Post-Orthodontic Lower Incisors Recessions: Combined Periodontic and Orthodontic Approach


Abstract
:1. Introduction
2. Materials and Methods
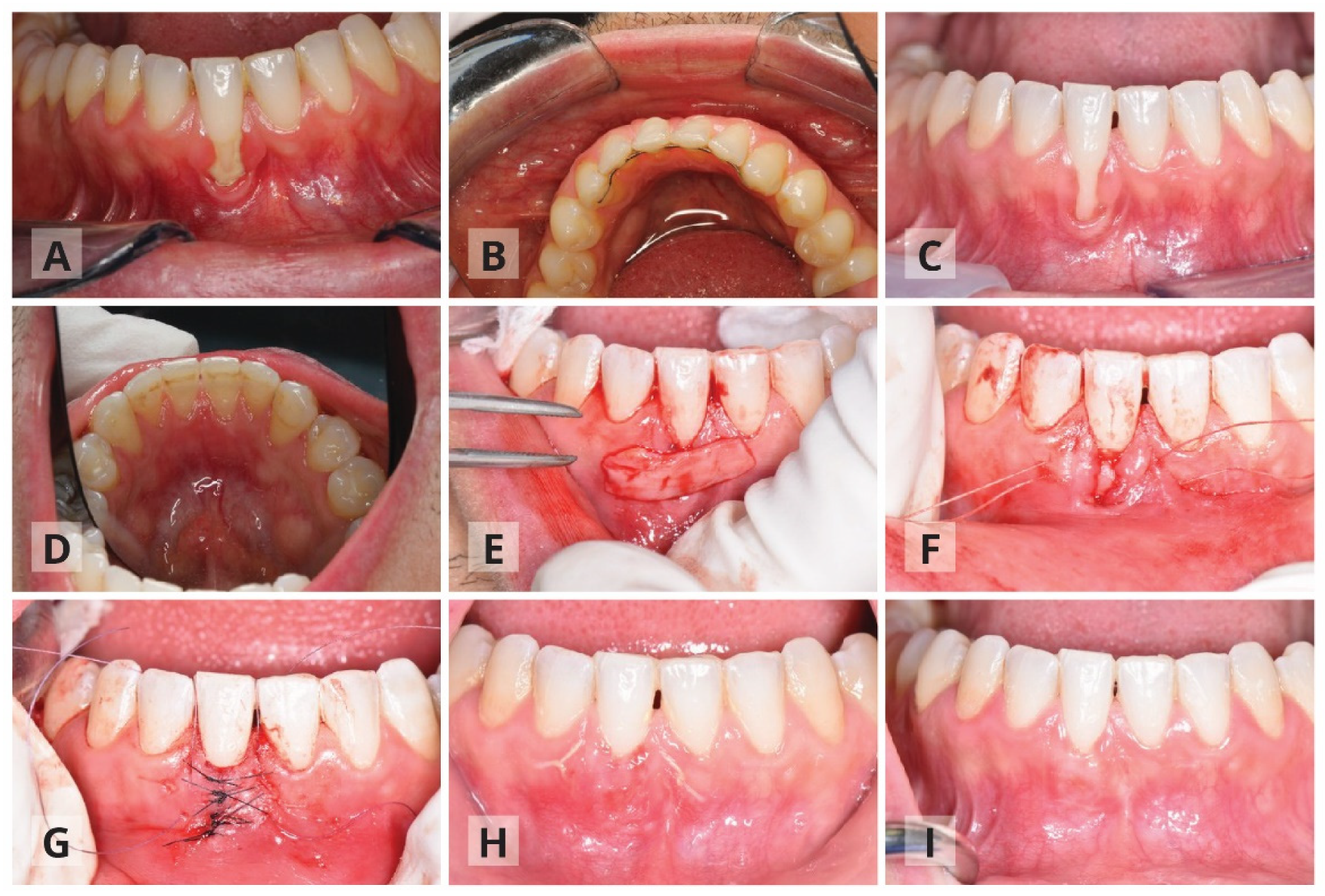
The Surgical Procedure: Modified Tunnel Double Papilla Procedure for Root Coverage
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Al Yami, E.A.; Kuijpers-Jagtman, A.M.; van ’t Hof, M.A. Stability of orthodontic treatment outcome: Follow-up until 10 years postretention. Am. J. Orthod. Dentofac. Orthop. 1999, 115, 300–304. [Google Scholar] [CrossRef]
- Littlewood, S.J.; Kandasamy, S.; Huang, G. Retention and relapse in clinical practice. Aust. Dent. J. 2017, 62, 51–57. [Google Scholar] [CrossRef] [Green Version]
- Littlewood, S.J.; Millett, D.T.; Doubleday, B.; Worthington, H.V. Retention procedures for establishing tooth position after treatment with orthodontic braces. Cochrane Database Syst. Rev. 2016, 51, 1–135. [Google Scholar] [CrossRef] [Green Version]
- Andriekute, A.; Vasiliauskas, A.; Sidlauskas, A. A survey of protocols and trends in orthodontic retention. Prog. Orthod. 2017, 18, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padmos, J.A.; Fudalej, P.S.; Renkema, A.M. Epidemiologic study of orthodontic retention procedures. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 496–504. [Google Scholar] [CrossRef]
- Iliadi, A.; Kloukos, D.; Gkantidis, N.; Katsaros, C.; Pandis, N. Failure of fixed orthodontic retainers: A systematic review. J. Dent. 2015, 43, 876–896. [Google Scholar] [CrossRef]
- Roussarie, F.; Douady, G. A side-effect of bonded retention wires: The “wire syndrome”: Part 1. J. Dentofac. Anom. Orthod. 2016, 19, 106. [Google Scholar] [CrossRef] [Green Version]
- Shaughnessy, T.G.; Proffit, W.R.; Samara, S.A. Inadvertent tooth movement with fixed lingual retainers. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 277–286. [Google Scholar] [CrossRef] [Green Version]
- Adams, D.F. The American Academy of Periodontology. J. Periodontol. 1996, 67, 177–179. [Google Scholar] [CrossRef]
- Miller, P.D. A classification of marginal tissue recession. Int. J. Periodontics Restor. Dent. 1985, 5, 8–13. [Google Scholar]
- Tatakis, D.N.; Chambrone, L.; Allen, E.P.; Langer, B.; McGuire, M.K.; Richardson, C.R.; Zabalegui, I.; Zadeh, H.H. Periodontal Soft Tissue Root Coverage Procedures: A consensus report from the AAP regeneration workshop. J. Periodontol. 2015, 86, S52–S55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melsen, B.; Allais, D. Factors of importance for the development of dehiscences during labial movement of mandibular incisors: A retrospective study of adult orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 2005, 127, 552–561. [Google Scholar] [CrossRef] [PubMed]
