Older Aboriginal Australians’ Health Concerns and Preferences for Healthy Ageing Programs

 , , and
, , and
Abstract
:1. Introduction
1.1. The Significance of Community Collaboration
1.2. Technology as a Platform for Program Delivery
1.3. Study Aims
2. Materials and Methods
2.1. Participant Recruitment
2.2. Data Collection
- perceived susceptibility and severity of various health conditions,
- perceived benefits of and barriers to participation in healthy ageing programs,
- proposed strategies to activate readiness to adopt such programs,
- receptiveness to technology.
2.3. Data Analysis
2.4. Ethics Statement
2.5. Data Availability
3. Results
3.1. Perceived Health Concerns
3.1.1. Physical Health
Chronic Diseases
Dementia
Falls and Mobility
3.1.2. Social and Emotional Well-Being
Isolation and Loneliness
Grief and Loss
Health Issues Go Underground
3.1.3. Access to Healthcare Services
3.2. Participation in Current Health Programs
3.3. Strategies to Activate Readiness to Adopt Healthy Ageing Programs
3.3.1. Culturally Safe Care
Aboriginal-Specific Program
Aboriginal or Culturally Responsive Staff
Accessible and Culturally Secure Location
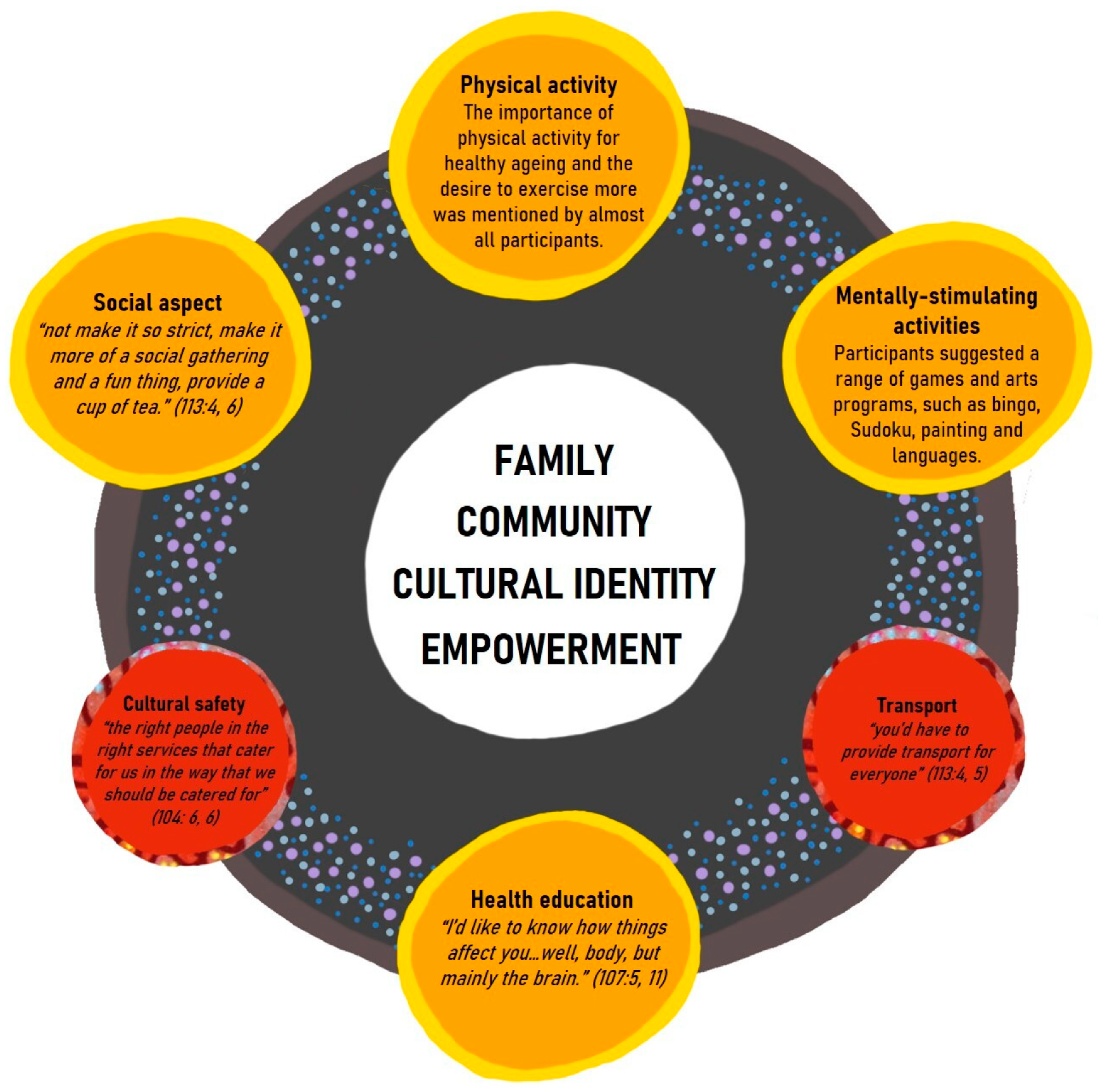
3.3.2. A Holistic Program
Family and Community
Empowerment Regarding Ageing Well
3.4. Technology
4. Discussion
4.1. A Co-Designed Healthy Ageing Program
4.2. Cultural Safety
4.3. Family, Community, and Cultural Identity
4.4. A Holistic Healthy Ageing Program
4.5. Cognitive Training
4.6. Cultural and Social Connectivity
4.7. Health Education and Empowerment
4.8. Using Technology to Deliver a Healthy Ageing Program
4.9. Study Limitations and Suggestions for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Australian Bureau of Statistics: Census of Population and Housing: Reflecting Australia—Stories from the Census, 2016, Cat. No. 2071.0. Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/productsbyCatalogue/732591A428CF1315CA2581BE0013BBED?OpenDocument (accessed on 7 October 2019).
