SARS-CoV-2 Pandemic Impact on Pediatric Emergency Rooms: A Multicenter Study

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Director—General’s Openings Remarks at the Media Briefing on COVID-19. 11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 28 October 2020).
- Istituto Superiore di Sanità. Epicentro. Epidemia COVID-19. Available online: https://www.epicentro.iss.it/coronavirus/sars-cov-2-dashboard (accessed on 23 November 2020).
- Chan, J.F.-W.; Yuan, S.; Kok, K.-H.; To, K.K.-W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.-Y.; Poon, R.W.-S.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Cai, J.; Wang, X.; Zhao, J.; Ge, Y.; Xu, J.; Tian, H.; Chang, H.; Xia, A.; Wang, J.; Zhang, J.; et al. Comparison of Clinical and Epidemiological Characteristics of Asymptomatic and Symptomatic SARS-CoV-2 Infection in Children. Virol. Sin. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Li, X.; Zhu, B.; Liang, H.; Fang, C.; Gong, Y.; Guo, Q.; Sun, X.; Zhao, D.; Shen, J.; et al. Characteristics of pediatric SARS-CoV-2 infection and potential evidence for persistent fecal viral shedding. Nat. Med. 2020, 26, 502–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, J.; Han, B.; Wang, J. COVID-19: Gastrointestinal Manifestations and Potential Fecal–Oral Transmission. Gastroenterology 2020, 158, 1518–1519. [Google Scholar] [CrossRef] [PubMed]
- Singh, T.; Heston, S.M.; Langel, S.N.; Blasi, M.; Hurst, J.H.; Fouda, G.G.; Kelly, M.S.; Permar, S.R. Lessons From COVID-19 in Children: Key Hypotheses to Guide Preventative and Therapeutic Strategies. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Xiao, F.; Tang, M.; Zheng, X.; Liu, Y.; Li, X.; Shan, H. Evidence for Gastrointestinal Infection of SARS-CoV-2. Gastroenterology 2020, 158, 1831–1833.e3. [Google Scholar] [CrossRef] [PubMed]
- Bialek, S.; Gierke, R.; Hughes, M.; McNamara, L.A.; Pilishvili, T.; Skoff, T. Coronavirus Disease 2019 in Children—United States, February 12–April 2, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 422–426. [Google Scholar] [CrossRef]
- Fontanet, A.; Tondeur, L.; Madec, Y.; Grant, R.; Besombes, C.; Jolly, N.; Pellerin, S.F.; Ungeheuer, M.-N.; Cailleau, I.; Kuhmel, L.; et al. Cluster of COVID-19 in Northern France: A Retrospective Closed Cohort Study. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Stein-Zamir, C.; Abramson, N.; Shoob, H.; Libal, E.; Bitan, M.; Cardash, T.; Cayam, R.; Miskin, I. A large COVID-19 outbreak in a high school 10 days after schools’ reopening, Israel, May 2020. Eurosurveillance 2020, 25, 2001352. [Google Scholar] [CrossRef]
- Torres, J.P.; Piñera, C.; De La Maza, V.; Lagomarcino, A.J.; Simian, D.; Torres, B.; Urquidi, C.; Valenzuela, M.T.; O’Ryan, M. Severe Acute Respiratory Syndrome Coronavirus 2 Antibody Prevalence in Blood in a Large School Community Subject to a Coronavirus Disease 2019 Outbreak: A Cross-sectional Study. Clin. Infect. Dis. 2020, 955. [Google Scholar] [CrossRef]
- Ahmed, W.; Angel, N.; Edson, J.; Bibby, K.; Bivins, A.; O’Brien, J.W.; Choi, P.M.; Kitajima, M.; Simpson, S.L.; Li, J.; et al. First confirmed detection of SARS-CoV-2 in untreated wastewater in Australia: A proof of concept for the wastewater surveillance of COVID-19 in the community. Sci. Total. Environ. 2020, 728, 138764. [Google Scholar] [CrossRef] [PubMed]
- La Rosa, G.; Iaconelli, M.; Mancini, P.; Ferraro, G.B.; Veneri, C.; Bonadonna, L.; Lucentini, L.; Suffredini, E. First detection of SARS-CoV-2 in untreated wastewaters in Italy. Sci. Total. Environ. 2020, 736, 139652. [Google Scholar] [CrossRef] [PubMed]
- Kitajima, M.; Ahmed, W.; Bibby, K.; Carducci, A.; Gerba, C.P.; Hamilton, K.A.; Haramoto, E.; Rose, J.B. SARS-CoV-2 in wastewater: State of the knowledge and research needs. Sci. Total. Environ. 2020, 739, 139076. [Google Scholar] [CrossRef] [PubMed]
- Cristiani, L.; Mancino, E.; Matera, L. Will children reveal their secret? The coronavirus dilemma. Eur. Respir. J. 2020, 55, 2000749. [Google Scholar] [CrossRef] [Green Version]
- Cao, Q.; Chen, Y.-C.; Chen, C.-L.; Chiu, C.-H. SARS-CoV-2 infection in children: Transmission dynamics and clinical characteristics. J. Formos. Med. Assoc. 2020, 119, 670–673. [Google Scholar] [CrossRef]
