Orofacial Trauma on the Anterior Zone of a Trumpet’s Player Maxilla: Concept of the Oral Rehabilitation—A Case Report

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Case Preparation
2.2. Data Collection of the Trumpet Sound Quality
2.3. Feature Extraction and Selection
3. Results
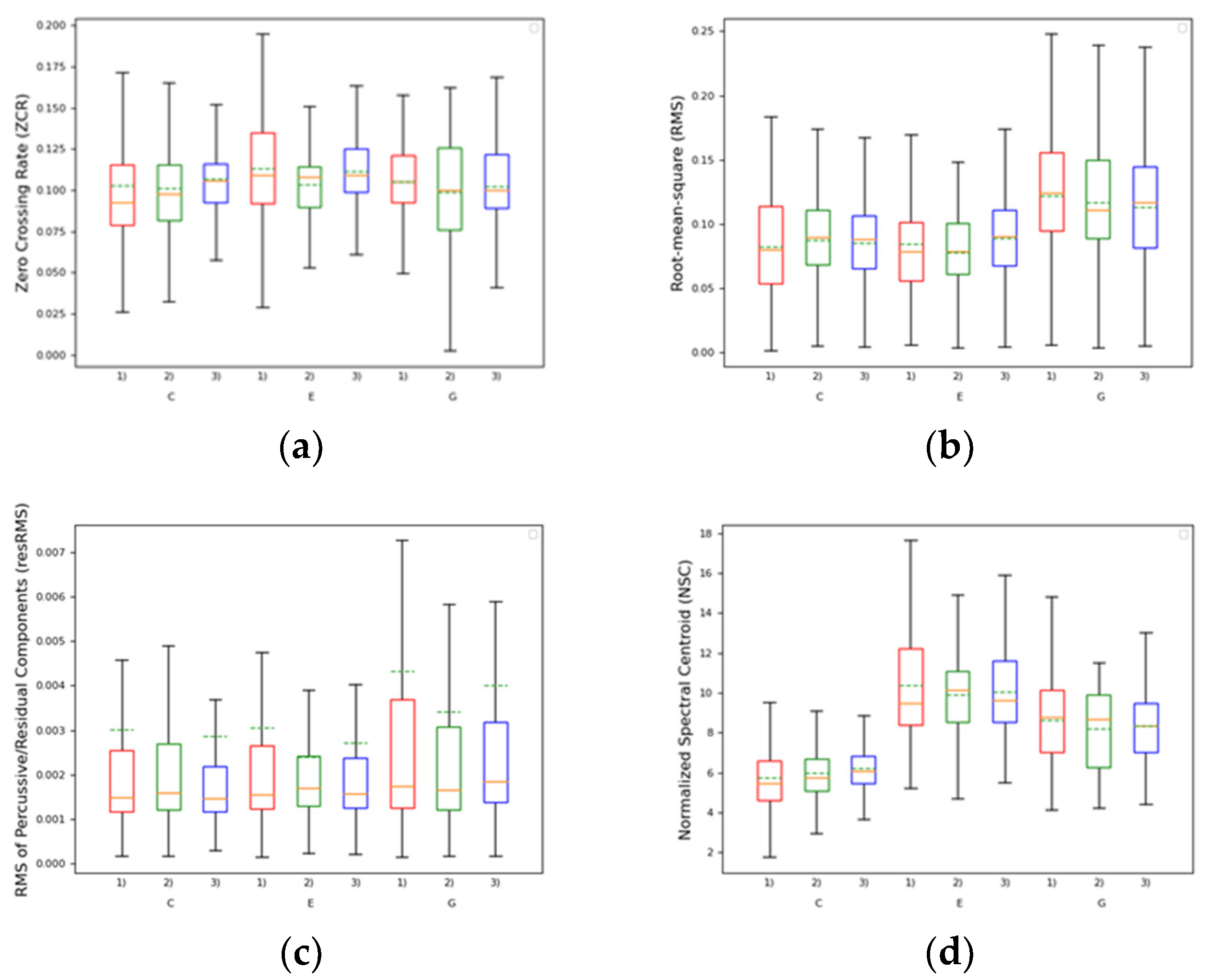
3.1. Pitch
3.2. Loudness
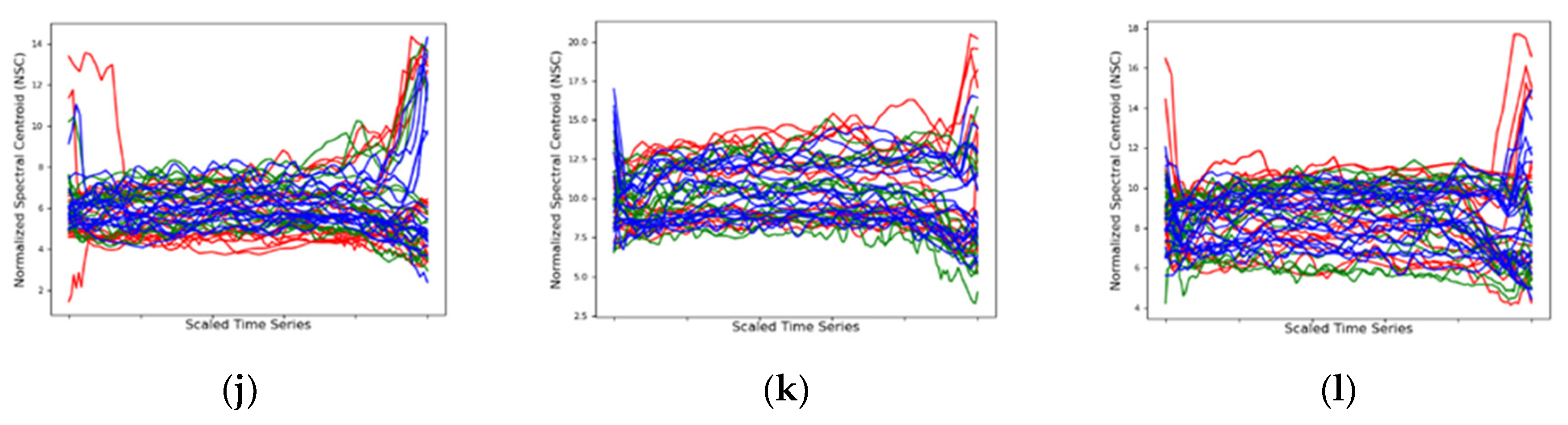
3.3. Timbre
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bouchardet, F.; de Souza Côrtes, M.; Bastos, J.; Caldas, I.; Franco, A.; Vieira, D. The impact of tooth avulsion on daily life performance using the Brazilian OIDP index in children and young adults. J. Forensic Odonto-Stomatol. 2014, 32, 9–14. [Google Scholar]
- Goswami, M.; Kumar, P.; Bhushan, U. Evaluation of Knowledge, Awareness, and Occurrence of Dental Injuries in Participant Children during Sports in New Delhi: A Pilot Study. Int. J. Clin. Pediatr. Dent. 2017, 10, 373–378. [Google Scholar] [PubMed]
- Emerich, K.; Czerwinska, M.; Ordyniec-Kwasnica, I. Immediate self-replantation of an avulsed permanent mandibular incisor—A case report. Dent. Traumatol. Off. Publ. Int. Assoc. Dent. Traumatol. 2010, 26, 443–446. [Google Scholar] [CrossRef] [PubMed]
- de Jesus Soares, A.; do Prado, M.; Farias Rocha Lima, T.; Gomes, B.P.F.d.A.; Augusto Zaia, A.; José de Souza-Filho, F. The multidisciplinary management of avulsed teeth: A case report. Iran Endod. J. 2012, 7, 203–206. [Google Scholar] [PubMed]
- Emerich, K.; Kaczmarek, J. First aid for dental trauma caused by sports activities: State of knowledge, treatment and prevention. Sports Med. 2010, 40, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Inouye, J.; McGrew, C. Dental problems in athletes. Curr. Sports Med. Rep. 2015, 14, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Krasner, P. Treatment of avulsed teeth by oral and maxillofacial surgeons. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2010, 68, 2888–2892. [Google Scholar] [CrossRef]
- Lin, S.; Zuckerman, O.; Fuss, Z.; Ashkenazi, M. New emphasis in the treatment of dental trauma: Avulsion and luxation. Dent. Traumatol. 2007, 23, 297–303. [Google Scholar] [CrossRef]
- Hiremath, G.; Kidiyoor, K.H. Avulsion and storage media. J. Investig. Clin. Dent. 2011, 2, 89–94. [Google Scholar] [CrossRef]
- Young, E.J.; Macias, C.R.; Stephens, L. Common Dental Injury Management in Athletes. Sports Health 2015, 7, 250–255. [Google Scholar] [CrossRef] [Green Version]
