
Spatial and Temporal Characteristics of Hand-Foot-and-Mouth Disease and Its Response to Climate Factors in the Ili River Valley Region of China


Abstract
:1. Introduction
2. Materials and methods
2.1. Study Area
2.2. Data Collection
2.3. Statistical Methods
3. Results
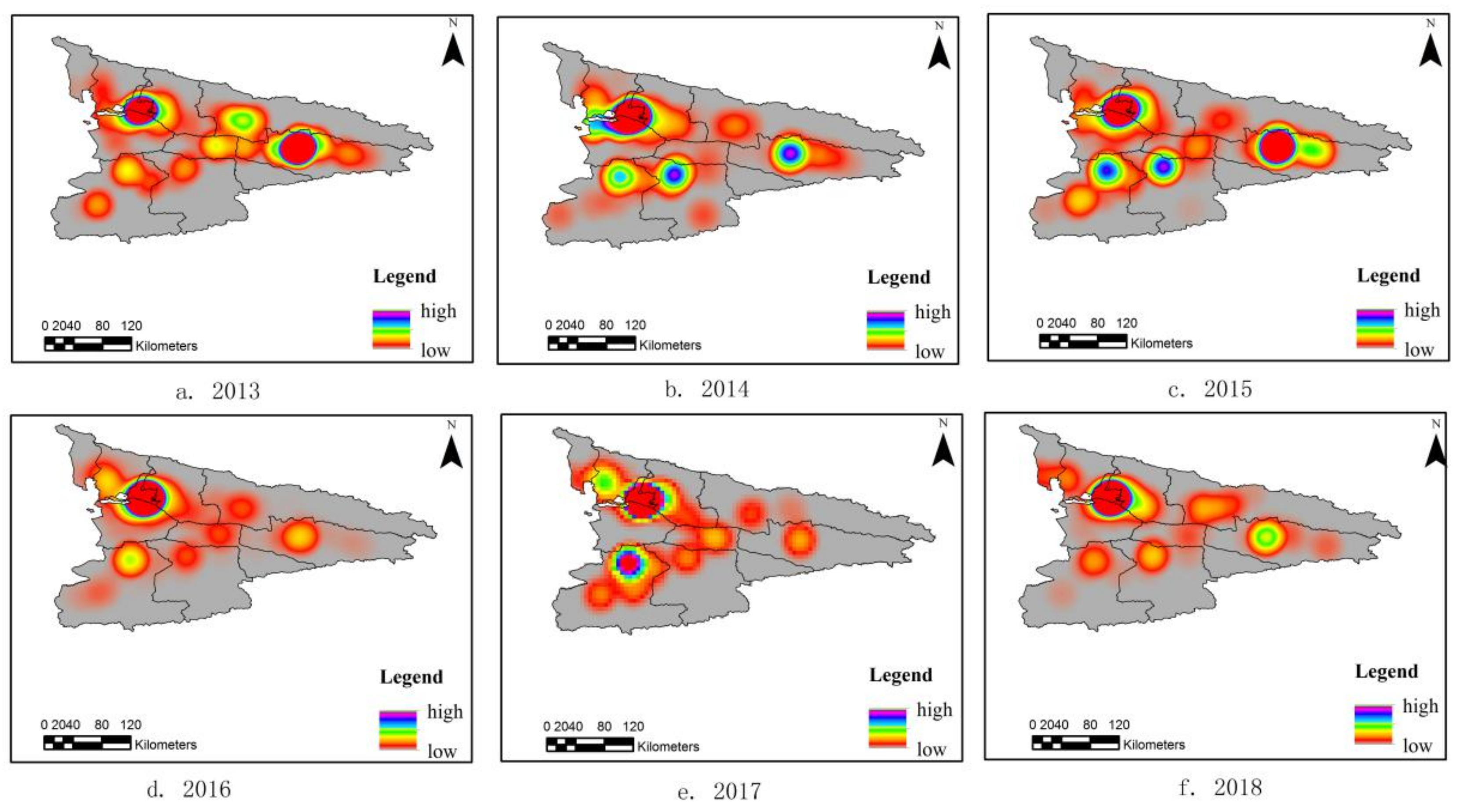
3.1. Spatiotemporal Variation
3.1.1. Year Scale Analysis
3.1.2. Month Scale Analysis
3.2. Temporal and Spatial Variation between Climate Factors and the Incidence of HFMD
3.2.1. Regression Model Selection
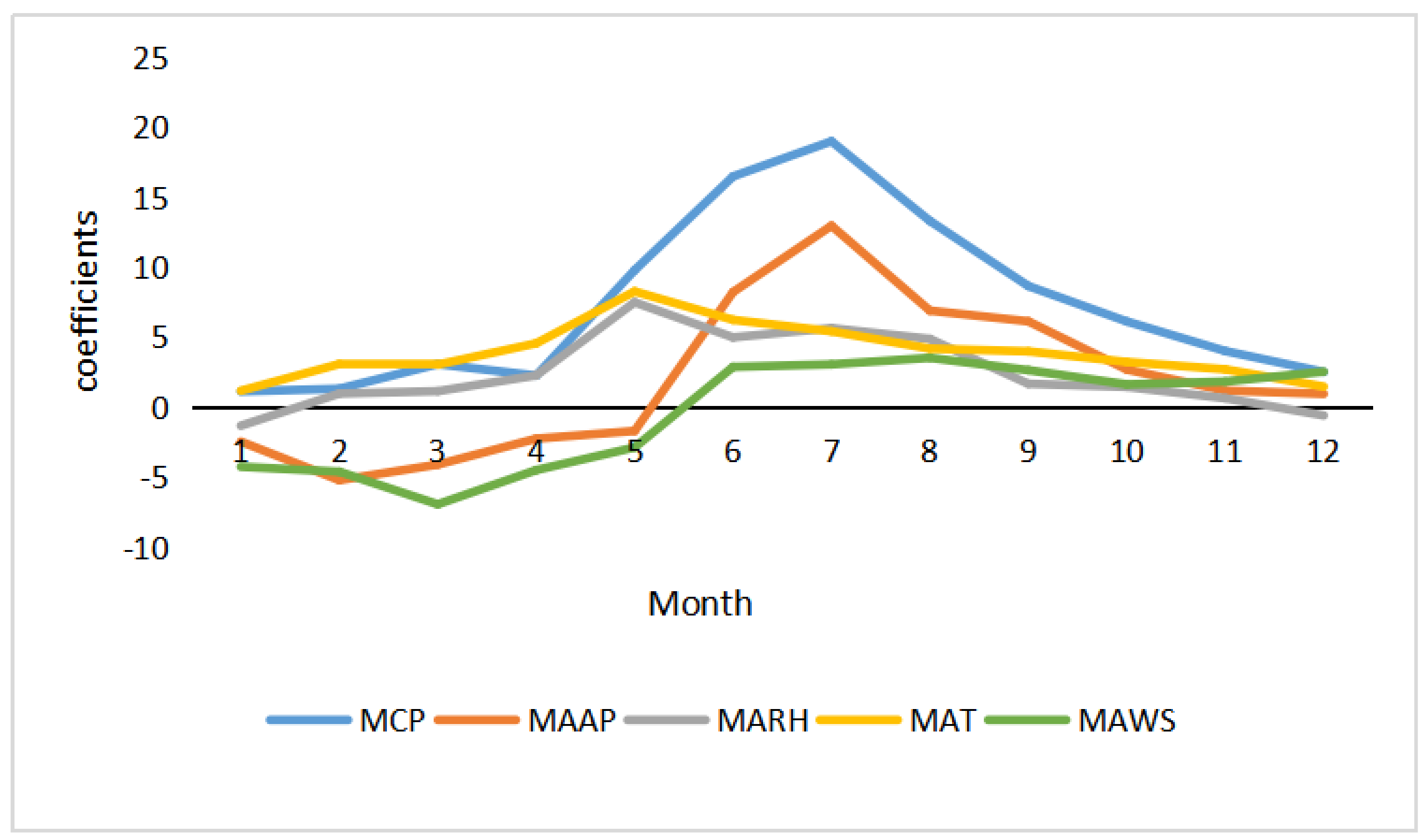
3.2.2. Temporal Distribution
3.2.3. Spatial Distribution
3.3. Quantification of Climate Factors Affecting the Incidence of HFMD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Robinson, C.R.; Doane, F.W.; Rhodes, A.J. Report of an outbreak of febrile illness with pharyngeal lesions and exanthem: Toronto, summer 1957; isolation of group A Coxsackie virus. Can. Med. Assoc. J. 1958, 79, 615–621. [Google Scholar]
- Mao, Q.; Wang, Y.; Bian, L.; Xu, M.; Liang, Z. EV71 vaccine, a new tool to control outbreaks of hand, foot and mouth disease (HFMD). Expert Rev. Vaccines 2016, 15, 599–606. [Google Scholar] [CrossRef]
- Zhang, Y.; Tan, X.; Wang, H.; Yan, D.; Zhu, S.; Wang, D.; Ji, F.; Wang, X.; Gao, Y.; Chen, L.; et al. An outbreak of hand, foot, and mouth disease associated with subgenotype C4 of human enterovirus 71 in Shandong, China. J. Clin. Virol. 2009, 44, 262–267. [Google Scholar] [CrossRef]