- Larsen, B.; Da, S.; Al, G. Faculty Opinions recommendation of Potential Maternal and Infant Outcomes from (Wuhan) Coronavirus 2019-nCoV Infecting Pregnant Women: Lessons from SARS, MERS, and Other Human Coronavirus Infections. Fac. Opin. Post Publ. Peer Rev. Biomed. Lit. 2020, 12, 194. [Google Scholar] [CrossRef]
- Castagnoli, R.; Votto, M.; Licari, A.; Brambilla, I.; Bruno, R.; Perlini, S.; Rovida, F.; Baldanti, F.; Marseglia, G.L. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in Children and Adolescents. JAMA Pediatr. 2020, 174, 882. [Google Scholar] [CrossRef] [Green Version]
- Lu, X.; Zhang, L.; Du, H.; Zhang, J.; Li, Y.Y.; Qu, J.; Zhang, W.; Wang, Y.; Bao, S.; Li, Y.; et al. SARS-CoV-2 Infection in Children. N. Engl. J. Med. 2020, 382, 1663–1665. [Google Scholar] [CrossRef] [Green Version]
- Cavallo, F.; Rossi, N.; Chiarelli, F. Novel coronavirus infection and children. Acta Bio-Med. Atenei Parm. 2020, 91, 172–176. [Google Scholar]
- Götzinger, F.; Santiago-García, B.; Noguera-Julián, A.; Lanaspa, M.; Lancella, L.; Carducci, F.; Gabrovska, N.; Velizarova, S.; Prunk, P.; Osterman, V.; et al. COVID-19 in children and adolescents in Europe: A multinational, multicentre cohort study. Lancet Child Adolesc. Health 2020. [Google Scholar] [CrossRef]
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiology of COVID-19 Among Children in China. Pediatrics 2020, 145, e20200702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, C.; Gu, J.; Chen, Q.; Deng, N.; Li, J.; Huang, L.; Zhou, X. Clinical and epidemiological characteristics of pediatric SARS-CoV-2 infections in China: A multicenter case series. PLoS Med. 2020, 17, e1003130. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Liu, S.; Chen, L.; Zhuang, L.; Zhang, J.; Xin, Y. The clinical characteristics of pediatric inpatients with SARS-CoV-2 infection: A meta-analysis and systematic review. J. Med. Virol. 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Yan, H.; Guo, W. Clinical Characteristics of Children With COVID-19: A Meta-Analysis. Front. Pediatr. 2020, 8, 431. [Google Scholar] [CrossRef] [PubMed]
- Du, W.; Yu, J.; Wang, H.; Zhang, X.; Zhang, S.; Li, Q.; Zhang, Z. Clinical characteristics of COVID-19 in children compared with adults in Shandong Province, China. Infection 2020, 48, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Qiu, H.; Wu, J.; Hong, L.; Luo, Y.; Song, Q.; Chen, D. Clinical and epidemiological features of 36 children with coronavirus disease 2019 (COVID-19) in Zhejiang, China: An observational cohort study. Lancet Infect. Dis. 2020, 20, 689–696. [Google Scholar] [CrossRef] [Green Version]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Shen, K.-L.; Yang, Y.; Wang, T.; Zhao, D.; Jiang, Y.; Jin, R.; Zheng, Y.; Xu, B.; Xie, Z.; Lin, L.; et al. Diagnosis, treatment, and prevention of 2019 novel coronavirus infection in children: Experts’ consensus statement. World J. Pediatr. 2020, 16, 223–231. [Google Scholar] [CrossRef] [Green Version]
- Luo, S.; Zhang, X.; Xu, H. Don’t Overlook Digestive Symptoms in Patients With 2019 Novel Coronavirus Disease (COVID-19). Clin. Gastroenterol. Hepatol. 2020, 18, 1636–1637. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patient infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Tong, S. Epidemiological characteristics of 2143 pediatric patients with 2019 coronavirus disease in China. Pediatrics 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shekerdemian, L.S.; Mahmood, N.R.; Wolfe, K.K.; Riggs, B.J.; Ross, C.E.; McKiernan, C.A.; Heidemann, S.M.; Kleinman, L.C.; Sen, A.I.; Hall, M.W.; et al. Characteristics and Outcomes of Children With Coronavirus Disease 2019 (COVID-19) Infection Admitted to US and Canadian Pediatric Intensive Care Units. JAMA Pediatr. 2020, 174, 868. [Google Scholar] [CrossRef] [PubMed]
- Zheng, F.; Liao, C.; Fan, Q.-H.; Chen, H.-B.; Zhao, X.-G.; Xie, Z.-G.; Li, X.-L.; Chen, C.-B.; Lu, X.-X.; Liu, Z.-S.; et al. Clinical Characteristics of Children with Coronavirus Disease 2019 in Hubei, China. Curr. Med. Sci. 2020, 40, 275–280. [Google Scholar] [CrossRef] [Green Version]
- Decreto del Presidente del Consiglio dei Ministri. 9 March 2020. Available online: https://www.gazzettaufficiale.it/eli/id/2020/03/09/20A01558/sg (accessed on 28 October 2020).
