Prevalence and Risk Factors for Post-Traumatic Stress in Hospitalized and Non-Hospitalized COVID-19 Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Population
2.1.1. Survey of Hospitalized Subjects
2.1.2. Survey of Non-Hospitalized Subjects
2.1.3. Ethical Considerations
2.2. Data Collection and Assessments
2.2.1. Assessment of PTSD
2.2.2. Assessment of Comorbidity and COVID-19 Symptoms
2.3. Statistical Analyses
3. Results
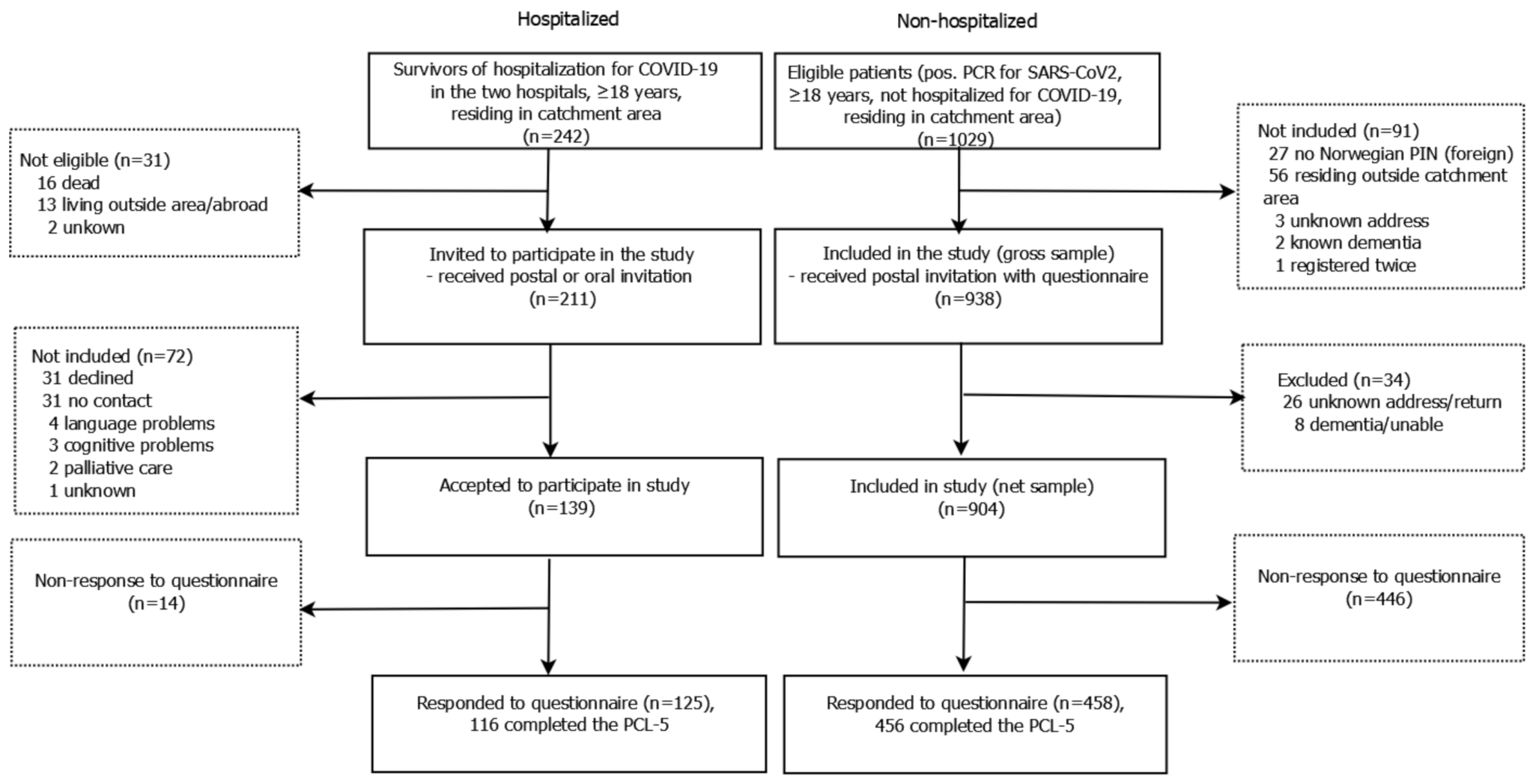
3.1. Study Population
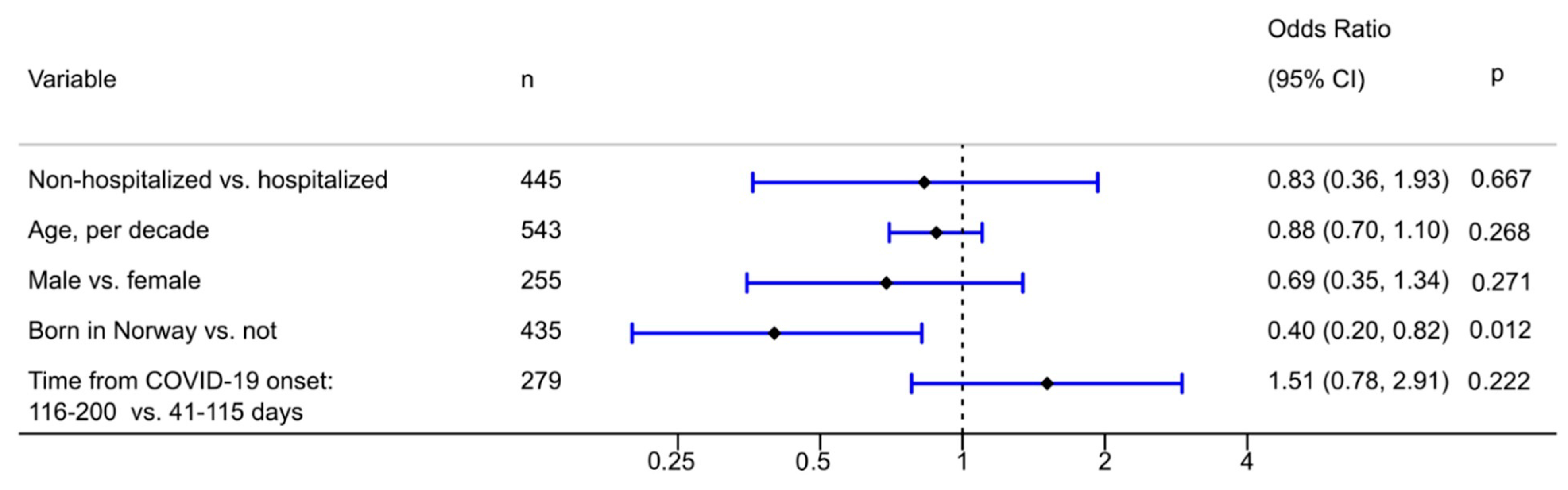
3.2. Prevalence and Determinants of Symptom-Defined PTSD
3.3. Determinants of the PTSD Symptom Scores
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 17 December 2020).
- Nystad, W.; Hjellvik, V.; Larsen, I.K.; Ariansen, I.; Helland, E.; Johansen, K.I.; Gulbrandsen, J.; Gulseth, H.L.; Eide, H.N.; Haberg, S.E.; et al. Underlying conditions in adults with COVID-19. Tidsskr. Nor. Legeforening 2020, 140. [Google Scholar] [CrossRef]
- Asmundson, G.J.G.; Taylor, S. Coronaphobia: Fear and the 2019-nCoV outbreak. J. Anxiety Disord. 2020, 70, 102196. [Google Scholar] [CrossRef] [PubMed]
- Parker, A.M.; Sricharoenchai, T.; Raparla, S.; Schneck, K.W.; Bienvenu, O.J.; Needham, D.M. Posttraumatic stress disorder in critical illness survivors: A metaanalysis. Crit. Care Med. 2015, 43, 1121–1129. [Google Scholar] [CrossRef]
- Badenoch, J.; Cross, B.; Hafeez, D.; Song, J.; Watson, C.; Butler, M.; Nicholson, T.R.; Rooney, A.G. Post-traumatic symptoms after COVID-19 may (or may not) reflect disease severity. Psychol. Med. 2020. [Google Scholar] [CrossRef]
- Liu, D.; Baumeister, R.F.; Veilleux, J.C.; Chen, C.; Liu, W.; Yue, Y.; Zhang, S. Risk factors associated with mental illness in hospital discharged patients infected with COVID-19 in Wuhan, China. Psychiatry Res. 2020, 292, 113297. [Google Scholar] [CrossRef]
- De Lorenzo, R.; Conte, C.; Lanzani, C.; Benedetti, F.; Roveri, L.; Mazza, M.G.; Brioni, E.; Giacalone, G.; Canti, V.; Sofia, V.; et al. Residual clinical damage after COVID-19: A retrospective and prospective observational cohort study. PLoS ONE 2020, 15, e0239570. [Google Scholar] [CrossRef]
- Chang, M.C.; Park, D. Incidence of Post-Traumatic Stress Disorder After Coronavirus Disease. Healthcare 2020, 8, 373. [Google Scholar] [CrossRef]
