Impact of Decreased Night Work on Workers’ Musculoskeletal Symptoms: A Quasi-Experimental Intervention Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
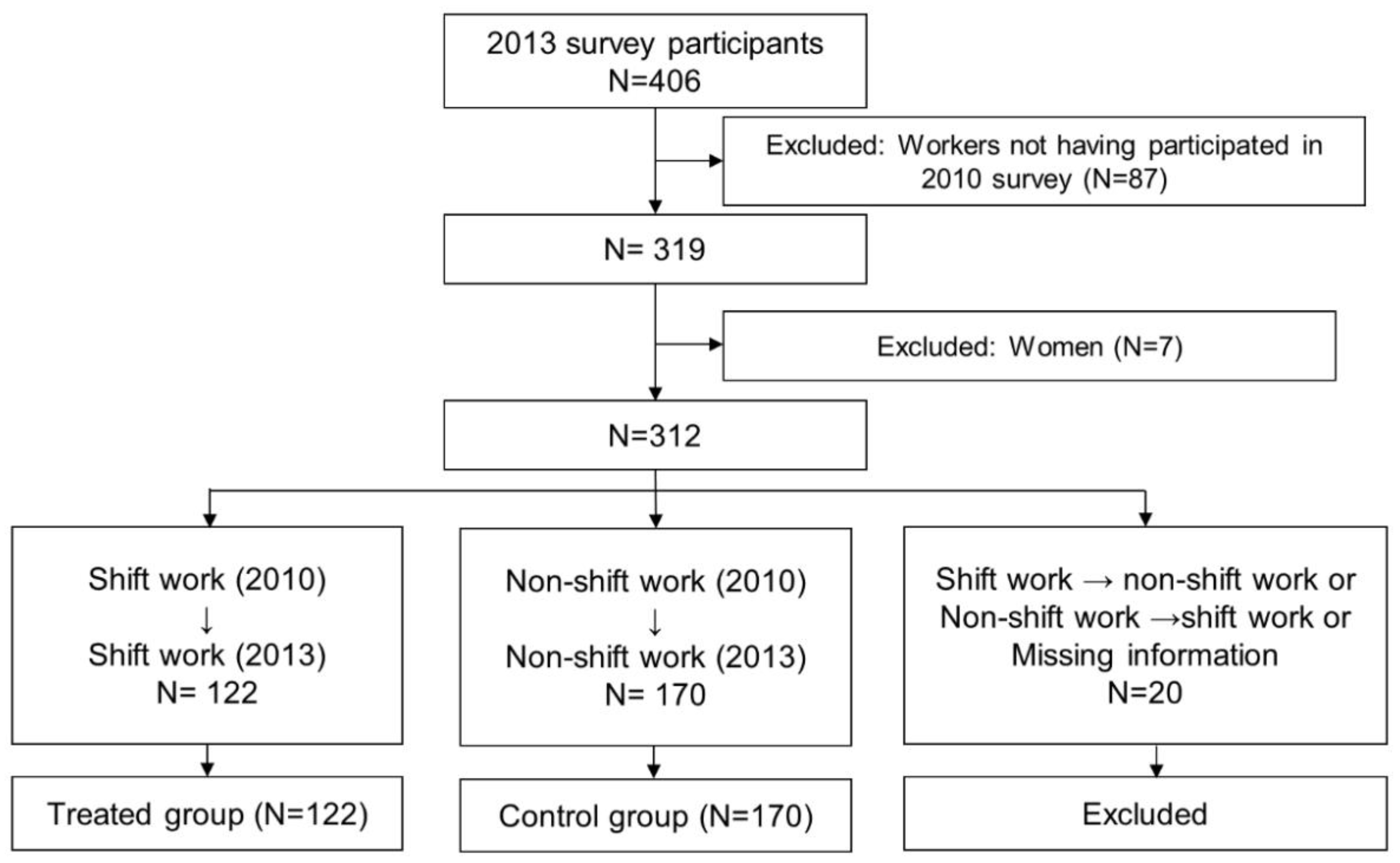
2.2. Study Population
2.3. Measures
2.4. Statistical Analysis
2.5. Parallel Trends Assumption
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lunn, R.M.; Blask, D.E.; Coogan, A.N.; Figueiro, M.G.; Gorman, M.R.; Hall, J.E.; Hansen, J.; Nelson, R.J.; Panda, S.; Smolensky, M.H.; et al. Health consequences of electric lighting practices in the modern world: A report on the National Toxicology Program’s workshop on shift work at night, artificial light at night, and circadian disruption. Sci. Total Environ. 2017, 607–608, 1073–1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parent-Thirion, A.; Biletta, I.; Cabrita, J.; Llave Vargas, O.; Vermeylen, G.; Wilczynska, A.; Wilkens, M. 6th European Working Conditions Survey: Overview Report; 2017 update; Publications Office of the European Union: Luxembourg, 2017; ISBN 978-92-897-1596-6. [Google Scholar]
- Park, J.; Lee, N. First Korean Working Conditions Survey: A comparison between South Korea and EU countries. Ind. Health 2009, 47, 50–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barro, D.; Olinto, M.T.A.; Macagnan, J.B.A.; Henn, R.L.; Pattussi, M.P.; Faoro, M.W.; da Garcez, A.S.; Paniz, V.M.V. Job characteristics and musculoskeletal pain among shift workers of a poultry processing plant in Southern Brazil. J. Occup. Health 2015, 57, 448–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choobineh, A.; Soltanzadeh, A.; Tabatabaee, H.; Jahangiri, M.; Khavaji, S. Health effects associated with shift work in 12-hour shift schedule among Iranian petrochemical employees. Int. J. Occup. Saf. Ergon. JOSE 2012, 18, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Kärkkäinen, S.; Ropponen, A.; Narusyte, J.; Mather, L.; Åkerstedt, T.; Silventoinen, K.; Mittendorfer-Rutz, E.; Svedberg, P. Night work as a risk factor of future disability pension due to musculoskeletal diagnoses: A prospective cohort study of Swedish twins. Eur. J. Public Health 2017, 27, 659–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, Y.; Zhao, S.; An, Z.; Wang, S.; Li, H.; Lu, L.; Yao, S. The associations of work style and physical exercise with the risk of work-related musculoskeletal disorders in nurses. Int. J. Occup. Med. Environ. Health 2019, 32, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Uhlig, B.L.; Sand, T.; Nilsen, T.I.; Mork, P.J.; Hagen, K. Insomnia and risk of chronic musculoskeletal complaints: Longitudinal data from the HUNT study, Norway. BMC Musculoskelet. Disord. 2018, 19, 128. [Google Scholar] [CrossRef]
