study" International Journal of Environmental Research and Public Health 17, no. 17: 6123. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17176123