
Assessing the Psychological Impacts of COVID-19 in Undergraduate Medical Students



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Sample
2.2. Rating Instruments
2.2.1. Demographic Characteristics
2.2.2. Perceived Stress Scale (PSS-4)
2.2.3. Generalized Anxiety Disorder Scale (GAD-7)
2.2.4. Unique Stressors during the COVID-19 Pandemic
2.2.5. Perceptions of Stress and Anxiety
2.3. Data Analysis
3. Results
3.1. Sample Characteristics
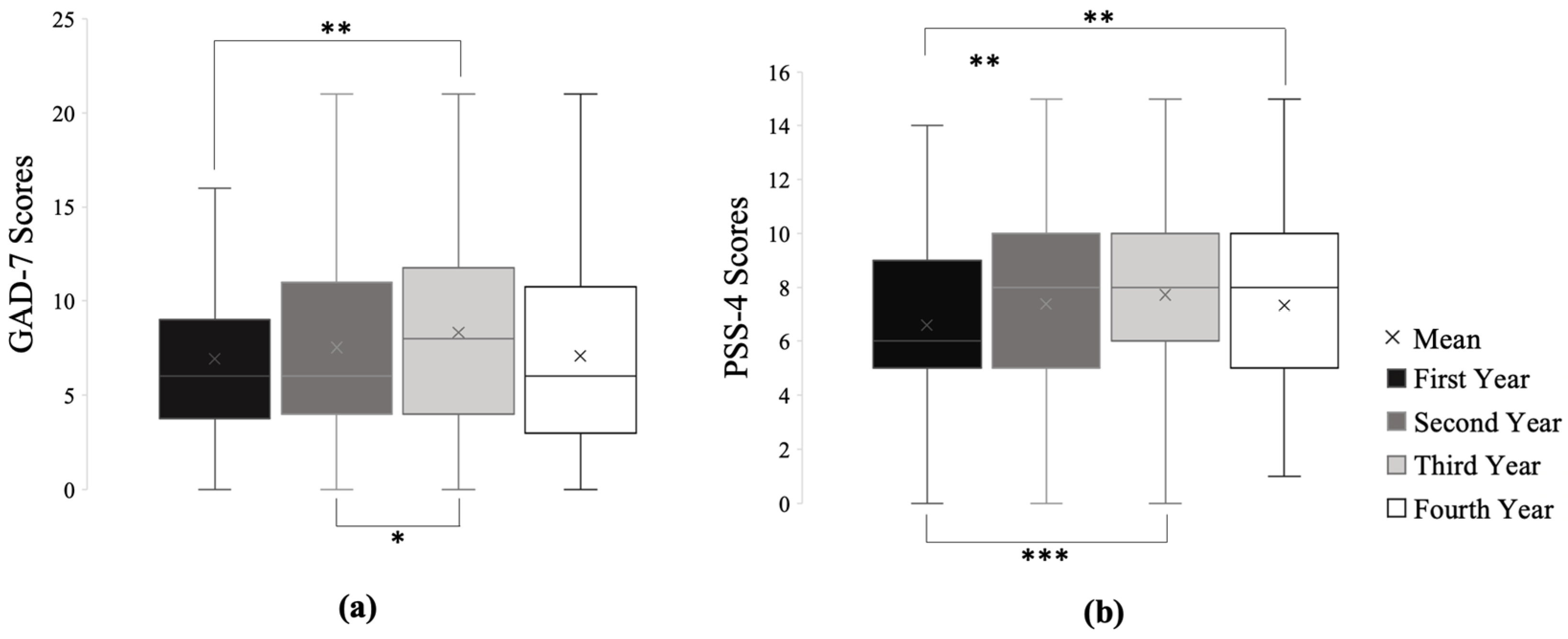
3.2. Anxiety in Undergraduate Medical Students
3.3. Stress in Undergraduate Medical Students
3.4. Predictors of Stress and Anxiety
3.5. Effects of Preexisting Mental Health on Stress and Anxiety
3.6. Perceptions of Stress and Anxiety
4. Discussion
4.1. Predictors of Anxiety and Stress
4.2. Unique Stressors to Each Class
4.3. The Effect of Preexisting Mental Health Conditions on Anxiety and Stress Levels during the COVID-19 Pandemic
4.4. Study Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miller, D.G.; Pierson, L.; Doernberg, S. The Role of Medical Students during the COVID-19 Pandemic. Ann. Intern. Med. 2020, 173, 145–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, S. Medical Student Education in the Time of COVID-19. JAMA 2020, 323, 2131. [Google Scholar] [CrossRef]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Esterwood, E.; Saeed, S.A. Past Epidemics, Natural Disasters, COVID19, and Mental Health: Learning from History as we Deal with the Present and Prepare for the Future. Psychiatr. Q. 2020, 91, 1121–1133. [Google Scholar] [CrossRef] [PubMed]