- Ropponen, A.; Silventoinen, K.; Hublin, C.; Svedberg, P.; Koskenvuo, M.; Kaprio, J. Sleep patterns as predictors for disability pension due to low back diagnoses: A 23-year longitudinal study of Finnish twins. Sleep 2013, 36, 891–897. [Google Scholar] [CrossRef] [Green Version]
- Kang, D.; Kim, Y.; Lee, Y.-I.; Koh, S.; Kim, I.; Lee, H. Work-related Musculoskeletal Disorders in Korea Provoked by Workers’ Collective Compensation Claims against Work Intensification. Ann. Occup. Environ. Med. 2014, 26, 19. [Google Scholar] [CrossRef]
- Bhattacharya, A. Costs of occupational musculoskeletal disorders (MSDs) in the United States. Int. J. Ind. Ergon. 2014, 44, 448–454. [Google Scholar] [CrossRef]
- Attarchi, M.; Raeisi, S.; Namvar, M.; Golabadi, M. Association between shift working and musculoskeletal symptoms among nursing personnel. Iran. J. Nurs. Midwifery Res. 2014, 19, 309–314. [Google Scholar] [PubMed]
- Zhao, I.; Bogossian, F.; Turner, C. The effects of shift work and interaction between shift work and overweight/obesity on low back pain in nurses: Results from a longitudinal study. J. Occup. Environ. Med. 2012, 54, 820–825. [Google Scholar] [CrossRef] [PubMed]
- Park, T. A Road to the Reduction of Working Time: In Search of the Day-time Two-shift System in Hyundai Motor Company. Labor Policy Res. 2013, 13, 1–29. [Google Scholar]
- Schlevis, R.M.; Oude Hengel, K.M.; Burdorf, A.; Blatter, B.M.; Strijk, J.E.; van der Beek, A.J. Evaluation of occupational health interventions using a randomized controlled trial: Challenges and alternative research designs. Scand. J. Work. Environ. Health 2015, 41, 491–503. [Google Scholar] [CrossRef] [Green Version]
- Baron, S.; Hales, T.; Hurrell, J. Evaluation of symptom surveys for occupational musculoskeletal disorders. Am. J. Ind. Med. 1996, 29, 609–617. [Google Scholar] [CrossRef]
- Bernard, B.; Sauter, S.; Fine, L.; Petersen, M.; Hales, T. Job task and psychosocial risk factors for work-related musculoskeletal disorders among newspaper employees. Scand. J. Work. Environ. Health 1994, 20, 417–426. [Google Scholar] [CrossRef] [Green Version]
- David, G.; Woods, V.; Li, G.; Buckle, P. The development of the Quick Exposure Check (QEC) for assessing exposure to risk factors for work-related musculoskeletal disorders. Appl. Ergon. 2008, 39, 57–69. [Google Scholar] [CrossRef]