- Abd-Elmeguid, A.; ElSalhy, M.; Yu, D.C. Pulp canal obliteration after replantation of avulsed immature teeth: A systematic review. Dent. Traumatol. 2015, 31, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Maniglia-Ferreira, C.; de Almeida Gomes, F.; Vitoriano, M.M. Intentional Replantation of an Avulsed Immature Permanent Incisor: A Case Report. J. Endod. 2017, 43, 1383–1386. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.M.; Williams, S.; Davidson, L.E.; Drummond, B.K. Orofacial and dental trauma of young children in Dunedin, New Zealand. Dent. Traumatol. 2011, 27, 199–202. [Google Scholar] [CrossRef] [PubMed]
- Garbin, C.A.S.; Guimarães e Queiroz, A.P.D.d.; Rovida, T.A.S.; Garbin, A.J.I. Occurrence of traumatic dental injury in cases of domestic violence. Braz. Dent. J. 2012, 23, 72–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frontera, R.R.; Zanin, L.; Ambrosano, G.M.; Flório, F.M. Orofacial trauma in Brazilian basketball players and level of information concerning trauma and mouthguards. Dent. Traumatol. Off. Publ. Int. Assoc. Dent. Traumatol. 2011, 27, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Bergman, L.; Milardović Ortolan, S.; Žarković, D.; Viskić, J.; Jokić, D.; Mehulić, K. Prevalence of dental trauma and use of mouthguards in professional handball players. Dent. Traumatol. Off. Publ. Int. Assoc. Dent. Traumatol. 2017, 33, 199–204. [Google Scholar] [CrossRef]
- Bazina, A.M.; Peričić, T.P.; Galić, I.; Mihanović, F.; Kovačević, N.; Galić, T. Knowledge and attitudes of water polo coaches about sports-related dental injuries and dental emergency procedures. Dent. Traumatol. 2020, 36, 382–389. [Google Scholar] [CrossRef]
- Hendrick, K.; Farrelly, P.; Jagger, R. Oro-facial injuries and mouthguard use in elite female field hockey players. Dent. Traumatol. 2008, 24, 189–192. [Google Scholar] [CrossRef]
- Sepet, E.; Aren, G.; Dogan Onur, O.; Pinar Erdem, A.; Kuru, S.; Tolgay, C.G.; Unal, S. Knowledge of sports participants about dental emergency procedures and the use of mouthguards. Dent. Traumatol. 2014, 30, 391–395. [Google Scholar] [CrossRef]
- Lechner, K.; Connert, T.; Kühl, S.; Filippi, A. Lip and tooth injuries at public swimming pools in Austria. Dent. Traumatol. Off. Publ. Int. Assoc. Dent. Traumatol. 2017, 33, 214–220. [Google Scholar] [CrossRef]
- Ceallaigh, P.O.; Ekanaykaee, K.; Beirne, C.J.; Patton, D.W. Diagnosis and management of common maxillofacial injuries in the emergency department. Part 5: Dentoalveolar injuries. Emerg. Med. J. 2007, 24, 429–430. [Google Scholar] [CrossRef] [PubMed]
- Emerich, K.; Wyszkowski, J. Clinical practice. Eur. J. Pediatr. 2010, 169, 1045–1050. [Google Scholar] [CrossRef] [PubMed]
