Effectiveness of Plyometric and Eccentric Exercise for Jumping and Stability in Female Soccer Players—A Single-Blind, Randomized Controlled Pilot Study



Abstract: Background
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
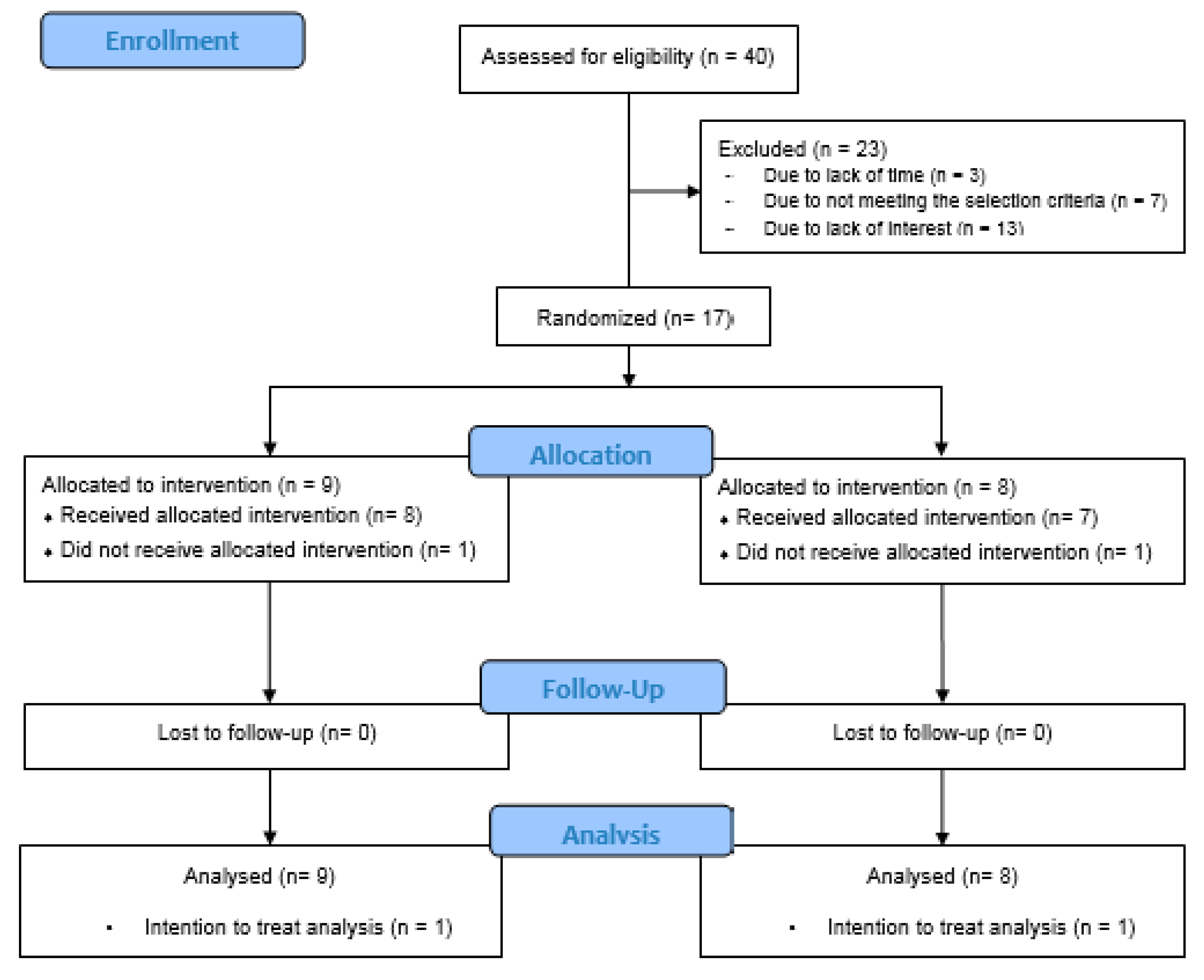
2.2. Participants
2.3. Instruments
- -
- Application “My jump 2.0”. With this mobile app, jumps were evaluated [20]. The rater stood at a distance of 1.5 m from the player, and a smartphone was placed at ground level to register the measurements. The test consisted of countermovement jump, starting from two-legged stance with hands on hips. Then, the athlete performed a jump from a 90º knee flexion position (avoiding bending the trunk). During the flight phase, the legs should be extended. When contacting the platform, the feet rested first on the metatarsal and subsequently on the back region. The unit of measurement for this instrument is centimeters.
