Is Biofeedback through an Intra-Aural Device an Effective Method to Treat Bruxism? Case Series and Initial Experience

 , ,
, , 
Abstract
:1. Introduction
- If the patients by using such devices be aware of their habit and therefore reduce or stop to bruxism
- Whether in-ear devices have a positive impact on patients suffering from bruxism or not.
2. Materials and Methods
2.1. Study Design
2.2. Treatment Procedures
- 1st to 3rd: day 3 h/day (only during the day)
- 4th to 7th day: 2 wearing times of 4 h/day (only during the day)
- 2nd week: if no complaints occurred in the 1st week, start from the 2nd week all day (only during the day)
- 3rd week: in consultation with the patient start of wearing also at night
2.3. Study Variables
2.4. Statistical Analysis
3. Results
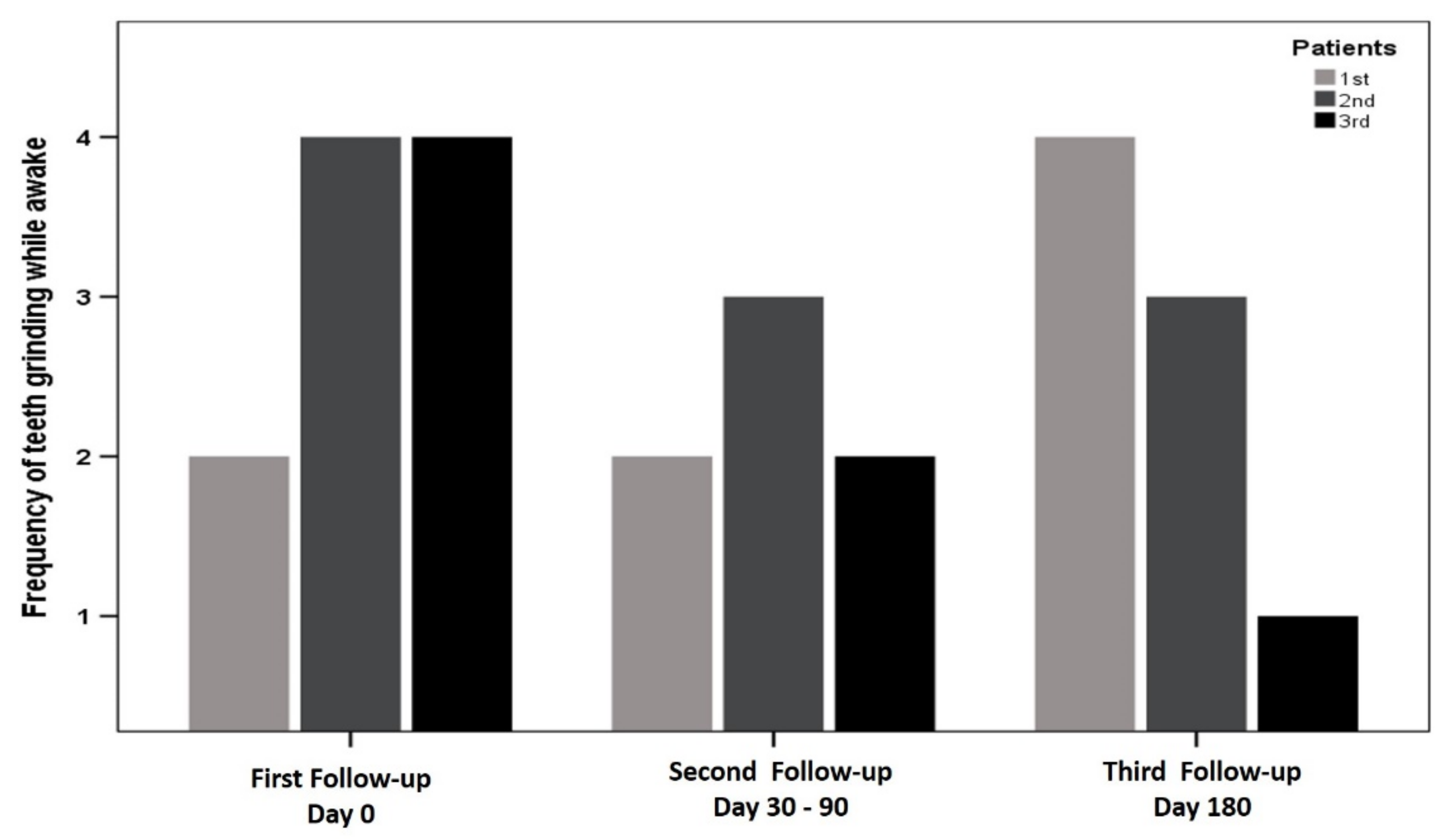
Improvement of Teeth-Grinding
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lobbezoo, F.; Ahlberg, J.; Glaros, A.; Kato, T.; Koyano, K.; Lavigne, G.; De Leeuw, R.; Manfredini, D.; Svensson, P.; Winocur, E. Bruxism defined and graded: An international consensus. J. Oral Rehabil. 2013, 40, 2–4. [Google Scholar] [CrossRef]
- Lobbezoo, F.; Ahlberg, J.; Raphael, K.; Wetselaar, P.; Glaros, A.; Kato, T.; Santiago, V.; Winocur, E.; De Laat, A.; De Leeuw, R. International consensus on the assessment of bruxism: Report of a work in progress. J. Oral Rehabil. 2018, 45, 837–844. [Google Scholar] [CrossRef]
- Wieckiewicz, M.; Winocur, E. Sleep Bruxism—The Controversial Sleep Movement Activity; Multidisciplinary Digital Publishing Institute: Basel, Switzerland, 2020. [Google Scholar]
- Murphy, M.K.; MacBarb, R.F.; Wong, M.E.; Athanasiou, K.A. Temporomandibular joint disorders: A review of etiology, clinical management, and tissue engineering strategies. Int. J. Oral Maxillofac. Implants 2013, 28, e393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, E.; Detamore, M.; Mercuri, L. Degenerative disorders of the temporomandibular joint: Etiology, diagnosis, and treatment. J. Dent. Res. 2008, 87, 296–307. [Google Scholar] [CrossRef] [PubMed]
- Solberg, W.K.; Woo, M.W.; Houston, J.B. Prevalence of mandibular dysfunction in young adults. J. Am. Dent. Assoc. 1979, 98, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, G.; LeResche, L. Epidemiology of temporomandibular disorders. In Temporomandibular Disorders and Related Pain Conditions; Sessle, B.J., Bryant, P.S., Dionne, R.A., Eds.; IASP Press: Seattle, WA, USA, 1995. [Google Scholar]
