COVID-19 Pandemic and Death Anxiety in Security Forces in Spain

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Objectives
2.2. Variables
2.2.1. Dependent Variable
2.2.2. Independent Variables
2.3. Participants
2.4. Procedure
3. Results
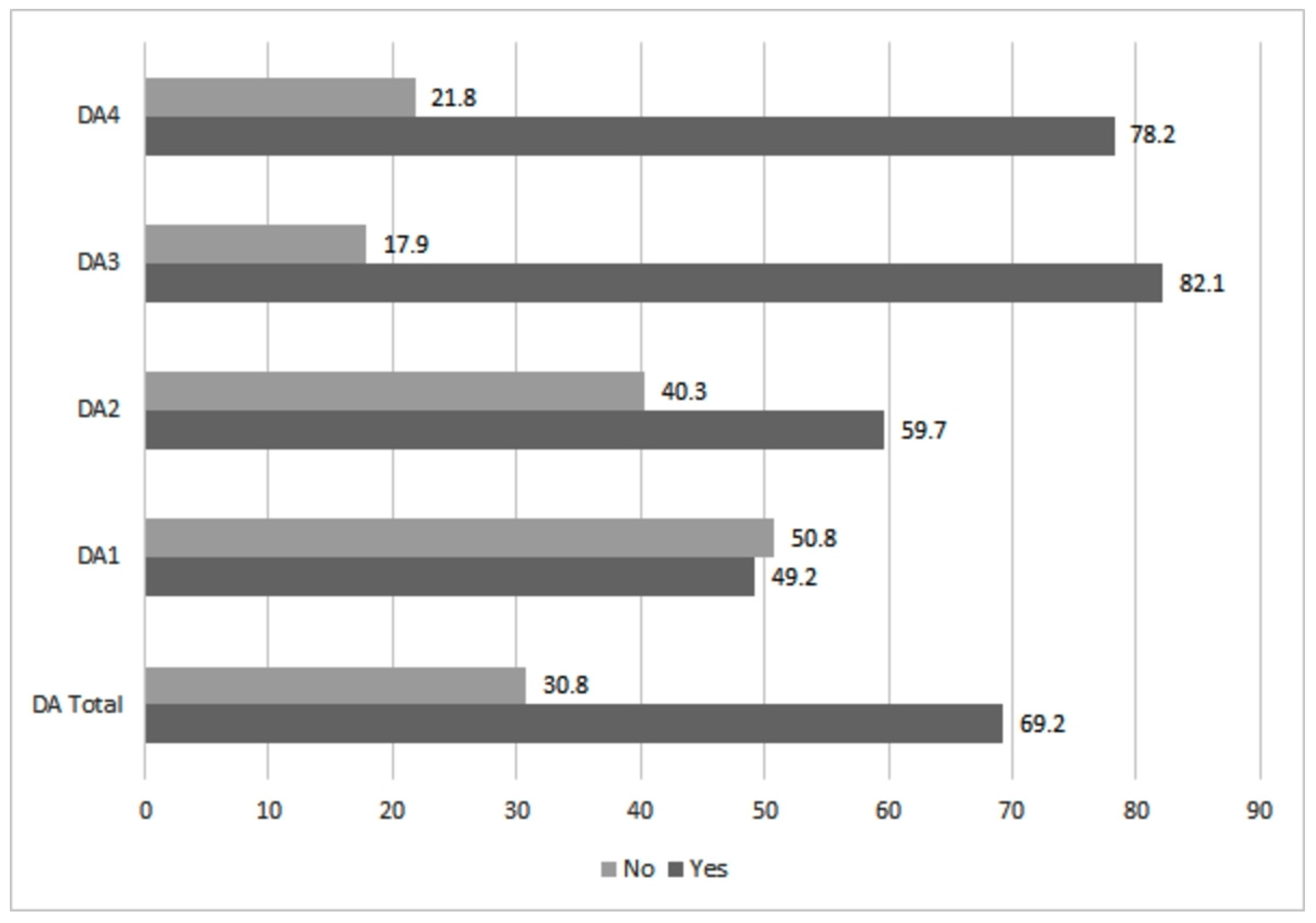
3.1. Descriptive Results of the Research
3.2. Predictive Variables in the Death Anxiety Phenomenon According to the Binary Logistic Regression Model
3.2.1. Fear of Death (DA1) Subscale
3.2.2. Fear of One’s Process of Dying (DA2) Subscale
3.2.3. Fear of Death of Others (DA3) Subscale
3.2.4. Fear of the Process of Dying of Others (DA4) Subscale
3.2.5. Death Anxiety Total
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pugliesi, K. The consequences of emotional labor: Effects on work stress, job satisfaction, and well-being. Motiv. Emot. 1999, 23, 125–154. [Google Scholar] [CrossRef]
- Hülsheger, U.R.; Schewe, A.F. On the costs and benefits of emotional labor: A meta-analysis of three decades of research. J. Occup. Health Psychol. 2011, 16, 361. [Google Scholar] [CrossRef]
- Bliese, P.D.; Edwards, J.R.; Sonnentag, S. Stress and well-being at work: A century of empirical trends reflecting theoretical and societal influences. J. Appl. Psychol. 2017, 102, 389. [Google Scholar] [CrossRef]
- Wong, E.; Tschan, F.; Semmer, N.K. Effort in emotion work and well-being: The role of goal attainment. Emotion 2017, 17, 67. [Google Scholar] [CrossRef]