- Xing, W.; Liao, Q.; Viboud, C.; Zhang, J.; Sun, J.; Wu, J.; Chang, Z.; Liu, F.; Fang, V.J.; Zheng, Y.; et al. Hand, foot, and mouth disease in China, 2008–2012: An epidemiological study. Lancet Infect. Dis. 2014, 14, 308–318. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Liao, Q.; Ooi, M.H.; Cowling, B.J.; Chang, Z.; Wu, P.; Liu, F.; Li, Y.; Luo, L.; Yu, S.; et al. Epidemiology of Recurrent Hand, Foot and Mouth Disease, China, 2008–2015. Emerg. Infect. Dis. 2018, 24, 432–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bo, Z.; Ma, Y.; Chang, Z.; Zhang, T.; Liu, F.; Zhao, X.; Long, L.; Yi, X.; Xiao, X.; Li, Z. The spatial heterogeneity of the associations between relative humidity and pediatric hand, foot and mouth disease: Evidence from a nation-wide multicity study from mainland China. Sci.Total. Environ. 2020, 707, 136103. [Google Scholar] [CrossRef]
- Wu, X.; Tian, H.; Zhou, S.; Chen, L.; Xu, B. Impact of global change on transmission of human infectious diseases. Sci. China Earth Sci. 2014, 57, 189–203. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Meng, Y.; Xiang, H.; Lu, Y.; Liu, S. Association of Short-Term Exposure to Meteorological Factors and Risk of Hand, Foot, and Mouth Disease: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 8017. [Google Scholar] [CrossRef]
- Koh, W.; Bogich, T.; Siegel, K.; Jin, J.; Chong, E.; Tan, C.; Chen, M.; Horby, P.; Cook, A.R. The Epidemiology of Hand, Foot and Mouth Disease in Asia: A Systematic Review and Analysis. Pediatr. Infect. Dis. J. 2016, 35, e285–e300. [Google Scholar] [CrossRef] [Green Version]
- Song, C.; He, Y.; Bo, Y.; Wang, J.; Ren, Z.; Yang, H. Risk Assessment and Mapping of Hand, Foot, and Mouth Disease at the County Level in Mainland China Using Spatiotemporal Zero-Inflated Bayesian Hierarchical Models. Int. J. Environ. Res. Public Health 2018, 15, 1476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, H.; Li, Y.; Zhang, J.; Chen, Y.; Guo, Y.; Xiao, S.; Hu, J.; Wang, W.; Zhang, W.; Hu, Y.; et al. Quantifying the risk of hand, foot, and mouth disease (HFMD) attributable to meteorological factors in East China: A time series modelling study. Sci. Total Environ. 