
Insomnia Associated with Tinnitus and Gender Differences

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants and Procedure
2.2. Statistical Methods
3. Results
3.1. Sociodemographic Characteristics
3.2. Psychometric Results
3.3. Insomnia and Psychiatric Comorbidities
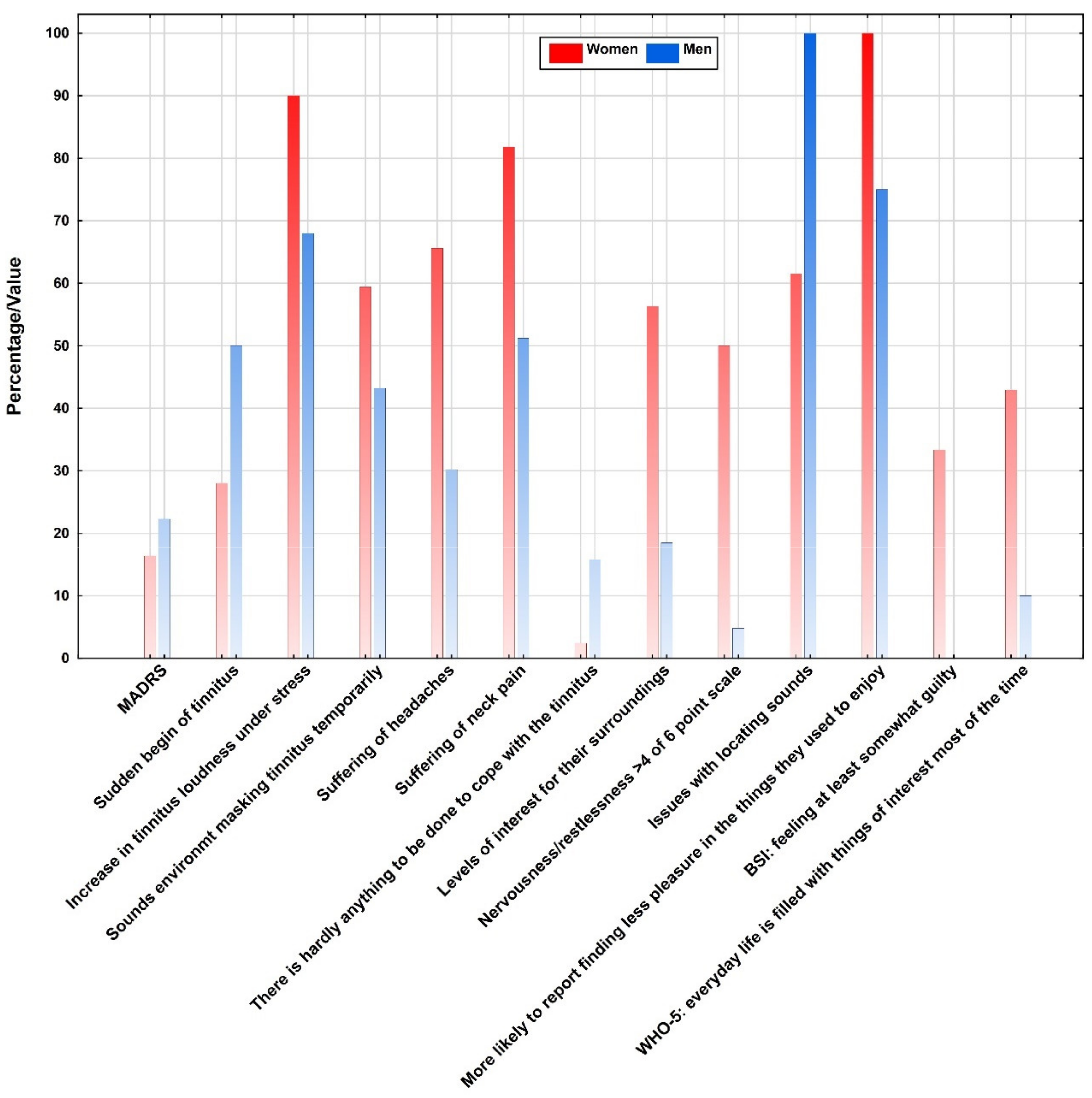
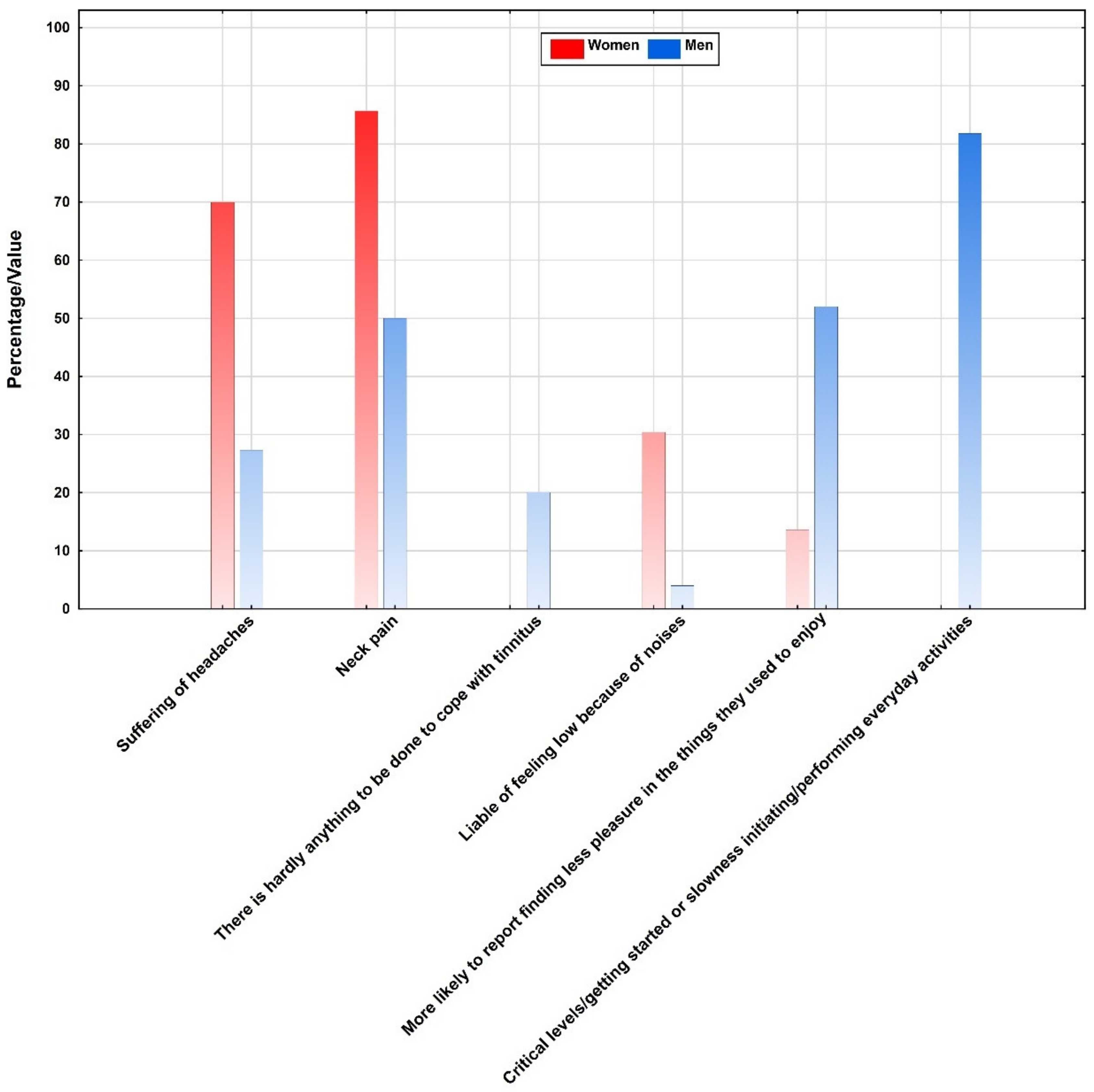
3.4. Tinnitus Related Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Asnis, G.; Majeed, K.; Henderson, M.; Sylvester, C.; Thomas, M.; La Garza, R. An Examination of the Relationship Between In-somnia and Tinnitus: A Review and Recommendations. Clin. Med. Insights Psychiatry 2018, 9. [Google Scholar] [CrossRef]
- Crönlein, T.; Spiegelhalder, K. Die insomnische Störung. Somnologie 2019, 23, 125–134. [Google Scholar] [CrossRef]
- Henry, J.; Zaugg, T.; Myers, P.; Schechter, M. The Role of Audiologic Evaluation in Progressive Audiologic Tinnitus Man-agement. Trends Amplif. 2008, 12, 170–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simoes, J.; Neff, P.; Schoisswohl, S.; Bulla, J.; Schecklmann, M.; Harrison, S.; Vesala, M.; Langguth, B.; Schlee, W. Toward Personalized Tinnitus Treatment: An Exploratory Study Based on Internet Crowdsensing. Front. Public Health 2019, 7, 157. [Google Scholar] [CrossRef]
- Alster, J.; Shemesh, Z.; Ornan, M.; Attias, J. Sleep disturbance associated with chronic tinnitus. Biol. Psychiatry 1993, 34, 84–90. [Google Scholar] [CrossRef]
- Crönlein, T.; Langguth, B.; Geisler, P.; Hajak, G. Tinnitus and insomnia. Prog. Brain Res. 2007, 166, 227–233. [Google Scholar] [CrossRef]
- Erlandsson, S.I.; Hallberg, L.R.; Axelsson, A. Psychological and Audiological Correlates of Perceived Tinnitus Severity. Int. J. Audiol. 1992, 31, 168–179. [Google Scholar] [CrossRef] [PubMed]
- Folmer, R.L.; Griest, S.E. Tinnitus and insomnia. Am. J. Otolaryngol. 2000, 21, 287–293. [Google Scholar] [CrossRef]
- Koning, H.M. Sleep Disturbances Associated with Tinnitus: Reduce the Maximal Intensity of Tinnitus. Int. Tinnitus J. 2019, 23, 64–68. [Google Scholar]
- Wakabayashi, S.; Saito, H.; Oishi, N.; Shinden, S.; Ogawa, K. Effects of tinnitus treatments on sleep disorders in patients with tinnitus. Int. J. Audiol. 2018, 57, 110–114. [Google Scholar] [CrossRef]