- Lee, J.W.; Lee, J.J.; Mun, H.J.; Lee, K.-J.; Kim, J.J. The Relationship between Musculoskeletal Symptoms and Work-related Risk Factors in Hotel Workers. Ann. Occup. Environ. Med. 2013, 25, 20. [Google Scholar] [CrossRef] [Green Version]
- Sveinsdottir, H. Self-assessed quality of sleep, occupational health, working environment, illness experience and job satisfaction of female nurses working different combination of shifts. Scand. J. Caring Sci. 2006, 20, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Parkes, K.R. Shiftwork, Job Type, and the Work Environment as Joint Predictors of Health-Related Outcomes. J. Occup. Health Psychol. 1999, 4, 256–268. [Google Scholar] [CrossRef]
- Thorbjörnsson, C.B.; Alfredsson, L.; Fredriksson, K.; Michélsen, H.; Punnett, L.; Vingård, E.; Torgén, M.; Kilbom, Å. Physical and Psychosocial Factors Related to Low Back Pain During a 24-Year Period: A Nested Case–Control Analysis. Spine 2000, 25, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, Y.; Miura, K.; Ishizaki, M.; Nakagawa, H.; Kido, T.; Naruse, Y.; Nogawa, K. Sickness absence and shift work among Japanese factory workers. J. Hum. Ergol. (Tokyo) 2001, 30, 393–398. [Google Scholar]
- Trinkoff, A.M.; Le, R.; Geiger-Brown, J.; Lipscomb, J.; Lang, G. Longitudinal relationship of work hours, mandatory overtime, and on-call to musculoskeletal problems in nurses. Am. J. Ind. Med. 2006, 49, 964–971. [Google Scholar] [CrossRef] [PubMed]
- Dattilo, M.; Antunes, H.K.M.; Medeiros, A.; Mônico Neto, M.; Souza, H.S.; Tufik, S.; de Mello, M.T. Sleep and muscle recovery: Endocrinological and molecular basis for a new and promising hypothesis. Med. Hypotheses 2011, 77, 220–222. [Google Scholar] [CrossRef]
- Dudek, M.; Meng, Q.-J. Running on time: The role of circadian clocks in the musculoskeletal system. Biochem. J. 2014, 463, 1–8. [Google Scholar] [CrossRef]
- Chun, M.Y.; Cho, B.-J.; Yoo, S.H.; Oh, B.; Kang, J.-S.; Yeon, C. Association between sleep duration and musculoskeletal pain: The Korea National Health and Nutrition Examination Survey 2010–2015. Medicine (Baltimore) 2018, 97, e13656. [Google Scholar] [CrossRef]
- Rasmussen-Barr, E.; Grooten, W.J.A.; Hallqvist, J.; Holm, L.W.; Skillgate, E. Are job strain and sleep disturbances prognostic factors for neck/shoulder/arm pain? A cohort study of a general population of working age in Sweden. BMJ Open 2014, 4, e005103. [Google Scholar] [CrossRef] [Green Version]