- Australia Institute of Health and Welfare: Deaths in Australia. Canberra: Australia Institute of Health and Welfare, Cat. No. PHE 229. Available online: https://www.aihw.gov.au/reports/life-expectancy-death/deaths-in-australia (accessed on 7 October 2019).
- Randall, D.A.; Lujic, S.; Havard, A.; Eades, S.; Jorm, L. Multimorbidity among Aboriginal people in New South Wales contributes significantly to their higher mortality. Med. J. Aust. 2018, 209, 19–23. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics: Estimates and Projections, Aboriginal and Torres Strait Islander Australians, 2001 to 2026, Cat. No. 3238.0. Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/Lookup/3238.0Main+Features12001%20to%202026?OpenDocument (accessed on 7 October 2019).
- National Aboriginal Health Strategy Working Party. A National Aboriginal Health Strategy; National Aboriginal Health Strategy Working Party: Canberra, Australia, 1989. [Google Scholar]
- Broe, G.; Radford, K. Multimorbidity in Aboriginal and non-Aboriginal people. Med. J. Aust. 2018, 209, 16–17. [Google Scholar] [CrossRef] [PubMed]
- Marmot, M. Social determinants and the health of Indigenous Australians. Med. J. Aust. 2011, 194, 512–513. [Google Scholar] [CrossRef] [PubMed]
- Australia Institute of Health and Welfare: Australia’s Welfare 2017, Cat. No. AUS 214. Available online: https://www.aihw.gov.au/reports/australias-welfare/australias-welfare-2017 (accessed on 7 October 2019).
- Australian Health Ministers’ Advisory Council: Aboriginal and Torres Strait Islander Health Performance Framework 2017 Report. Available online: https://www.niaa.gov.au/sites/default/files/publications/2017-health-performance-framework-report_1.pdf (accessed on 7 October 2019).