- -
- Y-Balance test. This instrument was used to assess lower limb stability in accordance with the protocol developed by Plisky et al. [21]. The Y-Balance test is a validated derivation of the Star Excursion Balance Test (SEBT). This instrument uses the anterior, posteromedial, and posterolateral components of the SEBT to evaluate neuromuscular characteristics such as lower extremity coordination, balance, flexibility, and strength. The subject stood in monopodal stance in the center of an inverted Y-shape on the leg to be evaluated. Three attempts were made for each reaching direction (anterior, posteromedial, and posterolateral). The distance was measured in centimeters, and the arithmetic mean of three attempts made in each range was calculated [22]. The Y-shape was made with tape on the floor. Distance was measured with a tape measure.
2.4. Experimental Design
- -
- The Nordic hamstring exercise was performed using the protocol designed by Van der Horst et al. [23]. One subject in each pair kneeled, while the other subject, behind her, held her legs. The first one let herself drop forward in a controlled manner until touching the ground.
- -
- To perform “the diver” exercise, we followed the protocol described by Askling et al. [24]. The player stood in monopodal stance performing a hip flexion while maintaining support. She was asked to bring her arms forward, while moving the contralateral lower limb backwards. The knee should be supported at around 10–20 degrees flexion and the exercise, was performed slowly, returning to the starting position.
- -
- “The glider” exercise was conducted according to the protocol described by Askling et al. [24]. The athlete stood on both feet in front of her partner while holding each other’s shoulders and gliding one leg backwards while the other remained steady. She then returned to the starting position with the help of her partner, without letting the knee fall below 10 degrees flexion.
- -
- For the single-leg squat and lunge exercise, the athlete adopted a squatting position with her partner behind her, lifting and holding the back leg. The player then performed a monopodal jump with the supported leg. In the first week, a set with 5 repetitions and 30 s rest between sets was performed, increasing the intensity until reaching 3 sets with 8 repetitions in the last two weeks of the study.
- -
- To perform the 180 jump exercise, the player started from a bipedal stance position, with the trunk upright and hands on hips. She was asked to jump with both legs while turning 180 degrees in rotation during the jump, attempting to sustain the fall for 2 s. In each repetition, rotation was performed in a different direction. Two 20 s sets were performed, with 20 s rest between sets. Every two weeks, the intensity increased until reaching 3 sets of 30 s in the last two weeks.
- -
- For the broad jump stick landing exercise, the players stood in bipedal support, with their hands free, jumping with both feet as far as possible. The knees should not go beyond the tips of the toes and the fall should be with the trunk as straight as possible. Five jumps were performed in the first two weeks, increasing the number to 8 in the next two weeks, and eventually reaching 10 jumps in the last two weeks of the study.
