The History, Efficacy, and Safety of Potential Therapeutics: A Narrative Overview of the Complex Life of COVID-19

 ,
,  , ,
, ,  and
and 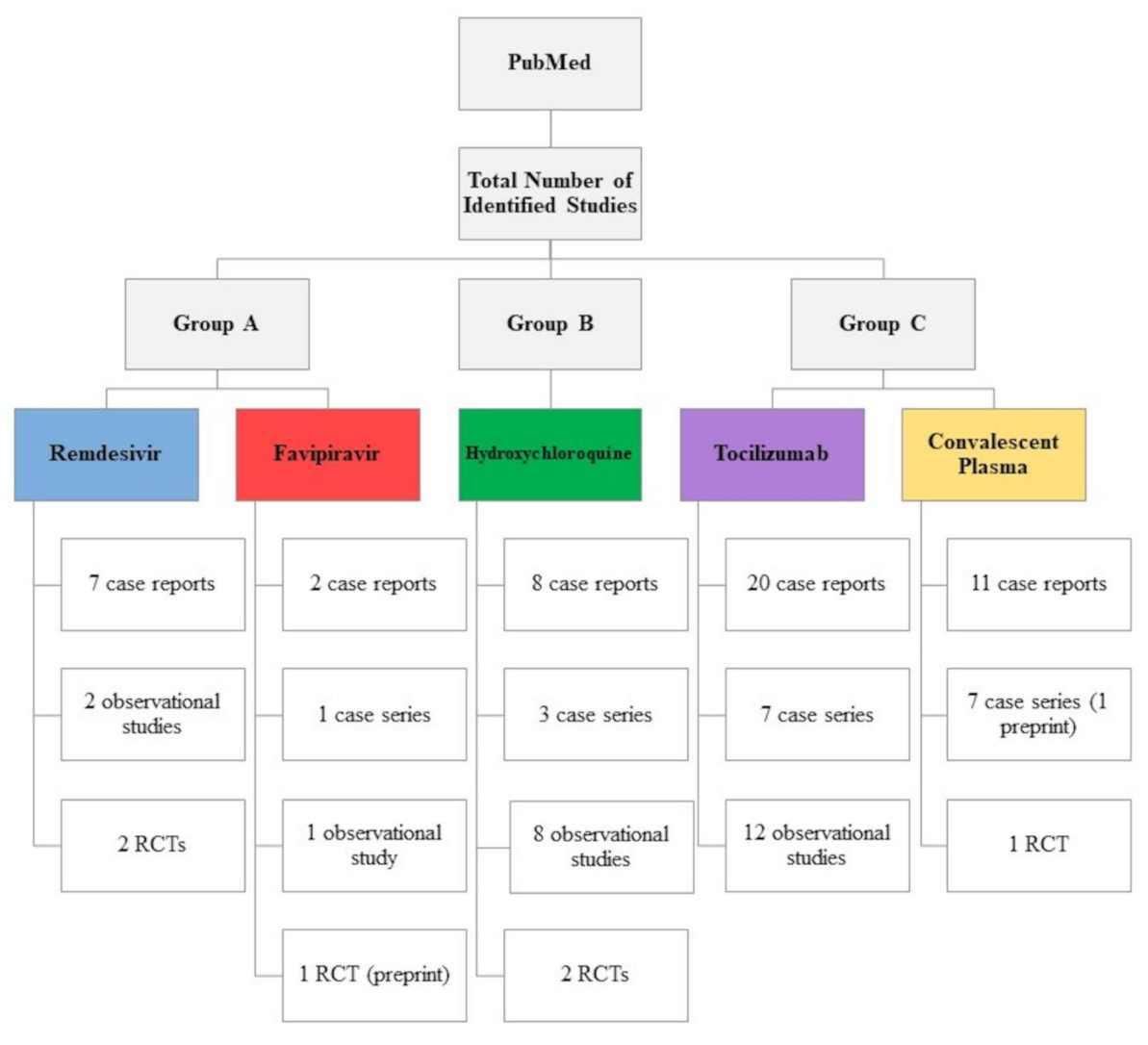{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
- Withdrawals from study participation: defined as the percentage of patients who withdrew from the studies because of adverse drug events,
- Any adverse event: defined as the percentage of patients who reported adverse drug events of any grade,
- Serious adverse events: defined as the percentage of patients who reported serious adverse drug events (grade 3 or 4).