2020, 728, 138548. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Hu, W.; Jiao, K.; Ren, C.; Jiang, B.; Ma, W. The effect of temperature on childhood hand, foot and mouth disease in Guangdong Province, China, 2010–2013: A multicity study. BMC Infect Dis. 2019, 19, 969. [Google Scholar] [CrossRef] [Green Version]
- Hao, J.; Yang, Z.; Yang, W.; Huang, S.; Tian, L.; Zhu, Z.; Lu, Y.; Xiang, H.; Liu, S. Impact of Ambient Temperature and Relative Humidity on the Incidence of Hand-Foot-Mouth Disease in Wuhan, China. Int. J. Environ. Res. Public Health 2020, 17, 428. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Lin, H.; Li, X.; Lang, L.; Xiao, X.; Ding, P.; He, P.; Zhang, Y.; Wang, M.; Liu, Q. Short-term effects of meteorological factors on children hand, foot and mouth disease in Guangzhou, China. Int. J. Biometeorol. 2014, 58, 1605–1614. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Xie, X.; Chen, X.; Li, Y.; Lu, Y.; Mei, S.; Liao, Y.; Lin, H. Short-term effects of meteorological factors on hand, foot and mouth disease among children in Shenzhen, China: Non-linearity, threshold and interaction. Sci Total Environ. 2016, 539, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Tian, L.; Liang, F.; Xu, M.; Jia, L.; Pan, X.; Clements, A.C.A. Spatio-temporal analysis of the relationship between meteorological factors and hand-foot-mouth disease in Beijing, China. BMC Infect. Dis. 2018, 18, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, T.; Huang, Y.; Yu, S.; Gu, J.; Huang, C.; Xiao, G.; Hao, Y. Spatial-temporal