- Kamak, G.; Kamak, H.; Keklik, H.; Gurel, H.G. The effect of changes in lower incisor inclination on gingival recession. Sci. World J. 2015, 2015, 193206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahab, R.F.; Oktawati, S.; Mappangara, S. Gingival recession of mandibular incisor post-orthodontic treatment: A systematic review. MDJ 2020, 9, 118–120. [Google Scholar]
- Pazera, P.; Fudalej, P.; Katsaros, C. Severe complication of a bonded mandibular lingual retainer. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 406–409. [Google Scholar] [CrossRef]
- Renkema, A.M.; Fudalej, P.S.; Renkema, A.; Kiekens, R.; Katsaros, C. Development of labial gingival recessions in orthodontically treated patients. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 206–212. [Google Scholar] [CrossRef]
- Cairo, F.; Rotundo, R.; Miller, P.D.; Prato, G.P.P. Root Coverage Esthetic Score: A System to Evaluate the Esthetic Outcome of the Treatment of Gingival Recession Through Evaluation of Clinical Cases. J. Periodontol. 2009, 80, 705–710. [Google Scholar] [CrossRef]
- Stefanini, M.; Jepsen, K.; de Sanctis, M.; Baldini, N.; Greven, B.; Heinz, B.; Wennström, J.; Cassel, B.; Vignoletti, F.; Sanz, M.; et al. Patient-reported outcomes and aesthetic evaluation of root coverage procedures: A 12-month follow-up of a randomized controlled clinical trial. J. Clin. Periodontol. 2016, 43, 1132–1141. [Google Scholar] [CrossRef]
- Mounssif, I.; Stefanini, M.; Mazzotti, C.; Marzadori, M.; Sangiorgi, M.; Zucchelli, G. Esthetic evaluation and patient-centered outcomes in root-coverage procedures. Periodontology 2000 2018, 77, 19–53. [Google Scholar] [CrossRef]
- Hürzeler, M.B.; Weng, D. A single-incision technique to harvest subepithelial connective tissue grafts from the palate. Int. J. Periodontics Restor. Dent. 1999, 19, 279–287. [Google Scholar]
- Katsaros, C.; Livas, C.; Renkema, A.M. Unexpected complications of bonded mandibular lingual retainers. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 838–841. [Google Scholar] [CrossRef] [PubMed]
- Pandis, N.; Vlahopoulos, K.; Madianos, P.; Eliades, T. Long-term periodontal status of patients with mandibular lingual fixed retention. Eur. J. Orthod. 2007, 29, 471–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laursen, M.G.; Rylev, M.; Melsen, B. The role of orthodontics in the repair of gingival recessions. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 29–34. [Google Scholar] [CrossRef]
- Chaushu, S.; Stabholz, A. Orthodontic-associated localized gingival recession of lower incisors: Who should treat it? Compend. Contin. Educ. Dent. 2013, 34, 6–12. [Google Scholar] [PubMed]
- Mahajan, A. Mahajan’s modification of miller’s classification for gingival recession. Dent. Hypotheses 2010, 1, 45–50. [Google Scholar] [CrossRef]