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Study Limitations
4.2. Recommendations for Clinical Practice
4.3. Recommendations for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fuller, C.W.; Dick, R.W.; Corlette, J.; Schmalz, R. Comparison of the incidence, nature and cause of injuries sustained on grass and new generation artificial turf by male and female soccer players. Part 1: Match injuries. Br. J. Sports Med. 2007, 41, i20–i26. [Google Scholar] [CrossRef] [Green Version]
- Fuller, C.W.; Dick, R.W.; Corlette, J.; Schmalz, R. Comparison of the incidence, nature and cause of injuries sustained on grass and new generation artificial turf by male and female soccer players. Part 2: Training injuries. Br. J. Sports Med. 2007, 41, i27–i32. [Google Scholar] [CrossRef] [Green Version]
- Sentsomedi, K.R.; Puckree, T. Epidemiology of injuries in female high school soccer players. Afr. Health Sci. 2016, 16, 298–305. [Google Scholar] [CrossRef] [Green Version]
- Le Gall, F.; Carling, C.; Reilly, T. Injuries in young elite female soccer players: An 8-season prospective study. Am. J. Sports Med. 2008, 36, 276–284. [Google Scholar] [CrossRef]
- Gaulrapp, H.; Becker, A.; Walther, M.; Hess, H. Injuries in women’s soccer: A 1-year all players prospective field study of the women’s Bundesliga (German premier league). Clin. J. Sport Med. 2010, 20, 264–271. [Google Scholar] [PubMed]
- Söderman, K.; Alfredson, H.; Pietilä, T.; Werner, S. Risk factors for leg injuries in female soccer players: A prospective investigation during one out-door season. Knee Surg. Sports Traumatol. Arthrosc. 2001, 9, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Fitch, C. A new framework for research leading to sports injury prevention. J. Sci. Med. Sport 2006, 9, 3–9. [Google Scholar]
- Chalmers, D.J. Injury prevention in sport: Not yet part of the game? Inj. Prev. 2002, 8, IV22–IV25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hägglund, M.; Waldén, M.; Ekstrand, J. Injury incidence and distribution in elite soccer—A prospective study of the Danish and the Swedish top divisions. Scand. J. Med. Sci. Sports 2005, 15, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Hägglund, M.; Waldén, M.; Ekstrand, J. Injuries among male and female elite soccer players. Scand. J. Med. Sci. Sports 2009, 19, 819–827. [Google Scholar] [CrossRef]
- Verrall, G.M.; Slavotinek, J.P.; Barnes, P.G.; Spriggins, A. Clinical risk factors for hamstring muscle strain injury: A prospective study with correlation of injury by magnetic resonance imaging. Br. J. Sports Med. 2001, 35, 435–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henderson, G.; Barnes, C.A.; Portas, M.D. Factors associated with increased propensity for hamstring injury in English Premier League soccer players. J. Sci. Med. Sport 2010, 13, 397–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silder, A.; Reeder, S.B.; Thelen, D.G. The influence of prior hamstring injury on lengthening muscle tissue mechanics. J. Biomech. 2010, 43, 2254–2260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekstrand, J.; Hägglund, M.; Walden, M. Injury incidence and injury patterns in professional football: The UEFA injury study. Br. J. Sports Med. 2011, 45, 553–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, J.; Thorborg, K.; Nielsen, M.B.; Budtz-Jørgensen, E.; Hölmich, P. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer: A cluster-randomized controlled trial. Am. J. Sports Med. 2011, 39, 2296–2303. [Google Scholar] [CrossRef] [PubMed]