clusters and risk factors of hand, foot, and mouth disease at the district level in Guangdong Province, China. PLoS ONE 2013, 8, e56943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenblatt, M. Remarks on Some Nonparametric Estimates of a Density Function. Ann. Math. Statist. 1956, 27, 832–837. [Google Scholar] [CrossRef]
- Spencer, J.; Angeles, G. Kernel density estimation as a technique for assessing availability of health services in Nicaragua. Health Serv. Outcomes Res. Methodol. 2007, 7, 145–157. [Google Scholar] [CrossRef]
- Kulldorff, M.; Athas, W.F.; Feurer, E.J.; Miller, B.A.; Key, C.R. Evaluating cluster alarms: A space-time scan statistic and brain cancer in Los Alamos, New Mexico. Am. J. Public Health 1998, 88, 1377–1380. [Google Scholar] [CrossRef] [Green Version]
- Fotheringham, A.S.; Brunsdon, C.; Charlton, M. Geographically Weighted Regression: The Analysis of SpatiallyVarying Relationships; John Wiley & Sons Ltd.: Chichester, UK, 2002; pp. 27–64. [Google Scholar]
- Huang, B.; Wu, B.; Barry, M. Geographically and temporally weighted regression for modeling spatio-temporal variation in house prices. Int. J. GIS. 2010, 24, 383–401. [Google Scholar] [CrossRef]
- Hu, Z. Spatial analysis of MODIS aerosol optical depth, PM2.5, and chronic coronary heart disease. Int. J. Health Geogr. 2009, 8, 27. [Google Scholar] [CrossRef] [Green Version]
- Hastie, T.; Tibshirani, R. Generalized Additive Models, 2nd ed.; Chapman & Hall/CRC Press: Boca Raton, FL, USA, 1990; pp. 1–22. [Google Scholar]
- R Development Core Team. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: http://www.rproject.org/ (accessed on 15 November 2020).
