Motivating Pregnant and Breastfeeding Women in Spain to Avoid Persistent Toxic Substances in Their Diet

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample, Participants, and Context
- Advice on dietary changes or continuity.
- Foods that the participants believed contained chemical substances, inquiring about the dangers and trust associated with these foods and the women’s reasons for such beliefs. When necessary, the topics of pesticides, preservatives, metals, sweeteners, etc. were discussed.
- Participants’ perceptions regarding the long-term accumulation of these chemical substances in the body and how they are eliminated and transmitted.
- Knowledge about PTS and verification in the discourse of the participants. Inquiry into their knowledge in this respect and whether they employed practices or strategies to avoid them in everyday life.
2.2. Data Categorization and Analysis
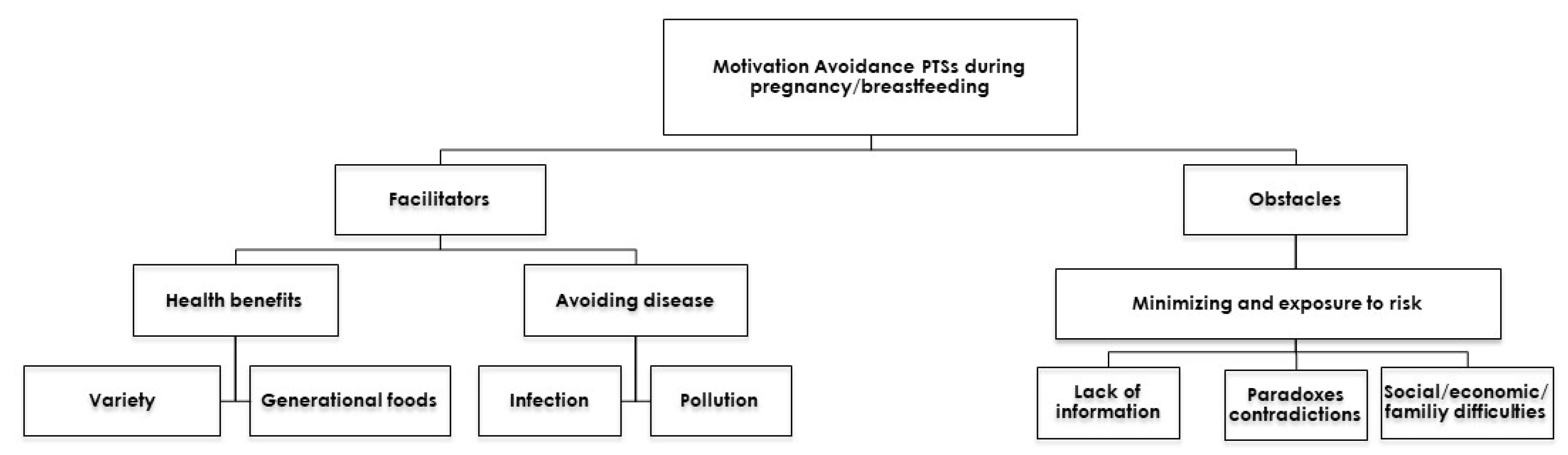
3. Results
3.1. Motivation for Dietary Changes during Pregnancy/Breastfeeding
3.1.1. Rewards—Promoting Health
Variety
“I guess you have to pay more attention to the vitamins you get, you know? You need to take vitamins, but especially, have more fruit and vegetables, raw ones, to get all the nutrients. This is a little bit of what I would vary from what I usually eat”.(Virginia, pregnant, 40, Barcelona)
“A little bit of everything, you know? You need to eat everything like…vegetables, fish, meat, eggs, a variety… I mean, a varied diet”.(Luisa, breastfeeding, 28, Granada)
Generational Foods: From Mothers to Grandmothers
“The other day someone told me that we should go to the supermarket imagining we were our great-grandmothers, and buy what they would buy. I suppose nothing would have been in a bag or package or frozen. And it seems to me that’s what it’s about, that the right thing and the good thing is that. I should stop thinking about what my great grandmother would have bought”.(Susana, breastfeeding, 40, Barcelona)
3.1.2. Avoiding Harm or Illness
“When you aren’t pregnant, you’re just on your own, so it’s a little like, if one week you’re a little more relaxed, and you eat an ice cream every day, it doesn’t matter, or if you have a Coke or whatever. I feel like, well, it’s my body, and there’s no problem; it doesn’t matter. But, when you have a baby inside you, it’s like what you’re eating, you pass on to the baby, so I think about it. If I drink a coke, it’s like I’m pouring coke into the baby, and I don’t know, it’s different”.(Barbara, pregnant, 36, Barcelona)
Infection
“Well, since I haven’t had toxoplasmosis, right, well, of course, for example, I can’t eat chorizo, ham, or sausage, and so normally, I always take a sandwich to work, and normally, it’s either sausage or ham or something. So now we’ve changed; I have tuna, an omelette or … something like that”.(Isabel, pregnant, 36, Barcelona)
Pollution
“They accumulate in the body. You can’t eliminate heavy metals. And fish carry heavy metals, the very large ones. And your body doesn’t eliminate them, like lead, mercury; it all stays there. And pesticides, I don’t know what to say. It’s that, um, often I think that more than them accumulating, it’s the alterations they cause internally. Because, there are also free radicals, how to fight them, all that promotes aging. And externally, and also with the organs. I mean, I no longer think it’s a matter of accumulation, but it’s about genetic alteration”.(Teresa, pregnant, 38, Macael, Almería)
3.2. Obstacles to Change
3.2.1. Need for Better Information
“Well, yes, it sounds familiar, the whole topic of pesticides commented on (…) I think everything has … but well, there are many more bad things that cause cancer, or diabetes because what can you eat? Everything seems to cause something”.(Laura, pregnant, 36, Barcelona)
3.2.2. Paradoxes and Contradictions in the Discourses