- Lerum, T.V.; Aalokken, T.M.; Bronstad, E.; Aarli, B.; Ikdahl, E.; Lund, K.M.A.; Durheim, M.T.; Rodriguez, J.R.; Meltzer, C.; Tonby, K.; et al. Dyspnoea, lung function and CT findings three months after hospital admission for COVID-19. Eur. Respir. J. 2020. [Google Scholar] [CrossRef]
- Stavem, K.; Ghanima, W.; Olsen, M.K.; Gilboe, H.M.; Einvik, G. Persistent symptoms 1.5-6 months after COVID-19 in non-hospitalised subjects: A population-based cohort study. Thorax 2020. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- Weathers, F.W.; Litz, B.T.; Keane, T.M.; Palmieri, P.A.; Marx, B.P.; Schnurr, P.P. The PTSD Checklist for DSM-5 (PCL-5)—Standard. Available online: www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp (accessed on 18 December 2020).
- Using the PTSD Checklist for DSM-5. Available online: https://www.ptsd.va.gov/professional/assessment/documents/using-PCL5.pdf (accessed on 20 February 2021).
- Bonsaksen, T.; Heir, T.; Schou-Bredal, I.; Ekeberg, O.; Skogstad, L.; Grimholt, T.K. Post-Traumatic Stress Disorder and Associated Factors during the Early Stage of the COVID-19 Pandemic in Norway. Int. J. Environ. Res. Public Health 2020, 17, 9210. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.N.; Chang, L.C.; Sangha, O.; Fossel, A.H.; Bates, D.W. Can comorbidity be measured by questionnaire rather than medical record review? Med. Care 1996, 34, 73–84. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic. Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- WHO/ISARIC. COVID-19 Case Record Form. Global COVID-19 Clinical Platform Novel Coronavirus (COVID-19)—Rapid Version. Available online: https://media.tghn.org/medialibrary/2020/09/ISARIC_COVID-19_RAPID_CRF_25Aug20.pdf (accessed on 20 February 2021).
- Poyraz, B.C.; Poyraz, C.A.; Olgun, Y.; Gurel, O.; Alkan, S.; Ozdemir, Y.E.; Balkan, I.I.; Karaali, R. Psychiatric morbidity and protracted symptoms after COVID-19. Psychiatry Res. 2021, 295, 113604. [Google Scholar] [CrossRef]
- Cai, X.; Hu, X.; Ekumi, I.O.; Wang, J.; An, Y.; Li, Z.; Yuan, B. Psychological Distress and Its Correlates Among COVID-19 Survivors During Early Convalescence Across Age Groups. Am. J. Geriatr. Psychiatry 2020, 28, 1030–1039. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Zhu, Y.; Xu, F.; Xi, J.; Xu, G. Factors associated with mental health outcomes among patients with COVID-19 treated in the Fangcang shelter hospital in China. Asia Pac. Psychiatry 2020, e12443. [Google Scholar] [CrossRef]