- Salo, P.; Oksanen, T.; Sivertsen, B.; Hall, M.; Pentti, J.; Virtanen, M.; Vahtera, J.; Kivimäki, M. Sleep disturbances as a predictor of cause-specific work disability and delayed return to work. Sleep 2010, 33, 1323–1331. [Google Scholar] [CrossRef]
- Takahashi, M.; Iwakiri, K.; Sotoyama, M.; Hirata, M.; Hisanaga, N. Musculoskeletal pain and night-shift naps in nursing home care workers. Occup. Med. Oxf. Engl. 2009, 59, 197–200. [Google Scholar] [CrossRef] [Green Version]
- Fischer, F.M.; Silva-Costa, A.; Griep, R.H.; Smolensky, M.H.; Bohle, P.; Rotenberg, L. Working Time Society consensus statements: Psychosocial stressors relevant to the health and wellbeing of night and shift workers. Ind. Health 2019, 57, 175–183. [Google Scholar] [CrossRef] [Green Version]
- Menzel, N.N. Psychosocial factors in musculoskeletal disorders. Crit. Care Nurs. Clin. North Am. 2007, 19, 145–153. [Google Scholar] [CrossRef]
- Mäntyniemi, A.; Oksanen, T.; Salo, P.; Virtanen, M.; Sjösten, N.; Pentti, J.; Kivimäki, M.; Vahtera, J. Job strain and the risk of disability pension due to musculoskeletal disorders, depression or coronary heart disease: A prospective cohort study of 69,842 employees. Occup. Environ. Med. 2012, 69, 574–581. [Google Scholar] [CrossRef] [PubMed]
- Buckle, P.W.; Devereux, J.J. The nature of work-related neck and upper limb musculoskeletal disorders. Appl. Ergon. 2002, 33, 207–217. [Google Scholar] [CrossRef]
- Hoe, V.C.; Urquhart, D.M.; Kelsall, H.L.; Zamri, E.N.; Sim, M.R. Ergonomic interventions for preventing work-related musculoskeletal disorders of the upper limb and neck among office workers. Cochrane Database Syst. Rev. 2018, 10, CD008570. [Google Scholar] [CrossRef] [PubMed]
- Punnett, L.; Wegman, D.H. Work-related musculoskeletal disorders: The epidemiologic evidence and the debate. J. Electromyogr. Kinesiol. 2004, 14, 13–23. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Treated (N = 122) | Control (N = 170) | p | |||
|---|---|---|---|---|---|
| Mean ± SD | N (%) | Mean ± SD | N (%) | ||
| Age | 42.2 ± 4.5 | 45.2 ± 4.8 | <0.0001 | ||
| Education | 0.50 | ||||
| <High school | 0 (0.0) | 4 (2.4) | |||
| High school | 98 (80.3) | 125 (73.5) | |||
| >High school | 23 (18.9) | 35 (20.6) | |||
| Missing | 1 (0.8) | 6 (3.5) | |||
| Working years | 18.6 ± 4.2 | 21.2 ± 3.9 | <0.0001 | ||
| Income (KRW 10,000 per year) | 5273 ± 803 (2010) | 5092 ± 702 (2010) | 0.07 | ||
| 6246 ± 666 (2013) | 6307 ± 694 (2013) | 0.45 | |||