3. Results
3.1. Group A: Inhibitors of SARS-CoV-2 Replication
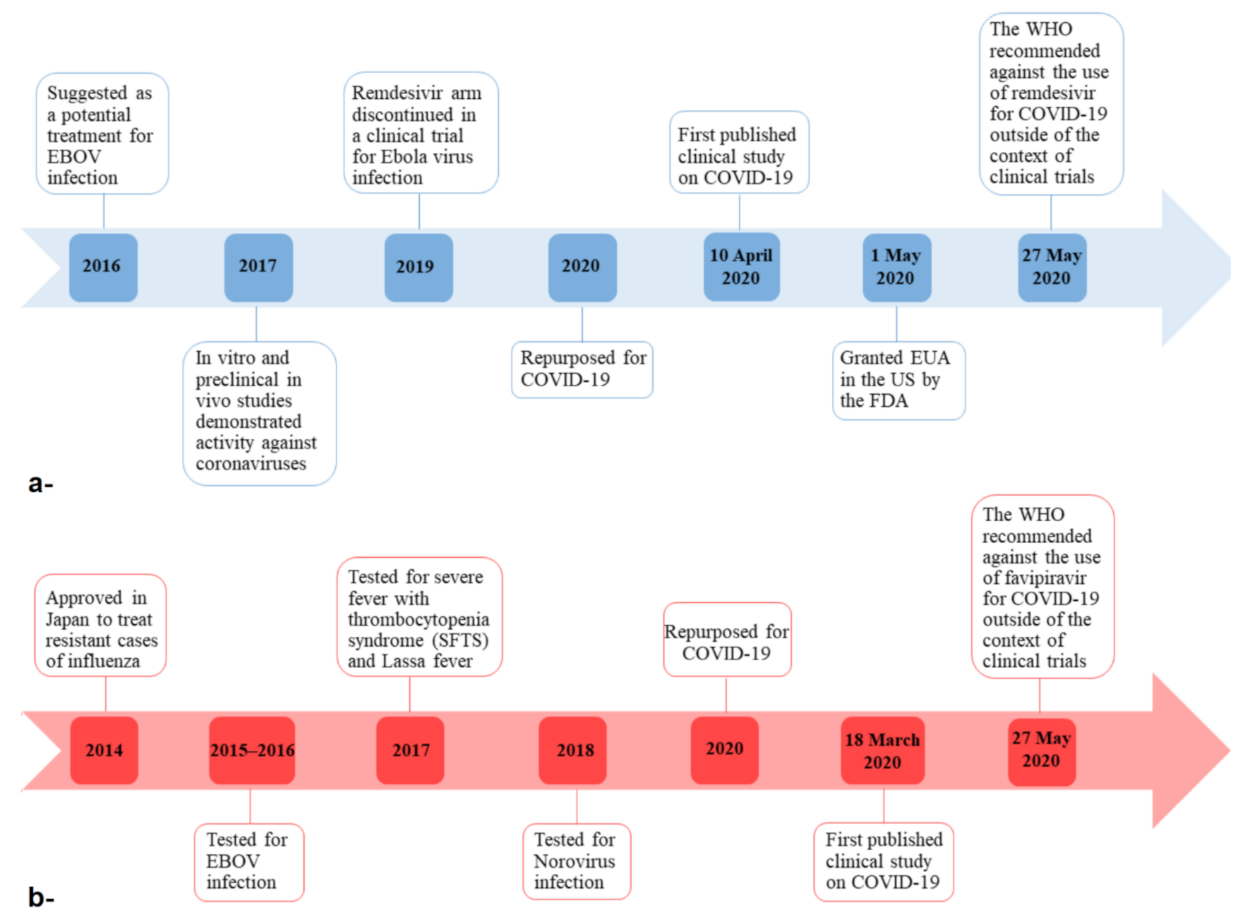
3.1.1. Remdesivir
3.1.2. Favipiravir
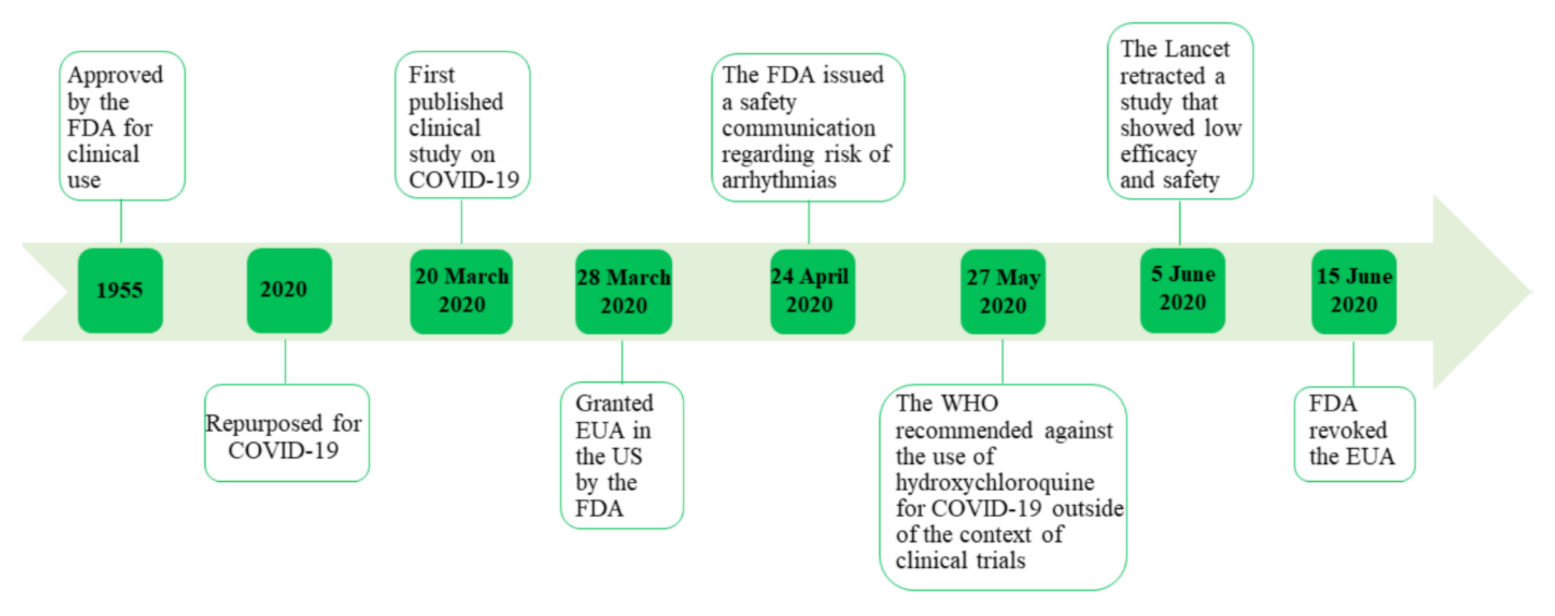
3.2. Group B: Inhibitors of SARS-CoV-2 Entry
Hydroxychloroquine
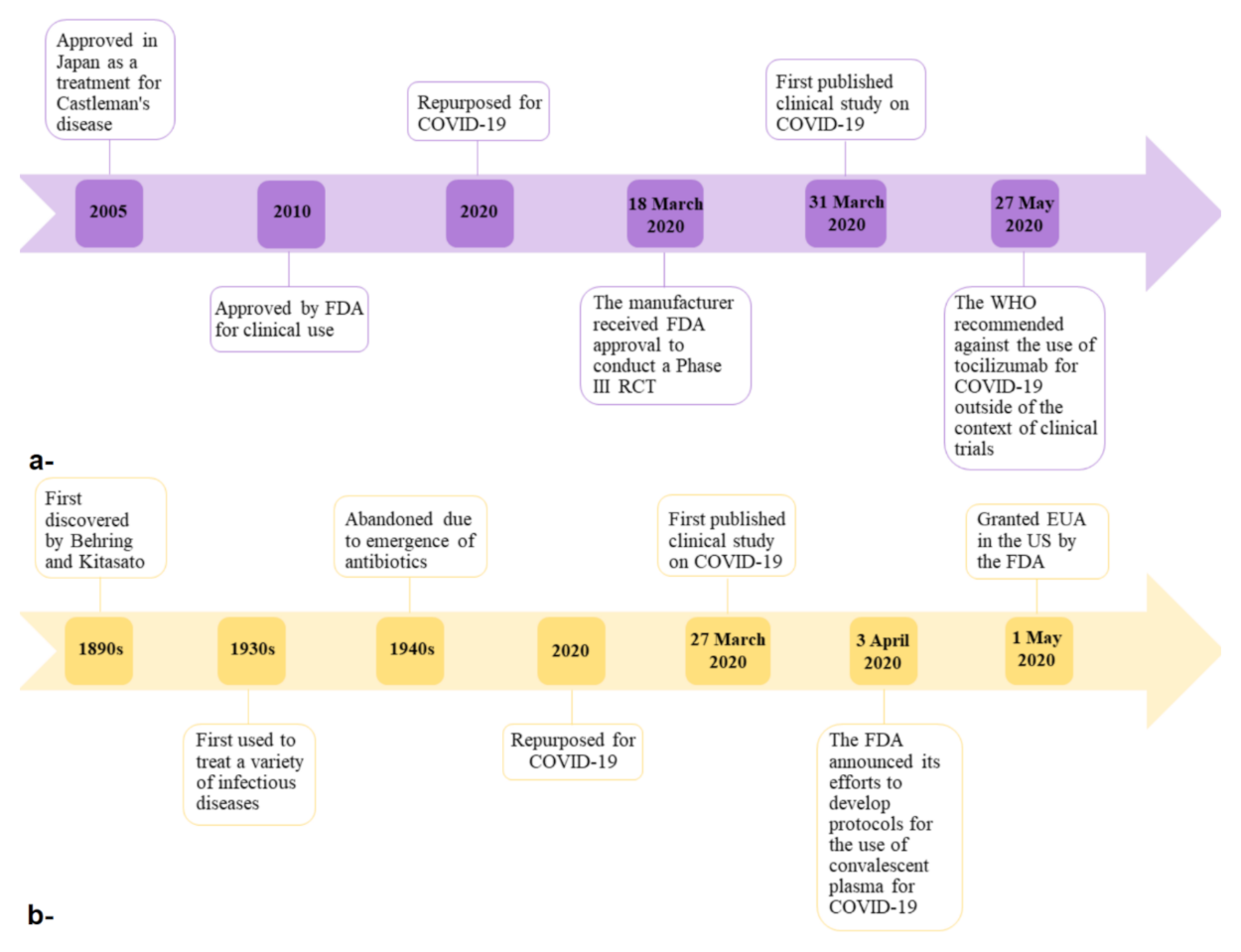
3.3. Group C: Adjunctive Therapies
3.3.1. Tocilizumab
3.3.2. Convalescent Plasma
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Drosten, C.; Stephan, G.; Wolfgang, P.; Sylvie, V.D.W.; Hans-Reinhard, B.; Stephan, B.; Holger, R.; Marcus, P.; Larissa, K.; Ron, A.M.; et al. Identification of a Novel Coronavirus in Patients with Severe Acute Respiratory Syndrome. N. Engl. J. Med. 2003, 348, 1967–1976. [Google Scholar] [CrossRef] [PubMed]
- Zaki, A.M.; Van Boheemen, S.; Bestebroer, T.M.; Osterhaus, A.D.; Fouchier, R.A. Isolation of a Novel Coronavirus from a Man with Pneumonia in Saudi Arabia. N. Engl. J. Med. 2012, 367, 1814–1820. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A Pneumonia Outbreak Associated with a New Coronavirus of Probable Bat Origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrosillo, N.; Viceconte, G.; Ergonul, O.; Ippolito, G.; Petersen, E. Covid-19, Sars and Mers: Are They Closely Related? Clin. Microbiol. Infect. 2020, 26, 729–734. [Google Scholar] [CrossRef]