- Brüllmann, D.; Schulze, R.K.; d’Hoedt, B. The treatment of anterior dental trauma. Dtsch. Arztebl. Int. 2010, 108, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Pais Clemente, M.; Moreira, A.; Mendes, J.; Pinhão Ferreira, A.; Amarante, J.M. Wind Instrumentalist Embouchure and the Applied Forces on the Perioral Structures. Open Dent. J. 2019, 13, 107–114. [Google Scholar] [CrossRef] [Green Version]
- Pais Clemente, M.; Mendes, J.; Vardasca, R.; Pinhão Ferreira, A.; Amarante, J.M. Combined Acquisition Method of Image and Signal Technique (CAMIST) for Assessment of Temporomandibular Disorders in Performing Arts Medicine. Med. Probl. Perform. Artist. 2018, 33, 205–212. [Google Scholar] [CrossRef]
- Pais Clemente, M.; Mendes, J.; Moreira, A.; Branco, C.; Pinhão Ferreira, A.; Amarante, J.M. Gesture technique analysis of the craniocervical mandibular complex in string and wind instrumentalists. Phys. Med. Rehabil. Res. 2018, 3, 1–7. [Google Scholar] [CrossRef]
- Clemente, M.P.; Mendes, J.; Vardasca, R.; Moreira, A.; Branco, C.A.; Ferreira, A.P.; Amarante, J.M. Infrared thermography of the crânio-cervico-mandibular complex in wind and string instrumentalists. Int. Arch. Occup. Environ. Health 2020, 93, 645–658. [Google Scholar] [CrossRef]
- Clemente, M.; Mendes, J.; Moreira, A.; Bernardes, G.; Van Twillert, H.; Ferreira, A.; Amarante, J.M. A new classification of wind instruments: Orofacial considerations. J. Oral Biol. Craniofac. Res. 2019, 9, 268–276. [Google Scholar] [CrossRef]
- Peeters, G.; Giordano, B.L.; Susini, P.; Misdariis, N.; McAdams, S. The timbre toolbox: Extracting audio descriptors from musical signals. J. Acoust. Soc. Am. 2011, 130, 2902–2916. [Google Scholar] [CrossRef] [Green Version]
- Peeters, G.; McAdams, S.; Herrera, P. Instrument Sound Description in the Context of MPEG-7. In Proceedings of the International Computer Music Conference, Berlin, Germany, 27 August–1 September 2000; pp. 166–169. [Google Scholar]
- McAdams, S.; Winsberg, S.; Donnadieu, S.; De Soete, G.; Krimphoff, J. Perceptual scaling of synthesized musical timbres: Common dimensions, specificities, and latent subject classes. Psychol. Res. 1995, 58, 177–192. [Google Scholar] [CrossRef] [Green Version]
- Eerola, T.; Ferrer, R.; Alluri, V. Timbre and Affect Dimensions: Evidence from Affect and Similarity Ratings and Acoustic Correlates of Isolated Instrument Sounds. Music Percept. 2012, 30, 49–70. [Google Scholar] [CrossRef] [Green Version]
- Elliott, T.M.; Hamilton, L.S.; Theunissen, F.E. Acoustic structure of the five perceptual dimensions of timbre in orchestral instrument tones. J. Acoust. Soc. Am. 2013, 133, 389–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terasawa, H.; Slaney, M.; Berger, J. The Thirteen Colors of Timbre; IEEE Workshop on Applications of Signal Processing to Audio and Acoustics: Piscatawaym, NJ, USA, 2005; pp. 323–326. [Google Scholar]