- Kim, B.I.; Ki, H.; Park, S.; Cho, E.; Chun, B.C. Effect of Climatic Factors on Hand, Foot, and Mouth Disease in South Korea, 2010–2013. PLoS ONE 2016, 11, e0157500. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Lai, Y.; Du, Z.; Zhang, W.; Feng, C.; Li, R.; Hao, Y. Spatiotemporal Distribution of Hand, Foot, and Mouth Disease in Guangdong Province, China and Potential Predictors, 2009–2012. Int. J. Environ. Res. Public Health 2019, 16, 1191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, P.; Zhao, H.; You, F.; Zhou, H.; Goggins, W.B. Seasonal modeling of hand, foot, and mouth disease as a function of meteorological variations in Chongqing, China. Int. J. Biometeorol. 2017, 61, 1411–1419. [Google Scholar] [CrossRef]
- Wong, S.; Yip, C.; Lau, S.; Yuen, K. Human enterovirus 71 and hand, foot and mouth disease. Epidemiol. Infect. 2010, 138, 1071–1089. [Google Scholar] [CrossRef] [Green Version]
- Onozuka, D.; Hashizume, M. The influence of temperature and humidity on the incidence of hand, foot, and mouth disease in Japan. Sci. Total Environ. 2011, 410–411, 119–125. [Google Scholar] [CrossRef]
- Yu, G.; Li, Y.; Cai, J.; Yu, D.; Tang, J.; Zhai, W.; Wei, Y.; Chen, S.; Chen, Q.; Qin, J. Short-term effects of meteorological factors and air pollution on childhood hand-foot-mouth disease in Guilin, China. Sci. Total Environ. 2019, 646, 460–470. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Zhou, M.; Yang, Y.; You, E.; Wu, J.; Zhang, W.; Jin, J.; Huang, F. Short-term effects of extreme meteorological factors on childhood hand, foot, and mouth disease reinfection in Hefei, China: A distributed lag non-linear analysis. Sci. Total Environ. 2019, 653, 839–848. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.; Wei, L.; Duan, Y.; Li, H.; Liao, Y.; Lv, Q.; Zhu, F.; Wang, Z.; Lu, W.; Yin, P.; et al. Short-Term Effects of Meteorological Factors and Air Pollutants on Hand, Foot and Mouth Disease among Children in Shenzhen, China, 2009–2017. Int. J. Environ. Res. Public Health 2019, 16, 3639. [Google Scholar] [CrossRef] [Green Version]
- Cheng, J.; Wu, J.; Xu, Z.; Zhu, R.; Wang, X.; Li, K.; Wen, L.; Yang, H.; Su, H. Associations between extreme precipitation and childhood hand, foot and mouth disease in urban and rural areas in Hefei, China. Sci. Total Environ. 2014, 497–498, 484–490. [Google Scholar] [CrossRef]