- Peeri, N.C.; Shrestha, N.; Rahman, M.S.; Zaki, R.; Tan, Z.; Bibi, S.; Baghbanzadeh, M.; Aghamohammadi, N.; Zhang, W.; Haque, U. The Sars, Mers and Novel Coronavirus (Covid-19) Epidemics, the Newest and Biggest Global Health Threats: What Lessons Have We Learned? Int. J. Epidemiol. 2020, 49, 717–726. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Coronavirus Disease (Covid-19) Situation Report 152. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 7 June 2020).
- Consensus Document on the Epidemiology of Severe Acute Respiratory Syndrome (Sars). Available online: https://apps.who.int/iris/handle/10665/70863 (accessed on 7 June 2020).
- Who Mers Global Summary and Assessment of Risk. Available online: https://www.who.int/publications/i/item/who-mers-cov-global-summary-and-assessment-of-risk (accessed on 7 June 2020).
- Report of the Who-China Joint Mission on Coronavirus Disease 2019 (Covid-19). Available online: https://www.who.int/publications/i/item/report-of-the-who-china-joint-mission-on-coronavirus-disease-2019-(covid-19) (accessed on 7 June 2020).
- Tobaiqy, M.; Qashqary, M.; Al-Dahery, S.; Mujallad, A.; Hershan, A.A.; Kamal, M.A.; Helmi, N. Therapeutic Management of Patients with Covid-19: A Systematic Review. Infect. Prev. Pract. 2020, 2, 100061. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Clinical Management of Covid-19. Available online: https://www.who.int/publications/i/item/clinical-management-of-covid-19 (accessed on 7 June 2020).
- Draft Landscape of Covid-19 Candidate Vaccines 2 June 2020. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 8 June 2020).