- Vidwans, A.; Gururani, S.; Wu, C.-W.; Subramanian, V.; Swaminathan, R.V.; Lerch, A. Objective Descriptors for the Assessment of Student Music Performances; AES International Conference on Semantic Audio, Audio Engineering Society: Erlangen, Germany, 2017. [Google Scholar]
- Abeßer, J.; Hasselhorn, J.; Dittmar, C.; Lehmann, A.; Grollmisch, S. Automatic Quality Assessment of Vocal and Instrumental Performances of Ninth-Grade and Tenth-Grade Pupils. In Proceedings of the International Symposium on Computer Music Multidisciplinary Research (CMMR), Marseille, France, 15–18 October 2013. [Google Scholar]
- Han, Y.; Lee, K. Hierarchical Approach to Detect Common Mistakes of Beginner Flute Players. In Proceedings of the International Socieity for Music Information Retrieval Conference (ISMIR), Taipei, Taiwan, 27–31 October 2014; pp. 77–82. [Google Scholar]
- Wu, C.-W.; Gururani, S.; Laguna, C.; Pati, A.; Vidwans, A.; Lerch, A. Towards the Objective Assessment of Music Performances. In Proceedings of the International Conference on Music Perception and Cognition (ICMPC), San Francisco, CA, USA, 5–9 July 2016; pp. 99–103. [Google Scholar]
- Devaney, J.; Mandel, M.; Fujinaga, I. A study of intonation in three-part singing using the Automatic Music Performance Analysis and Comparison Toolkit (AMPACT). In Proceedings of the 13th International Society for Music Information Retrieval Conference, ISMIR, Porto, Portugal, 8–12 October 2012; pp. 511–516. [Google Scholar]
- Mayor, O.; Bonada, J.; Loscos, A. Performance Analysis and Scoring of the Singing Voice. In Proceedings of the 35th International Conference: Audio for Games, London, UK, 2 November 2009; pp. 1–7. [Google Scholar]
- Fitzgerald, D. Harmonic/Percussive Separation using Median Filtering. In Proceedings of the 13th International Conference on Digital Audio Effects (DAFx-10), Graz, Austria, 6–10 September 2010. [Google Scholar]
- Geringer, J.M.; Worthy, M.D. Effects of Tone-Quality Changes on Intonation and Tone-Quality Ratings of High School and College Instrumentalists. J. Res. Music Educ. 1999, 47, 135–149. [Google Scholar] [CrossRef] [Green Version]
- Fouad, A.F.; Abbott, P.V.; Tsilingaridis, G.; Cohenca, N.; Lauridsen, E.; Bourguignon, C.; O’Connell, A.; Flores, M.T.; Day, P.F.; Hicks, L.; et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. Dent. Traumatol. 2020, 36, 331–342. [Google Scholar] [CrossRef]
- Guideline on management of acute dental trauma. Pediatr. Dent. 2008, 30 (Suppl. 7), 175–183.