- Horn, M.; Wathelet, M.; Fovet, T.; Amad, A.; Vuotto, F.; Faure, K.; Astier, T.; Noel, H.; Duhem, S.; Vaiva, G.; et al. Is COVID-19 Associated With Posttraumatic Stress Disorder? J. Clin. Psychiatry 2020, 82. [Google Scholar] [CrossRef]
- Bo, H.X.; Li, W.; Yang, Y.; Wang, Y.; Zhang, Q.; Cheung, T.; Wu, X.; Xiang, Y.T. Posttraumatic stress symptoms and attitude toward crisis mental health services among clinically stable patients with COVID-19 in China. Psychol. Med. 2020. [Google Scholar] [CrossRef] [Green Version]
- Maekelae, M.J.; Reggev, N.; Dutra, N.; Tamayo, R.M.; Silva-Sobrinho, R.A.; Klevjer, K.; Pfuhl, G. Perceived efficacy of COVID-19 restrictions, reactions and their impact on mental health during the early phase of the outbreak in six countries. R. Soc. Open Sci. 2020, 7, 200644. [Google Scholar] [CrossRef] [PubMed]
- Berntsen, D.; Rubin, D.C. The centrality of event scale: A measure of integrating a trauma into one’s identity and its relation to post-traumatic stress disorder symptoms. Behav. Res. Ther. 2006, 44, 219–231. [Google Scholar] [CrossRef] [Green Version]
- Blix, I.; Birkeland, M.S.; Solberg, Ø.; Hansen, M.B.; Heir, T. The Launching and Ensnaring Effects of Construing a Traumatic Event as Central to One’s Identity and Life Story. Appl. Cogn. Psychol. 2016, 30, 526–531. [Google Scholar] [CrossRef]
- Heir, T.; Piatigorsky, A.; Weisaeth, L. Longitudinal changes in recalled perceived life threat after a natural disaster. Br. J. Psychiatry 2009, 194, 510–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heir, T.; Blix, I.; Knatten, C.K. Thinking that one’s life was in danger: Perceived life threat in individuals directly or indirectly exposed to terror. Br. J. Psychiatry 2016, 209, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Heir, T.; Hussain, A.; Weisæth, L. Managing the after-effects of disaster trauma—The essentials of early intervention. Eur. Psychiatr. Rev. 2008, 1, 66–69. [Google Scholar]
- Bryant, R.A. Post-traumatic stress disorder: A state-of-the-art review of evidence and challenges. World Psychiatry 2019, 18, 259–269. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.M.; Wong, J.G.; McAlonan, G.M.; Cheung, V.; Cheung, C.; Sham, P.C.; Chu, C.M.; Wong, P.C.; Tsang, K.W.; Chua, S.E. Stress and psychological distress among SARS survivors 1 year after the outbreak. Can. J. Psychiatry 2007, 52, 233–240. [Google Scholar] [CrossRef] [Green Version]