- Guzman Herrador, B.R.; de Blasio, B.F.; MacDonald, E.; Nichols, G.; Sudre, B.; Vold, L.; Semenza, J.C.; Nygård, K. Analytical studies assessing the association between extreme precipitation or temperature and drinking water-related waterborne infections: A review. Environ. Health 2015, 14, 29. [Google Scholar] [CrossRef] [Green Version]
- Qi, H.; Chen, Y.; Xu, D.; Su, H.; Zhan, L.; Xu, Z.; Huang, Y.; He, Q.; Hu, Y.; Lynn, H.; et al. Impact of meteorological factors on the incidence of childhood hand, foot, and mouth disease (HFMD) analyzed by DLNMs-based time series approach. Infect. Dis. Poverty 2018, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Ma, E.; Lam, T.; Wong, C.; Chuang, S.K. Is hand, foot and mouth disease associated with meteorological parameters? Epidemiol. Infect. 2010, 138, 1779–1788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escombe, A.R.; Oeser, C.C.; Gilman, R.H.; Navincopa, M.; Ticona, E.; Pan, W.; Martínez, C.; Chacaltana, J.; Rodríguez, R.; Moore, D.A.; et al. Natural ventilation for the prevention of airborne contagion. PLoS Med. 2007, 4, e68. [Google Scholar] [CrossRef] [Green Version]
- Jiao, K.; Hu, W.; Ren, C.; Xu, Z.; Ma, W. Impacts of tropical cyclones and accompanying precipitation and wind velocity on childhood hand, foot and mouth disease in Guangdong Province, China. Environ Res. 2019, 173, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Yang, Z.; Liu, X.; Kang, Y.; Wang, M. Hand-foot-and-mouth disease epidemiological status and relationship with meteorological variables in Guangzhou, southern China, 2008-2012. Rev. Inst. Med. Trop. Sao Paulo 2014, 56, 533–539. [Google Scholar] [CrossRef]
- Maes, M.; De Meyer, F. Relationships of climatic data to immune and hematologic variables in normal human. Neuro Endocrinol. Lett. 2000, 21, 127–136. [Google Scholar] [PubMed]
- Song, C.; Shi, X.; Bo, Y.; Wang, J.; Wang, Y.; Huang, D. Exploring spatiotemporal nonstationary effects of climate factors on hand, foot, and mouth disease using Bayesian Spatiotemporally Varying Coefficients (STVC) model in Sichuan, China. Sci. Total. Environ. 2019, 648, 550–560. [Google Scholar] [CrossRef] [PubMed]
