Is Visual Pedagogy Effective in Improving Cooperation towards Oral Hygiene and Dental Care in Children with Autism Spectrum Disorder? A Systematic Review and Meta-Analysis

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
- Population: Children with autism spectrum disorders;
- Intervention: Effect of visual pedagogy;
- Comparison: Visual pedagogy vs. no treatment or outcomes measured before and after visual pedagogy administration;
- Outcome: Oral hygiene skills (primary outcome) and/or cooperation during dental care (secondary outcome).
2.1. Eligibility Criteria
- Type of study: prospective clinical studies, randomized trials, interruptive case series, before and after comparison studies, cross-sectional studies;
- Publication languages: papers published in English, Italian, and French;
- Time of publication: no time restriction applied, last accessed on 23 July 2020;
- Type of tool used: PECS, images on paper, such as dental books, picture cards, drawings, and printed photos, or on digital supports, such as tablets, dental apps, and/or videos;
- Primary outcome: clinical indices of oral hygiene skills, such as the plaque index (PI) and the gingival index (GI). Tooth brushing performance was also considered.
- Secondary outcome: indices of patient’s cooperation level during dental procedures, such as the Frankl Behavior Score and the Likert Anxiety Scale, and/or the number of steps/procedures completed and time spent, measured by a dentist or a dental hygienist and/or a psychologist/educator.
2.2. Information Sources and Search Strategy
2.3. Study Selection
2.4. Data Collection, Summary Measures, and Synthesis of Results
2.5. Quality Assessment and Scientific Evidence
2.6. Statistical Analysis
3. Results
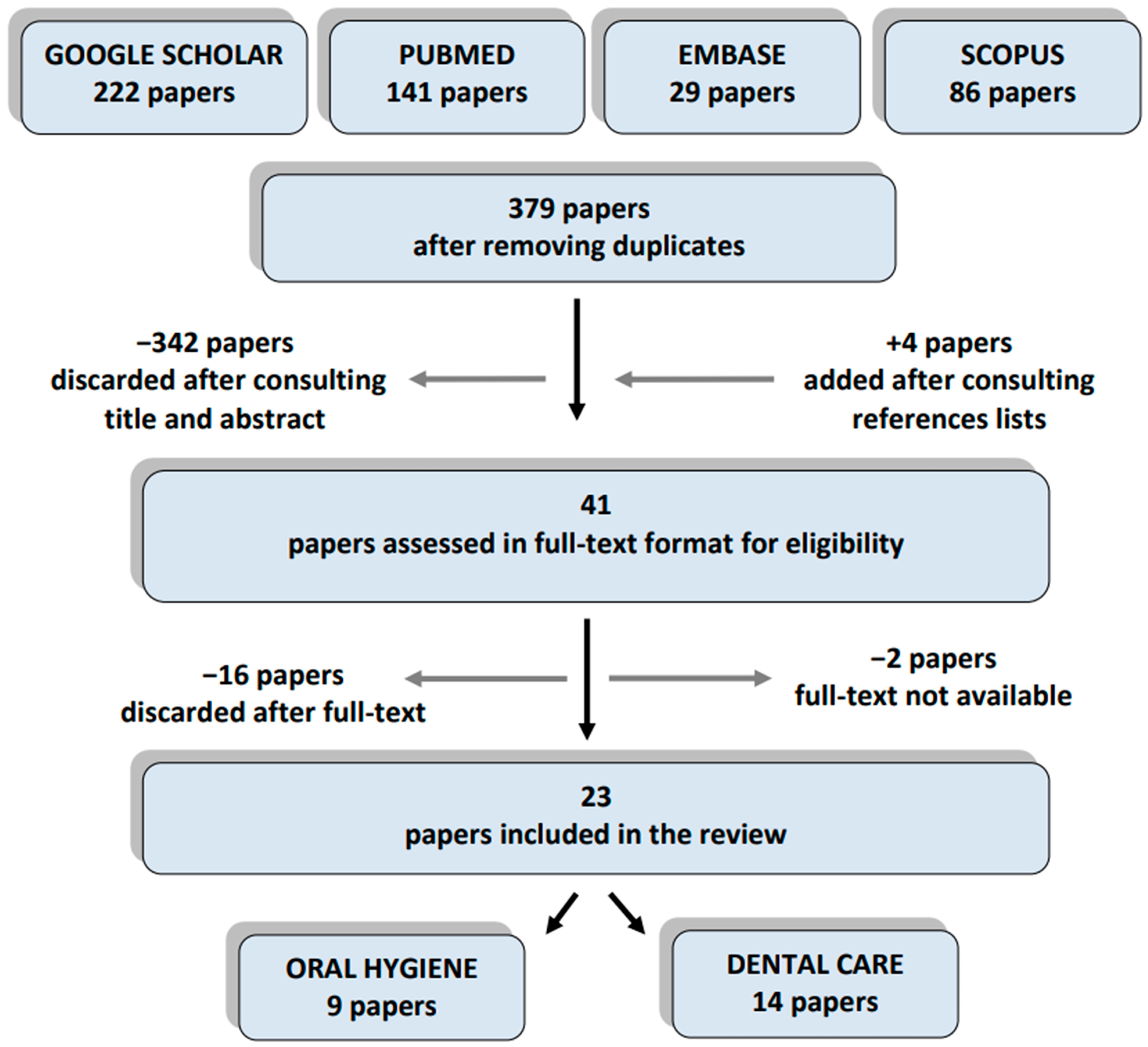
3.1. Study Selection
3.2. Study Characteristics
3.3. Subjects Involved
3.4. Visual Pedagogy Tools and Protocol
3.5. Oral Hygiene Outcome
3.6. Dental Care Outcomes
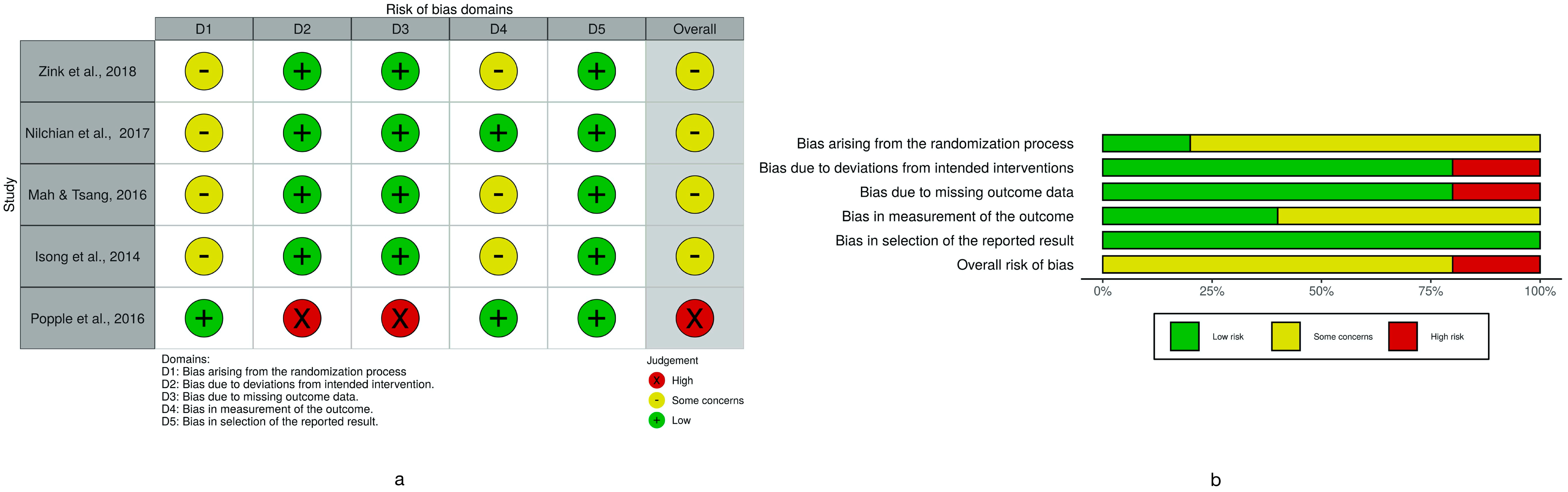
3.7. Risk of Bias Assessment
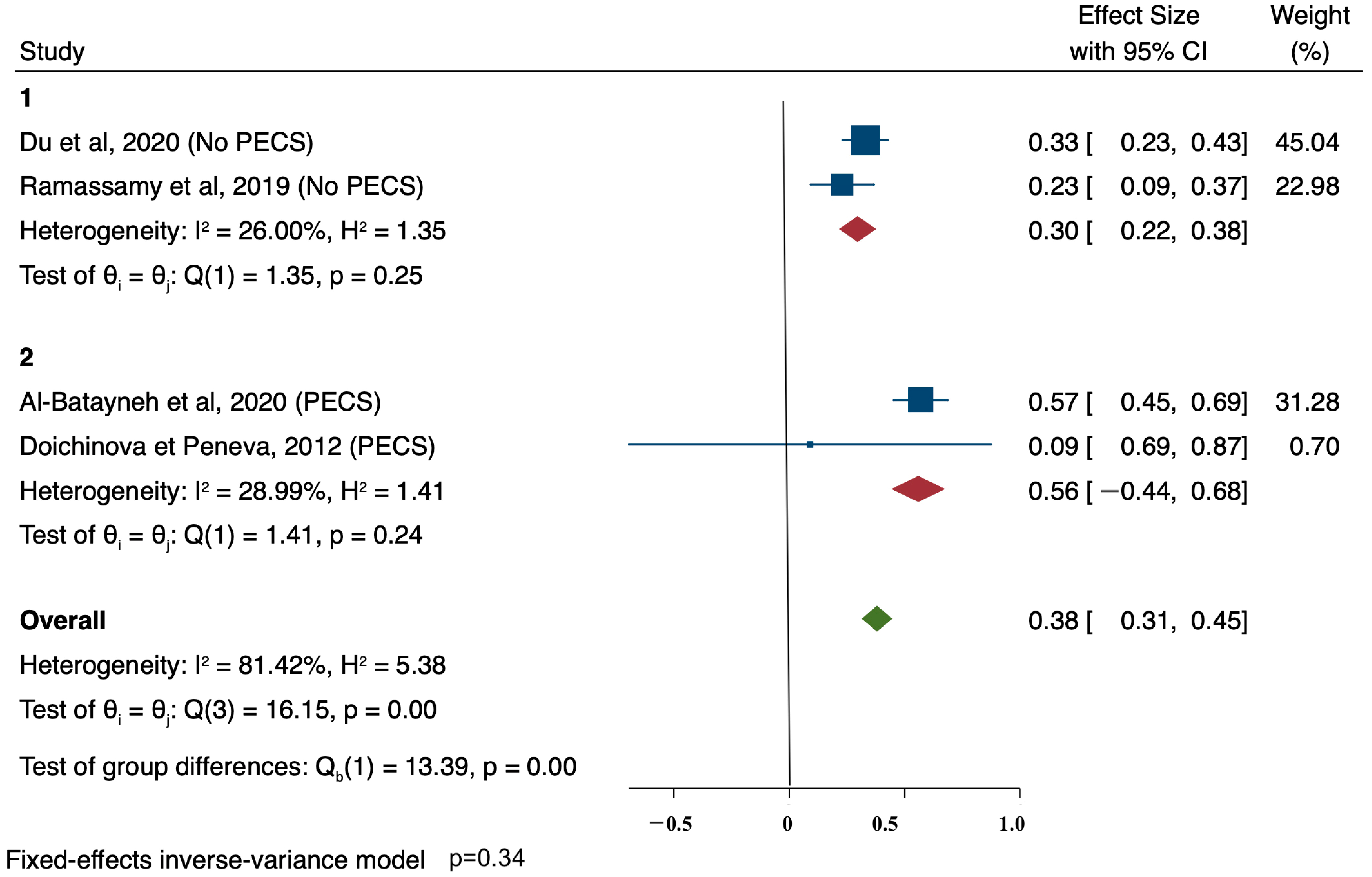
3.8. Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lai, M.-C.; Lombardo, M.V.; Baron-Cohen, S. Autism. Lancet 2014, 383, 896–910. [Google Scholar] [CrossRef]
- Lai, M.-C.; Kassee, C.; Besney, R.; Bonato, S.; Hull, L.; Mandy, W.; Szatmari, P.; Ameis, S.H. Prevalence of co-occurring mental health diagnoses in the autism population: A systematic review and meta-analysis. Lancet Psychiatry 2019, 6, 819–829. [Google Scholar] [CrossRef]
- Lyall, K.; Croen, L.; Daniels, J.; Fallin, M.D.; Ladd-Acosta, C.; Lee, B.K.; Park, B.Y.; Snyder, N.W.; Schendel, D.; Volk, H.; et al. The changing epidemiology of autism spectrum disorders. Annu. Rev. Public Health 2017, 38, 81–102. [Google Scholar] [CrossRef] [Green Version]
- Cagetti, M.G.; Mastroberardino, S.; Campus, S.; Olivari, B.; Faggioli, R.; Lenti, C.; Strohmenger, L. Dental care protocol based on visual supports for children with autism spectrum disorders. Med. Oral Patol. Oral Cir. Bucal 2015, 20, e598–e604. [Google Scholar] [CrossRef]
- Fakhruddin, K.S.; El Batawi, H.Y. Effectiveness of audiovisual distraction in behavior modification during dental caries assessment and sealant placement in children with autism spectrum disorder. Dent. Res. J. 2017, 14, 177–182. [Google Scholar] [CrossRef]
- Ferrazzano, G.F.; Salerno, C.; Bravaccio, C.; Ingenito, A.; Sangianantoni, G.; Cantile, T. Autism spectrum disorders and oral health status: Review of the literature. Eur. J. Paediatr. Dent. 2020, 21, 9–12. [Google Scholar] [CrossRef]
- da Silva, S.N.; Gimenez, T.; Souza, R.C.; Mello-Moura, A.C.V.; Raggio, D.P.; Morimoto, S.; Lara, J.S.; Soares, G.C.; Tedesco, T.K. Oral health status of children and young adults with autism spectrum disorders: Systematic review and meta-analysis. Int. J. Paediatr. Dent. 2017, 27, 388–398. [Google Scholar] [CrossRef]
- Yost, Q.; Nelson, T.; Sheller, B.; McKinney, C.M.; Tressel, W.; Chim, A.N. Children with autism spectrum disorder are able to maintain dental skills: A two-year case review of desensitization treatment. Pediatr. Dent. 2019, 41, 397–403. [Google Scholar]
- Limeres-Posse, J.; Castaño-Novoa, P.; Abeleira-Pazos, M.; Ramos-Barbosa, I. Behavioural aspects of patients with Autism Spectrum Disorders (ASD) that affect their dental management. Med. Oral Patol. Oral Cir. Bucal 2014, 19, e467–e472. [Google Scholar] [CrossRef]