- Remuzzi, A.; Remuzzi, G. COVID-19 and Italy: What next? Lancet 2020, 395, 1225–1228. [Google Scholar] [CrossRef]
- Presidenza del Consiglio dei Ministri, Linee di Indirizzo per la Promozione e il Miglioramento della Qualità, della Sicurezza e Dell’appropriatezza degli Interventi Assistenziali in Area Pediatrico-Adolescenziale. Available online: http://www.salute.gov.it/portale/news/p3_2_1_1_1.jsp?lingua=italiano&menu=notizie&p=dalministero&id=3256 (accessed on 28 October 2020).
- Linee di indirizzo nazionali sul triage intraospedaliero. Ministero della salute. 2019. Available online: http://www.salute.gov.it/imgs/C_17_notizie_3849_listaFile_itemName_1_file.pdf (accessed on 28 October 2020).
- Li, H.; Yu, G.; Duan, H.; Fu, J.; Shu, Q. Changes in Children’s Healthcare Visits During Coronavirus Disease-2019 Pandemic in Hangzhou, China. J. Pediatr. 2020, 224, 146–149. [Google Scholar] [CrossRef]
- Baum, A.; Schwartz, M.D. Admissions to Veterans Affairs Hospitals for Emergency Conditions During the COVID-19 Pandemic. JAMA 2020, 324, 96. [Google Scholar] [CrossRef]
- NHS England. A&E Attendances and Emergency Admissions 2019–20: Adjusted Monthly. A&E Time Series. 2020. Available online: https://www.england.nhs.uk/statistics/statistical-work-areas/ae-waiting-times-and-activity/ae-attendances-and-emergency-admissions-2019-20/ (accessed on 28 October 2020).
- Raza, M.W.; Iqbal, M.Z.; Ahmed, M.I.; Nawaz, T. Emergency Surgery during Lockdown: Experience at a tertiary care hospital. J. Rawalpindi Med. Coll. 2020, 24, 63–66. [Google Scholar] [CrossRef]
- Grandi, G.; Del Savio, M.C.; Caroli, M.; Capobianco, G.; Dessole, F.; Tupponi, G.; Petrillo, M.; Succu, C.; Paoletti, A.M.; Facchinetti, F. The impact of COVID-19 lockdown on admission to gynecological emergency departments: Results from a multicenter Italian study. Int. J. Gynecol. Obstet. 2020, 151, 39–42. [Google Scholar] [CrossRef]
- Oseran, A.S.; Nash, D.; Kim, C.; Moisuk, S.; Lai, P.Y.; Pyhtila, J.; Sequist, T.D.; Wsafy, J.H. Changes in Hospital Admissions for Urgent Conditions During COVID-19 Pandemic. Am. J. Manag. Care 2020, 26, 327–328. [Google Scholar]
- Rausa, E.; Kelly, M.E.; Manfredi, R.; Riva, I.; Lucianetti, A. Impact of COVID-19 on attendances to a major emergency department: An Italian perspective. Intern. Med. J. 2020, 50, 1159–1160. [Google Scholar] [CrossRef] [PubMed]