- Kuroda, S.; Yamamoto, I. Why do people overwork at the risk of impairing mental health? J. Happiness Stud. 2019, 20, 1519–1538. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, N.; Docherty, M.; Gnanapragasam, S.; Wessely, S. Managing mental health challenges faced by healthcare workers during covid-19 pandemic. BMJ 2020, 368, m1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-López, J.Á.; Lázaro-Pérez, C.; Gómez-Galán, J.; Fernández-Martínez, M.M. Psychological impact of COVID-19 emergency on health professionals: Burnout incidence at the most critical period in Spain. J. Clin. Med. 2020, 9, 3029. [Google Scholar] [CrossRef]
- Gribble, R.; Connelly, V.; Fear, N. Living a life less ordinary: What UK military families can teach the families of essential workers responding to COVID-19. J. Mil. Veteran Fam. Health 2020. [Google Scholar] [CrossRef]
- Shimazu, A.; Nakata, A.; Nagata, T.; Arakawa, Y.; Kuroda, S.; Inamizu, N.; Yamamoto, I. Psychosocial impact of COVID-19 for general workers. J. Occup. Health 2020, 62, e12132. [Google Scholar] [CrossRef]
- Gómez Galán, J. The Black Death and other historical pandemics. Front. Sci. 2020, 7, 62–75. [Google Scholar]
- World Health Organization. Brote de Enfermedad Por Coronavirus (COVID-19). 2020. Available online: https://www.who.int/es/emergencies/diseases/novel-coronavirus-2019 (accessed on 19 September 2020).
- Ministerio de Sanidad. COVID-19 en España. 2020. Available online: https://cnecovid.isciii.es/ (accessed on 20 September 2020).
- Romero, J.M. Los Muertos de la Pandemia en España. El País. 26 July 2020. Available online: https://cutt.ly/yf9ZCAV (accessed on 9 September 2020).
- BOE. Real Decreto 463/2020, de 14 de marzo, por el que se Declara el Estado de Alarma Para la Gestión de la Situación de Crisis Sanitaria Ocasionada por el COVID-19. Available online: https://cutt.ly/nf9ZNDB (accessed on 23 September 2020).