- Rosier, K.; McDonald, M. The Relationship between Transport and Disadvantage in Australia; CAFCA: Melbourne, Australia, 2011; Volume 10. [Google Scholar]
- King, M.; Smith, A.; Gracey, M. Indigenous health part 2: The underlying causes of the health gap. Lancet 2009, 374, 76–85. [Google Scholar] [CrossRef]
- Kingsley, J.; Townsend, M.; Henderson-Wilson, C.; Bolam, B. Developing an exploratory framework linking Australian Aboriginal peoples’ connection to country and concepts of wellbeing. Int. J. Environ. Res. Public Health 2013, 10, 678–698. [Google Scholar] [CrossRef] [PubMed]
- Australia Institute of Health and Welfare: The Health and Welfare of Australia’s Aboriginal and Torres Strait Islander Peoples: 2015, Cat. No. IHW 147. Available online: https://www.aihw.gov.au/reports/indigenous-health-welfare/indigenous-health-welfare-2015 (accessed on 7 October 2019).
- Dance, P.; Brown, R.; Bammer, G.; Sibthorpe, B. Aged care services for Indigenous people in the Australian Capital Territory and surrounds: Analysing needs and implementing change. Aust. N. Z. J. Public Health 2004, 28, 579–583. [Google Scholar] [CrossRef] [Green Version]
- Shahid, S.; Finn, L.D.; Thompson, S.C. Barriers to participation of Aboriginal people in cancer care: Communication in the hospital setting. Med. J. Aust. 2009, 190, 574–579. [Google Scholar] [CrossRef]
- Durey, A.; McEvoy, S.P.; Swift-Otero, V.; Taylor, K.P.; Katzenellenbogen, J.M.; Bessarab, D. Improving healthcare for Aboriginal Australians through effective engagement between community and health services. BMC Health Serv. Res. 2016, 16, 224. [Google Scholar] [CrossRef] [Green Version]
- Waugh, E.; MacKenzie, L. Ageing well from an urban Indigenous Australian perspective. Aust. Occup. Ther. J. 2011, 58, 25–33. [Google Scholar] [CrossRef]
- Warburton, J.; Chambers, B. Older indigenous Australians: Their integral role in culture and community. Australas. J. Ageing 2007, 26, 3–7. [Google Scholar] [CrossRef]
- Coombes, J.; Lukaszyk, C.; Sherrington, C.; Keay, L.; Tiedemann, A.; Moore, R.; Ivers, R.Q. First Nation Elders’ perspectives on healthy ageing in NSW, Australia. Aust. N. Z. J. Public Health 2018, 42, 361–364. [Google Scholar] [CrossRef] [PubMed]
- Ottmann, G. Exploring community-based aged care with Aboriginal elders in three regional and remote Australian communities: A qualitative study. Soc. Work Policy Stud. Soc. Justice Pract. Theory 2018, 1, 1–26. [Google Scholar]
- Dimer, L.; Dowling, T.; Jones, J.; Cheetham, C.; Thomas, T.; Smith, J.; McManus, A.; Maiorana, A.J. Build it and they will come: Outcomes from a successful cardiac rehabilitation program at an Aboriginal medical service. Aust. Health Rev. 2013, 37, 79–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lukaszyk, C.; Coombes, J.; Sherrington, C.; Tiedemann, A.; Keay, L.; MacKean, T.; Clemson, L.; Cumming, R.; Broe, T.; Ivers, R.Q. The Ironbark program: Implementation and impact of a community-based fall prevention pilot program for older Aboriginal and Torres Strait Islander people. Health Promot. J. Aust. 2017, 29, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Schutzer, K.A. Barriers and motivations to exercise in older adults. Prev. Med. 2004, 39, 1056–1061. [Google Scholar] [CrossRef] [PubMed]
- Riper, H.; Kramer, J.; Smit, F.; Conijn, B.; Schippers, G.; Cuijpers, P. Web-based self-help for problem drinkers: A pragmatic randomized trial. Addiction 2008, 103, 218–227. [Google Scholar] [CrossRef]
- Barak, A.; Klein, B.; Proudfoot, J.G. Defining internet-supported therapeutic interventions. Ann. Behav. Med. 2009, 38, 4–17. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics: The Health and Welfare of Australia’s Aboriginal and Torres Strait Islander Peoples, October 2010, Cat. No.: 4704.0. Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/39433889d406eeb9ca2570610019e9a5/84984cdbe0abb161ca2574390014e970!OpenDocument (accessed on 7 October 2019).