“I almost don’t trust anything because it’s all about money, so everything is super manipulated, super bought off. I don’t believe anything; they tell me that something is super healthy, and a year from now they tell me that it wasn’t so healthy”.(Cristina, 39, breastfeeding, Tarragona)
“I think I could probably do better; I could take better care of myself, not eating so many sweets, for sure, as in all areas of life, of course, but I’m relaxed. In the end, if you eat something with pleasure, it can’t be that bad for you!”.(Raquel, 35, breastfeeding, Tarragona)
3.2.3. Social, Economic, and Family Difficulties in Having a Healthy Diet without PTS
“I understand that local products would be more ideal, but sometimes the prices are just too high; if you buy for a single person … but if you’re buying for a whole family, local products seem very expensive to me (…) And, besides, I don’t have time to go to the main market today, to the neighborhood street market on Saturday, etc. If you have time, it’s great, but that’s not my case. In the end, you have to choose…”(Yolanda, 33, breastfeeding, Tarragona)
4. Discussions
“Trying to change eating habits through information without first questioning the origin of these habits rests on several assumptions that are not true, such as: (a) that individuals are quite fixed in their erroneous practices; (b) the social environment is more or less stable; (c) nutritional knowledge is definitive”[49]
- Contextual: the sphere in which daily life takes place.
- Personal: genes, beliefs, abilities, attitudes.
- Social: family relationships, friendships, and relationship to the community in general.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fischler, C. L’Homnivore; Odile Jacob: Paris, France, 1990. [Google Scholar]
- Poulain, J.P. Sociologies de L’alimentation; PUF: Paris, France, 2002. [Google Scholar]
- Contreras, J.; Gracia-Arnaiz, M. Alimentación y Cultura: Perspectivas Antropólogicas; Ariel: Barcelona, Spain, 2005. [Google Scholar]
- Lupton, D. Food, the Body and the Self; Sage Publications: London, UK, 1996. [Google Scholar]
- Ascher, F. Le Mangeur Hypermoderne; Odile Jacob: Paris, France, 2005. [Google Scholar]
- Poulain, J.P. Sociologie de l’obésité; PUF: Paris, France, 2009. [Google Scholar]
- Apfelbaum, M. Introduction. In Risques et Peurs Alimentaires; Apfelbaum, M., Ed.; Odile Jacob: Paris, France, 1998. [Google Scholar]
- Fischler, C. La maladie de la ‘vache folle’. In Risques et Peurs Alimentaires; Apfelbaum, M., Ed.; Odile Jacob: Paris, France, 1998; pp. 45–56. [Google Scholar]
- Beck, U. La Sociedad del Riesgo: Hacia una Nueva Modernidad; Paidós: Barcelona, Spain, 1992. [Google Scholar]
- Begueria, A. Un Equilibrio Imperfecto: Alimentación Ecológica, Cuerpo y Toxicidad; Editorial UOC: Barcelona, Spain, 2016. [Google Scholar]
- Porta, M.; Puigdomènech, E.; Ballester, F. (Eds.) Nuestra contaminación interna. In Concentraciones de Compuestos Tóxicos Persistentes en la Población Española; Los libros de la Catarata: Madrid, Spain, 2009. [Google Scholar]
- Pumarega, J.; Larrea-Killinger, C.; Muñoz, A.; Pallarès, N.; Gasull, M.; Rodriguez, G.; Jariod, M.; Porta, M. Citizens’ perceptions of the presence and health risks of synthetic chemicals in food: Results of an online survey in Spain. Gac. Sanit. 2017, 31, 371–381. [Google Scholar] [CrossRef] [PubMed]
- Poti, J.M.; Braga, B.; Qin, B. Ultra-processed Food Intake and Obesity: What Really Matters for Health-Processing or Nutrient Content? Curr. Obes. Rep. 2017, 6, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Kong, A.P.S.; Cai, Z.; Chung, A.C. Persistent Organic Pollutants as Risk Factors for Obesity and Diabetes. Curr. Diab. Rep. 2017, 17, 132. [Google Scholar] [CrossRef] [PubMed]