- Hammel, J.M.; Fischel, J. Dental Emergencies. Emerg. Med. Clin. N. Am. 2019, 37, 81–93. [Google Scholar] [CrossRef]
- DiAngelis, A.J.; Andreasen, J.O.; Ebeleseder, K.A.; Kenny, D.J.; Trope, M.; Sigurdsson, A.; Andersson, L.; Bourguignon, C.; Flores, M.T.; Hicks, M.L.; et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations of permanent teeth. Dent. Traumatol. 2012, 28, 2–12. [Google Scholar] [CrossRef]
- Ranalli, D.N. Dental injuries in sports. Curr. Sports Med. Rep. 2005, 4, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Pohl, Y.; Filippi, A.; Kirschner, H. Results after replantation of avulsed permanent teeth. II. Periodontal healing and the role of physiologic storage and antiresorptive-regenerative therapy. Dent. Traumatol. Off. Publ. Int. Assoc. Dent. Traumatol. 2005, 21, 93–101. [Google Scholar] [CrossRef]
- von Büren, A.; Krastl, G.; Kühl, S.; Filippi, A. Management of avulsions in Switzerland 2007–2010. Dent. Traumatol. 2014, 30, 176–181. [Google Scholar] [CrossRef] [Green Version]
- Santos, M.E.S.M.; Habecost, A.P.Z.; Gomes, F.V.; Weber, J.B.B.; De Oliveira, M.G. Parent and caretaker knowledge about avulsion of permanent teeth. Dent. Traumatol. 2009, 25, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Bahammam, L.A. Knowledge and attitude of emergency physician about the emergency management of tooth avulsion. BMC Oral Health 2018, 18, 57. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues Campos Soares, T.; de Andrade Risso, P.; Cople Maia, L. Traumatic dental injury in permanent teeth of young patients attended at the federal University of Rio de Janeiro, Brazil. Dent. Traumatol. 2014, 30, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Fujita, Y.; Shiono, Y.; Maki, K. Knowledge of emergency management of avulsed tooth among Japanese dental students. BMC Oral Health 2014, 14, 34. [Google Scholar] [CrossRef] [Green Version]
- Mori, G.G.; Turcio, K.H.L.; Borro, V.P.B.; Mariusso, Â.M. Evaluation of the knowledge of tooth avulsion of school professionals from Adamantina, São Paulo, Brazil. Dent. Traumatol. 2007, 23, 2–5. [Google Scholar] [CrossRef]
- Krause-Parello, C.A. Tooth Avulsion in the School Setting. J. Sch. Nurs. 2005, 21, 279–282. [Google Scholar] [CrossRef]
- Marshall, S.; Dawson, D.; Southard, K.A.; Lee, A.N.; Casko, J.S.; Southard, T.E. Transverse molar movements during growth. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 615–624. [Google Scholar] [CrossRef]
- Hesby, R.M.; Marshall, S.D.; Dawson, D.V.; Southard, K.A.; Casko, J.S.; Franciscus, R.G.; Southard, T.E. Transverse skeletal and dentoalveolar changes during growth. Am. J. Orthod. Dentofac. Orthop. Off. Publ. Am. Assoc. Orthod. Its Const. Soc. Am. Board Orthod. 2006, 130, 721–731. [Google Scholar] [CrossRef]