- Gallo, O.; Locatello, L.G.; Orlando, P.; Martelli, F.; Bruno, C.; Cilona, M.; Fancello, G.; Mani, R.; Vitali, D.; Bianco, G.; et al. The clinical consequences of the COVID -19 lockdown: A report from an Italian referral ENT department. Laryngoscope 2020, 5, 824–831. [Google Scholar] [CrossRef] [PubMed]
- Ojetti, V.; Covino, M.; Brigida, M.; Petruzziello, C.; Saviano, A.; Migneco, A.; Candelli, M.; Franceschi, F. Non-COVID Diseases during the Pandemic: Where Have All Other Emergencies Gone? Medicina 2020, 56, 512. [Google Scholar] [CrossRef] [PubMed]
- Bhambhvani, H.P.; Rodrigues, A.J.; Yu, J.S.; Carr, J.B.; Gephart, M.H. Hospital Volumes of 5 Medical Emergencies in the COVID-19 Pandemic in 2 US Medical Centers. JAMA Intern. Med. 2020. [Google Scholar] [CrossRef]
- Gissey, L.C.; Casella, G.; Russo, M.F.; Del Corpo, G.; Iodice, A.; Lattina, I.; Ferrari, P.; Iannone, I.; Mingoli, A.; La Torre, F. Impact of COVID-19 outbreak on emergency surgery and emergency department admissions: An Italian level 2 emergency department experience. BJS 2020, 107. [Google Scholar] [CrossRef]
- Cheng, V.C.-C.; Wong, S.-C.; Chuang, V.W.-M.; So, S.Y.-C.; Chen, J.H.-K.; Sridhar, S.; To, K.K.-W.; Chan, J.F.-W.; Hung, I.F.-N.; Ho, P.-L.; et al. The role of community-wide wearing of face mask for control of coronavirus disease 2019 (COVID-19) epidemic due to SARS-CoV-2. J. Infect. 2020, 81, 107–114. [Google Scholar] [CrossRef]
- Cheng, V.C.-C.; Wong, S.-C.; Chan, V.W.-M.; So, S.Y.-C.; Chen, J.H.-K.; Yip, C.C.-Y.; Chan, K.-H.; Chu, H.; Chung, T.W.-H.; Sridhar, S.; et al. Air and environmental sampling for SARS-CoV-2 around hospitalized patients with coronavirus disease 2019 (COVID-19). Infect. Control Hosp. Epidemiol. 2020, 41, 1–8. [Google Scholar] [CrossRef]
- Leung, N.H.L.; Chu, D.K.W.; Shiu, E.Y.C.; Chan, K.-H.; McDevitt, J.J.; Hau, B.J.P.; Yen, H.-L.; Li, Y.; Ip, D.K.M.; Peiris, J.S.M.; et al. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat. Med. 2020, 26, 676–680. [Google Scholar] [CrossRef] [Green Version]
- Kampf, G.; Brüggemann, Y.; Kaba, H.; Steinmann, J.; Pfaender, S.; Scheithauer, S. Potential sources, modes of transmission and effectiveness of prevention measures against SARS-CoV-2. J. Hosp. Infect. 2020, 106, 678–697. [Google Scholar] [CrossRef]
- Chin, A.W.H.; Chu, J.T.S.; Perera, M.R.; Hui, K.P.Y.; Yen, H.-L.; Chan, M.C.W.; Peiris, M.; Poon, L.L. Stability of SARS-CoV-2 in different environmental conditions. Lancet Microbe 2020, 1, e10. [Google Scholar] [CrossRef]