- Hedley, A.; Hui, L.; Kypke, K.; Malisch, R.; Van Leeuwen, F.; Moy, G.; Wong, T.; Nelson, E.A.S. Residues of persistent organic pollutants (POPs) in human milk in Hong Kong. Chemosphere 2010, 79, 259–265. [Google Scholar] [CrossRef]
- Fernández-Cruz, T.; Martínez-Carballo, E.; Simal-Gándara, J. Perspective on pre- and post-natal agro-food exposure to persistent organic pollutants and their effects on quality of life. Environ. Int. 2017, 100, 79–101. [Google Scholar] [CrossRef]
- Wigle, D.T.; Arbuckle, T.E.; Turner, M.C.; Bérubé, A.; Yang, Q.; Liu, S.; Krewski, D. Epidemiologic evidence of relationships between reproductive and child health outcomes and environmental chemical contaminants. J. Toxicol. Environ. Health. B Crit. Rev. 2008, 11, 373–517. [Google Scholar] [CrossRef]
- Zielińska, A.; Hamulka, J. Protective Effect of Breastfeeding onthe Adverse Health Effects Induced by Air Pollution: Current Evidence and Possible Mechanisms. Int. J. Environ. Res. Public Health 2019, 16, 4181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larrea-Killinger, C.; Muñoz, A.; Mascaró, J.A. Cuerpos tóxicos: La percepción del riesgo de la contaminación interna por compuestos químicos en España. Salud Colect 2017, 13, 225–237. [Google Scholar] [CrossRef]
- Larrea-Killinger, C.; Muñoz, A.; Mascaró, J.; Zafra, E.; Porta, M. Discourses on the Toxic Effects of Internal Chemical Contamination in Catalonia, Spain. Med. Anthropol. 2017, 36, 125–140. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, L.; Shaw, R.L.; French, D. Is pregnancy a teachable moment for diet and physical activity behaviour change? An interpretative phenomenological analysis of the experiences of women during their first pregnancy. Br. J. Health Psychol. 2016, 21, 842–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juvinya-Canal, D. Salutogénesis, nuevas perspectivas para promover la salud. Enferm. Clin. 2013, 23, 87–88. [Google Scholar] [CrossRef] [PubMed]
- Sui, Z.X.; Moran, L.I.; Dodd, J.M. Physical activity levels during pregnancy and gestational weight gain among women who are overweight or obese. Health Promot. J. Austr. 2013, 24, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Spencer. The effect of weight management interventions that include a diet component on weight-related outcomes in pregnant and postpartum women: A systematic review protocol. JBI Database Syst. Rev. Implement Rep. 2015, 13, 88–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padmanabhan, U.; Summerbell, C.D.; Heslehurst, N. A qualitative study exploring pregnant women’s weight-related attitudes and beliefs in UK: The BLOOM study. BMC Pregnancy Childbirth 2015, 15, 99. [Google Scholar] [CrossRef] [Green Version]
- Setia, M.S. Methodology Series Module 10: Qualitative Research in Health. Indian J. Dermatol. 2017, 62, 367–370. [Google Scholar] [CrossRef]
- Kaufmann, J.K. L’enquête et ses méthodes. In L’entretien Compréhensif; Armand Colin: Paris, France, 2008. [Google Scholar]
- Blanchet, A.; Gotman, A. L’entretien; Armand Colin: Paris, France, 2005. [Google Scholar]
- Sobal, J. Cultural comparison research designs in food, eating, and nutrition. Food Qual. Prefer. 1998, 9, 385–392. [Google Scholar] [CrossRef]
- Lupton, D. Medicine as Culture: Illness, Disease and the Body; Sage Publications: London, UK, 2012. [Google Scholar] [CrossRef]
- Baker, R.; Camosso-Stefinovic, J.; Gillies, C.; Shaw, E.J.; Cheater, F.; Flottorp, S.; Robertson, N. Tailored interventions to overcome identified barriers to change: Effects on professional practice and health care outcomes. Cochrane Database Syst. Rev. 2005, 3, CD005470. [Google Scholar]
- Raynor, H.A.; Vadiveloo, M. Understanding the Relationship Between Food Variety, Food Intake, and Energy Balance. Curr. Obes. Rep. 2018, 7, 68–75. [Google Scholar] [CrossRef] [Green Version]
- Alimentation Saine. Available online: www.who.int/mediacentre/factsheets/fs394/fr (accessed on 9 July 2020).