- Compton, M.T.; Carrera, J.; Frank, E. Stress and Depressive Symptoms/Dysphoria Among US Medical Students. J. Nerv. Ment. Dis. 2008, 196, 891–897. [Google Scholar] [CrossRef]
- Dyrbye, L.N.; Thomas, M.R.; Shanafelt, T.D. Systematic Review of Depression, Anxiety, and Other Indicators of Psychological Distress among U.S. and Canadian Medical Students. Acad. Med. 2006, 81, 354–373. [Google Scholar] [CrossRef]
- Rotenstein, L.S.; Ramos, M.A.; Torre, M.; Segal, J.B.; Peluso, M.J.; Guille, C.; Sen, S.; Mata, D.A. Prevalence of Depression, Depressive Symptoms, and Suicidal Ideation Among Medical Students. JAMA 2016, 316, 2214–2236. [Google Scholar] [CrossRef] [Green Version]
- Lasheras, I.; Gracia-García, P.; Lipnicki, D.M.; Bueno-Notivol, J.; López-Antón, R.; De La Cámara, C.; Lobo, A.; Santabárbara, J. Prevalence of Anxiety in Medical Students during the COVID-19 Pandemic: A Rapid Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 6603. [Google Scholar] [CrossRef]
- Chandavarkar, U.; Azzam, A.; Mathews, C.A. Anxiety symptoms and perceived performance in medical students. Depress. Anxiety 2007, 24, 103–111. [Google Scholar] [CrossRef]
- Harcourt, J.; Tamin, A.; Lu, X.; Kamili, S.; Sakthivel, S.K.; Murray, J.; Queen, K.; Tao, Y.; Paden, C.R.; Zhang, J.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 from Patient with Coronavirus Disease, United States. Emerg. Infect. Dis. 2020, 26, 1266–1273. [Google Scholar] [CrossRef]
- Guidance on Medical Students’ Participation in Direct In-person Patient Contact Activities. 2020, pp. 1–6. Available online: https://www.aamc.org/system/files/2020-08/meded-August-14-Guidance-on-Medical-Students-on-Clinical-Rotations.pdf (accessed on 30 January 2021).