- Maspero, C.; Cavagnetto, D.; Abate, A.; Cressoni, P.; Farronato, M. Effects on the facial growth of rapid palatal expansion in growing patients affected by juvenile idiopathic arthritis with monolateral involvement of the temporomandibular joints: A case-control study on posteroanterior and lateral cephalograms. J. Clin. Med. 2020, 9, 1159. [Google Scholar] [CrossRef] [PubMed]
- Farronato, G.; Maspero, C.; Esposito, L.; Briguglio, E.; Farronato, D.; Giannini, L. Rapid maxillary expansion in growing patients. Hyrax versus transverse sagittal maxillary expander: A cephalometric investigation. Eur. J. Orthod. 2011, 33, 185–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scrivani, S.J.; Keith, D.A.; Kaban, L.B. Temporomandibular disorders. N. Engl. J. Med. 2008, 359, 2693–2705. [Google Scholar] [CrossRef]
- Ohlmann, B.; Waldecker, M.; Leckel, M.; Bömicke, W.; Behnisch, R.; Rammelsberg, P.; Schmitter, M. Correlations between sleep bruxism and temporomandibular disorders. J. Clin. Med. 2020, 9, 611. [Google Scholar] [CrossRef] [Green Version]
- Molina, O.F.; Santos, J.D.; Mazzetto, M.; Nelson, S.; Nowlin, T.; Mainieri, É.T. Oral jaw behaviors in TMD and bruxism: A comparison study by severity of bruxism. Cranio® 2001, 19, 114–122. [Google Scholar] [CrossRef]
- Melo, G.; Duarte, J.; Pauletto, P.; Porporatti, A.L.; Stuginski-Barbosa, J.; Winocur, E.; Flores-Mir, C.; De Luca Canto, G. Bruxism: An umbrella review of systematic reviews. J. Oral Rehabil. 2019, 46, 666–690. [Google Scholar] [CrossRef]
- Van der Meulen, M.J.; Ohrbach, R.; Aartman, I.H.; Naeije, M.; Lobbezoo, F. Temporomandibular disorder patients’ illness beliefs and self-efficacy related to bruxism. J. Orofac. Pain 2010, 24, 367. [Google Scholar] [PubMed]
- Bereznicki, T.; Barry, E.; Wilson, N.H. Unintended changes to the occlusion following the provision of night guards. Part two: Management. Br. Dent. J. 2019, 226, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Magdaleno, F.; Ginestal, E. Side effects of stabilization occlusal splints: A report of three cases and literature review. Cranio® 2010, 28, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Bereznicki, T.; Barry, E.; Wilson, N. Unintended changes to the occlusion following the provision of night guards. Br. Dent. J. 2018, 225, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Mora, M.C.S.; Weber, D.; Neff, A.; Rief, W. Biofeedback-based cognitive-behavioral treatment compared with occlusal splint for temporomandibular disorder: A randomized controlled trial. Clin. J. Pain 2013, 29, 1057–1065. [Google Scholar] [CrossRef] [PubMed]