- Estrategia Para la Nutrición, Actividad Fisica y Prevención de la Obesidad (Estrategia NAOS); AESAN: Madrid, Spain, 2005.
- Paisley, J.; Sheeshka, J.; Daly, K. Qualitative investigation of the meanings of eating fruits and vegetables for adult couples. J. Nutr. Educ. 2001, 33, 199–207. [Google Scholar] [CrossRef]
- Observatorio de la Alimentación La alimentación y sus circunstancias: Placer, conveniencia y salud—Estudio sobre la realidad de los comportamientos de la población española. In Proceedings of the V Foro Internacional de la Alimentación, Barcelona, Spain, 8–12 March 2004.
- Paquette, M.C. Perceptions of healthy eating. Can J. Pub. Health 2005, 96, S11–S19. [Google Scholar]
- European Commission Health and Food. Special Eurobarometer, n. 246; TNS Opinion & Social: Brussels, Belgium, 2006. [Google Scholar]
- Gaspar, M.C.M.P.; Blanco, L.F. La noción del “comer bien” para jóvenes brasileñas y españolas: Dietética, cultura, placer y disciplina. Revista de Estudios Etnográficos 2015, 7, 19–36. [Google Scholar]
- Costa, H.S.; Vasilopoulou, E.; Trichopoulou, A.; Finglas, P. New nutritional data on traditional foods for European food composition databases. Eur. J. Clin. Nutr. 2010, 64 (Suppl. 3), S73–S81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bessière, J. Patrimoine alimentaire, patrimonialisation. In Dictionnaire des Cultures Alimentaires; Poulain, J.P., Ed.; PUF: Paris, France, 2012; pp. 978–985. [Google Scholar]
- Arrebola, J.P.; Garcia, A.M.; Martínez, S.F.; Larrea-Killinger, C. Perceptions and Attitudes of Gynecologic and Pediatric Professionals Regarding Dietary Exposure to Chemical Pollutants. Int. J. Environ. Res. Public Health 2020, 17, 3946. [Google Scholar] [CrossRef] [PubMed]
- Hampton, M.M. Congenital Toxoplasmosis: A Review. Neonatal Netw. 2015, 34, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Gehring, U.; Casas, M.; Brunekreef, B.; Bergström, A.; Bonde, J.P.; Botton, J.; Chevrier, C.; Cordier, S.; Heinrich, J.; Hohmann, C.; et al. Environmental exposure assessment in European birth cohorts: Results from the ENRIECO project. Environ. Health 2013, 12, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machín, L.; Aschemann-Witzel, J.; Patiño, A.; Moratorio, X.; Bandeira, E.; Curutchet, M.R.; Martínez, J.; Bove, I.; Molina, V.; Giménez, A.; et al. Barriers and Facilitators to Implementing the Uruguayan Dietary Guidelines in Everyday Life: A Citizen Perspective. Health Educ. Behav. 2017, 45, 511–523. [Google Scholar] [CrossRef]
- Morales, S.; Kendall, P.A.; Medeiros, L.C.; Hillers, V.; Schroeder, M. Healthcare providers’ attitudes toward current food safety recommendations for pregnant women. Appl. Nurs. Res. 2004, 17, 178–186. [Google Scholar] [CrossRef]
- Zafra-Aparici, E.; Muñoz-García, A. Larrea-Killinger, CSabemos lo que comemos?: Percepciones sobre el riesgo alimentario en Cataluña. España. Salud Colect 2016, 12, 505. [Google Scholar] [CrossRef]
- Adam, P.; Herzlich, C. Sociologie de la Maladie et de la Médecine; Armand Colin: Saint-Jean de Braye, France, 2012. [Google Scholar]
- Poulain, J.P. Manger Aujourd’hui: Attitudes, Normes et Pratiques; Privat: Toulouse, France, 2002. [Google Scholar]
- Darnton, A. Practical Guide: An Overview of Behavior Change Model and Their Uses; Government Social Research Unit: London, UK, 2008.