- Hodgetts, S.; Park, E. Preparing for the future: A review of tools and strategies to support autonomous goal setting for children and youth with autism spectrum disorders. Disabil. Rehabil. 2017, 39, 535–543. [Google Scholar] [CrossRef]
- LaBelle, C. Using Visual Pedagogy to tell our stories. J. Appl. Commun. 2012, 96, 6–14. [Google Scholar] [CrossRef] [Green Version]
- Bondy, A.; Frost, L. The Picture Exchange Communication System. Behav. Modif. 2001, 25, 725–744. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Al-Batayneh, O.B.; Nazer, T.S.; Khader, Y.S.; Owais, A.I. Effectiveness of a tooth-brushing programme using the picture exchange communication system (PECS) on gingival health of children with autism spectrum disorders. Eur. Arch. Paediatr. Dent. 2020, 21, 277–283. [Google Scholar] [CrossRef]
- Doichinova, L.; Peneva, M. PECS picture system for non verbal communication role in oral hygiene education of children with autism. Probl. Dent. Med. 2012, 1, 10–16. [Google Scholar]
- Doichinova, L.; Gateva, N.; Hristov, K. Oral hygiene education of special needs children. Part 1: Children with autism spectrum disorder. Biotechnol. Biotechnol. Equip. 2019, 33, 748–755. [Google Scholar] [CrossRef] [Green Version]
- Du, R.Y.; Lam, P.P.Y.; Yiu, C.K.Y.; McGrath, C.P. Evaluation of visual pedagogy in improving plaque control and gingival inflammation among preschool children with autism spectrum disorder: An interventional study. Int. J. Paediatr. Dent. 2020. [Google Scholar] [CrossRef]
- Pilebro, C.; Bäckman, B. Teaching oral hygiene to children with autism. Int. J. Paediatr. Dent. 2005, 15, 1–9. [Google Scholar] [CrossRef]
- Lopez Cazaux, S.; Lefer, G.; Rouches, A.; Bourdon, P. Toothbrushing training programme using an iPad® for children and adolescents with autism. Eur. Arch. Paediatr. Dent. 2019, 20, 277–284. [Google Scholar] [CrossRef]
- Popple, B.; Wall, C.; Flink, L.; Powell, K.; Discepolo, K.; Keck, D.; Mademtzi, M.; Volkmar, F.; Shic, F. Brief report: Remotely delivered video modeling for improving oral hygiene in children with ASD: A pilot study. J. Autism Dev. Disord. 2016, 46, 2791–2796. [Google Scholar] [CrossRef] [Green Version]
- Zhou, N.; Wong, H.M.; McGrath, C. Efficacy of social story intervention in training toothbrushing skills among special-care children with and without autism. Autism Res. 2020, 13, 666–674. [Google Scholar] [CrossRef]
- Ramassamy, E.; Gajula Shivashankarappa, P.; Adimoulame, S.; Meena, R.; Elangovan, H.; Govindasamy, E. Yoga therapy as an adjunct to traditional tooth brushing training methods in children with autism spectrum disorder. Spec. Care Dent. 2019, 39, 551–556. [Google Scholar] [CrossRef]
- Zink, A.G.; Molina, E.C.; Diniz, M.B.; Santos, M.T.B.R.; Guaré, R.O. Communication application for use during the first dental visit for children and adolescents with autism spectrum disorders. Pediatr. Dent. 2018, 40, 18–22. [Google Scholar]
- Bäckman, B.; Pilebro, C. Visual pedagogy in dentistry for children with autism. ASDC J. Dent. Child. 1999, 66, 294, 325–331. [Google Scholar]
- Bossù, M.; Corridore, D.; D’Errico, A.; Ladniak, B.; Ottolenghi, L.; Polimeni, A. Education and dentistry: Advanced synergy in the dental treatment of children with autism; a pilot clinical trial. Senses Sci. 2014, 1. [Google Scholar] [CrossRef]
- Hidayatullah, T.; Agustiani, H.; Setiawan, A.S. Behavior management-based applied behaviour analysis within dental examination of children with autism spectrum disorder. Dent. J. 2018, 51, 71–75. [Google Scholar] [CrossRef] [Green Version]
- Isong, I.A.; Rao, S.R.; Holifield, C.; Iannuzzi, D.; Hanson, E.; Ware, J.; Nelson, L.P. Addressing dental fear in children with autism spectrum disorders: A randomized controlled pilot study using electronic screen media. Clin. Pediatr. 2014, 53, 230–237. [Google Scholar] [CrossRef]
- Lefer, G.; Rouches, A.; Bourdon, P.; Lopez Cazaux, S. Training children with autism spectrum disorder to undergo oral assessment using a digital iPad® application. Eur. Arch. Paediatr. Dent. 2019, 20, 113–121. [Google Scholar] [CrossRef]
- Mah, J.W.; Tsang, P. Visual schedule system in dental care for patients with autism: A pilot study. J. Clin. Pediatr. Dent. 2016, 40, 393–399. [Google Scholar] [CrossRef]
- Murshid, E.Z. Effectiveness of a preparatory aid in facilitating oral assessment in a group of Saudi children with autism spectrum disorders in Central Saudi Arabia. Saudi Med. J. 2017, 38, 533–540. [Google Scholar] [CrossRef]