- Klasser, G.D.; Greene, C.S. Oral appliances in the management of temporomandibular disorders. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 107, 212–223. [Google Scholar] [CrossRef]
- Frank, D.L.; Khorshid, L.; Kiffer, J.F.; Moravec, C.S.; McKee, M.G. Biofeedback in medicine: Who, when, why and how? Ment. Health Fam. Med. 2010, 7, 85. [Google Scholar]
- Gu, W.; Yang, J.; Zhang, F.; Yin, X.; Wei, X.; Wang, C. Efficacy of biofeedback therapy via a mini wireless device on sleep bruxism contrasted with occlusal splint: A pilot study. J. Biomed. Res. 2015, 29, 160. [Google Scholar]
- Needham, R.; Davies, S. Use of the Grindcare® device in the management of nocturnal bruxism: A pilot study. Br. Dent. J. 2013, 215, E1. [Google Scholar] [CrossRef]
- Kim, K.J.; Lee, K.W.; Bahng, J. Case study of reducing the occlusion effect and improving telephone usage and cosmetic satisfaction by invisible-in-the canal hearing aids. Audiol. Speech Res. 2017, 13, 251–256. [Google Scholar] [CrossRef]
- Soderfeldt, B.; Halling, A.; Americans, A. Cerezen device provides treatment for temporomandibular joint disorders day and night. Br. Dent. J. 2016, 220, 666. [Google Scholar]
- Zhao, N.N.; Evans, R.W.; Byth, K.; Murray, G.M.; Peck, C.C. Development and validation of a screening checklist for temporomandibular disorders. J. Orofac. Pain 2011, 25, 210–222. [Google Scholar] [PubMed]
- John, M.T.; Miglioretti, D.L.; LeResche, L.; Koepsell, T.D.; Hujoel, P.; Micheelis, W. German short forms of the oral health impact profile. Community Dent. Oral Epidemiol. 2006, 34, 277–288. [Google Scholar] [CrossRef]
- Michelotti, A.; Cioffi, I.; Festa, P.; Scala, G.; Farella, M. Oral parafunctions as risk factors for diagnostic TMD subgroups. J. Oral Rehabil. 2010, 37, 157–162. [Google Scholar] [CrossRef]
- Voerman, G.E.; Vollenbroek-Hutten, M.M.; Hermens, H.J. Changes in pain, disability, and muscle activation patterns in chronic whiplash patients after ambulant myofeedback training. Clin. J. Pain 2006, 22, 656–663. [Google Scholar] [CrossRef]
- Tate, J.J.; Milner, C.E. Real-time kinematic, temporospatial, and kinetic biofeedback during gait retraining in patients: A systematic review. Phys. Ther. 2010, 90, 1123–1134. [Google Scholar] [CrossRef] [Green Version]
- Florjanski, W.; Malysa, A.; Orzeszek, S.; Smardz, J.; Olchowy, A.; Paradowska-Stolarz, A.; Wieckiewicz, M. Evaluation of biofeedback usefulness in masticatory muscle activity management—A systematic review. J. Clin. Med. 2019, 8, 766. [Google Scholar] [CrossRef] [Green Version]