- San Martín, M. Coronavirus y la neumonía de Wuhan: COVID-19. Front. Cienc. 2020, 7, 16–22. [Google Scholar]
- Ministerio de Sanidad. Procedimiento de Actuación para los Servicios de Prevención de Riesgos Laborales Frente a la Exposición al Nuevo Coronavirus (SARS-COV-2). 2020. Available online: https://url2.cl/NvBb4 (accessed on 5 September 2020).
- Stogner, J.; Miller, B.; McLean, K. Police Stress, Mental Health, and Resiliency. American. J. Crim. Justice 2020, 45, 718–730. [Google Scholar] [CrossRef] [PubMed]
- Lázaro-Pérez, C.; Martínez-López, J.Á.; Gómez-Galán, J.; López-Meneses, E. Anxiety about the risk of death of their patients in health professionals in Spain: Analysis at the peak of the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 5938. [Google Scholar] [CrossRef] [PubMed]
- García-Basteiro, A.; Alvarez-Dardet, C.; Arenas, A.; Bengoa, R.; Borrell, C.; Del Val, M.; Gea-Sánchez, M.; Otero, J.J.; Valcárcel, B.G.; Hernández, I. The need for an independent evaluation of the COVID-19 response in Spain. Lancet 2020, 396, 529–530. [Google Scholar] [CrossRef]
- Han, E.; Mei, M.; Turk, E.; Sridhar, D.; Leung, G.; Shibuya, K.; Asgari, N.; Oh, J.; García-Basteiro, A.L.; Hanefeld, J.; et al. Lessons learnt from easing COVID-19 restrictions: An analysis of countries and regions in Asia Pacific and Europe. Lancet 2020. [Google Scholar] [CrossRef]
- Stojanov, J.; Malobabic, M.; Stanojevic, G.; Stevic, M.; Milosevic, V.; Stojanov, A. Quality of sleep and health-related quality of life among health care professionals treating patients with coronavirus disease-19. Int. J. Soc. Psychiatry 2020. [Google Scholar] [CrossRef]
- Banerjee, D. The COVID-19 outbreak: Crucial role the psychiatrists can play. Asian J. Psychiatr. 2020, 50, 102014. [Google Scholar] [CrossRef]
- Liu, Z.; Han, B.; Jiang, R.; Huang, Y.; Ma, C.; Wen, J.; Zhang, T.; Wang, Y.; Chen, H.; Ma, Y. Mental health status of phisicians and nurses during COVID-19 epidemic in China. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Lázaro-Pérez, C. La conciencia en las experiencias cercanas a la muerte. Una aproximación a las nuevas teorías. Concienc. Cult. Rev. Antropol. 2016, 2, 99–106. [Google Scholar]
- Antón, F. Antropología del sufrimiento social. Antropol. Exp. 2017, 17, 345–355. [Google Scholar]
- Gómez-Galán, J. La inmortalidad en las religiones. Front. Cienc. 2018, 3, 68–79. [Google Scholar] [CrossRef]
- Lewis, A. Problems presented by the ambiguous word “anxietty” as used in psychopathology. Isr. Ann. Psychiatry Relat. Discip. 1967, 5, 105–121. [Google Scholar]
- Fernández Valdés, J. Relación Entre Ansiedad Rasgo, Sensibilidad a la Ansiedad y Síntomas de Ansiedad en Niños y Adolescentes; Universidad de Málaga: Málaga, Spain, 2015. [Google Scholar]
- Sierra, J.C.; Ortega, V.; Zubeidat, I. Ansiedad, angustia y estrés: Tres conceptos a diferenciar. Rev. Mal. Estar E Subj. 2003, 3, 10–59. [Google Scholar]
- Tomás-Sábado, J. Miedo y ansiedad ante la muerte en el contexto de la pandemia de la COVID-19. Rev. Enfermería Salud Ment. 2020, 16, 26–30. [Google Scholar] [CrossRef]
- Harding, S.R.; Flannelly, K.J.; Weaver, A.J.; Costa, K.G. The influence of religion on death anxiety and death acceptance. Ment. Health Relig. Cult. 2005, 8, 253–261. [Google Scholar] [CrossRef]
- Castano, E.; Leidner, B.; Bonacossa, A.; Nikkah, J.; Perrulli, R.; Spencer, B.; Humphrey, N. Ideology, fear of death, and death anxiety. Political Psychol. 2011, 32, 601–621. [Google Scholar] [CrossRef]