- Nilchian, F.; Shakibaei, F.; Jarah, Z.T. Evaluation of visual pedagogy in dental check-ups and preventive practices among 6-12-year-old children with autism. J. Autism Dev. Disord. 2017, 47, 858–864. [Google Scholar] [CrossRef]
- Orellana, L.-M.; Cantero-Fuentealba, C.; Schmidlin-Espinoza, L.; Luengo, L. Psychoeducational intervention to improve oral assessment in people with autism spectrum disorder, BIO-BIO region, Chile. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e37–e46. [Google Scholar] [CrossRef]
- Orellana, L.M.; Martínez-Sanchis, S.; Silvestre, F.J. Training adults and children with an autism spectrum disorder to be compliant with a clinical dental assessment using a TEACCH-based approach. J. Autism Dev. Disord. 2014, 44, 776–785. [Google Scholar] [CrossRef] [Green Version]
- Schindel, R.H.; Chahine, A.; Anderson, N.; Banville, N.; Eaton-Bove, J.; Weidenbaum, N. Behavior modification of children with autism spectrum disorder in an orthodontic setting. J. Clin. Orthod. 2014, 44, 285–291. [Google Scholar]
- Zink, A.G.; Diniz, M.B.; Rodrigues Dos Santos, M.T.B.; Guaré, R.O. Use of a Picture Exchange Communication System for preventive procedures in individuals with autism spectrum disorder: Pilot study. Spec. Care Dent. 2016, 36, 254–259. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2020. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Weil, T.N.; Inglehart, M.R. Dental education and dentists’ attitudes and behavior concerning patients with autism. J. Dent. Educ. 2010, 74, 1294–1307. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Authors | Sources | Location | Database | Type of Study | Aim | Risk Of Bias Assessment |
|---|---|---|---|---|---|---|
| Du et al. [17] | Int. J. Paediatr. Dent. 2021, 31, 89–105 | Hong Kong (China) | PM, E | ITSS | Oral Hygiene | Moderate |
| Al-Batayneh et al. [14] | Eur. Arch. Paediatr. Dent. 2020, 21, 277–283 | Irbid (Jordan) | PM, E, S | ITSS | Oral Hygiene | Moderate |
| Zhou et al. [21] | Autism. Res. 2020, 13, 666–674 | Hong Kong (China) | PM, E, GS | CBA | Oral Hygiene | Moderate |
| Doichinova et al. [16] | Biotechnol. Biotechnol. Equip. 2019,33, 748–755 | Sofia (Bulgaria) | GS | BA | Oral Hygiene | Moderate |
| Orellana et al. [32] | Med. Oral Patol. Oral Cir. Bucal. 2019, 24, 37–46 | BIO-BIO region (Chile) | PM, GS, S | ITSS | Dental Care | Moderate |
| Lopez-Cazaux et al. [19] | Eur. Arch. Paediatr. Dent. 2019, 20, 277–284 | Nantes (France) | PM, GS, S | ITSS | Oral Hygiene | Moderate |
| Lefer et al. [28] | Eur. Arch. Paediatr. Dent. 2019, 20, 113–121 | Nantes (France) | PM, S | ITSS | Dental Care | Moderate |
| Ramassany et al. [22] | Spec. Care Dentist. 2019, 39, 551–556 | Puducherry (India) | PM, E, GS, S | ITSS | Oral Hygiene | Low |
| Hidayatullah et al. [26] | Dent. J. 2018, 51, 71–75 | Bandung (Indonesia) | GS | ITSS | Dental Care | Moderate |
| Zink et al. [23] | Pediatr. Dent. 2018, 40, 18–22 | Sao Paolo (Brazil) | PM, E, GS, S | RCT | Dental Care | Moderate |
| Murshid. [30] | Saudi. Med. J. 2017, 38, 533–540 | Riyadh (Saudi Arabia) | PM | BA | Dental Care | Moderate |
| Nilchian et al. [31] | J. Autism. Dev. Disord. 2017, 47, 858–864 | Isfahan (Iran) | PM, E, GS | RCT | Dental Care | Moderate |
| Popple et al. [20] | J. Autism. Dev. Disord. 2016, 46, 2791–2796 | New Haven (USA) | PM, GS | RCT | Oral Hygiene | Moderate |
| Zink et al. [35] | Spec. Care Dentist. 2016, 36, 254–259 | Sao Paolo (Brazil) | PM, S | BA | Dental Care | Moderate |
| Mah & Tsang [29] | J. Clin. Pediatr. Dent. 2016, 40, 393–399 | Vancouver (Canada) | PM, E, GS, S | RCT | Dental Care | Moderate |
| Cagetti et al. [4] | Med. Oral Patol. Oral Cir. Bucal. 2015, 20, 598–604 | Milan (Italy) | PM, GS, S | ITSS | Dental Care | Moderate |
| Isong etal. [27] | Clin. Pediatr. 2014, 53, 230–237 | Boston (USA) | PM, GS | RCT | Dental Care | Moderate |
| Schindel etal. [34] | J. Clin. Orthod. 2014, 48, 285–291 | Commack (USA) | PM, E | BA | Dental Care | Serious |
| Bossù et al. [25] | Senses Sci. 2014, 1, 107–112 | Rome (Italy) | GS | ITSS | Dental Care | Moderate |
| Orellana et al. [33] | J. Autism. Dev. Disord. 2014, 44, 776–785 | Valencia (Spain) | PM, GS | BA | Dental Care | Moderate |
| Doichinova & Peneva [15] | Prob. Dent. Med. 2012, 38, 12–18 | Sofia (Bulgaria) | GS | ITSS | Oral Hygiene | Moderate |