- Callinan, T. Remote Indigenous Australians Rely on Facebook to Stay in Touch. SBS National Indigenous Television. 2014. Available online: https://www.sbs.com.au/nitv/nitv-news/article/2014/08/26/remote-indigenous-australians-rely-facebook-stay-touch (accessed on 7 April 2019).
- Ormond-Parker, L.; Corn, A. Information technologies and Indigenous communities. Arch. Manuscr. 2019, 47, 1–2. [Google Scholar] [CrossRef]
- Povey, J.; Mills, P.P.J.R.; Dingwall, K.M.; Lowell, A.; Singer, J.; Rotumah, D.; Bennett-Levy, J.; Nagel, T.; Mohd-Sidik, S.; Davies, J. Acceptability of mental health apps for Aboriginal and Torres Strait Islander Australians: A qualitative study. J. Med. Internet Res. 2016, 18, 65. [Google Scholar] [CrossRef]
- Hunter, E.; Travers, H.; McCulloch, B. Bridging the information gap: IT and health in indigenous populations. Australas. Psychiatry 2003, 11, 51–56. [Google Scholar] [CrossRef]
- Noble, N.; Paul, C.; Carey, M.L.; Sanson-Fisher, R.W.; Blunden, S.; Stewart, J.; Conigrave, K.M. A cross-sectional survey assessing the acceptability and feasibility of self-report electronic data collection about health risks from patients attending an Aboriginal Community controlled health service. BMC Med. Inform. Decis. Mak. 2014, 14, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minkler, M. Using participatory action research to build healthy communities. Public Health Rep. 2000, 115, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Cornwall, A.; Jewkes, R. What is participatory research? Soc. Sci. Med. 1995, 41, 1667–1676. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care. 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harfield, S.; Pearson, O.; Morey, K.; Kite, E.; Canuto, K.; Glover, K.; Gomersall, J.; Carter, D.; Davy, C.; Aromataris, E.; et al. Assessing the quality of health research from an Indigenous perspective: The Aboriginal and Torres Strait Islander quality appraisal tool. BMC Med. Res. Methodol. 2020, 20, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Radford, K.; Mack, H.A.; Robertson, H.; Draper, B.; Chalkley, S.; Daylight, G.; Cumming, R.; Bennett, H.; Pulver, L.J.; Broe, G.A. The koori growing old well study: Investigating aging and dementia in urban Aboriginal Australians. Int. Psychogeriatr. 2014, 26, 1033–1043. [Google Scholar] [CrossRef]
- Harari, P.; Legge, K. Psychology and Health; Heinemann: Portsmouth, NH, USA, 2001. [Google Scholar]
- Glaser, B.G.; Strauss, A.L. The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine: New Brunswick, NJ, USA, 1967. [Google Scholar]
- Strauss, A.; Corbin, J. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory, 2nd ed.; Sage Publications Inc.: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Morse, J.M.; Barrett, M.; Mayan, M.; Olson, K.; Spiers, J. Verification strategies for establishing reliability and validity in qualitative research. Int. J. Qual. Methods 2002, 1, 13–22. [Google Scholar] [CrossRef]
- Denzin, N.; Lincoln, Y. The Landscape of Qualitative Research: Theories and Issues, 2nd ed.; Sage Publications: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Hampshire, W. DHANGUDE DUNGHUTTI BURRAI Welcomed to Dunghutti Land: Towards a Shared Understanding of Grief and Loss. Ph.D. Thesis, Southern Cross University, Lismore, NSW, Australia, 2011. [Google Scholar]