- Akers, A.; Blough, C.; Iyer, M.S. COVID-19 Implications on Clinical Clerkships and the Residency Application Process for Medical Students. Cureus 2020, 12, e7800. [Google Scholar] [CrossRef] [Green Version]
- Gabrielson, A.T.; Kohn, J.R.; Sparks, H.T.; Clifton, M.M.; Kohn, T.P. Proposed Changes to the 2021 Residency Application Process in the Wake of COVID-19. Acad. Med. 2020, 95. [Google Scholar] [CrossRef] [PubMed]
- Mortazavi, S.S.; Assari, S.; Alimohamadi, A.; Rafiee, M.; Shati, M. Fear, Loss, Social Isolation, and Incomplete Grief Due to COVID-19: A Recipe for a Psychiatric Pandemic. Basic Clin. Neurosci. J. 2020, 11, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Lopez, M.; Ungaro, R.F.; Baker, H.V.; Moldawer, L.L.; Morris, J.G. Loneliness: A Signature Mental Health Concern in the Era of COVID-19. Psychiatry Res. 2020, 290, 19–21. [Google Scholar]
- Mertens, G.; Gerritsen, L.; Duijndam, S.; Salemink, E.; Engelhard, I.M. Fear of the coronavirus (COVID-19): Predictors in an online study conducted in March 2020. J. Anxiety Disord. 2020, 74, 102258. [Google Scholar] [CrossRef]
- Mann, F.D.; Krueger, R.F.; Vohs, K.D. Personal economic anxiety in response to COVID-19. Pers. Individ. Differ. 2020, 167, 110233. [Google Scholar] [CrossRef]
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Zhang, C.; Boyle, C.; Smith, M.; Phillips, J.P. Fair Allocation of Scarce Medical Resources in the Time of Covid-19. N. Engl. J. Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef]
- Warttig, S.L.; Forshaw, M.J.; South, J.; White, A.K. New, normative, English-sample data for the Short Form Perceived Stress Scale (PSS-4). J. Health Psychol. 2012, 18, 1617–1628. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Jia, R.; Ayling, K.; Chalder, T.; Massey, A.; Broadbent, E.; Coupland, C.; Vedhara, K. Mental health in the UK during the COVID-19 pandemic: Cross-sectional analyses from a community cohort study. BMJ Open 2020, 10, e040620. [Google Scholar] [CrossRef]
- Li, D.C.Y.; Leung, L. Psychometric data on knowledge and fear of coronavirus disease 2019 and perceived stress among workers of filipino origin in Hong Kong. Data Brief 2020, 33, 106395. [Google Scholar] [CrossRef]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and Standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the General Population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief Measure for Assessing Generalized Anxiety Disorder. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.; Monahan, P.O.; Löwe, B. Anxiety Disorders in Primary Care: Prevalence, Impairment, Comorbidity, and Detection. Ann. Intern. Med. 2007, 146, 317–325. [Google Scholar] [CrossRef] [PubMed]
- American Osteopathic Association. Available online: https://osteopathic.org/about/aoa-statistics/#:~:text=Number%20of%20new%20DOs%20sets%20a%20record%20in%202019&text=Nearly%207%2C000%20new%20physicians%20graduated,of%20the%20American%20physician%20population (accessed on 30 January 2021).
- Association of American Medical Colleges. Available online: https://www.aamc.org/data-reports/students-residents/interactive-data/2020-facts-enrollment-graduates-and-md-phd-data (accessed on 30 January 2021).
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Quek, T.T.-C.; Tam, W.W.-S.; Tran, B.X.; Zhang, Z.; Ho, R.C.-M. The Global Prevalence of Anxiety Among Medical Students: A Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 2735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mousa, O.Y.; Dhamoon, M.S.; Lander, S.; Dhamoon, A.S. The MD Blues: Under-Recognized Depression and Anxiety in Medical Trainees. PLoS ONE 2016, 11, e0156554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tull, M.T.; Edmonds, K.A.; Scamaldo, K.M.; Richmond, J.R.; Rose, J.P.; Gratz, K.L. Psychological Outcomes Associated with Stay-at-Home Orders and the Perceived Impact of COVID-19 on Daily Life. Psychiatry Res. 2020, 289, 113098. [Google Scholar] [CrossRef]
- Rosal, M.C.; Ockene, I.S.; Ockene, J.K.; Barrett, S.V.; Ma, Y.; Hebert, J.R. A longitudinal study of studentsʼ depression at one medical school. Acad. Med. 1997, 72, 542–546. [Google Scholar] [CrossRef]
- Hatcher, W. A Failure of Political Communication Not a Failure of Bureaucracy: The Danger of Presidential Misinformation during the COVID-19 Pandemic. Am. Rev. Public Adm. 2020, 50, 614–620. [Google Scholar] [CrossRef]
- Painter, M.; Qiu, T. Political Beliefs affect Compliance with COVID-19 Social Distancing Orders. SSRN Electron. J. 2020, 103–119. [Google Scholar] [CrossRef]
- Kahane, L.H. Politicizing the Mask: Political, Economic and Demographic Factors Affecting Mask Wearing Behavior in the USA. East. Econ. J. 2021, 1–21. [Google Scholar] [CrossRef]
- American Medical Association. Available online: https://www.ama-assn.org/residents-students/usmle/delays-miscommunications-add-even-more-stress-usmle-step-exams (accessed on 30 January 2021).