| Pilebro & Bäckman [13] | Int. J. Paediatr. Dent. 2005, 15, 1–9 | Umea (Sweden) | PM, E, GS, S | ITSS | Oral Hygiene | Moderate |
| Bäckman & Pilebro [24] | J. Dent. Child. 1999, 66, 325–331 | Umea (Sweden) | PM, S | CBA | Dental Care | Moderate |
| Author (Year) | N-Subjects M/F Age-Range | Intellectual Disability/Verbal Fluency | Study Length | Type of Tool | Visual Pedagogy Protocol | Adjunctive Tool | Study Design/Groups (Outcome) | Results Mean (SD) | Findings | |
|---|---|---|---|---|---|---|---|---|---|---|
| PECS | ||||||||||
| Al-Batayneh et al. (2020) [14] | 37 | Fluent, non-fluent and non-verbal | Six mo | PECS (paper) | Provided daily by parents/caregivers | - | Two groups: | G1 | G2 | PI and GI showed a statistically significant improvement at three-month and six-month evaluations in both groups (p < 0.01). No comparison between groups was performed |
| M/F | G1: 4–10 yy (n = 24) | Plaque Index (PI) | ||||||||
| 4–16 yy | G2: 10–16 yy (n = 13) | Baseline 1.88 (0.36) | Baseline 2.17 (0.26) | |||||||
| Three mo 1.47 (0.30) | Three mo 1.47 (0.26) | |||||||||
| GI and PI | Six mo 1.27 (0.34) | Six mo 1.38 (0.24) | ||||||||
| Gingival Index (GI) | ||||||||||
| Baseline 1.12 (0.22) | Baseline 1.26 (0.23) | |||||||||
| Three mo 0.89 (0.19) | Three mo 0.97 (0.28) | |||||||||
| Six mo 0.85 (0.17) | Six mo 0.95 (0.27) | |||||||||
| Doichinova et al. (2019) [16] | 30 | Non-verbal and non-fluent | 12 mo | PECS (paper) | Provided daily by parents/caregivers | Behavioral management; TSD | One group (n = 30) | Plaque Index (PI) | PI showed a statistically significant improvement at three-, six-, and 12-month evaluations (p < 0.05) | |
| - | Baseline 2.29 | |||||||||
| 6–11 yy | PI | Three mo 1.95 (0.36) | ||||||||
| Six mo 1.88 (0.35) | ||||||||||
| 12 mo 1.79 (0.36) | ||||||||||
| Doichinova & Peneva, (2012) [15] | 30 | Moderately severe | 12 mo | PECS (paper) | Provided daily by parents and for 15 min every two weeks by dental specialist | Behavioral management; TSD | One group (n = 30) | Plaque Index (PI) | PI improved but did not reach a statistical significance (p > 0.05) | |
| M/F | Baseline 2.49 (0.55) | |||||||||
| 4–11 yy | PI | Three mo 2.40 (0.15) | ||||||||
| Six mo 2.42 (0.21) | ||||||||||
| 12 mo 2.34 (0.21) | ||||||||||
| Different Kind of Images | ||||||||||
| Du, (2020) [17] | 122 | From mild to severe | Six mo | Photos (paper) | Provided daily by parents/caregiver | - | One group (n = 122) | Plaque Index (PI) | PI and GI showed a statistically significant improvement at three- and six-month evaluations (p < 0.01) | |
| M/F | Baseline 1.00 (0.32) | |||||||||
| 2.5–7 yy | GI and PI | Three mo 0.67 (0.27) | ||||||||
| Six mo 0.63 (0.25) | ||||||||||
| Gingival Index (GI) | ||||||||||
| Baseline 0.91 (0.26) | ||||||||||
| Three mo 0.58 (0.26) | ||||||||||
| Six mo 0.60 (0.26) | ||||||||||
| Zhou, (2020) [21] | 169 | From mild to severe | Six mo | Social Story (paper) | Provided daily by parents/caregivers | - | Two groups: | G1 | G2 | Tooth brushing performance, DI-S, and MGI showed a statistically significant improvement at the six-month evaluation in both groups (p < 0.01). Children with ASDs showed better oral hygiene status (p = 0.01) and gingival status (p < 0.01) than their peers with other disabilities. No significant difference in the tooth brushing performance between groups was found. |
| - | G1: ASD (n = 84) | Plaque Index (DI-S) | ||||||||
| <6 yy | G2: other disability (n = 85) | Baseline 1.63 (0.82) | Baseline 1.64 (0.77) | |||||||
| Six mo 0.68 (0.42) | Six mo 0.85 (0.44) | |||||||||
| Gingival Index (MGI) | ||||||||||
| Tooth brushing performance, DI-S, and MG | Baseline 1.02 (0.64) | Baseline 1.17 (0.56) | ||||||||
| Six mo 0.43 (0.42) | Six mo 0.69 (0.50) | |||||||||
| Tooth brushing performance, DI-S, and MGI | Tooth brushing performance (steps achieved) | |||||||||
| Baseline 6.69 (3.23) | Baseline 6.62 (2.69) | |||||||||
| Six mo 8.30 (3.36) | Six mo 8.07 (3.41) | |||||||||
| Lopez Cazaux et al. (2019) [19] | 52 | - | Eight mo | Pictograms and photos (digital) | Provided daily by parents/caregivers and weekly by dentist | - | One group (n = 52) | Tooth brushing performance * | Tooth brushing performance showed a statistically significant improvement at the eight-month evaluation at each step (p < 0.01) | |
| M/F | Put toothpaste on the brush | |||||||||
| 3–19 yy | Tooth brushing performance | Baseline 4.2 (0.8) | ||||||||