- Tang, W.; Hu, T.; Hu, B.; Jin, C.; Wang, G.; Xie, C.; Chen, S.; Xu, J. Prevalence and correlates of PTSD and depressive symptoms one month after the outbreak of the COVID-19 epidemic in a sample of home-quarantined Chinese university students. J. Affect. Disord. 2020, 274, 1–7. [Google Scholar] [CrossRef]
- Liu, N.; Zhang, F.; Wei, C.; Jia, Y.; Shang, Z.; Sun, L.; Wu, L.; Sun, Z.; Zhou, Y.; Wang, Y.; et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: Gender differences matter. Psychiatry Res. 2020, 287, 112921. [Google Scholar] [CrossRef]
- Casagrande, M.; Favieri, F.; Tambelli, R.; Forte, G. The enemy who sealed the world: Effects quarantine due to the COVID-19 on sleep quality, anxiety, and psychological distress in the Italian population. Sleep Med. 2020, 75, 12–20. [Google Scholar] [CrossRef]
- Krogstad, H.; Loge, J.H.; Grotmol, K.S.; Kaasa, S.; Kiserud, C.E.; Salvesen, O.; Hjermstad, M.J. Symptoms in the general Norwegian adult population—Prevalence and associated factors. BMC Public Health 2020, 20, 988. [Google Scholar] [CrossRef] [PubMed]
- Galea, S.; Tracy, M. Participation rates in epidemiologic studies. Ann. Epidemiol. 2007, 17, 643–653. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Hospitalized (n = 125) | Non-hospitalized (n = 458) | p | |||
|---|---|---|---|---|---|
| n | n | ||||
| Age, date of response, mean (SD) | 125 | 57.7 (14.2) | 458 | 49.6 (15.3) | <0.001 |
| Sex, males | 72 | (58) | 202 | (44) | 0.007 |
| Highest attained education (n = 123/458) | <0.001 | ||||
| Primary school (<11 years) | 33 | (27) | 41 | (9) | |
| Secondary school (11–13 years) | 43 | (35) | 174 | (38) | |
| University (>13 years) | 47 | (38) | 243 | (53) | |
| Marital status (n = 112/457) | |||||
| Married/cohabiting | 77 | (69) | 336 | (74) | 0.31 |
| Born in Norway (n = 112/454) | 70 | (63) | 382 | (84) | <0.001 |
| Smoking status (n = 111/453) | |||||
| Previous/current smoker | 47 | (42) | 155 | (34) | 0.11 |
| Place of contraction (n = 125/456) | 0.001 | ||||
| Travel abroad | 40 | (32) | 117 | (26) | |
| In Norway, known contact | 30 | (24) | 194 | (43) | |
| In Norway, unknown contact | 55 | (44) | 145 | (32) | |
| Time from COVID-19 onset, days, mean (SD) | 119 | 112 (30) | 452 | 118 (27) | |
| Time from COVID-19 onset, days (n = 119/452) | 0.006 | ||||
| 41–115 | 72 | (60) | 209 | (46) | |
| 116–200 | 47 | (40) | 243 | (54) | |
| Comorbidity | |||||