- Kratzel, A.; Todt, D.; V’Kovski, P.; Steiner, S.; Gultom, M.; Thao, T.T.N.; Ebert, N.; Holwerda, M.; Steinmann, J.; Niemeyer, D.; et al. Inactivation of Severe Acute Respiratory Syndrome Coronavirus 2 by WHO-Recommended Hand Rub Formulations and Alcohols. Emerg. Infect. Dis. 2020, 26, 1592–1595. [Google Scholar] [CrossRef] [PubMed]
- Rabenau, H.; Kampf, G.; Cinatl, J.; Doerr, H. Efficacy of various disinfectants against SARS coronavirus. J. Hosp. Infect. 2005, 61, 107–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bae, S.; Kim, M.-C.; Kim, J.Y.; Cha, H.-H.; Lim, J.S.; Jung, J.; Oh, D.K.; Lee, M.-K.; Choi, S.-H.; Sung, M.; et al. Effectiveness of Surgical and Cotton Masks in Blocking SARS–CoV-2: A Controlled Comparison in 4 Patients. Ann. Intern. Med. 2020, 173, W22–W23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]
- Koo, J.R.; Cook, A.R.; Park, M.; Sun, Y.; Sun, H.; Lim, J.T.; Tam, C.; Dickens, B.L. Interventions to mitigate early spread of SARS-CoV-2 in Singapore: A modelling study. Lancet Infect. Dis. 2020, 20, 678–688. [Google Scholar] [CrossRef] [Green Version]
- WHO. Rational use of personal protective equipment for coronavirus disease (COVID-19) and considerations during severe shortages. In Interim Guidance; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Rodríguez-Barranco, M.; Rivas-García, L.; Quiles, J.L.; Redondo-Sánchez, D.; Aranda-Ramírez, P.; Llopis-González, J.; Pérez, M.J.S.; Sanchez-Gonzalez, C. The spread of SARS-CoV-2 in Spain: Hygiene habits, sociodemographic profile, mobility patterns and comorbidities. Environ. Res. 2021, 192, 110223. [Google Scholar] [CrossRef]
- Grüber, C.; Keil, T.; Kulig, M.; Roll, S.; Wahn, U.; Wahn, V. The MAS-90 Study Group History of respiratory infections in the first 12 yr among children from a birth cohort. Pediatr. Allergy Immunol. 2008, 19, 505–512. [Google Scholar] [CrossRef]
- Blecker, S.; Jones, S.A.; Petrilli, C.M.; Admon, A.J.; Weerahandi, H.; Francois, F.; Horwitz, L.I. Hospitalizations for Chronic Disease and Acute Conditions in the Time of COVID-19. JAMA Intern. Med. 2020, 26. [Google Scholar] [CrossRef]
- Papadopoulos, N.G.; Custovic, A.; Deschildre, A.; Mathioudakis, A.G.; Phipatanakul, W.; Wong, G.; Xepapadaki, P.; Agache, I.; Bacharier, L.; Bonini, M.; et al. Impact of COVID-19 on Pediatric Asthma: Practice Adjustments and Disease Burden. J. Allergy Clin. Immunol. Pr. 2020, 8, 2592–2599.e3. [Google Scholar] [CrossRef]