| Four mo 4.5 (0.7) | ||||||||||
| Eight mo 4.8 (0.5) | ||||||||||
| Brush occlusal surface | ||||||||||
| Baseline 3.1 (1.0) | ||||||||||
| Four mo 3.9 (1.0) | ||||||||||
| Eight mo 4.2 (0.7) | ||||||||||
| Brush buccal surface | ||||||||||
| Baseline 2.6 (1.2) | ||||||||||
| Four mo 3.5 (0.9) | ||||||||||
| Eight mo 3.8 (0.9) | ||||||||||
| Brush lingual surface | ||||||||||
| Baseline 2.1 (1.0) | ||||||||||
| Four mo 3.4 (1.0) | ||||||||||
| Eight mo 3.8 (0.9) | ||||||||||
| Spit and store the brush | ||||||||||
| Baseline 3.9 (0.9) | ||||||||||
| Four mo 4.2 (0.8) | ||||||||||
| Eight mo 4.3 (0.8) | ||||||||||
| Pilebro & Bäckman, (2005) [18] | 14 | Fluent and non-fluent | 18 mo | Photo (paper) | Provided daily by parents | - | One group (n = 14) | Plaque Index (PI) | PI showed improvement at eight- and 12-month evaluations (no statistical analysis available) | |
| M | Baseline 2.57 | |||||||||
| 5–13 yy | PI | Eight mo 1.64 | ||||||||
| 12 mo 1.92 | ||||||||||
| Videos or Videos Plus Images | ||||||||||
| Ramassamy et al. (2019) [22] | 67 | Moderate | Six mo | Pictures (paper) and video | Provided daily by parents or teacher | - | Two groups: | G1 | G2 | Children in G2 demonstrated better oral hygiene. PI and GI were statistically significantly different at two months (p = 0.04 and p = 0.01), three months (p = 0.01 and p = 0.01), and six months (p = 0.01 for both) between groups. |
| M/F | G1: visual pedagogy (n = 32) | Plaque Index (PI) | ||||||||
| 7–15 yy | G2: visual pedagogy + yoga therapy (n = 35) | Baseline 1.78 (0.14) | Baseline 1.75 (0.25) | |||||||
| Three mo 1.55 (0.21) | Three mo 1.22 (0.39) | |||||||||
| Six mo 1.35 (0.35) | Six mo 0.96 (0.34) | |||||||||
| PI and GI | Gingival Index (GI) | |||||||||
| Baseline 1.76 (0.14) | Baseline 1.72 (0.22) | |||||||||
| Three mo 1.59 (0.17) | Three mo 1.36 (0.36) | |||||||||
| Six mo 1.49 (0.18) | Six mo 1.09 (0.27) | |||||||||
| Popple et al. (2016) [20] | 18 | Moderate | Six wk | Video | Provided daily by parents | - | Two groups: | G1 | G2 | PI-PH showed a statistically significant improvement at three-week and six-week evaluations in both groups (p < 0.01); statistically significant differences between G1 and G2 at the six-week evaluation were found (d = 1.02) |
| M/F | G1: intervention video (n = 9) | Plaque Index (PI-PH) | ||||||||
| 5–14 yy | G2: control video (n = 9) | Baseline 1.78 (0.62) | Baseline 1.75 (0.83) | |||||||
| Three wk 0.92 (0.65) | Three wk 1.45 (0.91) | |||||||||
| PI-PH | Six wk 0.38 (0.43) | Six wk 1.20 (1.05) | ||||||||
| Author (Year) | N-Sunjects M/F Age-Range | Intellectual Disability/Verbal Fluency | Study Length | Type of Tool | Visual Pedagogy Protocol | Adjunctive Tool | Study Design/Groups (Outcome) | Dental Visit Results Mean (SD) or Counts | Findings | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PECS | |||||||||||||
| Zink et al. (2018) [23] | 40 | - | - | Images (digital) or PECS (paper) | Provided once by dentist | BM | Two Groups: | G1 | G2 | The mean number of attempts for acquiring each step (p < 0.01) and number of visits to fully cooperate (p < 0.01) were significantly lower in G1 compared to G2 | |||
| M/F | G1: app on iPad® (n = 20) | Mean number of attempts (n) * | |||||||||||
| 9–15 yy | G2: PECS (n = 20) | Step One | 1.1 (0.3) | 1.5 (0.8) | |||||||||
| Step Two | 1.1 (0.5) | 1.6 (0.6) | |||||||||||
| Professional teeth-cleaning, divided in seven steps, reported as the number of attempts for acquiring each step and number of visits to fully cooperate | Step Three | 1.5 (0.5) | 1.6 (0.7) | ||||||||||
| Step Four | 1.0 (0.2) | 1.7 (1.1) | |||||||||||
| Step Five | 1.2 (0.4) | 1.6 (0.9) | |||||||||||
| Step Six | 1.2 (0.6) | 1.8 (0.9) | |||||||||||
| Step Seven | 2.1 (0.9) | 2.6 (1.7) | |||||||||||
| Number of visits (n) * | |||||||||||||
| 3.0 (1.0) | 4.3 (1.2) | ||||||||||||
| Hidayatullah et al. (2018) [26] | 13 | From mild to moderate | One mo | PECS (paper) | Provided weekly by teacher and by dentist | BM | One group (n = 13) | Mean number of steps completed (n) † | Patients were able to perform more steps within a dental visit at one-, two-, three-, and four-week evaluations (p < 0.01) | ||||
| M/F | One wk | 1.9 (1.3) | |||||||||||
| 5–18 yy | Dental visit divided into 10 steps | Two wk | 3.5 (0.9) | ||||||||||
| Three wk | 4.5 (1.7) | ||||||||||||
| Four wk | 5.6 (1.9) | ||||||||||||