- Pini-Prato, G. The Miller classification of gingival recession: Limits and drawbacks. J. Clin. Periodontol. 2011, 38, 243–245. [Google Scholar] [CrossRef]
- Cairo, F.; Nieri, M.; Cincinelli, S.; Mervelt, J.; Pagliaro, U. The interproximal clinical attachment level to classify gingival recessions and predict root coverage outcomes: An explorative and reliability study. J. Clin. Periodontol. 2011, 38, 661–666. [Google Scholar] [CrossRef]
- Roccuzzo, M.; Bunino, M.; Needleman, I.; Sanz, M. Periodontal plastic surgery for treatment of localized gingival recessions: A systematic review. J. Clin. Periodontol. 2002, 29, 178–194. [Google Scholar] [CrossRef]
- Chambrone, L.; Chambrone, D.; Pustiglioni, F.E.; Chambrone, L.A.; Lima, L.A. Can subepithelial connective tissue grafts be considered the gold standard procedure in the treatment of Miller Class I and II recession-type defects? J. Dent. 2008, 36, 659–671. [Google Scholar] [CrossRef]
- Chambrone, L.; Sukekava, F.; Araújo, M.G.; Pustiglioni, F.E.; Chambrone, L.A.; Lima, L.A. Root-Coverage Procedures for the Treatment of Localized Recession-Type Defects: A Cochrane Systematic Review. J. Periodontol. 2010, 81, 452–478. [Google Scholar] [CrossRef]
- Greenwell, H.; Bissada, N.F.; Henderson, R.D.; Dodge, J.R. The Deceptive Nature of Root Coverage Results. J. Periodontol. 2000, 71, 1327–1337. [Google Scholar] [CrossRef]
- Langer, B.; Langer, L. Subepithelial Connective Tissue Graft Technique for Root Coverage. J. Periodontol. 1985, 56, 715–720. [Google Scholar] [CrossRef]
- Nemcovsky, C.E.; Artzi, Z.; Tal, H.; Kozlovsky, A.; Moses, O. A Multicenter Comparative Study of Two Root Coverage Procedures: Coronally Advanced Flap with Addition of Enamel Matrix Proteins and Subpedicle Connective Tissue Graft. J. Periodontol. 2004, 75, 600–607. [Google Scholar] [CrossRef]
- Moses, O.; Artzi, Z.; Sculean, A.; Tal, H.; Kozlovsky, A.; Romanos, G.E.; Nemcovsky, C.E. Comparative Study of Two Root Coverage Procedures: A 24-Month Follow-Up Multicenter Study. J. Periodontol. 2006, 77, 195–202. [Google Scholar] [CrossRef]
- Raetzke, P.B. Covering Localized Areas of Root Exposure Employing the “Envelope” Technique. J. Periodontol. 1985, 56, 397–402. [Google Scholar] [CrossRef]
- Allen, A.L. Use of the supraperiosteal envelope in soft tissue grafting for root coverage. I. Rationale and technique. Int. J. Periodontics Restor. Dent. 1994, 14, 216–227. [Google Scholar] [CrossRef]
- Allen, A.L. Use of the supraperiosteal envelope in soft tissue grafting for root coverage. II. Clinical results. Int. J. Periodontics Restor. Dent. 1994, 14, 302–315. [Google Scholar]