| Asthma | 25 | (20) | 52 | (11) | 0.016 |
| Chronic obstructive pulmonary disease | 4 | (3) | 5 | (1) | 0.10 |
| Other chronic lung | (0) | 8 | (2) | 0.21 | |
| Lymphoma | (0) | (0) | - | ||
| Other cancer | 4 | (3) | 6 | (1) | 0.23 |
| Gastrointestinal | 5 | (4) | 32 | (7) | 0.30 |
| Heart problems | 13 | (10) | 27 | (6) | 0.11 |
| Hypertension | 35 | (28) | 86 | (19) | 0.034 |
| Circulatory | 1 | (1) | 8 | (2) | 0.69 |
| Chronic kidney disease | 2 | (2) | 5 | (1) | 0.65 |
| Liver disease | 0 | (0) | 1 | (0) | 1 |
| Neuromuscular | 6 | (5) | 3 | (1) | 0.004 |
| Stroke | 4 | (3) | 8 | (2) | 0.30 |
| Rheumatic | 1 | (1) | 23 | (5) | 0.039 |
| Venous thromboembolism | 5 | (4) | 11 | (2) | 0.35 |
| Diabetes | 15 | (12) | 16 | (3) | 0.001 |
| Number of 16 comorbidities | 0.001 | ||||
| 0 | 52 | (42) | 269 | (59) | |
| 1 | 42 | (34) | 124 | (27) | |
| ≥2 | 31 | (25) | 65 | (14) | |
| Depression (n = 458) * | N/A | 30 | (7) | - | |
| Symptoms during acute COVID-19 | |||||
| Dyspnea (n = 125/449) | 88 | (70) | 260 | (58) | 0.013 |
| Confusion (n = 456) * | N/A | 64 | (14) | - | |
| Fever (n = 125/453) | 105 | (84) | 331 | (73) | 0.013 |
| Hospitalized | Non-Hospitalized | p | |||
|---|---|---|---|---|---|
| n | n | ||||
| PTSD (DSM-5 scoring), number (%) | 116 | 11 (9.5) | 455 | 32 (7.0) | 0.80 |
| PCL-5 total score (0–80 range), mean (SD) | 116 | 12.4 (14.5) | 456 | 9.7 (11.3) | 0.042 |
| All | Hospitalized | Non-Hospitalized | ||||||
|---|---|---|---|---|---|---|---|---|
| Model | (1) | (2) | (3) | (4) | ||||
| Coef. | 95% CI | Coef. | 95% CI | Coef. | 95% CI | Coef. | 95% CI | |
| Cohort | ||||||||
| Hospitalized | 0 | |||||||
| Non-hospitalized | −1.05 | [−4.38,2.28] | ||||||
| Age, per decade | −0.31 | [−0.98,0.36] | −1.87 | [−4.14,0.40] | 0.01 | [−0.72,0.75] | 0.01 | [−0.70,0.73] |
| Sex | ||||||||
| Female | 0 | 0 | 0 | 0 | ||||
| Male | −3.01 ** | [−5.01,−1.01] | −3.47 | [−10.24,3.30] | −3.25 ** | [−5.38,−1.13] | −2.69 ** | [−4.67,−0.71] |
| Born in Norway | ||||||||
| No | 0 | 0 | 0 | 0 | ||||
| Yes | −6.82 *** | [−9.82,−3.82] | −5.64 | [−12.97,1.68] | −7.17 *** | [−10.45,−3.89] | −5.14 ** | [−8.59,−1.68] |
| Highest attained education | ||||||||
| Primary school (<11 years) | 0 | 0 | 0 | 0 | ||||
| Secondary school (11–13 years) | 2.14 | [−1.37,5.65] | 2.57 | [−4.90,10.03] | 0.92 | [−3.33,5.16] | 1.69 | [−1.97,5.35] |