- The Impact of COVID-19 on Mental, Neurological and Substance Use Services: Results of a Rapid Assessment. Available online: https://www.who.int/publications/i/item/978924012455 (accessed on 10 December 2020).
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, C.U.; Byrne, L.; Carr, S.; et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef]
- Hardeman, R.R.; Przedworski, J.M.; Burke, S.E.; Burgess, D.J.; Phelan, S.M.; Dovidio, J.F.; Nelson, D.; Rockwood, T.H.; Van Ryn, M. Mental Well-Being in First Year Medical Students: A Comparison by Race and Gender. J. Racial Ethn. Health Disparities 2015, 2, 403–413. [Google Scholar] [CrossRef]
- Dyrbye, L.N.; Thomas, M.R.; Power, D.V.; Durning, S.; Moutier, C.; Massie, F.S.; Harper, W.; Eacker, A.; Szydlo, D.W.; Sloan, J.A.; et al. Burnout and Serious Thoughts of Dropping Out of Medical School: A Multi-Institutional Study. Acad. Med. 2010, 85, 94–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Association of American Medical Colleges. Available online: https://www.aamc.org/media/38916/download (accessed on 4 March 2021).
- Dalsania, A.K.; Fastiggi, M.J.; Kahlam, A.; Shah, R.; Patel, K.; Shiau, S.; Rokicki, S.; Dallapiazza, M. The Relationship Between Social Determinants of Health and Racial Disparities in COVID-19 Mortality. J. Racial Ethn. Health Disparities 2021, 1–8. [Google Scholar] [CrossRef]
- Cho, H.; Li, W.; Cannon, J.; Lopez, R.; Song, C. (Chuck) Testing three explanations for stigmatization of people of Asian descent during COVID-19: Maladaptive coping, biased media use, or racial prejudice? Ethn. Health 2021, 26, 94–109. [Google Scholar] [CrossRef] [PubMed]
- American Psychological Association. Available online: https://www.apa.org/topics/anxiety (accessed on 4 March 2021).
- Haleem, A.; Javaid, M.; Vaishya, R. Effects of COVID-19 pandemic in daily life. Curr. Med. Res. Pr. 2020, 10, 78–79. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | 852 (100%) |
|---|---|
| Year in School | |
| First Year | 210 (24.65) |
| Second Year | 286 (33.57) |
| Third Year | 180 (21.13) |
| Fourth Year | 176 (20.66) |
| Race | |
| Black/African American | 42 (4.93) |
| American Indian or Alaska Native | 1 (0.12) |
| Asian | 119 (13.97) |
| Hispanic, Latino, or of Spanish Origin | 40 (4.69) |
| Native Hawaiian or Other Pacific Islander | 1 (0.12) |
| White | 576 (67.61) |
| Multiracial | 60 (7.04) |
| Others | 13 (1.53) |
| Anxiety Level | First Year | Second Year | Third Year | Fourth Year | Overall |
|---|---|---|---|---|---|
| Normal | 70 (33.33) | 93 (32.52) | 55 (30.56) | 71 (40.34) | 289 (33.92) |
| Mild | 90 (42.86) | 101 (35.31) | 55 (30.56) | 52 (29.55) | 298 (34.98) |
| Moderate | 31 (14.76) | 57 (19.93) | 43 (23.89) | 33 (18.75) | 164 (19.25) |
| Severe | 19 (9.05) | 35 (12.24) | 27 (15.00) | 20 (11.36) | 101 (11.85) |
| Stressors | First Year | Second Year | Third Year | Fourth Year | Overall |
|---|---|---|---|---|---|
| Academic | |||||
| Quality of Clinical Educational Experiences | 5.2 ± 3.2 | 5.7 ± 3.0 | 6.3 ± 2.7 | 6.1 ± 2.6 | 5.8 ± 2.9 |