- Ellis, L.; Wahab, E.A.; Ratnasingan, M. Religiosity and fear of death: A three-nation comparison. Ment. Health Relig. Cult. 2013, 16, 179–199. [Google Scholar] [CrossRef]
- Tomás-Sábado, J. Miedo y Ansiedad Ante la Muerte: Aproximación Conceptual, Factores Relacionados e Instrumentos de Evaluación; Herder Editorial: Barcelona, Spain, 2016. [Google Scholar]
- Menzies, R.E.; Menzies, R.G. Death anxiety in the time of COVID-19: Theoretical explanations and clinical implications. Cogn. Behav. Ther. 2020, 13, e19. [Google Scholar] [CrossRef]
- Collett, L.; Lester, D. The fear of death end the fear of dying. J. Psychol. 1969, 72, 179–181. [Google Scholar] [CrossRef]
- Bugen, L.A. Coping: Effects of death education. J. Death Dying 1981, 11, 175–183. [Google Scholar] [CrossRef]
- Galiana, L.; Oliver, A.; De Simone, G.; Linzitto, J.P.; Benito, E.; Sansó, N. A Brief Measure for the Assessment of Competence in Coping with Death: The Coping with Death Scale Short Version. J. Pain Symptom Manag. 2019, 57, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Moya, F.J.; Barcia, D.; Canteras, M.; Garcés, E.J. La escala clínica de ansiedad ante la muerte-DACS. EduPsykhé Revista de Psicología y Psicopedagogía 2010, 9, 147–158. [Google Scholar]
- Tomás-Sábado, J.; Gómez-Benito, J. Construction and validation of the death anxiety inventory (DAI). Eur. J. Psychol. Assess. 2005, 21, 108–114. [Google Scholar] [CrossRef]
- Bentley, H. Death Concerns and Police Use of Force; Department of Psychology Texas Christian University: Fort Worth, TX, USA, 2019. [Google Scholar]
- Hawkins, H.C. Police Officer Burnout: A Partial Replication of Maslach’s Burnout Inventory. Police Q. 2001, 4, 343–360. [Google Scholar] [CrossRef]
- Briones, D.; Kinkead, A.P. Burnout and coping strategies in male staff from National Police in Valparaíso, Chile. Iran. J. Public Health 2013, 42, 950–959. [Google Scholar]
- Venegas, M.E.; Alvarado, O.S.; Barriga, O. Validación de la Escala de Miedo a la Muerte de Collett-Lester en una muestra de estudiantes de Enfermería. Rev. Lat. Am. Enferm. 2011, 19, 1171–1180. [Google Scholar] [CrossRef] [Green Version]
- Maslach, C.; Jackson, S. Maslach Burnout Inventory; Consulting Psychology Press: Palo Alto, CA, USA, 1981. [Google Scholar]
- Iwanicki, E.F.; Schwab, R.L. A cross validation study of the Maslach Burnout Inventory. Educ. Psychol. Meas. 1981, 41, 1167–1174. [Google Scholar] [CrossRef]
- Grover, S.; Sahoo, S.; Mehra, A.; Avasthi, A.; Tripathi, A.; Subramanyan, A.; Pattojoshi, A.; Rao, G.P.; Saha, G.; Mishra, K.K.; et al. Psychological impact of COVID-19 lockdown: An online survey from India. Indian J. Psychiatry 2020, 62, 354. [Google Scholar] [CrossRef]
- Kira, I.A.; Shuwiekh, H.A.; Rice, K.G.; Ashby, J.S.; Elwakeel, S.A.; Sous, M.S.; Alhuwailah, A.; Baali, S.B.; Azdaou, C.; Oliemat, E.M.; et al. Measuring COVID-19 as Traumatic Stress: Initial Psychometrics and Validation. J. Loss Trauma 2020. [Google Scholar] [CrossRef]
- Roy, D.; Tripathy, S.; Kar, S.K.; Sharma, N.; Verma, S.K.; Kaushal, V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J. Psychiatry 2020, 51, 102083. [Google Scholar]
- Instituto de Salud Carlos III. COVID-19. Informes Previos. Informes Generales. Available online: https://cutt.ly/vf9N9p4 (accessed on 3 September 2020).