- Richter, K.; Acker, J.; Miloseva, L.; Peter, L.; Niklewski, G. Management of chronic tinnitus and insomnia with repetitive tran-scranial magnetic stimulation and cognitive behavioral therapy—A combined approach. Front. Psychol. 2017, 8, 575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miguel, G.S.; Yaremchuk, K.; Roth, T.; Peterson, E. The Effect of Insomnia on Tinnitus. Ann. Otol. Rhinol. Laryngol. 2014, 123, 696–700. [Google Scholar] [CrossRef] [PubMed]
- Crönlein, T.; Langguth, B.; Pregler, M.; Kreuzer, P.M.; Wetter, T.C.; Schecklmann, M. Insomnia in patients with chronic tinnitus: Cognitive and emotional distress as moderator variables. J. Psychosom. Res. 2016, 83, 65–68. [Google Scholar] [CrossRef]
- McKenna, L.; Handscomb, L.; Hoare, D.J.; Hall, D.A. A scientific cognitive-behavioral model of tinnitus: Novel conceptualiza-tions of tinnitus distress. Front. Neurol. 2014, 6, 5–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cima, R.F.; Maes, I.H.; Joore, M.A.; Scheyen, D.; El Refaie, A.; Baguley, D.M.; Anteunis, L.J.C. Specialised treatment based on cognitive be-haviour therapy versus usual care for tinnitus: A randomised controlled trial. Lancet 2012, 379, 1951–1959. [Google Scholar] [CrossRef]
- Seydel, C.; Haupt, H.; Olze, H.; Szczepek, A.J.; Mazurek, B. Gender and Chronic Tinnitus. Ear Hearth 2013, 34, 661–672. [Google Scholar] [CrossRef]
- Spiegelhalder, K.; Regen, W.; Feige, B.; Holz, J.; Piosczyk, H.; Baglioni, C.; Riemann, D.; Nissen, C. Increased EEG sigma and beta power during NREM sleep in primary insomnia. Biol. Psychol. 2012, 91, 329–333. [Google Scholar] [CrossRef]
- Vanneste, S.; Joos, K.; De Ridder, D. Prefrontal Cortex Based Sex Differences in Tinnitus Perception: Same Tinnitus Intensity, Same Tinnitus Distress, Different Mood. PLoS ONE 2012, 7, e31182. [Google Scholar] [CrossRef]
- Protopopescu, X.; Pan, H.; Altemus, M.; Tuescher, O.; Polanecsky, M.; McEwen, B.; Silbersweig, D.; Stern, E. Orbitofrontal cortex activity related to emotional processing changes across the menstrual cycle. Proc. Natl. Acad. Sci. USA 2005, 102, 16060–16065. [Google Scholar] [CrossRef] [Green Version]
- Hori, S.; Mori, K.; Mashimo, T.; Seiyama, A. Effects of Light and Sound on the Prefrontal Cortex Activation and Emotional Function: A Functional Near-Infrared Spectroscopy Study. Front. Neurosci. 2017, 11, 321. [Google Scholar] [CrossRef]