- Hayman, N.E.; White, N.E.; Spurling, G.K. Improving indigenous patients’ access to mainstream health services: The Inala experience. Med. J. Aust. 2009, 190, 604–606. [Google Scholar] [CrossRef]
- Liaw, S.T.; Yau, P.; Pyett, P.; Furler, J.S.; Burchill, M.; Rowley, K.; Kelaher, M. Successful chronic disease care for Aboriginal Australians requires cultural competence. Aust. N. Z. J. Public Health 2011, 35, 238–248. [Google Scholar] [CrossRef]
- Aspin, C.; Brown, N.; Jowsey, T.; Yen, L.; Leeder, S.R. Strategic approaches to enhanced health service delivery for Aboriginal and Torres Strait Islander people with chronic illness: A qualitative study. BMC Health Serv. Res. 2012, 12, 143. [Google Scholar] [CrossRef] [Green Version]
- Giudice, D.L. The health of older Aboriginal and Torres Strait Islander peoples. Australas. J. Ageing 2016, 35, 82–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isaacs, A.N.; Pyett, P.; Oakley-Browne, M.A.; Gruis, H.; Waples-Crowe, P. Barriers and facilitators to the utilization of adult mental health services by Australia’s Indigenous people: Seeking a way forward. Int. J. Ment. Health Nurs. 2010, 19, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Treloar, C.; Jackson, L.C.; Gray, R.; Newland, J.; Wilson, H.; Saunders, V.; Johnson, P.; Brener, L. Multiple stigmas, shame and historical trauma compound the experience of Aboriginal Australians living with hepatitis C. Health Sociol. Rev. 2016, 25, 18–32. [Google Scholar] [CrossRef]
- Shahid, S.; Finn, L.; Bessarab, D.; Thompson, S.C. Understanding, beliefs and perspectives of Aboriginal people in Western Australia about cancer and its impact on access to cancer services. BMC Health Serv. Res. 2009, 9, 132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohoar, S.; Butera, N.; Kennedy, E. Strengths of Australian Aboriginal Cultural Practices in Family Life and Child Rearing. Canberra: Australia Institute of Family Studies; 2014. CFCA Paper No. 25. Available online: https://aifs.gov.au/cfca/publications/strengths-australian-aboriginal-cultural-practices-fam (accessed on 21 November 2019).
- Sherwood, J.; Edwards, T. Decolonisation: A critical step for improving Aboriginal health. Contemp. Nurse 2006, 22, 178–190. [Google Scholar] [CrossRef]
- Radford, K.; Allan, W.; Donovan, T.; Delbaere, K.; Garvey, G.; Broe, G.A.; Daylight, G.; Anderson, M.; Timbery, A.; Sullivan, K.; et al. Sharing the Wisdom of Our Elders Final Report; Neuroscience Research Australia: Sydney, NSW, Australia, 2019. [Google Scholar]
- Smith, K.; Gilchrist, L.; Taylor, K.; Clinch, C.; Logiudice, D.; Edgill, P.; Ratcliffe, J.; Flicker, L.; Douglas, H.; Bradley, K.; et al. Good spirit, good life: A quality of life tool and framework for older Aboriginal peoples. Gerontologist 2020. [Google Scholar] [CrossRef]
- Genat, B.; Bushby, S.; McGuire, M.; Taylor, E.; Walley, Y.; Weston, T. Aboriginal Healthworkers: Primary Health Care at the Margins; University of West Australia Press: Perth, WA, Australia, 2006. [Google Scholar]
- Ware, V.-A. Supporting Healthy Communities through Arts Programs; Australia Institute of Health and Welfare: Canberra, Australia, 2014.