- Rodríguez, J.A.G.D.C.; Del Castillo-López, Á.G.; López-Sánchez, C.; Dias, P.C. Configuración teórica de la motivación de salud desde la teoría de la autodeterminación. Salud Drogas 2015, 15, 151–159. [Google Scholar]
- Cerasoli, C.P.; Nicklin, J.M.; Ford, M.T. Intrinsic motivation and extrinsic incentives jointly predict performance: A 40-year meta-analysis. Psychol. Bull. 2014, 140, 980–1008. [Google Scholar] [CrossRef]
- Butland, B.; Jebb, S.; Kopelman, P.; McPherson, K.; Thomas, S.; Mardell, J.; Parry, V. Tackling Obesities: Future Choices—Project Report, 2nd ed.; Government Office for Science: London, UK, 2007.
- Balaam, M.C.; Thomson, G. Building capacity and wellbeing in vulnerable/marginalised mothers: A qualitative study. Women Birth 2018, 31, e341–e347. [Google Scholar] [CrossRef]
- Tobias, D.; Zhang, C.; van Dam, R.M.; Bowers, K.; Hu, F.B. Physical activity before and during pregnancy and risk of gestational diabetes mellitus: A meta-analysis. Diabetes Care 2011, 34, 223–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zielinska, M.A.; Hamulka, J. Reason of non-exclusive breastfeeding to infants within the first 6 months. Pediatr. Int. 2018, 60, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Schmied, V.; Beake, S.; Sheehan, A.; McCourt, C.; Dykes, F. A meta-synthesis of women’s perceptions and experiences of breastfeeding support. JBI Libr. Syst. Rev. 2009, 7, 583–614. [Google Scholar] [CrossRef] [PubMed]
- Ni, P.K.; Siew, L.S. The role of family and friends in providing social support towards enhancing the wellbeing of postpartum women: A comprehensive systematic review. JBI Libr. Syst. Rev. 2011, 9, 313–370. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Pregnant and Breastfeeding Women | ||||
|---|---|---|---|---|
| Profiles | Pregnant | Breastfeeding | Total | |
| 62 | 49 | 111 | ||
| Age range | Age—20–29 | Age—30–39 | Age—40+ | |
| 17 | 81 | 13 | ||
| Education level | Primary | Secondary | Higher | |
| 6 | 37 | 68 | ||
| Number of children | Child-1 | Child-2 | Child-3 or + | |
| 58 | 45 | 8 | ||
| Province | Almería | Barcelona | Granada | Tarragona |
| 30 | 51 | 20 | 10 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fontalba-Navas, A.; Zafra Aparici, E.; Prata-Gaspar, M.C.d.M.; Herrera-Espejo, E.; Company-Morales, M.; Larrea-Killinger, C. Motivating Pregnant and Breastfeeding Women in Spain to Avoid Persistent Toxic Substances in Their Diet. Int. J. Environ. Res. Public Health 2020, 17, 8719. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17238719
Fontalba-Navas A, Zafra Aparici E, Prata-Gaspar MCdM, Herrera-Espejo E, Company-Morales M, Larrea-Killinger C. Motivating Pregnant and Breastfeeding Women in Spain to Avoid Persistent Toxic Substances in Their Diet. International Journal of Environmental Research and Public Health. 2020; 17(23):8719. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17238719
Chicago/Turabian StyleFontalba-Navas, Andres, Eva Zafra Aparici, Maria Clara de Moraes Prata-Gaspar, Esther Herrera-Espejo, Miguel Company-Morales, and Cristina Larrea-Killinger. 2020. "Motivating Pregnant and Breastfeeding Women in Spain to Avoid Persistent Toxic Substances in Their Diet" International Journal of Environmental Research and Public Health 17, no. 23: 8719. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17238719