- Alhumaid, S.; Tobaiqy, M.; Albagshi, M.; Alrubaya, A.; Algharib, F.; Aldera, A.; Alali, J. Mers-Cov Transmitted from Animal-to-Human vs. Merscov Transmitted from Human-to-Human: Comparison of Virulence and Therapeutic Outcomes in a Saudi Hospital. Trop. J. Pharm. Res. 2018, 17, 1155–1164. [Google Scholar] [CrossRef]
- James, S.; Marguerite, M.; Monogue, L.; Jodlowski, T.Z.; Cutrell, J.B. Pharmacologic Treatments for Coronavirus Disease 2019 (Covid-19): A Review. JAMA 2020, 323, 1824–1836. [Google Scholar]
- National Center for Biotechnology Information (NCBI). Remdesivir, Cid=121304016. PubChem Database. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Remdesivir (accessed on 31 May 2020).
- Warren, K.T.; Jordan, R.; Lo, M.K.; Ray, A.S.; Mackman, R.L.; Soloveva, V.; Siegel, D.; Perron, M.; Bannister, R.; Hui, H.C.; et al. Therapeutic Efficacy of the Small Molecule Gs-5734 against Ebola Virus in Rhesus Monkeys. Nature 2016, 531, 381–385. [Google Scholar] [CrossRef]
- Mulangu, S.; Dodd, L.E.; Davey, R.T., Jr.; Tshiani Mbaya, O.; Proschan, M.; Mukadi, D.; Manzo, M.L.; Nzolo, D.; Oloma, A.T.; Ibanda, A.; et al. A Randomized, Controlled Trial of Ebola Virus Disease Therapeutics. N. Engl. J. Med. 2019, 381, 2293–2303. [Google Scholar] [CrossRef]
- Robert, J.; Hogg, A.; Warren, T.; de Wit, E.; Sheahan, T.; Lo, M.; Soloveva, V.; Weidner, J.; Gomba, L.; Feldmann, F.; et al. Broad-Spectrum Investigational Agent Gs-5734 for the Treatment of Ebola, Mers Coronavirus and Other Pathogenic Viral Infections with High Outbreak Potential. Open Forum Infect. Dis. 2017, 4, S737. [Google Scholar]
- Wu, R.; Wang, L.; Kuo, H.C.D.; Shannar, A.; Peter, R.; Chou, P.J.; Li, S.; Hudlikar, R.; Liu, X.; Liu, Z.; et al. An Update on Current Therapeutic Drugs Treating Covid-19. Curr. Pharmacol. Rep. 2020, 6, 56–70. [Google Scholar] [CrossRef] [PubMed]
- Gordon, C.J.; Tchesnokov, E.P.; Woolner, E.; Perry, J.K.; Feng, J.Y.; Porter, D.P.; Götte, M. Remdesivir Is a Direct-Acting Antiviral That Inhibits Rna-Dependent Rna Polymerase from Severe Acute Respiratory Syndrome Coronavirus 2 with High Potency. J Biol. Chem. 2020, 295, 6785–6797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Food and Drug Administration (FDA). Emergency Use Authorization (Eua) Information, and List of All Current Euas. Available online: https://www.fda.gov/emergency-preparedness-and-response/mcm-legal-regulatory-and-policy-framework/emergency-use-authorization (accessed on 1 June 2020).
- Hillaker, E.; Belfer, J.J.; Bondici, A.; Murad, H.; Dumkow, L.E. Delayed Initiation of Remdesivir in a Covid-19-Positive Patient. Pharmacotherapy 2020, 40, 592–598. [Google Scholar] [CrossRef] [Green Version]
- Spinello, A.; Cossu, M.V.; Ridolfo, A.L.; Rech, R.; Bonazzetti, C.; Pagani, G.; Gubertini, G.; Coen, M.; Magni, C.; Castelli, A.; et al. Compassionate Remdesivir Treatment of Severe Covid-19 Pneumonia in Intensive Care Unit (Icu) and Non-Icu Patients: Clinical Outcome and Differences in Post-Treatment Hospitalisation Status. Pharmacol. Res. 2020, 158, 104899. [Google Scholar]
- Grein, J.; Ohmagari, N.; Shin, D.; Diaz, G.; Asperges, E.; Castagna, A.; Feldt, T.; Green, G.; Green, M.L.; Lescure, F.-X.; et al. Compassionate Use of Remdesivir for Patients with Severe Covid-19. N. Engl. J. Med. 2020, 382, 2327–2336. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of Covid-19 Preliminary Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in Adults with Severe Covid-19: A Randomised, Double-Blind, Placebo-Controlled, Multicentre Trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- Shannon, A.; Le, N.T.T.; Selisko, B.; Eydoux, C.; Alvarez, K.; Guillemot, J.C.; Decroly, E.; Peersen, O.; Ferron, F.; Canard, B. Remdesivir and Sars-Cov-2: Structural Requirements at Both Nsp12 Rdrp and Nsp14 Exonuclease Active-Sites. Antivir. Res. 2020, 178, 104793. [Google Scholar] [CrossRef]
- Boltz, D.; Jerry, A.; Aldridge, R.; Webster, R.G.; Govorkova, E.A. Drugs in Development for Influenza. Drugs 2010, 70, 1349–1362. [Google Scholar] [CrossRef]
- Shiraki, K.; Daikoku, T. Favipiravir, an Anti-Influenza Drug against Life-Threatening Rna Virus Infections. Pharmacol. Ther. 2020, 209, 107512. [Google Scholar] [CrossRef] [PubMed]
- Cai, Q.; Yang, M.; Liu, D.; Chen, J.; Shu, D.; Xia, J.; Liao, X.; Gu, Y.; Cai, Q.; Yang, Y.; et al. Experimental Treatment with Favipiravir for Covid-19: An Open-Label Control Study. Engineering 2020, 6, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zhang, Y.; Huang, J.; Yin, P.; Cheng, Z.; Wu, J.; Chen, S.; Zhang, Y.; Chen, B.; Lu, M.; et al. Favipiravir Versus Arbidol for Covid-19: A Randomized Clinical Trial. medRxiv 2020. Available online: https://www.medrxiv.org/content/medrxiv/early/2020/04/15/2020.03.17.20037432.full.pdf (accessed on 21 January 2021).
- National Center for Biotechnology Information (NCBI). Favipiravir, Cid=492405. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Favipiravir (accessed on 11 June 2020).