- Tavera, A.T.; Montoya, M.C.P.; Calderón, E.F.G.G.; Gorodezky, G.; Wixtrom, R.N. Approaching temporomandibular disorders from a new direction: A randomized controlled clinical trial of the TMD es TM ear system. Cranio® 2012, 30, 172–182. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age | Gender | Initial Diagnose | Symptomes | Relife of Symptoms | Duration of Usage | Discontinuation of Treatment | First Reported Improvements of the Symptomes |
|---|---|---|---|---|---|---|---|---|
| 1 | 58 | f | arthrosis | headaches, pain in teeth, pain in periodontal apparatus, pain in muscles, neck pain | yes | 2 months | yes | 2 months |
| 2 | 23 | f | disc displacement without reduction | headaches, pain in muscles, pain in temporomandibular joint, neck pain | yes | 12 months | no | 3 months |
| 3 | 64 | f | TMD | muscle pain, pain in temporomandibular joint, pain in teeth and periodontal apparatus, neck pain | yes | 11 months | no | 3.5 months |
| 4 | 58 | f | TMD | Headaches, pain in teeth, temporomandibular joint, neck pain | No | 1 month | yes | No beneficial effect |
| 5 | 49 | f | TMD | headaches, pain in muscles, temporomandibular joint, neck pain | NA | 2 months | yes | No effect reported |
| 6 | 35 | f | TMD | headaches, pain in temporomandibular joint, pain in periodontal apparatus, neck pain | yes | 6 months | yes | 1 month |
| 7 | 44 | f | TMD | pain in temporomandibular joint, neck pain | NA | 1 month | yes | No effect reported |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pfeiffer, K.; El Khassawna, T.; Malhan, D.; Langer, C.; Sommer, B.; Mekhemar, M.; Howaldt, H.-P.; Attia, S. Is Biofeedback through an Intra-Aural Device an Effective Method to Treat Bruxism? Case Series and Initial Experience. Int. J. Environ. Res. Public Health 2021, 18, 51. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010051
Pfeiffer K, El Khassawna T, Malhan D, Langer C, Sommer B, Mekhemar M, Howaldt H-P, Attia S. Is Biofeedback through an Intra-Aural Device an Effective Method to Treat Bruxism? Case Series and Initial Experience. International Journal of Environmental Research and Public Health. 2021; 18(1):51. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010051
Chicago/Turabian StylePfeiffer, Kira, Thaqif El Khassawna, Deeksha Malhan, Christine Langer, Barbara Sommer, Mohamed Mekhemar, Hans-Peter Howaldt, and Sameh Attia. 2021. "Is Biofeedback through an Intra-Aural Device an Effective Method to Treat Bruxism? Case Series and Initial Experience" International Journal of Environmental Research and Public Health 18, no. 1: 51. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010051