- Matsumoto, K.; Saito, H. Does asthma affect morbidity or severity of COVID-19? J. Allergy Clin. Immunol. 2020, 146, 55–57. [Google Scholar] [CrossRef]
- Kimura, H.; Francisco, D.; Conway, M.; Martinez, F.D.; Vercelli, D.; Polverino, F.; Billheimer, D.; Kraft, M. Type 2 inflammation modulates ACE2 and TMPRSS2 in airway epithelial cells. J. Allergy Clin. Immunol. 2020, 146, 80–88.e8. [Google Scholar] [CrossRef] [PubMed]
- Barroso, B.; Valverde-Monge, M.; Cañas, J.A.; Rodrigo-Muñoz, J.M.; Gonzalez-Cano, B.; Villalobos-Violan, V.; Betancor, D.; Gomez-Cardeñosa, A.; Vallejo-Chamorro, G.; Baptista, L.; et al. Presenting prevalence, characteristics and outcome of asthmatic patients with T2 diseases in hospitalized subjects with COVID-19 in Madrid, Spain. J. Investig. Allergol. Clin. Immunol. 2020, 30, 382–384. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Ortega, J.; López-Carrasco, V.; Barranco, P.; Ifim, M.; Luna, J.A.; Romero, D.; Quirce, S. Early experiences of SARS-CoV-2 infection in severe asthmatics receiving biologic therapy. J. Allergy Clin. Immunol. Pr. 2020, 8, 2784–2786. [Google Scholar] [CrossRef] [PubMed]
- Chhiba, K.D.; Patel, G.B.; Vu, T.H.T.; Chen, M.M.; Guo, A.; Kudlaty, E.; Mai, Q.; Yeh, C.; Muhammad, L.N.; Harris, K.E.; et al. Prevalence and characterization of asthma in hospitalized and nonhospitalized patients with COVID-19. J. Allergy Clin. Immunol. 2020, 146, 307–314.e4. [Google Scholar] [CrossRef] [PubMed]
- Rial, M.J.; Valverde, M.; Del Pozo, V.; González-Barcala, F.J.; Martínez-Rivera, C.; Muñoz, X.; Olaguibel, J.M.; Plaza, V.; Curto, E.; Quirce, S.; et al. Clinical characteristics in 545 patients with severe asthma on biological treatment during the COVID-19 outbreak. J. Allergy Clin. Immunol. Pr. 2020. [Google Scholar] [CrossRef]
- Grandbastien, M.; Piotin, A.; Godet, J.; Abessolo-Amougou, I.; Ederlé, C.; Enache, I.; Fraisse, P.; Hoang, T.C.T.; Kassegne, L.; Labani, A.; et al. SARS-CoV-2 Pneumonia in Hospitalized Asthmatic Patients Did Not Induce Severe Exacerbation. J. Allergy Clin. Immunol. Pr. 2020, 8, 2600–2607. [Google Scholar] [CrossRef]
- Cosgriff, R.; Ahern, S.; Bell, S.C.; Brownlee, K.; Burgel, P.-R.; Byrnes, C.; Corvol, H.; Cheng, S.Y.; Elbert, A.; Faro, A.; et al. A multinational report to characterise SARS-CoV-2 infection in people with cystic fibrosis. J. Cyst. Fibros. 2020, 19, 355–358. [Google Scholar] [CrossRef]