| Remote Learning | 5.8 ± 2.9 | 6.0 ± 2.7 | 5.4 ± 2.7 | 5.1 ± 2.7 | 5.6 ± 2.8 |
| Delay and Availability of Standardized Exams | 2.8 ± 3.1 | 3.6 ± 3.5 | 7.4 ± 3.2 | 7.2 ± 2.9 | 4.9 ± 3.8 |
| Impact on Rotations and Residency | 2.3 ± 3.1 | 2.5 ± 3.3 | 5.0 ± 3.6 | 7.8 ± 2.9 | 4.1 ± 3.9 |
| Health | |||||
| Becoming Ill | 6.2 ± 2.7 | 6.4 ± 2.5 | 6.5 ± 2.6 | 6.3 ± 2.6 | 6.3 ± 2.6 |
| Death and Disability | 3.6 ± 3.0 | 3.9 ± 3.1 | 4.1 ± 2.9 | 3.8 ± 3.0 | 3.9 ± 3.0 |
| Personal Protective Equipment Availability | 4.3 ± 2.7 | 4.4 ± 2.8 | 4.9 ± 2.6 | 4.9 ± 2.9 | 4.6 ± 2.7 |
| Social | |||||
| Impact on Daily Life | 6.2 ± 2.3 | 6.2 ± 2.4 | 6.6 ± 2.3 | 6.2 ± 2.4 | 6.3 ± 2.4 |
| Social Distancing Practices of Others | 6.3 ± 2.5 | 6.5 ± 2.6 | 6.2 ± 2.5 | 5.9 ± 2.9 | 6.3 ± 2.6 |
| Trust in Government Institutions | 6.7 ± 2.6 | 7.0 ± 2.7 | 6.8 ± 2.8 | 6.9 ± 2.7 | 6.8 ± 2.7 |
| Variable | Mental Health Diagnosis | Number of Students | Mean | Standard Deviation | p-Value |
|---|---|---|---|---|---|
| PSS-4 Scores | Yes | 227 | 8.08 | 3.00 | <0.001 |
| No | 599 | 6.86 | 2.99 | ||
| Prefer Not to Say | 26 | 8.88 | 2.88 | ||
| GAD-7 Scores | Yes | 227 | 9.29 | 5.32 | <0.001 |
| No | 599 | 6.72 | 5.07 | ||
| Prefer Not to Say | 26 | 8.65 | 5.32 | ||
| Percentage of Stress Due to COVID-19 | Yes | 227 | 54.33% | 21.45% | <0.05 |
| No | 599 | 49.35% | 24.23% | ||
| Prefer Not to Say | 26 | 53.15% | 21.03% |
| Variable | Stress Compared to Other Students (before COVID) | Anxiety Compared to Other Students (before COVID) | Changes in Anxiety Levels Since March 2020 | Changes in Stress Levels Since March 2020 | PSS-4 | GAD-7 |
|---|---|---|---|---|---|---|
| Stress Compared to Other Students (Before COVID) | - | 0.715 | 0.405 | 0.327 | 0.492 | 0.572 |
| Anxiety Compared to Other Students (Before COVID) | 0.715 | - | 0.351 | 0.415 | 0.496 | 0.532 |
| Changes in Stress Levels Since March 2020 | 0.405 | 0.351 | - | 0.751 | 0.551 | 0.570 |
| Changes in Anxiety Levels Since March 2020 | 0.327 | 0.415 | 0.751 | - | 0.553 | 0.516 |
| PSS-4 | 0.492 | 0.496 | 0.551 | 0.553 | - | 0.715 |
| GAD-7 | 0.572 | 0.532 | 0.570 | 0.516 | 0.715 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, A.A.; Crum, M.A.; Fowler, L.A. Assessing the Psychological Impacts of COVID-19 in Undergraduate Medical Students. Int. J. Environ. Res. Public Health 2021, 18, 2952. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18062952
Guo AA, Crum MA, Fowler LA. Assessing the Psychological Impacts of COVID-19 in Undergraduate Medical Students. International Journal of Environmental Research and Public Health. 2021; 18(6):2952. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18062952
Chicago/Turabian StyleGuo, Alyssa A., Marissa A. Crum, and Lauren A. Fowler. 2021. "Assessing the Psychological Impacts of COVID-19 in Undergraduate Medical Students" International Journal of Environmental Research and Public Health 18, no. 6: 2952. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18062952