- Thordarson, A.; Johannsdottir, B.; Magnusson, T.E. Craniofacial changes in Icelandic children between 6 and 16 years of age—A longitudinal study. Eur. J. Orthod. 2005, 28, 152–165. [Google Scholar] [CrossRef] [Green Version]
- Trenouth, M.J.; Joshi, M. Proportional Growth of Craniofacial Regions. J. Orofac. Orthop. Fortschr. Der Kieferorthopädie 2006, 67, 92–104. [Google Scholar] [CrossRef]
- Arboleda, C.; Buschang, P.H.; Camacho, J.A.; Botero, P.; Roldan, S. A mixed longitudinal anthropometric study of craniofacial growth of Colombian mestizos 6–17 years of age. Eur. J. Orthod. 2010, 33, 441–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atik, E.; Esen Aydinli, F.; Kulak Kayikçi, M.E.; Ciger, S. Comparing the effects of Essix and Hawley retainers on the acoustics of speech. Eur. J. Orthod. 2017, 39, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Haydar, B.; Karabulut, G.; Özkan, S.; Aksoy, A.Ü.; Ciğer, S. Effects of retainers on the articulation of speech. Am. J. Orthod. Dentofac. Orthop. 1996, 110, 535–540. [Google Scholar] [CrossRef]
- Chen, J.; Wan, J.; You, L. Speech and orthodontic appliances: A systematic literature review. Eur. J. Orthod. 2017, 40, 29–36. [Google Scholar] [CrossRef]
- Dale, D.A. Trumpet Technique/by Delbert A. Dale; Oxford University Press: London, UK; New York, NY, USA; Toronto, ON, Canada, 1965; Volume viii, 93p. [Google Scholar]
- Krumhansl, C.L. Why is musical timbre so hard to understand. Struct. Percept. Electroacoust. Sound Music 1989, 9, 43–53. [Google Scholar]
- McAdams, S.; Cunible, J.-C. Perception of timbral analogies. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 1992, 336, 383–389. [Google Scholar]
- Iverson, P.; Krumhansl, C.L. Isolating the dynamic attributes of musical timbre. J. Acoust. Soc. Am. 1993, 94, 2595–2603. [Google Scholar] [CrossRef] [Green Version]
- Luo, Y.-J.; Su, L.; Yang, Y.-H.; Chi, T.-S. Detection of Common Mistakes in Novice Violin Playing. In Proceedings of the International Society for Music Information Retrieval Conference (ISMIR), Málaga, Spain, 26–30 October 2015; pp. 316–322. [Google Scholar]
- Knight, T.; Upham, F.; Fujinaga, I. The Potential for Automatic Assessment of Trumpet Tone Quality. In Proceedings of the International Society for Music Infromation Retrieval Conference, Miami, FL, USA, 24–28 October 2011; pp. 573–578. [Google Scholar]
- Romani Picas, O.; Parra Rodriguez, H.; Dabiri, D.; Tokuda, H.; Hariya, W.; Oishi, K.; Serra, X. A Real-Time System for Measuring Sound Goodness in Instrumental Sounds; Audio Engineering Society Convention 138: Warsaw, Poland, 2015; pp. 1106–1111. [Google Scholar]
- Lerch, A.; Arthur, C.; Pati, A.; Gururani, S. Music Performance Analysis: A Survey. In Proceedings of the Society for Music Information Retrieval Conference (ISMIR), Delft, The Netherlands, 4–8 November 2019; pp. 33–43. [Google Scholar]