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines; World Health Organization: Geneva, Switzerland, 1992. [Google Scholar]
- Zenner, H.-P.; Delb, W.; Kröner-Herwig, B.; Jäger, B.; Peroz, I.; Hesse, G.; Mazurek, B.; Goebel, G.; Gerloff, C.; Trollmann, R.; et al. Zur interdisziplinären S3-Leitlinie für die Therapie des chronisch-idiopathischen Tinnitus. HNO 2015, 63, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, S.A.; Åsberg, M. A New Depression Scale Designed to be Sensitive to Change. Br. J. Psychiatry 1979, 134, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Derogatis, L.R.; Melisaratos, N. The Brief Symptom Inventory: An introductory report. Psychol. Med. 1983, 13, 595–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johns, M.W. A New Method for Measuring Daytime Sleepiness: The Epworth Sleepiness Scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Wellbeing Measures in Primary Health Care/The Depcare Project; WHO Regional Office for Europe: Copenhagen, Denmark, 1998. [Google Scholar]
- Goebel, G.; Hiller, W. Tinnitus-Fragebogen (TF). Ein Instrument zur Erfassung von Belastung und Schweregrad bei Tinnitus; Hogrefe: Göttingen, Germany; Bern, Switzerland; Toronto, ON, Canada, 1998. [Google Scholar]
- Landgrebe, M.; Zeman, F.; Koller, M.; Eberl, Y.; Mohr, M.; Reiter, J.; Staudinger, S.; Hajak, G.; Langguth, B. The Tinnitus Research Initiative (TRI) database: A new approach for delineation of tinnitus subtypes and generation of predictors for treatment outcome. BMC Med. Inform. Decis. Mak. 2010, 10, 42. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.T.; Hautzinger, M.; Steer, R.A. Testhandbuch, 2nd ed.; Huber: Bern, Germany, 1995. [Google Scholar]
- Langguth, B.; Goodey, R.; Azevedo, A.; Bjorne, A.; Cacace, A.; Crocetti, A.; Del Bo, L.; De Ridder, D.; Diges, I.; Elbert, T.; et al. Consensus for tinnitus patient assessment and treatment outcome measurement: Tinnitus Research Initiative meeting, Regensburg, July 2006. Prog. Brain Res. 2007, 166, 525–536. [Google Scholar] [CrossRef] [Green Version]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- Hill, T. Statistics: Methods and Applications: A Comprehensive Reference from Science, Industry, and Data Mining; Statsoft Inc.: Tulsa, OK, USA, 2005. [Google Scholar]