- Hong, Z.; Hao, H.; Li, C.; Du, W.; Wei, L.; Wang, H. Exploration of potential risks of Hand, Foot, and Mouth Disease in Inner Mongolia Autonomous Region, China Using Geographically Weighted Regression Model. Sci. Rep. 2018, 8, 17707. [Google Scholar] [CrossRef]
- Dong, W.; Li, X.; Yang, P.; Liao, H.; Wang, X.; Wang, Q. The Effects of Weather Factors on Hand, Foot and Mouth Disease in Beijing. Sci. Rep. 2016, 6, 19247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, Z.; Li, R. The contributions of socioeconomic indicators to global PM2.5 based on the hybrid method of spatial econometric model and geographical and temporal weighted regression. Sci. Total Environ. 2020, 703, 135481. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
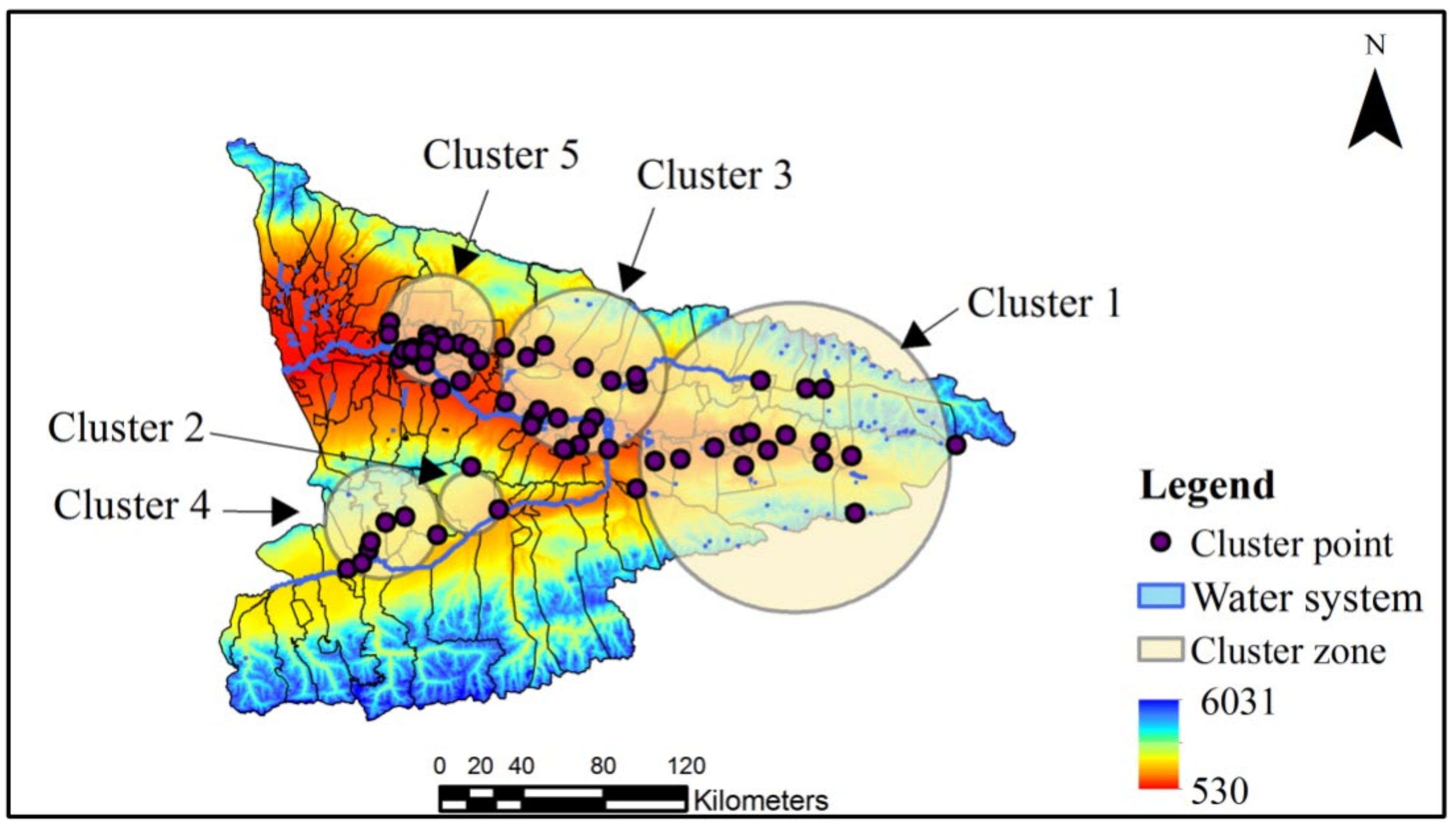
| No. | Coordinates | Locations | Radius 1 | Time | No. of Cases | No. Expect | LLR 2 |
|---|---|---|---|---|---|---|---|
| 1 | (43.423871 N, 83.521495 E) | Alemale Town, Tuergen Town, Areletuobie Town, Xinyuan Town, Biesituobie Town, Wugong Town, 71 XPCC, Zeketai Town, Kaisu Town, Breeding Bee Farm, Talede Town, 72XPCC, Xiaoerbulake Town, Wulasitai Town, Nalati Town, Musi Town, Kuerdening Town, Kalabula Town | 75.49 | April 2013–June 2013 | 163 | 33.59 | 129.80 |
| 2 | (43.205440 N, 81.665532 E) | Qilewuzike Town, Tekesi Town | 15.18 | February 2016–April 2016 | 140 | 27 | 53.32 |
| 3 | (43.999270 N, 81.480720 E) | Tulufanyuzi Town, Panjing Town, Sadikeyuzi Town, Kalayageqi Town, agricultural center, Kaerdun Town, Dadatumu Town, Alanmubage subdistrict, Tashikeruike Town, Jiefang subdistrict, Qiongkeruike subdistrict, Doulaitibage subdistrict, Tuogelake subdistrict, Dunmaili subdistrict, Quluhai, Town, 70 XPCC, Sabuyi subdistrict, Yuqunweng Hui Town, Kazanqi subdistrict, economic cooperation zone, Yili dairy farm, Hanbin Town, Awuliya Town, Bayandai Town, Kebokeyu Town, Yilihe subdistrict, Miquan Hui Town, Arewusitang Town, Youth farm, Yingyeer Town, Kuohongqi Town | 26.90 | May 2018–October 2018 | 1048 | 798 | 46.91 |
| 4 | (43.157293 N, 81.130975 E) | 77 XPCC, Hongnahai Town, Zhaosu Town, Ambanbagh Breeding farm, Wuzunbulake farm, Akedala Town | 27.77 | August 2018–September 2018 | 44 | 11 | 28 |