- Madsen, C.K.; Geringer, J.M. Preferences for trumpet tone quality versus intonation. In Bulletin of the Council for Research in Music Education; University of Illinois Press: Champaign, IL, USA, 1976; pp. 13–22. [Google Scholar]
- Mahn, D.H.; Polack, M.A. Esthetic rehabilitation of maxillary incisors in conjunction with flapless surgical techniques, an implant zirconia crown, and porcelain veneers. J. Esthet. Restor. Dent. Off. Publ. Am. Acad. Esthet. Dent. 2009, 21, 294–302. [Google Scholar] [CrossRef]
- Jivraj, S.; Chee, W. Treatment planning of implants in the aesthetic zone. Br. Dent. J. 2006, 201, 77–89. [Google Scholar] [CrossRef] [Green Version]
- Hansson, S.; Halldin, A. Alveolar ridge resorption after tooth extraction: A consequence of a fundamental principle of bone physiology. J. Dent. Biomech. 2012, 3, 1758736012456543. [Google Scholar] [CrossRef]
- Atwood, D.A.; Coy, W.A. Clinical, cephalometric, and densitometric study of reduction of residual ridges. J. Prosthet. Dent. 1971, 26, 280–295. [Google Scholar] [CrossRef]
- Linkevičius, T.; Andrijauskas, R. Zero Bone Loss Concepts; Quintessence Publishing Company, Incorporated: Tokio, Japan, 2019. [Google Scholar]
- Fürhauser, R.; Florescu, D.; Benesch, T.; Haas, R.; Mailath, G.; Watzek, G. Evaluation of soft tissue around single-tooth implant crowns: The pink esthetic score. Clin. Oral Implant. Res. 2005, 16, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Gonzalez-Martin, O.; Weisgold, A.; Lee, E. Considerations of implant abutment and crown contour: Critical contour and subcritical contour. Int. J. Periodontics Restor. Dent. 2010, 30, 335–343. [Google Scholar]
- Gomes, A.L.; Montero, J. Zirconia implant abutments: A review. Med. OralPatol. Oral Y Cir. Bucal 2011, 16, e50–e55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derks, J.; Håkansson, J.; Wennström, J.L.; Tomasi, C.; Larsson, M.; Berglundh, T. Effectiveness of implant therapy analyzed in a Swedish population: Early and late implant loss. J. Dent. Res. 2015, 94 (Suppl. 3), 44s–51s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Boever, A.L.; Quirynen, M.; Coucke, W.; Theuniers, G.; De Boever, J.A. Clinical and radiographic study of implant treatment outcome in periodontally susceptible and non-susceptible patients: A prospective long-term study. Clin. Oral Implant. Res. 2009, 20, 1341–1350. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.A.; Mitra, D.K.; Rodrigues, S.V.; Pathare, P.N.; Podar, R.S.; Vijayakar, H.N. Implants in adolescents. J. Indian Soc. Periodontol. 2013, 17, 546–548. [Google Scholar] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Audio Descriptor | Definition |
|---|---|---|
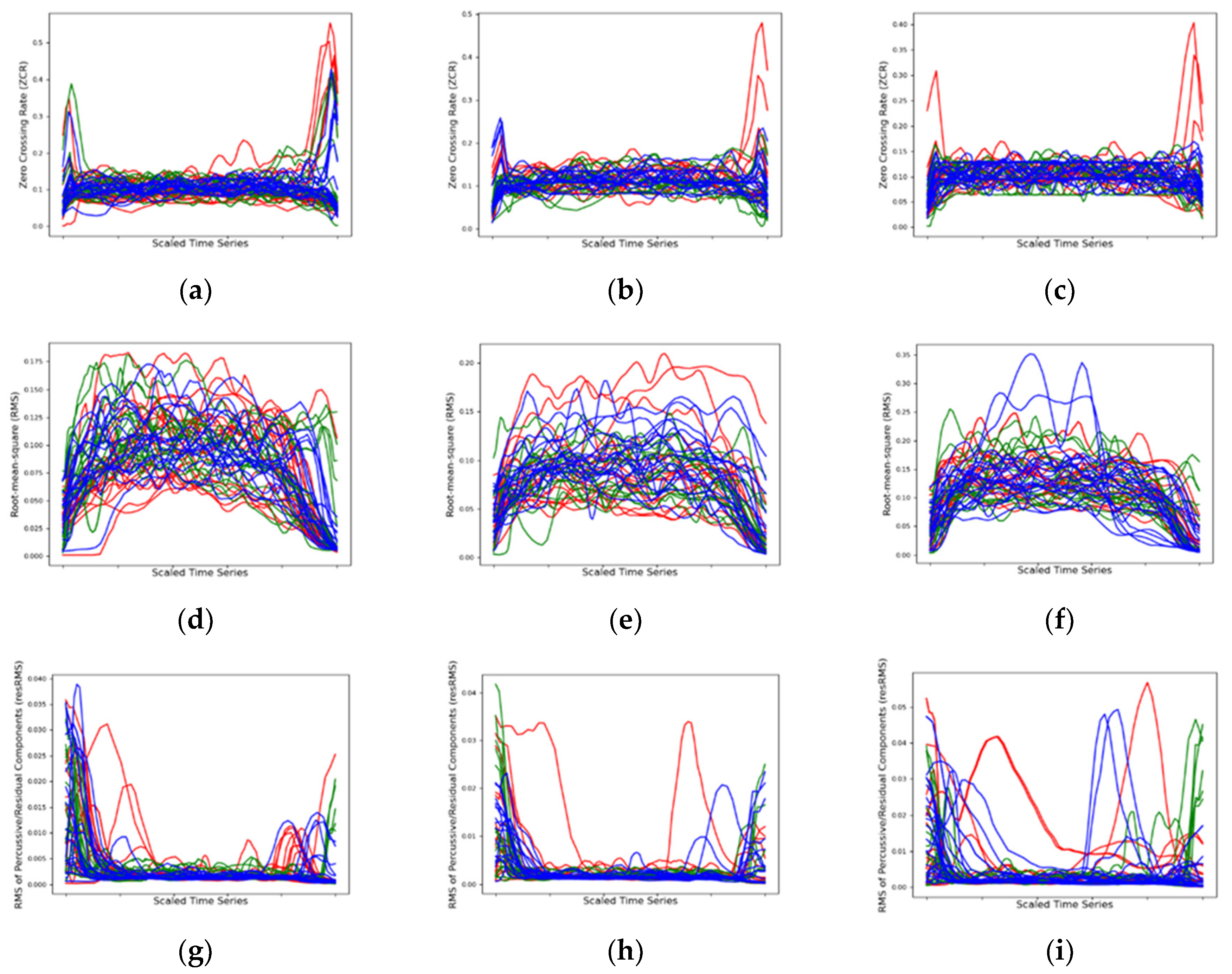
| Pitch | Zero-Crossing Rate (ZCR) | Computes the zero-crossing rate of an audio time series, adopted as a rough indicator of pitch (i.e., fundamental frequency) for monophonic sounds |