- Radford, K.; Mack, H.A.; Draper, B.; Chalkley, S.; Daylight, G.; Cumming, R.; Bennett, H.; Delbaere, K.; Broe, G.A. Prevalence of dementia in urban and regional Aboriginal Australians. Alzheimers Dement. 2015, 11, 271–279. [Google Scholar] [CrossRef] [Green Version]
- Martin, M.; Clare, L.; Altgassen, A.M.; Cameron, M.H.; Zehnder, F. Cognition-based interventions for healthy older people and people with mild cognitive impairment. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef]
- Smith, G.E.; Housen, P.; Yaffe, K.; Ruff, R.; Kennison, R.F.; Mahncke, H.W.; Zelinski, E.M. A cognitive training program based on principles of brain plasticity: Results from the improvement in memory with plasticity-based adaptive cognitive training (IMPACT) study. J. Am. Geriatr. Soc. 2009, 57, 594–603. [Google Scholar] [CrossRef] [Green Version]
- Scarmeas, N.; Luchsinger, J.A.; Schupf, N.; Brickman, A.M.; Cosentino, S.; Tang, M.X.; Stern, Y. Physical activity, diet, and risk of alzheimer disease. JAMA 2009, 302, 627–637. [Google Scholar] [CrossRef] [Green Version]
- Middleton, L.E.; Barnes, D.E.; Lui, L.-Y.; Yaffe, K. Physical activity over the life course and its association with cognitive performance and impairment in old age. J. Am. Geriatr. Soc. 2010, 58, 1322–1326. [Google Scholar] [CrossRef] [PubMed]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [Green Version]
- Marioni, R.E.; Proust-Lima, C.; Amieva, H.; Brayne, C.; Matthews, F.E.; Dartigues, J.-F.; Jacqmin-Gadda, H. Social activity, cognitive decline and dementia risk: A 20-year prospective cohort study. BMC Public Health 2015, 15, 1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahid, S.; Thompson, S.C. An overview of cancer and beliefs about the disease in Indigenous people of Australia, Canada, New Zealand and the US. Aust. New Zealand J. Public Health 2009, 33, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Giles, B.G.; Findlay, C.S.; Haas, G.; LaFrance, B.; Laughing, W.; Pembleton, S. Integrating conventional science and aboriginal perspectives on diabetes using fuzzy cognitive maps. Soc. Sci. Med. 2007, 64, 562–576. [Google Scholar] [CrossRef] [PubMed]
- Berkman, N.D.; Donahue, K.E.; Halpern, D.J.; Crotty, K.; Sheridan, S.L. Low health literacy and health outcomes: An updated systematic review. Ann. Intern. Med. 2011, 155, 97. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.M. Empowering patients: Issues and strategies. Soc. Sci. Med. 1996, 43, 697–705. [Google Scholar] [CrossRef]
- Chen, Y.-R.R.; Schulz, P.J.; Diviani, N.; Clemensen, J. The effect of information communication technology interventions on reducing social isolation in the elderly: A systematic review. J. Med. Internet Res. 2016, 18, e18. [Google Scholar] [CrossRef]
- Khosravi, P.; Rezvani, A.; Wiewiora, A. The impact of technology on older adults’ social isolation. Comput. Hum. Behav. 2016, 63, 594–603. [Google Scholar] [CrossRef]
- Ammann, R.; Vandelanotte, C.; de Vries, H.; Mummery, W.K. Can a website-delivered computer-tailored physical activity intervention be acceptable, usable, and effective for older people? Health Educ. Behav. 2013, 40, 160–170. [Google Scholar] [CrossRef]
- Irvine, M.A.B.; Gelatt, V.A.; Seeley, J.R.; Macfarlane, P.; Gau, J.M.; Davies, C.; Chen, G.; Langrial, S.; Stolte, E. Web-based intervention to promote physical activity by sedentary older adults: Randomized controlled trial. J. Med. Internet Res. 2013, 15, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silveira, P.; Van De Langenberg, R.; Reve, E.V.H.; Daniel, F.; Casati, F.; De Bruin, E.D.; Costabile, M.C.; Stanmore, E. Tablet-based strength-balance training to motivate and improve adherence to exercise in independently living older people: A phase II preclinical exploratory trial. J. Med. Internet Res. 2013, 15, 159. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Barriers | Enablers |