| Zink et al. (2016) [35] | 26 | - | - | PECS (paper) | Provided once by the dentist | BM | Two groups | G1 | G2 | The mean number of attempts required for steps two, four, five, and six were significantly lower (p < 0.05) in G1 compared to G2 | |||
| M/F | G1: no dental experience (n = 13) | Mean number of attempts (n) * | |||||||||||
| 5–19 yy | |||||||||||||
| M/F | G2: previous dental experience (n = 13) | Step One | 1.8 (1.0) | 1 2.8 (1.6) | |||||||||
| Step Two | 1.5 (1.5) | 2.5 (1.9) | |||||||||||
| Step Three | 2.8 (1.6) | 4.4 (2.5) | |||||||||||
| Dental visit divided into six steps, and professional teeth-cleaning (including fluoride therapy), considered as step seven, reported as the number of attempts for acquiring each step | Step Four | 2.0 (1.9) | 3.4 (2.1) | ||||||||||
| Step Five | 2.1 (1.7) | 4.6 (2.1) | |||||||||||
| Step Six | 2.5 (2.1) | 4.4 (1.7) | |||||||||||
| Step Seven | 3.8 (3.3) | 4.6 (2.4) | |||||||||||
| Mah and Tsang, (2016) [29] | 14 | Mild | Three wk | PECS (paper) | Provided weekly by dentist/hygienist | TSD | Two groups | G1 | G2 | The mean number of steps completed increased, completion time decreased, and anxiety decreased more in G1 compared to G2 at one-, two-, and three- week evaluations (no statistical analysis available) | |||
| M | G1: test group (n = 7) | Mean number of steps completed (n) | |||||||||||
| 4–8 yy | G2: control group (n = 7) | Baseline | 8.91 (2.04) | 7.95 (2.04) | |||||||||
| One wk | 10.12 (1.81) | 8.31 (1.81) | |||||||||||
| Dental visit, divided into seven steps, and professional teeth-cleaning, divided in the following five steps, reported as the number of steps completed at each visit and time to perform them | Two wk | 10.54 (1.68) | 9.17 (1.68) | ||||||||||
| Three wk | 11.48 (1.28) | 10.09 (1.28) | |||||||||||
| Completion time per step (min) | |||||||||||||
| Baseline | 1.41 (0.47) | 7.95 (2.04) | |||||||||||
| One wk | 1.04 (0.35) | 8.31 (1.81) | |||||||||||
| Two wk | 1.00 (0.43) | 9.17 (1.68) | |||||||||||
| Three wk | 0.98 (0.45) | 10.09 (1.28) | |||||||||||
| Anxiety Likert Scale Score | |||||||||||||
| Baseline | 1.55 (0.48) | 2.48 (0.48) | |||||||||||
| One wk | 1.62 (0.45) | 2.14 (0.45) | |||||||||||
| Two wk | 1.77 (0.57) | 2.15 (0.57) | |||||||||||
| Three wk | 1.65 (0.54) | 2.08 (0.54) | |||||||||||
| Bossù et al. (2014) [25] | 34 | - | Three yy | PECS (paper) | Provided once by the dentist | TSD, desensitization | One group (n = 34) | Cooperative patients (n) | The majority of children were cooperative during dental procedures (no statistical analysis available) | ||||
| M/F | Tooth extraction 2/2 | ||||||||||||
| 6–12 yy | Number of cooperative patients during preventive, restorative, and surgical procedures | Tooth Filling 8/10 | |||||||||||
| Oral hygiene 30/34 | |||||||||||||
| Dental sealant 18/28 | |||||||||||||
| Different Kind of Images | |||||||||||||
| Lefer et al. (2019) [28] | 52 | From mild to severe | Eight mo | Photos (digital) | Provided at weekdays by teacher | - | One group (n = 52) | Global Skill acquisition Score * | Both scores significantly improved at two-, four-, six-, and eight-month evaluations (p < 0.01) compared to baseline | ||||
| M/F | Baseline | 2.3 (0.6) | |||||||||||
| 3–19 yy | Dental visit, divided into six steps, reported as a score from 1 to 3 (1 = not acquired; 2 = emerging; 3 = acquired), and behavior assessment (Frankl Behavior Score) | Two mo | 2.5 (0.5) | ||||||||||
| Four mo | 2.7 (0.5) | ||||||||||||
| Six mo | 2.7 (0.4) | ||||||||||||
| Eight mo | 2.8 (0.6) | ||||||||||||
| Frankl Behavior Score * | |||||||||||||
| Baseline | 2.7 (0.8) | ||||||||||||
| Two mo | 3.2 (0.9) | ||||||||||||
| Four mo | 3.3 (1.0) | ||||||||||||
| Six mo | 3.4 (0.8) | ||||||||||||
| Eight mo | 3.4 (0.9) | ||||||||||||
| Murshid E. Z. (2017) [30] | 40 | - | Six mo | Dental book (Paper) | Provided daily by parents | - | One Group (n = 40) | Cooperative patients (%) * | Children’s behavior significantly improved at a four-month evaluation (p < 0.01) | ||||
| M/F | One wk | ||||||||||||
| 5–9 yy | Dental visit, professional teeth-cleaning, and fluoride therapy, reported as the number of patients for each behavior score (Frankl Behavior Score) | Definitely positive | 0 | ||||||||||
| Positive | 47.5 | ||||||||||||
| Negative | 32.5 | ||||||||||||
| Definitely negative | 20.0 | ||||||||||||
| Four mo | |||||||||||||