- Victoria, P.; Pepperrell, T.; Hill, A. A Review of the Safety of Favipiravir a Potential Treatment in the Covid-19 Pandemic? J. Virus Erad. 2020, 6, 45–51. [Google Scholar]
- Du, Y.-X.; Chen, X. Favipiravir: Pharmacokinetics and Concerns about Clinical Trials for 2019-Ncov Infection. Clin. Pharmacol. Ther. 2020, 108, 242–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Response to “Dose Rationale for Favipiravir Use in Patients Infected with Sars-Cov-2”. Clin. Pharmacol. Ther. 2020, 108, 190. [CrossRef]
- Philippine, E.; Solas, C.; Touret, F.; Mentré, F.; Malvy, D.; de Lamballerie, X.; Guedj, J. Dose Rationale for Favipiravir Use in Patients Infected with Sars-Cov-2. Clin. Pharmacol. Ther. 2020, 108, 188. [Google Scholar]
- Irie, K.; Nakagawa, A.; Fujita, H.; Tamura, R.; Eto, M.; Ikesue, H.; Muroi, N.; Tomii, K.; Hashida, T. Pharmacokinetics of Favipiravir in Critically Ill Patients with Covid-19. Clin. Transl. Sci. 2020, 13, 880–885. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information (NCBI). Hydroxychloroquine, Cid=3652. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Hydroxychloroquine (accessed on 29 May 2020).
- DrugBank. Hydroxychloroquine. Available online: https://www.drugbank.ca/drugs/DB01611 (accessed on 15 June 2020).
- Yao, X.; Ye, F.; Zhang, M.; Cui, C.; Huang, B.; Niu, P.; Liu, X.; Zhao, L.; Dong, E.; Song, C.; et al. In Vitro Antiviral Activity and Projection of Optimized Dosing Design of Hydroxychloroquine for the Treatment of Severe Acute Respiratory Syndrome Coronavirus 2 (Sars-Cov-2). Clin. Infect. Dis. 2020, 71, 732–739. [Google Scholar] [CrossRef] [Green Version]
- Philippe, G.; Lagier, J.-C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.E.; et al. Hydroxychloroquine and Azithromycin as a Treatment of Covid-19: Results of an Open-Label Non-Randomized Clinical Trial. Int. J. Antimicrob. Agents 2020, 56, 105949. [Google Scholar]
- Philippe, G.; Lagier, J.-C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Sevestre, J.; Mailhe, M.; Doudier, B.; Aubry, C.; Amrane, S.; et al. Clinical and Microbiological Effect of a Combination of Hydroxychloroquine and Azithromycin in 80 Covid-19 Patients with at Least a Six-Day Follow Up: A Pilot Observational Study. Travel Med. Infect. Dis. 2020, 34, 101663. [Google Scholar]
- Samia, A.; Kilgore, P.; Chaudhry, Z.S.; Jacobsen, G.; Wang, D.D.; Huitsing, K.; Brar, I.; Alangaden, G.J.; Ramesh, M.S.; McKinnon, J.E.; et al. Treatment with Hydroxychloroquine, Azithromycin, and Combination in Patients Hospitalized with Covid-19. Int. J. Infect. Dis. 2020, 97, 396–403. [Google Scholar]
- Rosenberg, E.S.; Dufort, E.M.; Udo, T.; Wilberschied, L.A.; Kumar, J.; Tesoriero, J.; Weinberg, P.; Kirkwood, J.; Muse, A.; DeHovitz, J.; et al. Association of Treatment with Hydroxychloroquine or Azithromycin with in-Hospital Mortality in Patients with Covid-19 in New York State. JAMA 2020, 323, 2493–2502. [Google Scholar] [CrossRef] [PubMed]
- Matthieu, M.; Tran, V.T.; Roumier, M.; Chabrol, A.; Paule, R.; Guillaud, C.; Fois, E.; Lepeule, R.; Szwebel, T.-A.; Lescure, F.-X.; et al. Clinical Efficacy of Hydroxychloroquine in Patients with Covid-19 Pneumonia Who Require Oxygen: Observational Comparative Study Using Routine Care Data. BMJ 2020, 369, m1844. [Google Scholar]
- Mehra, M.R.; Ruschitzka, F.; Patel, A.N. RETRACTED: Hydroxychloroquine or chloroquine with or without a macrolide for treatment of COVID-19: A multinational registry analysis. Lancet 2020. [Google Scholar] [CrossRef]
- Joshua, G.; Sun, Y.; Platt, J.; Zucker, J.; Baldwin, M.; Hripcsak, G.; Labella, A.; Manson, D.; Kubin, C.; Barr, R.G.; et al. Observational Study of Hydroxychloroquine in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2020, 382, 2411–2418. [Google Scholar]
- Tang, W.; Cao, Z.; Han, M.; Wang, Z.; Chen, J.; Sun, W.; Wu, Y.; Xiao, W.; Liu, S.; Chen, E.; et al. Hydroxychloroquine in Patients with Mainly Mild to Moderate Coronavirus Disease 2019: Open Label, Randomised Controlled Trial. BMJ 2020, 369, m1849. [Google Scholar] [CrossRef]
- Self, W.H.; Semler, M.W.; Leither, L.M.; Casey, J.D.; Angus, D.C.; Brower, R.G.; Chang, S.Y.; Collins, S.P.; Eppensteiner, J.C.; Filbin, M.R.; et al. Effect of Hydroxychloroquine on Clinical Status at 14 Days in Hospitalized Patients with Covid-19: A Randomized Clinical Trial. JAMA 2020, 324, 2165–2176. [Google Scholar] [CrossRef]
- Giuseppe, P.; Strumia, A.; Piliego, C.; Bruno, F.; del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. Covid-19 Diagnosis and Management: A Comprehensive Review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar]
- National Center for Biotechnology Information (NCBI). Azithromycin, Cid=447043. Available online: https://pubchem.ncbi.nlm.nih.gov/compound/Azithromycin (accessed on 29 May 2020).
- Food and Drug Administration (FDA). Fda Cautions against Use of Hydroxychloroquine or Chloroquine for Covid-19 Outside of the Hospital Setting or a Clinical Trial Due to Risk of Heart Rhythm Problems. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-cautions-against-use-hydroxychloroquine-or-chloroquine-covid-19-outside-hospital-setting-or (accessed on 1 June 2020).