| Loudness | Root mean square (RMS) | Computes the energy of an audio signal from its temporal (waveform) manifestation |
| Root mean square of residual sound components (resRMS) | Computes the root mean square (i.e., energy) of the residual components of the sound, resulting from the median filtering method proposed by Fitzgerald, which suppresses stationary signals (i.e., the harmonic components) [41] | |
| Timbre/Harmonic | Normalized spectral centroid (NSC) | Computes the center of gravity of the spectrogram, which is treated as a distribution over frequency bins. We further normalize the centroid value as the ratio to the fundamental frequency, resulting in a “unitless centroid” which allows the comparison of sounds with different fundamental frequencies while guaranteeing a robust perceptual indicator of sound brightness |
| Sound Attribute | Audio Descriptor | Intra-Oral Appliance | Mean | Median | |
|---|---|---|---|---|---|
| Pitch | ZCR | (1) | 0.1065 | 0.1011 | 0.0376 |
| (2) | 0.1013 | 0.1030 | 0.0352 | ||
| (3) | 0.1064 | 0.1064 | 0.0273 | ||
| Loudness RMS | (1) | 0.0962 | 0.0935 | 0.0273 | |
| (2) | 0.0934 | 0.0925 | 0.0470 | ||
| (3) | 0.0966 | 0.0957 | 0.0529 | ||
| resRMS | (1) | 0.0035 | 0.00156 | 0.0018 | |
| (2) | 0.0028 | 0.00165 | 0.0014 | ||
| (3) | 0.0033 | 0.00161 | 0.0013 | ||
| Timbre NSC | (1) | 7.9883 | 7.71546 | 3.8730 | |
| (2) | 7.9586 | 7.61702 | 4.0767 | ||
| (3) | 8.1075 | 7.92492 | 3.0412 | ||
| Chi-Squared (χ2) | p-Value | |
|---|---|---|
| ZCR | 128.391 | <0.001 |
| RMS | 8.221 | 0.0164 |
| resRMS | 5.695 | 0.058 |
| NSC | 715.529 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clemente, M.P.; Moreira, A.; Carvalho, N.; Bernardes, G.; Ferreira, A.P.; Amarante, J.M.; Mendes, J. Orofacial Trauma on the Anterior Zone of a Trumpet’s Player Maxilla: Concept of the Oral Rehabilitation—A Case Report. Int. J. Environ. Res. Public Health 2020, 17, 9423. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249423
Clemente MP, Moreira A, Carvalho N, Bernardes G, Ferreira AP, Amarante JM, Mendes J. Orofacial Trauma on the Anterior Zone of a Trumpet’s Player Maxilla: Concept of the Oral Rehabilitation—A Case Report. International Journal of Environmental Research and Public Health. 2020; 17(24):9423. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249423
Chicago/Turabian StyleClemente, Miguel Pais, André Moreira, Nádia Carvalho, Gilberto Bernardes, Afonso Pinhão Ferreira, José Manuel Amarante, and Joaquim Mendes. 2020. "Orofacial Trauma on the Anterior Zone of a Trumpet’s Player Maxilla: Concept of the Oral Rehabilitation—A Case Report" International Journal of Environmental Research and Public Health 17, no. 24: 9423. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249423