| Definitely positive | 0 | ||||||||||||
| Positive | 80.0 | ||||||||||||
| Negative | 12.5 | ||||||||||||
| Definitely negative | 7.5 | ||||||||||||
| Nilchian et al. (2017) [31] | 40 | From mild to moderate | Two mo | Coloring pictures (Paper) | Provided twice a day by a trained teacher | - | Two Groups: | G1 | G2 | Number of cooperative patients increased significantly at two-, four-, six-, and eight-week evaluations in both groups (p < 0.01) and at eight weeks during fluoride therapy only in G1 (p < 0.01). No further inter-group differences were found | |||
| M/F | G1: case group (n = 20) | Cooperative patients (%) | |||||||||||
| 6–12 yy | G2: control group (n = 20) | Dental visit | |||||||||||
| Baseline | 15 | 15 | |||||||||||
| Number of cooperative patients during dental visit and fluoride therapy | Two wk | 30 | 15 | ||||||||||
| Four wk | 40 | 25 | |||||||||||
| Six wk | 50 | 55 | |||||||||||
| Eight wk | 70 | 65 | |||||||||||
| Fluoride therapy | |||||||||||||
| Baseline | 0 | 0 | |||||||||||
| Two wk | 0 | 0 | |||||||||||
| Four wk | 0 | 0 | |||||||||||
| Six wk | 5 | 0 | |||||||||||
| Eight wk | 30 | 5 | |||||||||||
| Cagetti et al. (2015) [4] | 83 | From mild to severe | One and a half mo | Coloring pictures (digital) | Provided twice a week by psychologist, then daily by parents | - | One group (n = 83) | Cooperative patients (n) | The majority of children were cooperative (no statistical analysis available). Cooperation was statistically significantly influenced by the child’s verbal fluency in all treatments (p ranging from 0.04 to 0.01) and by intellectual disability in restorative treatment (p = 0.04) | ||||
| M/F | Number of cooperative patients during dental visit and preventive and restorative treatments | Oral examination 77/83 | |||||||||||
| 6–12 yy | Teeth-cleaning 77/77 | ||||||||||||
| Sealant 70/77 | |||||||||||||
| Restoration 41/44 | |||||||||||||
| Schindel et al. (2014) [34] | 16 | - | Two wk | Photos (Paper) | Provided twice a day by a trained teacher | TSD | One group (n = 20) | Mean number of steps completed (n) † | The mean number of steps completed increased and time required per step decreased at a two-week evaluation in all children except one. | ||||
| M/F | Baseline | 6.37 (5.10) | |||||||||||
| 10–23 yy | |||||||||||||
| Orthodontic examination, divided into 13 steps, reported as the number of steps completed and time to perform them. | Two wk | 11.12 (4.18) | |||||||||||
| Mean completion time (min) † | |||||||||||||
| Baseline | 18.78 (7.08) | ||||||||||||
| Two wk | 11.54 (4.58) | ||||||||||||
| Bäckman and Pilebro, (1999) [24] | 32 | From mild to severe | 18 mo | Dental book (Paper) | Provided once or more by parents | - | Two groups: | G1 | G2 | Children in G1 were more cooperative compared to G2 (no statistical analysis available) | |||
| M/F | G1: visual pedagogy (n = 16) | Number of cooperative patients (n) | |||||||||||
| 3–6 yy | G2: control group (n = 16) | Dental visit | 11 | 4 | |||||||||
| Fluoride therapy | 2 | 0 | |||||||||||
| Number of cooperative patients during dental visit, tooth-cleaning, and fluoride therapy | Teeth-cleaning | 4 | 0 | ||||||||||
| Video or Video + Images | |||||||||||||
| Orellana et al. (2019) [32] | 74 | From moderate to severe | - | Video | Provided weekly by dentist | TSD, BM, PM | 2 groups: | G1 | G2 | The mean number of steps completed increased (p < 0.01) and the children’s behavior improved (p < 0.01) at a seven-week evaluation and was maintained after one month. | |||
| M/F | G1: 4–9 yy group (n = 52) | Mean number of steps completed (n) * | |||||||||||
| 4–17 yy | G2: 10–17 yy group (n = 22) | Baseline | 3.9 (2.7) | 4.4 (2.6) | |||||||||
| One mo | 9.4 (1.5) | 9.5 (1.7) | |||||||||||
| Dental visit, divided in 10 steps, reported as the number of steps completed and behavior assessment (Frankl Behavior Score) | Frankl Behavior Score * | ||||||||||||
| Baseline | 1.9 (0.8) | 2.0 (0.8) | |||||||||||
| One mo | 3.3 (0.8) | 3.5 (0.7) | |||||||||||
| Isong et al. (2014) [27] | 80 | From mild to moderate | Six mo | Video | Once or more at the home with parents | - | Four groups: | G1 | G2 | G3 | G4 | Anxiety and behavior scores statistically significantly decreased at a six-month evaluation in G3 and G4 (p < 0.05). | |
| M/F | G1: control group (n = 20) | Venham Behavior Scale * | |||||||||||