- U.S. Food and Drug Administration (FDA). Coronavirus (Covid-19) Update: Fda Revokes Emergency Use Authorization for Chloroquine and Hydroxychloroquine. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-revokes-emergency-use-authorization-chloroquine-and (accessed on 15 June 2020).
- The Lancet Editors. Expression of Concern: Hydroxychloroquine or Chloroquine with or without a Macrolide for Treatment of Covid-19: A Multinational Registry Analysis. Lancet 2020, 395, E102. [Google Scholar] [CrossRef]
- The Lancet Editors. Retraction—Hydroxychloroquine or Chloroquine with or without a Macrolide for Treatment of Covid-19: A Multinational Registry Analysis. Lancet 2020, 395, P1820. [Google Scholar] [CrossRef]
- DrugBank. Tocilizumab. Available online: https://www.drugbank.ca/drugs/DB06273 (accessed on 15 June 2020).
- Venkiteshwaran, Adith. Tocilizumab. mAbs 2009, 1, 432–438. [Google Scholar] [CrossRef] [Green Version]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. Covid-19: Consider Cytokine Storm Syndromes and Immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with Covid-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Fu, B.; Xu, X.; Wei, H. Why Tocilizumab Could Be an Effective Treatment for Severe Covid-19? J. Transl. Med. 2020, 18, 164. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Wu, Z.; Li, J.; Zhao, H.; Wang, G. Cytokine Release Syndrome in Severe Covid-19: Interleukin-6 Receptor Antagonist Tocilizumab May Be the Key to Reduce Mortality. Int. J. Antimicrob. Agents 2020, 55, 105954. [Google Scholar] [CrossRef]
- Genentech. Genentech Initiates Phase Iii Clinical Trial of Actemra in Hospitalized Patients with Severe Covid-19 Pneumonia. Available online: https://www.gene.com/media/press-releases/14841/2020-03-18/genentech-initiates-phase-iii-clinical-t (accessed on 20 January 2021).
- Rand, A.; Ibrahim, T.B.H.; Shaar, S.H.; Abdalla, S.; Shukri, K.; Daghfal, J.N.; Khatib, M.Y.; Aboukamar, M.; Abukhattab, M.; Alsoub, H.A.; et al. Tocilizumab for the Treatment of Severe Coronavirus Disease 2019. J. Med. Virol. 2020, 92, 2042–2049. [Google Scholar] [CrossRef]
- Ruggero, C.; de Rossi, N.; Mattioli, F.; Romanelli, G.; Scarpazza, C.; Sormani, M.P.; Cossi, S. Impact of Low Dose Tocilizumab on Mortality Rate in Patients with Covid-19 Related Pneumonia. Eur. J. Intern. Med. 2020, 76, 31–35. [Google Scholar]
- Giambenedetto, D.S.; Ciccullo, A.; Borghetti, A.; Gambassi, G.; Landi, F.; Visconti, E.; Verme, L.Z.D.; Bernabei, R.; Tamburrini, E.; Cauda, R.; et al. Off-Label Use of Tocilizumab in Patients with Sars-Cov-2 Infection. J. Med. Virol. 2020, 92, 1787–1788. [Google Scholar] [CrossRef]
- Klopfenstein, T.S.; Zayet, A.; Lohse, J.C.; Balblanc, J.; Badie, P.Y.; Royer, L.; Toko, C.; Mezher, N.J.; Kadiane-Oussou, M.; Bossert, A.M.; et al. Hospital Tocilizumab multidisciplinary team. Tocilizumab Therapy Reduced Intensive Care Unit Admissions and/or Mortality in Covid-19 Patients. Med. Mal. Infect. 2020, 50, 397–400. [Google Scholar] [CrossRef]
- Luo, P.; Liu, Y.; Qiu, L.; Liu, X.; Liu, D.; Li, J. Tocilizumab Treatment in Covid-19: A Single Center Experience. J. Med. Virol. 2020, 92, 814–818. [Google Scholar] [CrossRef]
- Maria, M.; Arrighi, E.; Serapide, F.; Pelle, M.C.; Tassone, B.; Lionello, R.; Marrazzo, G.; Laganà, D.; Costanzo, F.S.; Matera, G.; et al. Use of Subcutaneous Tocilizumab in Patients with Covid-19 Pneumonia. J. Med. Virol. 2020, 93, 32–34. [Google Scholar]
- Luca, Q.; Sonaglia, A.; McGonagle, D.; Fabris, M.; Peghin, M.; Pecori, D.; de Monte, A.; Bove, T.; Curcio, F.; Bassi, F.; et al. Profiling Covid-19 Pneumonia Progressing into the Cytokine Storm Syndrome: Results from a Single Italian Centre Study on Tocilizumab Versus Standard of Care. J. Med. Virol. 2020, 129, 104444. [Google Scholar]
- Sciascia, S.; Aprà, F.; Baffa, A.; Baldovino, S.; Boaro, D.; Boero, R.; Bonora, S.; Calcagno, A.; Cecchi, I.; Cinnirella, G.; et al. Pilot Prospective Open, Single-Arm Multicentre Study on Off-Label Use of Tocilizumab in Patients with Severe Covid-19. Clin. Exp. Rheumatol. 2020, 38, 529–532. [Google Scholar]