| University (>13 years) | 1.34 | [−2.28,4.95] | 5.75 | [−2.41,13.91] | −0.58 | [−4.74,3.58] | 0.30 | [−3.15,3.75] |
| Marital status | ||||||||
| Single/divorced/widowed | 0 | 0 | 0 | 0 | ||||
| Married/cohabiting | −1.27 | [−3.40,0.85] | 3.44 | [−2.71,9.58] | −2.86 * | [−5.15,−0.57] | −1.78 | [−4.03,0.47] |
| No. of 16 comorbidities | ||||||||
| 0 | 0 | 0 | 0 | 0 | ||||
| 1 | 0.16 | [−2.12,2.43] | 1.17 | [−6.54,8.89] | −0.10 | [−2.41,2.20] | −0.99 | [−3.05,1.07] |
| ≥2 | 2.60 | [−0.42,5.62] | 3.76 | [−3.60,11.12] | 2.62 | [−0.78,6.02] | 1.87 | [−1.66,5.41] |
| Dyspnea during COVID-19 | ||||||||
| No | 0 | 0 | 0 | |||||
| Yes | 3.68 *** | [1.80,5.57] | 2.73 | [−2.51,7.97] | 3.66 *** | [1.58,5.73] | ||
| Fever during COVID-19 | ||||||||
| No | 0 | 0 | 0 | |||||
| Yes | 1.80 | [−0.26,3.86] | 0.98 | [−7.46,9.41] | 1.70 | [−0.39,3.78] | ||
| Time since COVID-19 onset, days | ||||||||
| 41–115 | 0 | 0 | 0 | 0 | ||||
| 116–200 | 0.63 | [−1.40,2.66] | 2.33 | [−3.51,8.17] | 0.59 | [−1.49,2.68] | 0.16 | [−1.78,2.11] |
| History of depression1 | ||||||||
| No | 0 | |||||||
| Yes | 4.58 * | [0.19,8.97] | ||||||
| No. of 23 symptoms during COVID-191 | ||||||||
| 0–5 | 0 | |||||||
| 6–9 | 0.59 | [−1.74,2.93] | ||||||
| 10–23 | 5.59 *** | [2.94,8.24] | ||||||
| Confusion during COVID-191 | ||||||||
| No | 0 | |||||||
| Yes | 6.80 *** | [3.12,10.49] | ||||||
| n | 531 | 98 | 433 | 444 | ||||
| R-squared | 0.11 | 0.13 | 0.13 | 0.24 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Einvik, G.; Dammen, T.; Ghanima, W.; Heir, T.; Stavem, K. Prevalence and Risk Factors for Post-Traumatic Stress in Hospitalized and Non-Hospitalized COVID-19 Patients. Int. J. Environ. Res. Public Health 2021, 18, 2079. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18042079
Einvik G, Dammen T, Ghanima W, Heir T, Stavem K. Prevalence and Risk Factors for Post-Traumatic Stress in Hospitalized and Non-Hospitalized COVID-19 Patients. International Journal of Environmental Research and Public Health. 2021; 18(4):2079. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18042079
Chicago/Turabian StyleEinvik, Gunnar, Toril Dammen, Waleed Ghanima, Trond Heir, and Knut Stavem. 2021. "Prevalence and Risk Factors for Post-Traumatic Stress in Hospitalized and Non-Hospitalized COVID-19 Patients" International Journal of Environmental Research and Public Health 18, no. 4: 2079. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18042079