- Solomou, I.; Constantinidou, F. Prevalence and predictors of anxiety and depression symptoms during the COVID-19 pandemic and compliance with precautionary measures: Age and sex matter. Int. J. Environ. Res. Public Health 2020, 17, 4924. [Google Scholar] [CrossRef] [PubMed]
- Dinibutun, S.R. Factors Associated with Burnout Among Physicians: An Evaluation During a Period of COVID-19 Pandemic. J. Healthc. Leadersh. 2020, 12, 85. [Google Scholar] [CrossRef] [PubMed]
- Sherman, A.C.; Williams, M.L.; Amick, B.C.; Hudson, T.J.; Messias, E.L. Mental health outcomes associated with the COVID-19 pandemic: Prevalence and risk factors in a southern us state. Psychiatry Res. 2020, 293, 113476. [Google Scholar] [CrossRef]
- Wang, P.W.; Ko, N.Y.; Chang, Y.P.; Wu, C.F.; Lu, W.H.; Yen, C.F. Subjective Deterioration of Physical and Psychological Health during the COVID-19 Pandemic in Taiwan: Their Association with the Adoption of Protective Behaviors and Mental Health Problems. Int. J. Environ. Res. Public Health 2020, 17, 6827. [Google Scholar] [CrossRef] [PubMed]
- Raudenská, J.; Steinerová, V.; Javůrková, A.; Urits, I.; Kaye, A.D.; Viswanath, O.; Varrassi, G. Occupational burnout syndrome and post-traumatic stress among healthcare professionals during the novel coronavirus disease 2019 (COVID-19) pandemic. Best Pract. Res. Clin. Anaesthesiol. 2020, 34, 553–560. [Google Scholar] [CrossRef]
- Azoulay, E.; De Waele, J.; Ferrer, R.; Staudinger, T.; Borkowska, M.; Povoa, P.; Iliopoulou, K.; Artigas, A.; Schaller, S.J.; Hari, M.S.; et al. Symptoms of burnout in intensive care unit specialists facing the COVID-19 outbreak. Ann. Intensive Care 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Labrague, L.J.; de Los Santos, J. Fear of Covid-19, psychological distress, work satisfaction and turnover intention among frontline nurses. J. Nurs. Manag. 2020. [Google Scholar] [CrossRef]
- Hernández-Vásquez, A.; Azañedo, D. COVID-19 in Peru: The need to pay attention to the high number of police deaths due to the pandemic. J. Public Health 2020, 382, 2267–2268. [Google Scholar] [CrossRef]
- López-Fonseca, O. Marlaska Destituye a Pérez de Los Cobos, jefe de la Guardia Civil en Madrid, por un Informe Sobre el 8-M y la COVID-19. El País. 25 May 2020. Available online: https://cutt.ly/Rf9VgzD (accessed on 14 September 2020).
- Europa Press. Cesan al Jefe de Prevención de Riesgos Laborales de la Policía Encargado del Protocolo Interno por el Coronavirus. 2020. Available online: https://cutt.ly/vf9Vnog (accessed on 14 September 2020).