- Viganò, M.; Mantovani, L.; Cozzolino, P.; Harari, S. Correction to: Treat all COVID 19‑positive patients, but do not forget those negative with chronic diseases. Intern. Emerg. Med. 2020, 1. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef]
- Panuccio, A.; Pinto, L.; Urbino, A.; Lubrano, R.; Guidi, B.; Zampogna, S.; Cantoni, B. I nuovi modelli di Triage. In Proceedings of the XII National Congress, Società Italiana di Medicina di Emergenza ed Urgenza Pediatrica (SIMEUP), Padova, Italy, 27–29 October 2016. [Google Scholar]
- Lazzerini, M.; Barbi, E.; Apicella, A.; Marchetti, F.; Cardinale, F.; Trobia, G. Delayed access or provision of care in Italy resulting from fear of COVID-19. Lancet Child Adolesc. Health 2020, 4, e10–e11. [Google Scholar] [CrossRef]
- Lynn, R.M.; Avis, J.L.; Lenton, S.; Amin-Chowdhury, Z.; Ladhani, S.N. Delayed access to care and late presentations in children during the COVID-19 pandemic: A snapshot survey of 4075 paediatricians in the UK and Ireland. Arch. Dis. Child. 2020. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, M.M.; D’Onofrio, G.; Paek, H.; Platts-Mills, T.F.; Soares, W.E.; Hoppe, J.A.; Genes, N.; Nath, B.; Melnick, E.R. Trends in Emergency Department Visits and Hospital Admissions in Health Care Systems in 5 States in the First Months of the COVID-19 Pandemic in the US. JAMA Intern. Med. 2020, 180, 1328–1333. [Google Scholar] [CrossRef] [PubMed]
- Thornton, J. Covid-19: A&E visits in England fall by 25% in week after lockdown. BMJ 2020, 369, m1401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isba, R.; Edge, R.; Jenner, R.; Broughton, E.; Francis, N.; Butler, J. Where have all the children gone? Decreases in paediatric emergency department attendances at the start of the COVID-19 pandemic of 2020. Arch. Dis. Child. 2020, 105. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
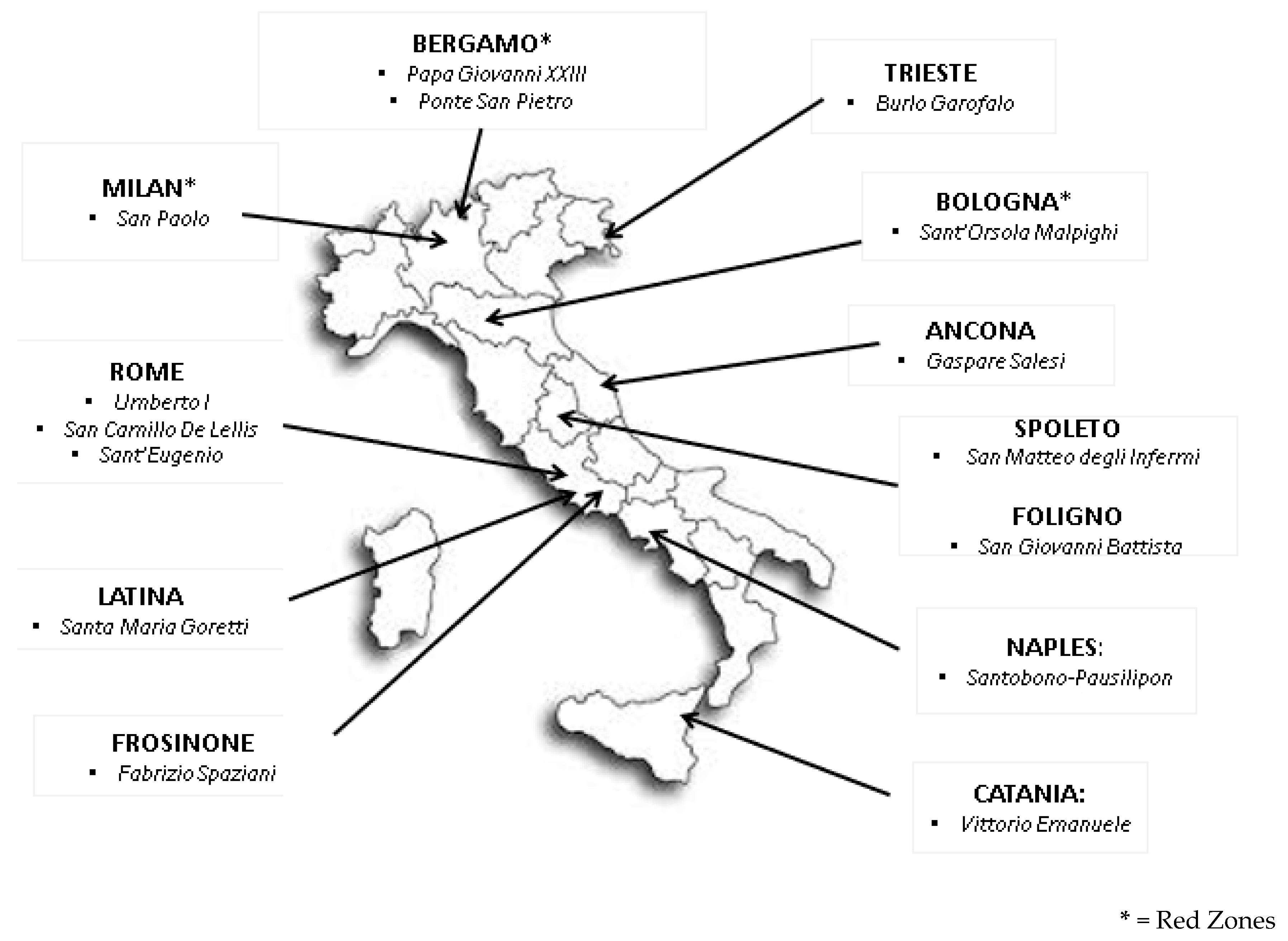
| Hospitals | 2019 | 2020 | Decrease |
|---|---|---|---|
| Umberto I—Rome | 3735 | 674 | −82% |
| San Camillo—Rome | 2240 | 400 | −82% |
| Sant’Eugenio—Rome | 1744 | 90 | −95% |
| Santa Maria Goretti—Latina | 1321 | 220 | −83% |
| Burlo-Garofolo—Trieste | 4127 | 1111 | −73% |
| Vittorio Emanuele—Catania | 2000 | 208 | −90% |