- WHO. The International Statistical Classification of Diseases and Health Related Problems Icd-10: Tabular List v. 1: Tenth Revision, 2nd ed.; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Schecklmann, M.; Pregler, M.; Kreuzer, P.M.; Poeppl, T.B.; Lehner, A.; Crönlein, T.; Wetter, T.C.; Frank, E.; Landgrebe, M.; Langguth, B. Psychophysiological Associations between Chronic Tinnitus and Sleep: A Cross Validation of Tinnitus and Insomnia Questionnaires. BioMed Res. Int. 2015, 2015, 461090. [Google Scholar] [CrossRef] [PubMed]
- Hoekstra, C.E.L.; Wesdorp, F.M.; Van Zanten, G.A. Socio-Demographic, Health, and Tinnitus Related Variables Affecting Tinnitus Severity. Ear Hearth 2014, 35, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, E.; Saijo, Y.; Kita, T.; Satoh, H.; Kawaharada, M.; Kishi, R. Effect of the Interaction Between Employment Level and Psychosocial Work Environment on Insomnia in Male Japanese Public Service Workers. Int. J. Behav. Med. 2012, 20, 355–364. [Google Scholar] [CrossRef]
- Lallukka, T.; Sares-Jäske, L.; Kronholm, E.; Sääksjärvi, K.; Lundqvist, A.; Partonen, T.; Rahkonen, O.; Kenkt, P. Sociodemographic and socioeconomic differences in sleep duration and insomnia-related symptoms in Finnish adults. BMC Public Health 2012, 12, 565. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sociodemographic Data | Women (%) | Men (%) | p-Value |
|---|---|---|---|
| Married | 73.3 | 60.0 | 0.22 |
| Higher education (at least intermediate school-leaving certificate) | 6.7 | 30.8 | 0.02 * |
| Vocational training | 93.3 | 52.0 | 0.01 * |
| University degree | 0.0 | 24.0 | 0.04 * |
| Working full time | 40.0 | 48.0 | 0.48 |
| Working part time | 33.3 | 12.0 | 0.19 |
| No employment | 26.7 | 40.0 | 0.43 |
| Symptoms and diagnoses | |||
| Year of first reported psychological issue (Ø; year) | 2010 | 2010 | 0.58 |
| Hyperacusis | 23.1 | 16.2 | 0.49 |
| Dysacusis | 32.1 | 32.6 | 0.97 |
| Noiser | 36.4 | 38.5 | 0.92 |
| Hearing aid | 38.5 | 18.0 | 0.15 |
| Mild depressive episode | 7.1 | 9.8 | 0.63 |
| Moderate depressive episode | 24.4 | 19.7 | 0.62 |
| Severe depressive episode | 0.0 | 3.3 | 0.24 |
| Recurrent depressive disorder | 7.3 | 1.6 | 0.16 |
| Anxiety disorder | 17.1 | 6.6 | 0.24 |
| Suspected anxiety disorder | 26.8 | 24.6 | 0.24 |