- Toniati, P.; Piva, S.; Cattalini, M.; Garrafa, E.; Regola, F.; Castelli, F.; Franceschini, F.; Airò, P.; Bazzani, C.; Beindorf, E.A.; et al. Tocilizumab for the Treatment of Severe Covid-19 Pneumonia with Hyperinflammatory Syndrome and Acute Respiratory Failure: A Single Center Study of 100 Patients in Brescia, Italy. Autoimmun. Rev. 2020, 19, 102568. [Google Scholar] [CrossRef]
- Xu, X.; Han, M.; Li, T.; Sun, W.; Wang, D.; Fu, B.; Zhou, Y.; Zheng, X.; Yang, Y.; Li, X.; et al. Effective Treatment of Severe Covid-19 Patients with Tocilizumab. Proc. Natl. Acad. Sci. USA 2020, 117, 10970. [Google Scholar] [CrossRef]
- Cellina, M.; Orsi, M.; Bombaci, F.; Sala, M.; Marino, P.; Oliva, G. Favorable Changes of Ct Findings in a Patient with Covid-19 Pneumonia after Treatment with Tocilizumab. Diagn. Interv. Imaging 2020, 101, 323–324. [Google Scholar] [CrossRef]
- De Luna, G.; Habibi, A.; Deux, J.F.; Colard, M.; d’Orengiani, P.H.D.A.; Schlemmer, F.; Joher, N.; Kassasseya, C.; Pawlotsky, J.M.; Ourghanlian, C.; et al. Rapid and Severe Covid-19 Pneumonia with Severe Acute Chest Syndrome in a Sickle Cell Patient Successfully Treated with Tocilizumab. Am. J. Hematol. 2020, 95, 876–878. [Google Scholar] [CrossRef] [Green Version]
- Michot, J.M.; Albiges, L.; Chaput, N.; Saada, V.; Pommeret, F.; Griscelli, F.; Balleyguier, C.; Besse, B.; Marabelle, A.; Netzer, F.; et al. Tocilizumab, an Anti-Il-6 Receptor Antibody, to Treat Covid-19-Related Respiratory Failure: A Case Report. Ann. Oncol. 2020, 31, 961–964. [Google Scholar] [CrossRef]
- Wang, L.; Peng, X.; Wang, Z.H.; Cai, J.; Zhou, F.C. Tocilizumab in the Treatment of a Critical Covid-19 Patient: A Case Report. Eur. Rev. Med. Pharm. Sci. 2020, 24, 5783–5787. [Google Scholar]
- Corrado, C.; Della-Torre, E.; Cavalli, G.; de Luca, G.; Ripa, M.; Boffini, N.; Tomelleri, A.; Baldissera, E.; Rovere-Querini, P.; Ruggeri, A.; et al. Efficacy and Safety of Tocilizumab in Severe Covid-19 Patients: A Single-Centre Retrospective Cohort Study. Eur. J. Intern. Med. 2020, 76, 43–49. [Google Scholar]
- Colaneri, M.; Bogliolo, L.; Valsecchi, P.; Sacchi, P.; Zuccaro, V.; Brandolino, F.; Montecucco, C.; Mojoli, F.; Giusti, E.M.; Bruno, R. Force The Covid Irccs San Matteo Pavia Task. Tocilizumab for Treatment of Severe Covid-19 Patients: Preliminary Results from Smatteo Covid19 Registry (Smacore). Microorganisms 2020, 8, 695. [Google Scholar] [CrossRef] [PubMed]
- Valentina, M.; Milazzo, L.; Oreni, L.; Bestetti, G.; Fossali, T.; Bassoli, C.; Torre, A.; Cossu, M.V.; Minari, C.; Ballone, E.; et al. Off-Label Use of Tocilizumab for the Treatment of Sars-Cov-2 Pneumonia in Milan, Italy. Eur. J. Intern. Med. 2020, 76, 36–42. [Google Scholar]
- Jared, R.; Narayanan, N.; Bhatt, P.J. Use of Tocilizumab for Covid-19-Induced Cytokine Release Syndrome: A Cautionary Case Report. Chest 2020. [Google Scholar] [CrossRef]
- Genentech Inc. Actemra (Tocilizumab) [Package Insert]; Genentech, Inc.: San Francisco, CA, USA, 2019. [Google Scholar]
- Casadevall, A.; Dadachova, E.; Pirofski, L.A. Passive Antibody Therapy for Infectious Diseases. Nat. Rev. Microbiol. 2004, 2, 695–703. [Google Scholar] [CrossRef]
- To, K.K.-W.; Tsang, O.T.Y.; Leung, W.S.; Tam, A.R.; Wu, T.C.; Lung, D.C.; Yip, C.C.; Cai, J.; Chan, J.M.; Chik, T.S.; et al. Temporal Profiles of Viral Load in Posterior Oropharyngeal Saliva Samples and Serum Antibody Responses During Infection by Sars-Cov-2: An Observational Cohort Study. Lancet. Infect. Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Malani, A.N.; Sherbeck, J.P.; Malani, P.N. Convalescent Plasma and Covid-19. JAMA 2020, 324, 524. [Google Scholar] [CrossRef]
- Shen, C.; Wang, Z.; Zhao, F.; Yang, Y.; Li, J.; Yuan, J.; Wang, F.; Li, D.; Yang, M.; Xing, L.; et al. Treatment of 5 Critically Ill Patients with Covid-19 with Convalescent Plasma. JAMA 2020, 323, 1582–1589. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration (FDA). Coronavirus (Covid-19) Update: Fda Coordinates National Effort to Develop Blood-Related Therapies for Covid-19. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-coordinates-national-effort-develop-blood-related-therapies-covid-19 (accessed on 14 June 2020).
- Recommendations for Investigational Covid-19 Convalescent Plasma. Available online: https://www.fda.gov/vaccines-blood-biologics/investigational-new-drug-ind-or-device-exemption-ide-process-cber/recommendations-investigational-covid-19-convalescent-plasma (accessed on 14 June 2020).