| Gaspare Salesi—Ancona | 4044 | 895 | −78% |
| San Paolo—Milan | 2234 | 189 | −92% |
| Ponte San Pietro—Bergamo | 1814 | 169 | −91% |
| Papa Giovanni XIII—Bergamo | 4191 | 762 | −82% |
| Sant’Orsola Malpighi—Bologna | 3893 | 1083 | −72% |
| Santobono—Naples | 16,797 | 3869 | −77% |
| San Matteo degli Infermi—Spoleto | 247 | 57 | −77% |
| Fabrizio Spaziani—Frosinone | 2757 | 262 | −90% |
| San Giovanni Battista—Foligno | 1220 | 123 | −90% |
| Total | 52,364 | 10,112 | −81% |
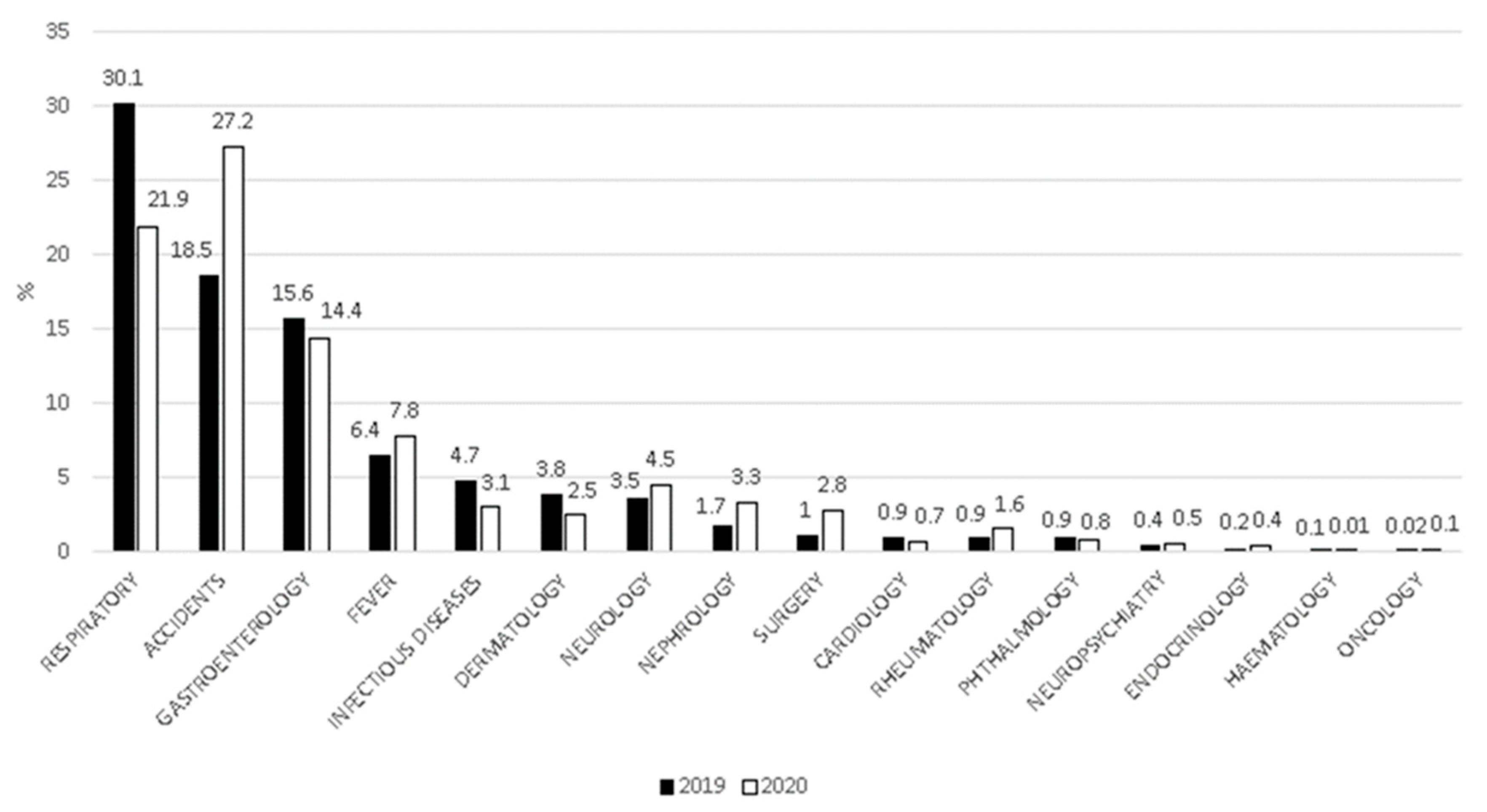
| Diseases | 2019 (n = 52,364) | 2020 (n = 10,112) | p Value |
|---|---|---|---|
| Air communicable diseases | 25,462 (48.6%) | 2934 (29%) | p < 0.001 |
| Non-air communicable diseases | 26,902 (51.4%) | 7178 (71%) |
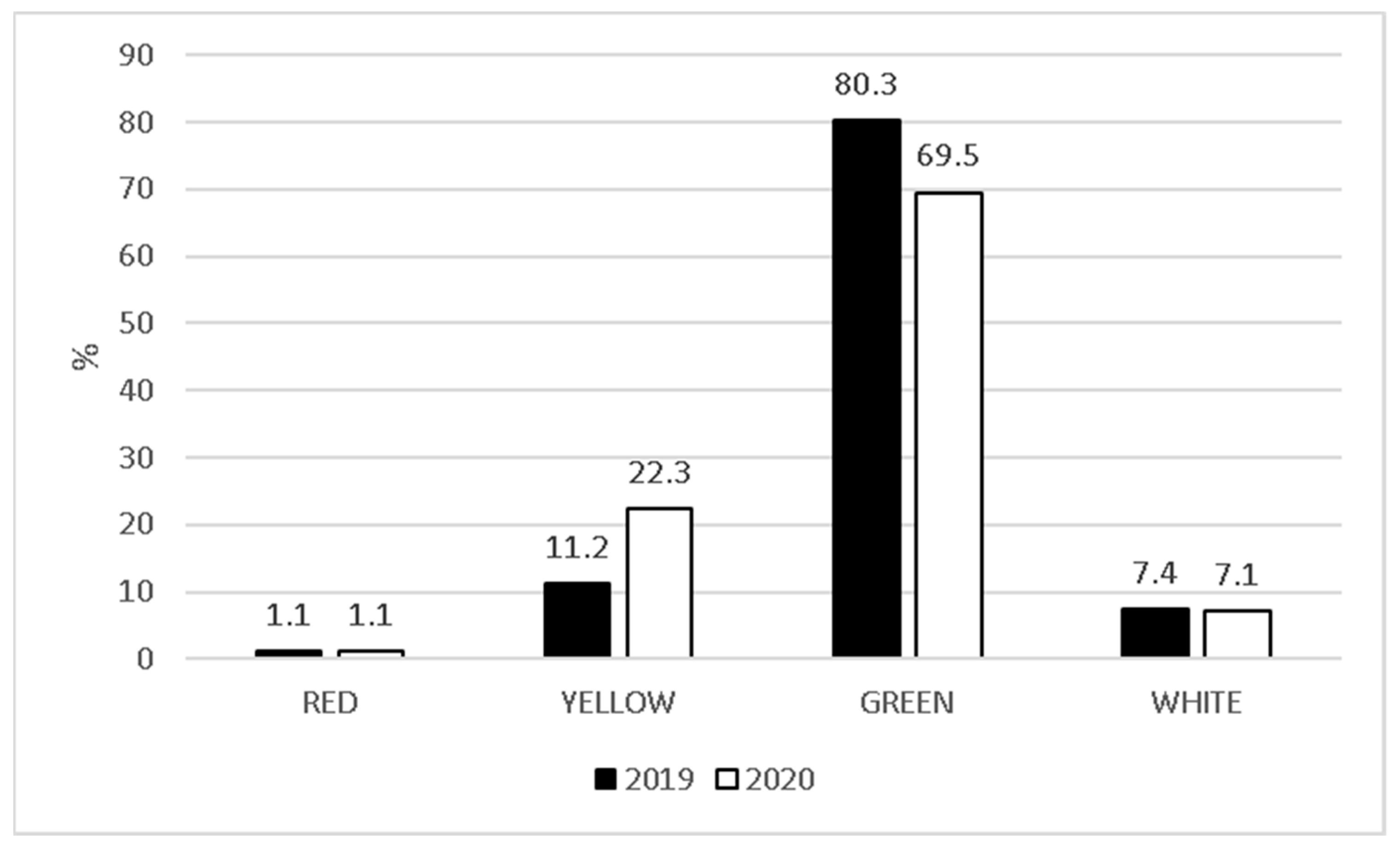
| Triage Categories | High-Incidence Areas | Low-Incidence Areas | p Value | |
|---|---|---|---|---|
| RED | 2019 | 71 (0.6%) | 337 (0.8%) | 0.79 |
| 2020 | 18 (0.8%) | 79 (1.0%) | ||
| YELLOW | 2019 | 1267 (10.4%) | 4411 (10.9%) | <0.001 |
| 2020 | 279 (12.6%) | 1301 (16.4%) | ||
| GREEN | 2019 | 9824 (81.0%) | 30,883 (76.8%) | <0.001 |
| 2020 | 1613 (73.2%) | 5726 (72.5%) | ||
| WHITE | 2019 | 958 (7.9%) | 4575 (11.4%) | <0.001 |
| 2020 | 302 (13.7%) | 770 (9.7%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matera, L.; Nenna, R.; Rizzo, V.; Ardenti Morini, F.; Banderali, G.; Calvani, M.; Calvi, M.; Cozzi, G.; Fabiani, E.; Falsaperla, R.; et al. SARS-CoV-2 Pandemic Impact on Pediatric Emergency Rooms: A Multicenter Study. Int. J. Environ. Res. Public Health 2020, 17, 8753. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17238753
Matera L, Nenna R, Rizzo V, Ardenti Morini F, Banderali G, Calvani M, Calvi M, Cozzi G, Fabiani E, Falsaperla R, et al. SARS-CoV-2 Pandemic Impact on Pediatric Emergency Rooms: A Multicenter Study. International Journal of Environmental Research and Public Health. 2020; 17(23):8753. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17238753
Chicago/Turabian StyleMatera, Luigi, Raffaella Nenna, Valentina Rizzo, Francesca Ardenti Morini, Giuseppe Banderali, Mauro Calvani, Matteo Calvi, Giorgio Cozzi, Elisabetta Fabiani, Raffaele Falsaperla, and et al. 2020. "SARS-CoV-2 Pandemic Impact on Pediatric Emergency Rooms: A Multicenter Study" International Journal of Environmental Research and Public Health 17, no. 23: 8753. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17238753