- Frone, M.R.; Russell, M.; Cooper, M.L. Job stressors, job involvement and employee health: A test of identy theory. J. Occup. Organ. Psychol. 1995, 68, 1–11. [Google Scholar] [CrossRef]
- Lodahl, T.M.; Kejner, M. The definition and measurement of job involvement. J. Appl. Psychol. 1965, 49, 24–33. [Google Scholar] [CrossRef]
- López-Araújo, B.; Osca-Segovia, A. Estrés de rol, implicación con el trabajo y burnout en soldados profesionales españoles. Rev. Latinoam. Psicol. 2008, 40, 293–304. [Google Scholar]
- El-Hage, W.; Hingray, C.; Lemogne, C.; Yrondi, A.; Brunault, P.; Bienvenu, T.; Etain, B.; Paquet, C.; Gohier, B.; Bennabi, D.; et al. Health professionals facing the coronavirus disease 2019 (COVID-19) pandemic: What are the mental health risks? L’Encephale 2020, 46, S73–S80. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Yang, L.; Zhang, C.; Xiang, Y.T.; Liu, Z.; Hu, S.; Zhang, B. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, 17–18. [Google Scholar] [CrossRef]
- Vignaud, P.; Prieto, N. Impact psychique de la pandémie de COVID-19 sur les professionnels soignants. Actual. Pharm. 2020. [Google Scholar] [CrossRef]
- Shreffler, J.; Petrey, J.; Huecker, M. The impact of COVID-19 on healthcare worker wellness: A scoping review. West J. Emerg. Med. 2020, 21, 1059–1066. [Google Scholar] [CrossRef]
- Sheraton, M.; Deo, N.; Dutt, T.; Surani, S.; Hall-Flavin, D.; Kashyap, R. Psychological effects of the COVID-19 pandemic on healthcare workers globally: A systematic review. Psychiatry Res. 2020, 292, 113360. [Google Scholar] [CrossRef]
- Kavaklı, M.; Ak, M.; Uğuz, F.; Türkmen, O. The mediating role of self-compassion in the relationship between perceived COVID-19 threat and death anxiety. Turk. J. Clin. Psychiatry 2020, 23. [Google Scholar] [CrossRef]
- Lee, S.A.; Jobe, M.C.; Mathis, A.A.; Gibbons, J.A. Incremental validity of coronaphobia: Coronavirus anxiety explains depression, generalized anxiety, and death anxiety. J. Anxiety Disord. 2020, 74, 102268. [Google Scholar] [CrossRef]


{kind=link}
| Title | % |
|---|---|
| Gender | |
| Woman | 12.5 |
| Man | 87.5 |
| Age | |
| Up to 30 | 18.5 |
| 31–40 | 35.2 |
| 41–50 | 34.4 |
| 51–60 | 11.1 |
| >60 | 0.9 |
| Work | |
| FFAA | 18.0 |
| Guardia Civil | 43.5 |
| Policía Nacional | 38.5 |
| Worked with COVID-19 during the First Wave of the Pandemic | |
| Yes | 73.2 |
| No | 26.8 |
| Sub Emotional Exhaustion (EE) | |
| Low | 29.8 |
| Medium | 16.4 |
| High | 53.8 |
| Sub Depersonalization (DP) | |
| Low | 17.5 |
| Medium | 24.1 |
| High | 58.4 |
| Sub Personal Accomplishment (PA) | |
| Low | 46.8 |
| Medium | 26.2 |
| High | 27.0 |
| Total MBI | |
| Yes | 28.9 |
| No | 71.1 |
| Need Psychological or Psychiatric Support (NAPP) | |
| Yes | 26.4 |
| No | 73.6 |
| Psychological or Psychiatric Support from the Workplace (APPC) | |
| Yes | 88.2 |
| No | 11.8 |