|---|---|
| Lack of programs “We got nothing here for older people” (Participant 104: 5, 14). | Flexibility of attendance “I have a choice. I can say one day, “I don’t feel like going” (Participant 113: 11, 1) |
| Unappealing programs Participants describe programs to be “boring” (Participant 106: 15, 6) (Participant 101: 21, 17), or are “too long” (Participant 111: 4, 11), or run by ineffectual staff who “need to lift their game” (Participant 106: 20, 18). | Social aspect “The camaraderie, they’re going to make you feel better in yourself. Health-wise, they can only help as well, but it’s just meeting and talking to everyone” (Participant 113: 10, 19). “It’s good fun…And you have a laugh and all that with them. And yeah, mainly just to get out the house for a couple of hours” (Participant 102: 40, 7). |
| Transport constraints Several participants noted that having to “find your own way” (Participant 111: 4, 16) or “getting someone to pick you up” (Participant 113: 12, 2) pose barriers. | Transport readily available They “always (have) transport” to programs (Participant 102: 41, 8) (Participant 112: 4, 19). “Transport around here is terrific” (Participant 101: 22, 8) |
| Shame or stigma associated with participation “Shame would be a big factor (barrier). Shame to admit that we ourselves are facing those crises within our lives. Shame of what the community may think about us.” (Participant 003: 5, 14) | |
| Disengagement associated with past experiences with programs or other program attendees. “I’ve seen it all, we’ve already been there and done that, tried to help, you know?” (Participant 110: 3, 1) “I want to find something better now than last time not with them–all them whinging and moaning all the time and they got everything.” (Participant 102: 38, 12) | |
| Sense of hopelessness or disempowerment regarding ageing well. Participants expressed feelings of hopelessness towards the challenges of ageing and were resigned to the inevitability of disease and poor prospects of old age. “We didn’t think it (growing old) was going to be so hard for us.” (Participant 104: 7, 4) “Well, you just live with it (chronic disease). What else can you do? You can’t do anything.” (Participant 110: 4, 18) Some suggested that health outcomes are a gamble, where taking better care of one’s health “doesn’t always pay off” (Participant 301: 3, 9). |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wettasinghe, P.M.; Allan, W.; Garvey, G.; Timbery, A.; Hoskins, S.; Veinovic, M.; Daylight, G.; Mack, H.A.; Minogue, C.; Donovan, T.; et al. Older Aboriginal Australians’ Health Concerns and Preferences for Healthy Ageing Programs. Int. J. Environ. Res. Public Health 2020, 17, 7390. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207390
Wettasinghe PM, Allan W, Garvey G, Timbery A, Hoskins S, Veinovic M, Daylight G, Mack HA, Minogue C, Donovan T, et al. Older Aboriginal Australians’ Health Concerns and Preferences for Healthy Ageing Programs. International Journal of Environmental Research and Public Health. 2020; 17(20):7390. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207390
Chicago/Turabian StyleWettasinghe, Pamela Ming, Wendy Allan, Gail Garvey, Alison Timbery, Sue Hoskins, Madeleine Veinovic, Gail Daylight, Holly A. Mack, Cecilia Minogue, Terrence Donovan, and et al. 2020. "Older Aboriginal Australians’ Health Concerns and Preferences for Healthy Ageing Programs" International Journal of Environmental Research and Public Health 17, no. 20: 7390. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17207390