| Weekly working hours * | 52.6 ± 8.8 (2010) | 51.6 ± 9.3 (2010) | 0.39 | ||
| 45.9 ± 3.4 (2013) | 45.6 ± 3.0 (2013) | 0.39 | |||
| QEC—back | 23.0 ± 8.4 | 25.1 ± 9.2 | 0.06 | ||
| QEC—shoulder/arm | 27.4 ± 9.1 | 29.2 ± 9.2 | 0.13 | ||
| QEC—wrist/hand | 23.4 ± 8.0 | 24.6 ± 8.0 | 0.23 | ||
| QEC—neck | 9.2 ± 4.2 | 9.6 ± 4.3 | 0.44 | ||
| Pre | Post | Difference (Post–Pre) | DID (Unadjusted) | DID (Adjusted) a | |
|---|---|---|---|---|---|
| Body Site | % | % | % | % (95% CI) | % (95% CI) |
| Neck | |||||
| Treated | 48.4 | 47.5 | −0.8 | 5.1 (−6.0, 16.1) | 5.4 (−6.3, 17.0) |
| Control | 50.6 | 44.7 | −5.9 | ||
| Shoulder | |||||
| Treated | 54.9 | 50.8 | −4.1 | −11.8 ** (−23.3, −0.2) | −10.3 * (−22.2, 1.6) |
| Control | 51.8 | 59.4 | 7.7 | ||
| Arm | |||||
| Treated | 30.3 | 21.3 | −9.0 | −13.7 ** (−25.1, −2.3) | −12.9 ** (−24.7, −1.2) |
| Control | 24.1 | 28.8 | 4.7 | ||
| Hand | |||||
| Treated | 42.6 | 37.7 | −4.9 | −7.9 (−20.0, 4.3) | −5.9 (−18.2, 6.5) |
| Control | 31.2 | 34.1 | 2.9 | ||
| Back | |||||
| Treated | 48.4 | 53.3 | 4.9 | 4.3 (−8.2, 16.9) | 6.4 (−6.7, 19.5) |
| Control | 47.7 | 48.2 | 0.6 | ||
| Leg | |||||
| Treated | 36.1 | 29.5 | −6.6 | −8.9 (−20.6, 2.8) | −8.9 (−21.1, 3.2) |
| Control | 27.7 | 30.0 | 2.4 | ||
| All sites b | |||||
| Treated | 80.3 | 81.2 | 0.8 | −11.0 ** (−20.1, −1.8) | −9.2 ** (−18.3, −0.2) |
| Control | 71.8 | 83.5 | 11.8 | ||
| Upper extremities c | |||||
| Treated | 70.5 | 64.8 | −5.7 | −16.3 ** (−27.1, −5.5) | −14.8 ** (−25.9, −3.8) |
| Control | 60.0 | 70.6 | 10.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.-E.; Choi, M.; Kim, H.-R.; Kawachi, I. Impact of Decreased Night Work on Workers’ Musculoskeletal Symptoms: A Quasi-Experimental Intervention Study. Int. J. Environ. Res. Public Health 2020, 17, 9092. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239092
Lee H-E, Choi M, Kim H-R, Kawachi I. Impact of Decreased Night Work on Workers’ Musculoskeletal Symptoms: A Quasi-Experimental Intervention Study. International Journal of Environmental Research and Public Health. 2020; 17(23):9092. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239092
Chicago/Turabian StyleLee, Hye-Eun, Min Choi, Hyoung-Ryoul Kim, and Ichiro Kawachi. 2020. "Impact of Decreased Night Work on Workers’ Musculoskeletal Symptoms: A Quasi-Experimental Intervention Study" International Journal of Environmental Research and Public Health 17, no. 23: 9092. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17239092