- Zabalegui, I.; Sicilia, A.; Cambra, J.; Gil, J.; Sanz, M. Treatment of multiple adjacent gingival recessions with the tunnel subepithelial connective tissue graft: A clinical report. Int. J. Periodontics Restor. Dent. 1999, 19, 199–206. [Google Scholar]
- Azzi, R.; Etienne, D.; Carranza, F. Surgical Reconstruction of the Interdental Papilla. Int. J. Periodontics Restor. Dent. 1998, 18, 467–473. [Google Scholar] [CrossRef]
- Zuhr, O.; Fickl, S.; Wachtel, H.; Bolz, W.; Hürzeler, M.B. Covering of gingival recessions with a modified microsurgical tunnel technique: Case report. Int. J. Periodontics Restor. Dent. 2007, 27, 457–463. [Google Scholar] [CrossRef]
- Sebaoun, A.; Nemcovsky, C.; Beitlitum, I.; Moses, O. Modified Tunnel Double Papilla Procedure for Root Coverage in the Anterior Mandible. Int. J. Periodontics Restor. Dent. 2019, 39, 503–509. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Recession Depth | ||||||||
|---|---|---|---|---|---|---|---|---|
| Patient Number | Gender | Age | Tooth Number | Bonded Lingual Retainer Removal | Recession Type | First Examination (mm) | After Surgery | Improvement (%) |
| (mm) | ||||||||
| 1 | Male | 37 | 32 | no | 1 | 6 | 1 | 83.33 |
| 2 | Male | 30 | 41 | no | 2 | 3 | 0.5 | 83.33 |
| 3 | Male | 27 | 41 | no | 1 | 5 | 3 | 40 |
| 4 | Female | 30 | 31 | no | 1 | 4 | 2.5 | 37.5 |
| 5 | Female | 25 | 31 | no | 2 | 4 | 3 | 25 |
| 6 | Female | 42 | 31 | no | 2 | 4 | 3 | 25 |
| 7 | Male | 28 | 31 | no | 1 | 4 | 2 | 50 |
| 8 | Female | 25 | 31 | no | 1 | 4 | 3 | 25 |
| 9 | Female | 28 | 31 | no | 1 | 4 | 3 | 25 |
| 10 | Female | 32 | 41 | yes | 1 | 4 | 0 | 100 |
| 11 | Female | 56 | 41 | yes | 2 | 6 | 1.5 | 75 |
| 12 | Female | 30 | 41 | yes | 2 | 4 | 1 | 75 |
| 13 | Male | 31 | 41 | yes | 2 | 5 | 0.5 | 90 |
| 14 | Male | 43 | 31 | yes | 2 | 6 | 1 | 83.33 |
| 15 | Male | 24 | 32 | yes | 1 | 3 | 0 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beitlitum, I.; Barzilay, V.; Rayyan, F.; Sebaoun, A.; Sarig, R. Post-Orthodontic Lower Incisors Recessions: Combined Periodontic and Orthodontic Approach. Int. J. Environ. Res. Public Health 2020, 17, 8060. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218060
Beitlitum I, Barzilay V, Rayyan F, Sebaoun A, Sarig R. Post-Orthodontic Lower Incisors Recessions: Combined Periodontic and Orthodontic Approach. International Journal of Environmental Research and Public Health. 2020; 17(21):8060. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218060
Chicago/Turabian StyleBeitlitum, Ilan, Vered Barzilay, Fatma Rayyan, Alon Sebaoun, and Rachel Sarig. 2020. "Post-Orthodontic Lower Incisors Recessions: Combined Periodontic and Orthodontic Approach" International Journal of Environmental Research and Public Health 17, no. 21: 8060. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17218060