- Chimera, N.J.; Swanik, K.A.; Swanik, C.B.; Straub, S.J. Effects of Plyometric Training on Muscle-Activation Strategies and Performance in Female Athletes. J. Athl. Train. 2004, 39, 24–31. [Google Scholar]
- Mendiguchia, J.; Martinez-Ruiz, E.; Morin, J.B.; Samozino, P.; Edouard, P.; Alcaraz, P.E.; Mendez-Villanueva, A. Effects of hamstring-emphasized neuromuscular training on strength and sprinting mechanics in soccer players. Scand. J. Med. Sci. Sports 2015, 25, e621–e629. [Google Scholar] [CrossRef]
- Ramírez-Campillo, R.; Vergara-Pedreros, M.; Henríquez-Olguín, C.; Martínez-Salazar, C.; Álvarez, C.; Nakamura, F.Y. Effects of plyometric training on maximal-intensity exercise and endurance in male and female soccer players. J. Sports Sci. 2016, 34, 687–693. [Google Scholar] [CrossRef]
- Ebben, W.P.; Vanderzanden, T.; Wurm, B.J.; Petushek, E.J. Evaluating plyometric exercises using time to stabilization. J. Strength Cond. Res. 2010, 24, 300–306. [Google Scholar] [CrossRef]
- Balsalobre-Fernández, C.; Glaister, M.; Lockey, R.A. The validity and reliability of an iPhone app for measuring vertical jump performance. J. Sports Sci. 2015, 33, 1574–1579. [Google Scholar] [CrossRef]
- Plisky, P.J.; Gorman, P.P.; Butler, R.J.; Kiesel, K.B.; Underwood, F.B.; Elkins, B. The reliability of an instrumented device for measuring components of the star excursion balance test. N. Am. J. Sports Phys. Ther. 2009, 4, 92–99. [Google Scholar] [PubMed]
- Calvo-Gonell, A.; Pina-Romero, J.A.; Macía-Soler, L. Relationship between the y balance test scores and soft tissue injury incidence in a soccer team. Int. J. Sports Phys. Ther. 2015, 10, 955–966. [Google Scholar]
- Van der Horst, N.; Smits, D.W.; Petersen, J.; Goedhart, E.A.; Backx, F.J. The preventive effect of the nordic hamstring exercise on hamstring injuries in amateur soccer players: A randomized controlled trial. Am. J. Sports Med. 2015, 43, 1316–1323. [Google Scholar] [CrossRef] [PubMed]
- Askling, C.M.; Tengvar, M.; Thorstensson, A. Acute hamstring injuries in Swedish elite football: A prospective randomised controlled clinical trial comparing two rehabilitation protocols. Br. J. Sports Med. 2013, 47, 953–959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsang, K.K.; Di Pasquale, A.A. Improving the Q:H strength ratio in women using plyometric exercises. J. Strength Cond. Res. 2011, 25, 2740–2745. [Google Scholar] [CrossRef] [Green Version]
- Pallant, J. SPSS Survival Manual, 6th ed.; McGraw-HillEducation: New York, NY, USA, 2013. [Google Scholar]
- Bouteraa, I.; Negra, Y.; Shephard, R.J.; Chelly, M.S. Effects of combined balance and plyometric training on athletic performance in female basketball players. J. Strength Cond. Res. 2020, 34, 1967–1973. [Google Scholar] [CrossRef]
- Hammami, R.; Granacher, U.; Makhlouf, I.; Behm, D.G.; Chaouachi, A. Sequencing Effects of Balance and Plyometric Training on Physical Performance in Youth Soccer Athletes. J. Strength Cond. Res. 2016, 30, 3278–3289. [Google Scholar] [CrossRef]
- Benis, R.; Bonato, M.; La Torre, A. Elite Female Basketball Players’ Body-Weight Neuromuscular Training and Performance on the Y-Balance Test. J. Athl. Train. 2016, 51, 688–695. [Google Scholar] [CrossRef] [Green Version]
- Mjolsnes, R.; Arnason, A.; Osthagen, T.; Raastad, T.; Bahr, R. A 10-week randomized trial comparing eccentric vs. concentric hamstring strength training in well-trained soccer players. Scand. J. Med. Sci. Sports 2004, 14, 311–317. [Google Scholar] [CrossRef]
- Opar, D.A.; Williams, M.D.; Timmins, R.G.; Hickey, J.; Duhig, S.J.; Shield, A.J. Eccentric hamstring strength and hamstring injury risk in Australian footballers. Med. Sci. Sports Exerc. 2015, 47, 857–865. [Google Scholar] [CrossRef] [Green Version]