| 7–17 yy | G2: video peer model (n = 20) | Baseline | 2.2 (1.9) | 2.7 (1.8) | 2.5 (1.6) | 2.9 (1.5) | |||||||
| G3: video googles (n = 20) | Six mo | 2.3 (1.6) | 2.9 (2.0) | 1.7 (1.9) | 2.1 (1.6) | ||||||||
| G4: video model + goggles (n = 20) | Venham Anxiety Scale * | ||||||||||||
| Baseline | 2.4 (1.8) | 2.6 (1.8) | 2.6 (1.3) | 2.9 (1.3) | |||||||||
| Dental visit, reported as a behavior and anxiety assessment (Venham scores) | Six mo | 2.3 (1.6) | 2.6 (1.9) | 1.7 (1.8) | 2.1 (1.6) | ||||||||
| Orellana et al. (2014) [33] | 38 | From mild to severe | Four wk | Images (paper) and video | Provided twice a week by dentist | TSD, desensitization, and modelling | 1 group (n = 38) | Mean number of steps completed (n) † | The mean number of steps completed statistically significantly increased (p < 0.01) and children’s behavior improved (p < 0.01) at a four-week evaluation. Improvements were observed in high-functioning children as well as children with mild and severe disability. | ||||
| M/F | Baseline | 3.03 (2.22) | |||||||||||
| 4–10 yy | Dental visit, divided into 10 steps, reported as the number of steps completed and behavior assessment (Frankl Behavior Score) | Four wk | 9.03 (2.05) | ||||||||||
| Frankl Behavior Score * | |||||||||||||
| Baseline | 1.95 (0.77) | ||||||||||||
| Four wk | 3.24 (0.88) | ||||||||||||
| Study | Confounding | Selection of Participants | Classification of Interventions | Deviations from Intervention | Missing Data | Measurements of Outcome | Selection of the Reported Results | Overall |
|---|---|---|---|---|---|---|---|---|
| ORAL HYGIENE | ||||||||
| Du et al., 2020 [17] | Serious | Low | Low | Low | Moderate | Serious | Low | Moderate |
| Al-Batayneh et al., 2020 [14] | Critical | Low | Low | Serious | Moderate | Serious | Low | Moderate |
| Zhou et al., 2020 [21] | Moderate | Low | Low | Moderate | Low | Serious | Low | Moderate |
| Doichinova et al., 2019 [16] | Serious | Low | Moderate | Serious | Low | Serious | Low | Moderate |
| Lopez Cazaux et al., 2019 [19] | Critical | Low | Low | Moderate | Low | Serious | Low | Moderate |
| Ramassamy et al., 2019 [22] | Moderate | Low | Low | Low | Low | Serious | Low | Low |
| Doichinova & Peneva, 2012 [15] | Critical | Low | Moderate | Moderate | Low | Serious | Low | Moderate |
| Pilebro & Bäckman, 2005 [18] | Serious | Low | Low | Low | Low | Serious | Low | Moderate |
| DENTAL CARE | ||||||||
| Orellana et al., 2019 [32] | Moderate | Low | Low | Low | Low | Serious | Moderate | Moderate |
| Lefer et al., 2019 [28] | Serious | Low | Low | Low | Low | Serious | Low | Moderate |
| Hidayatullah et al., 2018 [26] | Serious | Low | Low | Low | Low | Serious | Low | Moderate |
| Murshid, 2017 [30] | Critical | Low | Low | Serious | Low | Low | Low | Moderate |
| Zink et al., 2016 [23] | Critical | Low | Low | Low | Low | Serious | Low | Moderate |
| Cagetti et al., 2015 [4] | Serious | Low | Low | Moderate | Low | Serious | Low | Moderate |
| Schindel et al., 2014 [34] | Critical | Serious | Serious | Low | Moderate | Serious | Critical | Serious |
| Bossù et al., 2014 [25] | Serious | Serious | Low | Moderate | Low | Serious | Low | Moderate |
| Orellana et al., 2014 [33] | Serious | Low | Low | Low | Moderate | Serious | Low | Moderate |
| Bäckman & Pilebro, 1999 [24] | Moderate | Low | Moderate | Serious | Low | Serious | Low | Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balian, A.; Cirio, S.; Salerno, C.; Wolf, T.G.; Campus, G.; Cagetti, M.G. Is Visual Pedagogy Effective in Improving Cooperation towards Oral Hygiene and Dental Care in Children with Autism Spectrum Disorder? A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 789. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020789
Balian A, Cirio S, Salerno C, Wolf TG, Campus G, Cagetti MG. Is Visual Pedagogy Effective in Improving Cooperation towards Oral Hygiene and Dental Care in Children with Autism Spectrum Disorder? A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(2):789. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020789
Chicago/Turabian StyleBalian, Araxi, Silvia Cirio, Claudia Salerno, Thomas Gerhard Wolf, Guglielmo Campus, and Maria Grazia Cagetti. 2021. "Is Visual Pedagogy Effective in Improving Cooperation towards Oral Hygiene and Dental Care in Children with Autism Spectrum Disorder? A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 2: 789. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020789