| Tinnitus loudness (Ø; scale from 0 to 100) | 54.5 | 58.4 | 0.92 |
| Other psychological or psychiatric treatment | 21.2 | 31.0 | 0.34 |
| Sociodemographic Data | Women (%) | Men (%) | p-Value |
|---|---|---|---|
| Married | 75.0 | 50.0 | 0.46 |
| Higher education (at least intermediate school-leaving certificate) | 12.5 | 63.6 | 0.01 * |
| Vocational training | 87.5 | 18.2 | <0.01 * |
| University degree | 0.0 | 45.5 | 0.03* |
| Working full time | 50.0 | 45.5 | 0.87 |
| Working part time | 50.0 | 9.1 | 0.12 |
| No employment | 0.0 | 45.5 | 0.05 |
| Symptoms and diagnoses | |||
| Year of first reported psychological issue (Ø; year) | 2009 | 2012 | 0.38 |
| Hyperacusis | 25.0 | 9.1 | 0.17 |
| Dysacusis | 20.0 | 38.5 | 0.18 |
| Noiser | 41.2 | 33.3 | 0.84 |
| Hearing aid | 31.6 | 20.8 | 0.24 |
| Mild depressive episode | 14.3 | 25.0 | 0.37 |
| Moderate depressive episode | 47.6 | 45.8 | 0.93 |
| Severe depressive episode | 0.0 | 8.3 | 0.17 |
| Recurrent depressive disorder | 4.8 | 4.2 | 0.93 |
| Anxiety disorder | 14.3 | 8.3 | 0.70 |
| Suspected anxiety disorder | 38.1 | 33.3 | 0.70 |
| Tinnitus loudness (Ø; scale from 0 to 100) | 55.0 | 62.9 | 0.68 |
| Other psychological or psychiatric treatment | 23.8 | 38.1 | 0.32 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Richter, K.; Zimni, M.; Tomova, I.; Retzer, L.; Höfig, J.; Kellner, S.; Fries, C.; Bernstein, K.; Hitzl, W.; Hillemacher, T.; et al. Insomnia Associated with Tinnitus and Gender Differences. Int. J. Environ. Res. Public Health 2021, 18, 3209. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063209
Richter K, Zimni M, Tomova I, Retzer L, Höfig J, Kellner S, Fries C, Bernstein K, Hitzl W, Hillemacher T, et al. Insomnia Associated with Tinnitus and Gender Differences. International Journal of Environmental Research and Public Health. 2021; 18(6):3209. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063209
Chicago/Turabian StyleRichter, Kneginja, Melanie Zimni, Iva Tomova, Lukas Retzer, Joachim Höfig, Stefanie Kellner, Carla Fries, Karina Bernstein, Wolfgang Hitzl, Thomas Hillemacher, and et al. 2021. "Insomnia Associated with Tinnitus and Gender Differences" International Journal of Environmental Research and Public Health 18, no. 6: 3209. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18063209