- Bourne, M.N.; Pope, D.; Duhig, S.J.; Timmins, R.G.; Williams, M.D.; Al Najjar, A.; Shield, A.J. Impact of the Nordic hamstring and hip extension exercises on hamstring architecture and morphology: Implications for injury prevention. Br. J. Sports Med. 2017, 51, 469–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seymore, K.D.; Domire, Z.J.; De Vita, P.; Rider, P.M.; Kulas, A.S. The effect of Nordic hamstring strength training on muscle architecture, stiffness, and strength. Eur. J. Appl. Physiol. 2017, 117, 943–953. [Google Scholar] [CrossRef] [PubMed]
- Ter Stege, M.H.; Dallinga, J.M.; Benjaminse, A.; Lemmink, K.A. Effect of interventions on potential, modifiable risk factors for knee injury in team ball sports: A systematic review. Sports Med. 2014, 44, 1403–1426. [Google Scholar] [CrossRef] [PubMed]
- Plisky, P.J.; Rauh, M.J.; Kaminski, T.W.; Underwood, F.B. Star Excursion Balance Test as a predictor of lower extremity injury in high school basketball players. J. Orthop. Sports Phys. Ther. 2006, 36, 911–919. [Google Scholar] [CrossRef]
- Lee, D.K.; Kim, G.M.; Ha, S.M.; Oh, J.S. Correlation of the Y-Balance Test with lower-limb strength of adult women. J. Phys. Ther. Sci. 2014, 26, 641–643. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variables | All Sample | Experimental Group | Control Group | p Value ª |
|---|---|---|---|---|
| Age (years) | 21.71 (3.54) | 21.11 (4.16) | 22.38 (2.82) | 0.06 |
| Height (cm.) | 162.71 (4.37) | 163 (4.63) | 162.38 (4.34) | 0.33 |
| Weight (kg) * | 63.87 (12.51) | 61.83 (9.17) | 66.16 (15.81) | 0.03 |
| Body mass index (kg/m2) * | 24.02 (4.70) | 23.07 (3.41) | 25.07 (5.90) | 0.03 |
| Federated years (years) | 7.24 (5.94) | 7.56 (7.56) | 6.87 (3.87) | 0.08 |
| Matches played in the season (number) | 10.82 (4.90) | 10.44 (5.36) | 11.25 (4.65) | 0.06 |
| n (%) | n (%) | n (%) | ||
| Menstrual cycle status (follicular phase/luteal phase) | 10/7 | 6/4 | 4/3 | 0.07 b |
| Jumping height (cm) | 47.08 (1.65) | 45.76 (5.18) | 48.72 (14.83) | 0.05 |
| Right anterior stability (cm) * | 57.88 (4.41) | 60.22 (3.66) | 55.25 (3.77) | 0.03 |
| Right posteromedial stability (cm) | 61.00 (9.10) | 64.22 (7.22) | 57.38 (10.07) | 0.72 |
| Right posterolateral stability (cm) | 63.65 (9.37) | 64.11 (10.77) | 63.13 (8.21) | 0.50 |
| Left anterior stability (cm) | 57.47 (4.75) | 59.67 (4.44) | 55.00 (4.00) | 0.95 |
| Left posteromedial stability (cm) | 57.53 (6.61) | 59.22 (6.20) | 55.63 (6.94) | 0.93 |
| Left posterolateral stability (cm) | 68.06 (8.47) | 70.44 (9.20) | 65.38 (7.19) | 0.35 |
| Variables | Experimental Group | Control Group | ||
|---|---|---|---|---|
| T1 | T2 | T1 | T2 | |
| Jumping height (cm) | 46.14 (6.05) | 45.55 (6.03) | 50.18 (13.65) | 49.43 (11.94) |
| Right anterior stability (cm) | 63.11 (4.28) | 63.11 (4.67) | 59.38 (7.46) | 61.25 (5.23) |
| Right posteromedial stability (cm) | 69.67 (6.32) | 67.56 (5.48) | 65.00 (3.92) | 63.88 (7.66) |
| Right posterolateral stability (cm) | 69.78 (11.91) | 68.56 (10.94) | 70.38 (5.39) | 71.13 (5.38) |
| Left anterior stability (cm) | 62.44 (3.39) | 62.78 (4.14) | 57.88 (4.19) | 58.38 (4.68) |
| Left posteromedial stability (cm) | 62.33 (4.97) | 64.56 (7.09) | 62.00 (7.54) | 64.25 (6.49) |
| Left posterolateral stability (cm) | 73.11 (8.47) | 71.11 (8.23) | 66.88 (5.16) | 69.88 (6.70) |
| Variables | Measure Instrument | Experimental Group | Control Group | ||||
|---|---|---|---|---|---|---|---|
| T0–T1 | T1–T2 | T0–T2 | T0–T1 | T1–T2 | T0–T2 | ||
| Jump | Jumping height | −0.44 (0.16) | −0.13 (0.61) | 0.30 (0.07) | −0.26 (0.10) | −0.27 (0.10) | −0.01 (0.96) |