- Ahn, J.Y.; Sohn, Y.; Lee, S.H.; Cho, Y.; Hyun, J.H.; Baek, Y.J.; Jeong, S.J.; Kim, J.H.; Ku, N.S.; Yeom, J.S.; et al. Use of Convalescent Plasma Therapy in Two Covid-19 Patients with Acute Respiratory Distress Syndrome in Korea. J. Korean Med. Sci. 2020, 35, 14. [Google Scholar] [CrossRef] [Green Version]
- Çınar, O.E.; Sayınalp, B.; Karakulak, E.A.; Karataş, A.A.; Velet, M.; İnkaya, A.Ç.; Ortaç, N.E.E.; Öcal, S.; Aksu, S.; Haznedaroğlu, İ.C.; et al. Convalescent (Immune) Plasma Treatment in a Myelodysplastic Covid-19 Patient with Disseminated Tuberculosis. Transfus. Apher. Sci. 2020, 102821. [Google Scholar] [CrossRef]
- Duan, K.; Liu, B.; Li, C.; Zhang, H.; Yu, T.; Qu, J.; Zhou, M.; Chen, L.; Meng, S.; Hu, Y.; et al. Effectiveness of Convalescent Plasma Therapy in Severe Covid-19 Patients. Proc. Natl. Acad. Sci. USA 2020, 117, 9490–9496. [Google Scholar] [CrossRef] [Green Version]
- Kong, Y.; Cai, C.; Ling, L.; Zeng, L.; Wu, M.; Wu, Y.; Zhang, W.; Liu, Z. Successful Treatment of a Centenarian with Coronavirus Disease 2019 (Covid-19) Using Convalescent Plasma. Transfus. Apher. Sci. 2020, 102820. [Google Scholar] [CrossRef]
- Salazar, E.; Perez, K.K.; Ashraf, M.; Chen, J.; Castillo, B.; Christensen, P.A.; Eubank, T.; Bernard, D.W.; Eagar, T.N.; Long, S.W.; et al. Treatment of Covid-19 Patients with Convalescent Plasma in Houston, Texas. medRxiv 2020. Available online: https://www.medrxiv.org/content/10.1101/2020.05.08.20095471v1?fbclid=IwAR3jP3silQ4uLrotDCFGZf5-oCjnYtWRcKywzjpYcI6tD8FeI1Y_7rgsZYs (accessed on 21 January 2021).
- Ye, M.; Fu, D.; Ren, Y.; Wang, F.; Wang, D.; Zhang, F.; Xia, X.; Lv, T. Treatment with Convalescent Plasma for Covid-19 Patients in Wuhan, China. J. Med. Virol. 2020, 92, 1890–1901. [Google Scholar] [CrossRef] [Green Version]
- Zeng, Q.-L.; Yu, Z.J.; Gou, J.J.; Li, G.M.; Ma, S.H.; Zhang, G.F.; Xu, J.H.; Lin, W.B.; Cui, G.L.; Zhang, M.M.; et al. Effect of Convalescent Plasma Therapy on Viral Shedding and Survival in Covid-19 Patients. J. Infect. Dis. 2020, 222, 38–43. [Google Scholar] [CrossRef]
- Li, L.; Zhang, W.; Hu, Y.; Tong, X.; Zheng, S.; Yang, J.; Kong, Y.; Ren, L.; Wei, Q.; Mei, H.; et al. Effect of Convalescent Plasma Therapy on Time to Clinical Improvement in Patients with Severe and Life-Threatening Covid-19: A Randomized Clinical Trial. JAMA 2020, 324, 460–470. [Google Scholar] [CrossRef]
- Chai, K.L.; Valk, S.J.; Piechotta, V.; Kimber, C.; Monsef, I.; Doree, C.; Wood, E.M.; Lamikanra, A.A.; Roberts, D.J.; McQuilten, Z.; et al. Convalescent Plasma or Hyperimmune Immunoglobulin for People with Covid-19: A Living Systematic Review. Cochrane Database Syst. Rev. 2020, 7, CD013600. [Google Scholar]
- Merriam-Webster. Words We’re Watching: ‘nfodemic’. Available online: https://www.merriam-webster.com/words-at-play/words-were-watching-infodemic-meaning (accessed on 16 June 2020).
- World Health Organization (WHO). Coronavirus Disease (Covid-19) Advice for the Public: Myth Busters. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/myth-busters (accessed on 16 June 2020).
- Chen, Q.; Allot, A.; Lu, Z. Keep up with the Latest Coronavirus Research. Nature 2020, 579, 193. [Google Scholar] [CrossRef] [Green Version]
- ClinicalTrials.gov. Covid-19. NIH. Available online: https://clinicaltrials.gov/ct2/results?cond=COVID-19 (accessed on 16 June 2020).
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and Immunological Features of Severe and Moderate Coronavirus Disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [Green Version]
- Shweta, J.; Indari, O.; Baral, B.; Kashyap, D.; Varshney, N.; Das, A.; Chatterjee, S.; Jha, H.C. Comorbidity Assessment Is Essential During Covid-19 Treatment. Front. Physiol. 2020, 11, 984. [Google Scholar]
- Chopra, S.S. Industry Funding of Clinical Trials: Benefit or Bias? JAMA 2003, 290, 113–114. [Google Scholar] [CrossRef] [Green Version]
- McKee, D.L.; Sternberg, A.; Stange, U.; Laufer, S.; Naujokat, C. Candidate Drugs against Sars-Cov-2 and Covid-19. Pharmacol. Res. 2020, 157, 104859. [Google Scholar] [CrossRef]
- Liu, C.; Zhou, Q.; Li, Y.; Garner, L.V.; Watkins, S.P.; Carter, L.J.; Smoot, J.; Gregg, A.C.; Daniels, A.D.; Jervey, S.; et al. Research and Development on Therapeutic Agents and Vaccines for Covid-19 and Related Human Coronavirus Diseases. ACS Cent. Sci. 2020, 6, 315–331. [Google Scholar] [CrossRef] [PubMed]
- Itani, R.; Tobaiqy, M.; al Faraj, A. Optimizing Use of Theranostic Nanoparticles as a Life-Saving Strategy for Treating Covid-19 Patients. Theranostics 2020, 10, 5932–5942. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daou, F.; Abou-Sleymane, G.; Badro, D.A.; Khanafer, N.; Tobaiqy, M.; Al Faraj, A. The History, Efficacy, and Safety of Potential Therapeutics: A Narrative Overview of the Complex Life of COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 955. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18030955
Daou F, Abou-Sleymane G, Badro DA, Khanafer N, Tobaiqy M, Al Faraj A. The History, Efficacy, and Safety of Potential Therapeutics: A Narrative Overview of the Complex Life of COVID-19. International Journal of Environmental Research and Public Health. 2021; 18(3):955. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18030955
Chicago/Turabian StyleDaou, Farah, Gretta Abou-Sleymane, Danielle A. Badro, Nagham Khanafer, Mansour Tobaiqy, and Achraf Al Faraj. 2021. "The History, Efficacy, and Safety of Potential Therapeutics: A Narrative Overview of the Complex Life of COVID-19" International Journal of Environmental Research and Public Health 18, no. 3: 955. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18030955