| May Need Psychological or Psychiatric Support (PNPP) | |
| Yes | 52.6 |
| No | 47.4 |
| Lack of PPE Increased Your Stress and Anxiety Level (PPE) | |
| Yes | 87.8 |
| No | 12.2 |
| Feel that Your Work Has Been Recognized by Your Institution (SRI) | |
| Yes | 90.3 |
| No | 9.7 |
| B | Sig. | Exp (B) | 95% C.I. Exp (B) | ||
|---|---|---|---|---|---|
| Lower | Superior | ||||
| DA 1 | |||||
| PNPP | 0.696 | 0.000 | 2.005 | 1.662 | 2.418 |
| PPE | 0.488 | 0.001 | 1.629 | 1.210 | 2.192 |
| Total Burnout | 0.347 | 0.002 | 1.414 | 1.137 | 1.760 |
| EE | 0.627 | 0.000 | 1.873 | 1.494 | 2.347 |
| DP | 0.391 | 0.003 | 1.478 | 1.141 | 1.914 |
| Constant | −1.706 | 0.000 | 0.182 | ||
| DA 2 | |||||
| PNPP | 0.623 | 0.000 | 1.864 | 1.542 | 2.254 |
| PPE | 0.335 | 0.019 | 1.399 | 1.058 | 1.849 |
| Total Burnout | 0.381 | 0.001 | 1.464 | 1.167 | 1.836 |
| EE | 0.742 | 0.000 | 2.099 | 1.692 | 2.605 |
| Constant | −0.847 | 0.000 | 0.429 | ||
| DA 3 | |||||
| 41-50 years old | 0.366 | 0.025 | 1.442 | 1.047 | 1.987 |
| 51-60 years old | 0.734 | 0.002 | 2.084 | 1.320 | 3.288 |
| PNPP | 0.444 | 0.001 | 1.559 | 1.206 | 2.017 |
| PPE | 0.635 | 0.000 | 1.888 | 1.386 | 2.571 |
| EE | 0.721 | 0.000 | 2.057 | 1.601 | 2.643 |
| DP | 0.402 | 0.005 | 1.494 | 1.126 | 1.983 |
| Constant | −0.564 | 0.016 | 0.569 | ||
| DA 4 | |||||
| PNPP | 0.564 | 0.000 | 1.758 | 1.398 | 2.211 |
| PPE | 0.423 | 0.005 | 1.527 | 1.134 | 2.056 |
| Worked COVID-19 | −0.335 | 0.010 | 0.716 | 0.556 | 0.922 |
| EE | 0.894 | 0.000 | 2.444 | 1.937 | 3.084 |
| DP | 0.307 | 0.026 | 1.359 | 1.037 | 1.780 |
| Constant | 0.073 | 0.685 | 1.076 | ||
| DA Total | |||||
| PNPP | 0.599 | 0.000 | 1.820 | 1.482 | 2.234 |
| PPE | 0.481 | 0.001 | 1.617 | 1.220 | 2.144 |
| Total Burnout | 0.367 | 0.006 | 1.444 | 1.112 | 1.875 |
| EE | 0.798 | 0.000 | 2.221 | 1.770 | 2.786 |
| DP | 0.324 | 0.012 | 1.383 | 1.074 | 1.781 |
| Constant | −0.781 | 0.000 | 0.458 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lázaro-Pérez, C.; Martínez-López, J.Á.; Gómez-Galán, J.; Fernández-Martínez, M.d.M. COVID-19 Pandemic and Death Anxiety in Security Forces in Spain. Int. J. Environ. Res. Public Health 2020, 17, 7760. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17217760
Lázaro-Pérez C, Martínez-López JÁ, Gómez-Galán J, Fernández-Martínez MdM. COVID-19 Pandemic and Death Anxiety in Security Forces in Spain. International Journal of Environmental Research and Public Health. 2020; 17(21):7760. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17217760
Chicago/Turabian StyleLázaro-Pérez, Cristina, José Ángel Martínez-López, José Gómez-Galán, and María del Mar Fernández-Martínez. 2020. "COVID-19 Pandemic and Death Anxiety in Security Forces in Spain" International Journal of Environmental Research and Public Health 17, no. 21: 7760. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17217760