| Lower limb stability | Right anterior | −2.88 (0.04) * | 0.00 (1.00) | −2.88 (0.13) | −4.12 (0.15) | −1.87 (0.13) | −6.0 (0.01) * |
| Right posteromedial | −5.44 (0.03) * | 2.11 (0.14) | −3.33 (0.12) | −7.62 (0.10) | 1.12 (0.69) | −6.5 (0.01) * | |
| Right posterolateral | −5.66 (0.11) | 1.22 (0.26) | −4.44 (0.09) | −7.25 (0.02) * | −0.75 (0.66) | −8.0 (0.04) * | |
| Left anterior | −2.77 (0.04) * | −0.33 (0.71) | −3.11 (0.04) * | −2.87 (0.07) | −0.50 (0.69) | −3.3 (0.02) * | |
| Left posteromedial | −3.11 (0.17) | −2.22 (0.05) | −5.33 (0.03) * | −6.37 (0.10) | −2.25 (0.17) | −8.62 (0.02) * | |
| Left posterolateral | −2.66 (0.26) | 2.00 (0.19) | −0.66 (0.65) | −1.5 (0.45) | −3.00 (0.07) | −4.5 (0.02) * | |
| Variable | Measure | Mauchly Sphericity | Intra-Group Effect | Inter-Group Interaction | |||||
|---|---|---|---|---|---|---|---|---|---|
| W | Sig. | F | Sig. | η2p | F | Sig. | η2p | ||
| Jump | Jumping height | 0.93 | 0.62 | 0.97 | 0.04 * | 0.16 | 0.53 | 0.59 | 0.03 |
| Lower limb stability | Right anterior a | 0.62 | 0.03 | 6.77 | 0.00 * | 0.31 | 0.93 | 0.38 | 0.05 |
| Right posteromedial a | 0.58 | 0.02 | 5.29 | 0.02 * | 0.26 | 0.43 | 0.58 | 0.02 | |
| Right posterolateral a | 0.49 | 0.00 | 5.96 | 0.01 * | 0.28 | 0.51 | 0.53 | 0.03 | |
| Left anterior | 0.94 | 0.65 | 4.44 | 0.02 * | 0.22 | 0.01 | 0.98 | 0.00 | |
| Left posteromedial a | 0.48 | 0.00 | 7.17 | 0.01 * | 0.32 | 0.68 | 0.45 | 0.04 | |
| Left posterolateral | 0.72 | 0.10 | 3.46 | 0.04 * | 0.18 | 2.38 | 0.10 | 0.13 | |
| Variable | Measure | T0–T1 | T1–T2 | T0–T2 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| I-J | 95% CI | Sig. | I-J | 95% CI | Sig. | I-J | 95% CI | Sig. | ||
| Jump | Jumping height | −0.35 | −0.80, 0.19 | 0.14 | 0.15 | −0.20, 0.51 | 0.76 | −0.20 | −0.62, 0.41 | 0.06 |
| Lower limb stability | Right anterior | −3.47 | −7.12, 0.18 | 0.06 | −0.88 | −2.82, 1.06 | 0.72 | −4.35 | −7.72, −0.98 | 0.01 * |
| Right posteromedial | −6.47 | −12.46, −0.47 | 0.03 * | 1.64 | −2.35, 5.64 | 0.85 | −4.82 | −8.51, −1.12 | 0.00 * | |
| Right posterolateral | −6.41 | −12.05, −0.76 | 0.02 * | 0.29 | −2.25, 2.84 | 1.00 | −6.11 | −11.46, −0.76 | 0.02 * | |
| Left anterior | −2.82 | −5.18, −0.45 | 0.01 * | −0.41 | −2.37, 1.55 | 1.00 | −3.23 | −5.64, −0.82 | 0.00 * | |
| Left posteromedial | −4.64 | −9.38, 0.54 | 0.08 | −2.23 | −4.56. 0.09 | 0.06 | −6.88 | −11.85, −1.90 | 0.00 * | |
| Left posterolateral | −2.11 | −6.09, 1.86 | 0.51 | −0.35 | −3.06, 2.35 | 1.00 | −2.47 | −5.28, 0.34 | 0.09 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porrati-Paladino, G.; Cuesta-Barriuso, R. Effectiveness of Plyometric and Eccentric Exercise for Jumping and Stability in Female Soccer Players—A Single-Blind, Randomized Controlled Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 294. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010294
Porrati-Paladino G, Cuesta-Barriuso R. Effectiveness of Plyometric and Eccentric Exercise for Jumping and Stability in Female Soccer Players—A Single-Blind, Randomized Controlled Pilot Study. International Journal of Environmental Research and Public Health. 2021; 18(1):294. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010294
Chicago/Turabian StylePorrati-Paladino, Guillermo, and Rubén Cuesta-Barriuso. 2021. "Effectiveness of Plyometric and Eccentric Exercise for Jumping and Stability in Female Soccer Players—A Single-Blind, Randomized Controlled Pilot Study" International Journal of Environmental Research and Public Health 18, no. 1: 294. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010294