| 5 | (43.808751 N, 82.356540 E) | Keling Town, Jiahawulasi Town, Wuzan Town, Nileke Town, Kalatuobie Town, Subutai Town, Hujier Town, Kolkhoot Haor Mongolian Town, Mazha Town, Agaersen Town, Kosh Agash sheep farm, cow farm, Kashi Town, 73 XPCC, Aketubieke Town, Gongliu Town, Liangfan field, Dunmazha Town, Samuyuzi Town, Hudiyuzi Town | 40.27 | August 2013–September 2013 | 19 | 3.75 | 15 |
| Independent Variable | MCP | MAAP | MARH | MAT | MAWS |
|---|---|---|---|---|---|
| VIF | 1.559 | 1.366 | 6.407 | 5.712 | 1.851 |
| Tolerance | 0.626 | 0.732 | 0.256 | 0.375 | 0.540 |
| Model | R2 | AICC | RSS |
|---|---|---|---|
| OLS | 0.27 | 618.85 | 1104.03 |
| GWR | 0.28 | 622.91 | 1102.77 |
| GTWR | 0.52 | 610.99 | 736.19 |
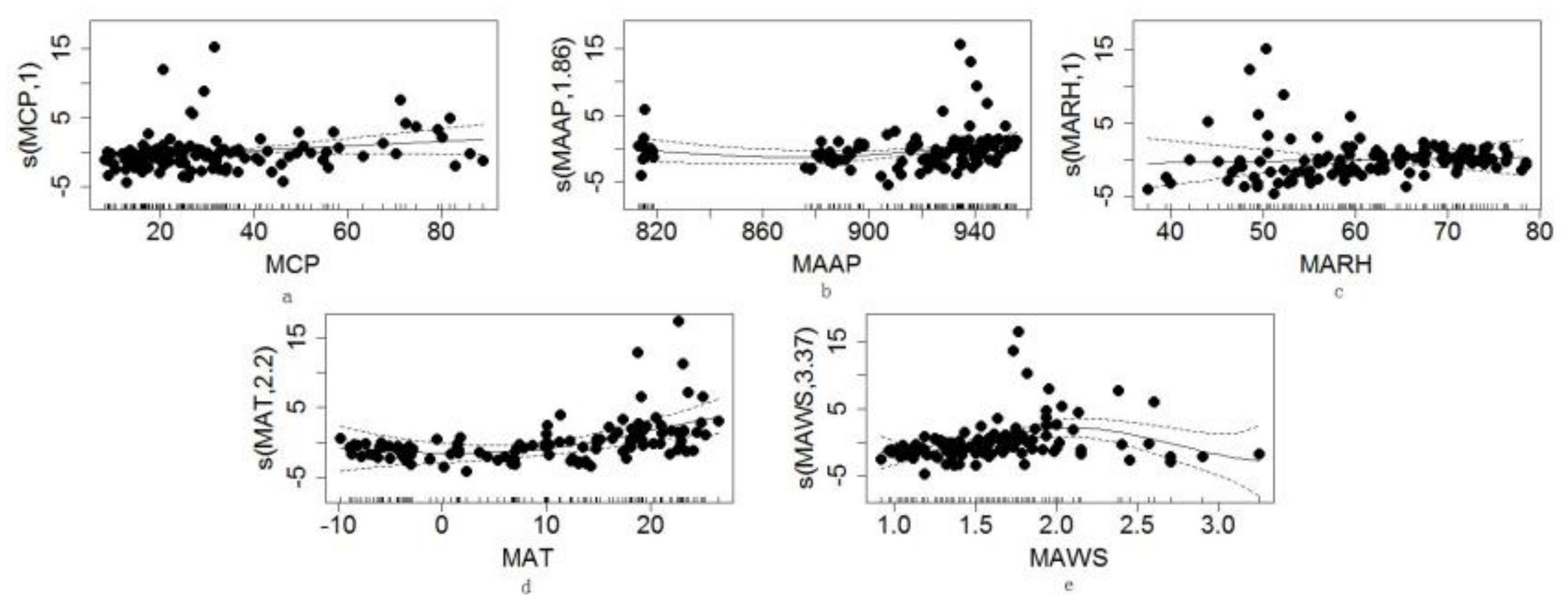
| Independent Variable | Edf 1 | Ref.df 2 | F 3 | p-Value 4 |
|---|---|---|---|---|
| MCP | 1.00 | 1.000 | 6.169 | 0.014507 |
| MAAP | 1.860 | 2.083 | 3.208 | 0.042133 |
| MARH | 1.000 | 1.000 | 0.181 | 0.671396 |
| MAT | 2.049 | 2.310 | 7.763 | 0.000575 |
| MAWS | 1.936 | 1.996 | 6.317 | 0.003371 |
| Explanatory Variables | F | p-Value |
|---|---|---|
| MCP | 4.150 | 0.004 |
| MAAP | 4.286 | 0.004 |
| MARH | 3.995 | 0.005 |
| MAT | 9.934 | 0.000 |
| MAWS | 7.008 | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yi, S.; Wang, H.; Yang, S.; Xie, L.; Gao, Y.; Ma, C. Spatial and Temporal Characteristics of Hand-Foot-and-Mouth Disease and Its Response to Climate Factors in the Ili River Valley Region of China. Int. J. Environ. Res. Public Health 2021, 18, 1954. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041954
Yi S, Wang H, Yang S, Xie L, Gao Y, Ma C. Spatial and Temporal Characteristics of Hand-Foot-and-Mouth Disease and Its Response to Climate Factors in the Ili River Valley Region of China. International Journal of Environmental Research and Public Health. 2021; 18(4):1954. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041954
Chicago/Turabian StyleYi, Suyan, Hongwei Wang, Shengtian Yang, Ling Xie, Yibo Gao, and Chen Ma. 2021. "Spatial and Temporal Characteristics of Hand-Foot-and-Mouth Disease and Its Response to Climate Factors in the Ili River Valley Region of China" International Journal of Environmental Research and Public Health 18, no. 4: 1954. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041954