
The Sequential Mediating Effects of Dietary Behavior and Perceived Stress on the Relationship between Subjective Socioeconomic Status and Multicultural Adolescent Health

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Sample
2.3. Variables
2.3.1. Subjective Socioeconomic Status
2.3.2. Dietary Behavior
2.3.3. Perceived Stress
2.3.4. Subjective Health Status
2.3.5. Sociodemographic Variables
2.4. Analysis
3. Results
3.1. Descriptive Statistics and Correlations of Key Variables
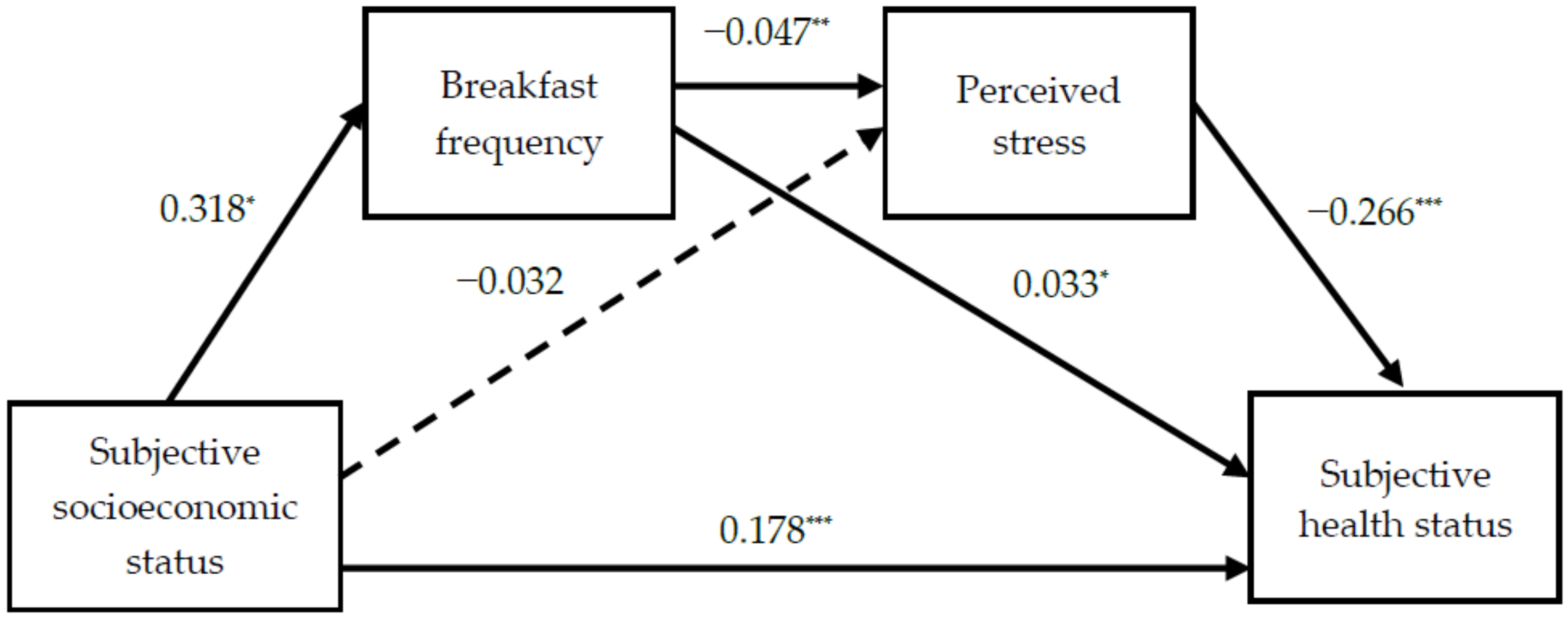
3.2. Association between Subjective SES, Breakfast Frequency, Perceived Stress, and Subjective Health Status
3.3. Sequential Mediating Effects Among Variables
4. Discussion
4.1. Subjective SES and Health Behavior
4.2. The Relationship between Breakfast Intake and Perceived Stress
4.3. Methodological Implications of Sequential Mediating Effects
4.4. Limitations and Recommendations for Further Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marmot, M.; Friel, S.; Bell, R.; Houweling, T.; Taylor, S. Closing the gap in a generation: Health equity through action on the social determinants of health. Lancet 2008, 372, 1661–1669. [Google Scholar] [CrossRef]
- Wickrama, K.A.; Bae, D.; O’Neal, C.W. Black-white disparity in young adults’ disease risk: An investigation of variation in the vulnerability of black young adults to early and later adversity. J. Adolesc. Health 2016, 59, 209–214. [Google Scholar] [CrossRef]
- Farmer, M.M.; Ferraro, K.F. Are racial disparities in health conditional on socioeconomic status? Soc. Sci. Med. 2005, 60, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Jung, E. Socioeconomic status and elderly health in life course perspective: Testing of multi-mediational effects of socioeconomic status in early adult and middle aged. Health Soc. Welf. Rev. 2016, 36, 53–84. [Google Scholar] [CrossRef]
- Sawyer, S.M.; Afifi, R.A.; Bearinger, L.H.; Blakemore, S.J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence: A foundation for future health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- East, P.; Doom, J.; Delker, E.; Estela Blanco, E.; Burrows, R.; Correa-Burrows, P.; Lozoff, B.; Gahagan, S. Childhood socioeconomic hardship, family conflict, and young adult hypertension: The Santiago Longitudinal Study. Soc. Sci. Med. 2020, 253, 112962. [Google Scholar] [CrossRef] [PubMed]
- Plenty, S.; Mood, C. Money, peers and parents: Social and economic aspects of inequality in youth wellbeing. J. Youth Adolesc. 2016, 45, 1294–1308. [Google Scholar] [CrossRef] [Green Version]
- Korea Ministry of Government Legislation. Easy to Find, Practical Law. Multicultural Families. 2020. Available online: https://www.easylaw.go.kr/CSM/SubCcfCmd.laf?csmSeq=1387 (accessed on 13 January 2021).
- Yang, K.; Shin, H.; Park, J. Longitudinal survey and research on policy plan for multicultural youth Ⅱ: Total report. Republic of Korea National Youth Policy Institute. 2014, pp. 1–465. Available online: https://203.254.187.10/dl_image/IMG/01/000000000385/SERVICE/000000000385_01.PDF (accessed on 11 November 2020).
- Statistics Korea. Dynamic Statistics of Multicultural Households. Seoul: Statistics Korea. 2018. Available online: http://kostat.go.kr/portal/korea/kor_nw/1/1/index.board?bmode=read&bSeq=&aSeq=378479&pageNo=1&rowNum=10&navCount=10&currPg=&searchInfo=srch&sTarget=title&sTxt=%EB%8B%A4%EB%AC%B8%ED%99%94 (accessed on 9 September 2020).
- Ministry of the Interior and Safety. Results of a Survey on the Status of Foreign Residents in Local Governments. Seoul: Ministry of the Interior and Safety. 2018. Available online: mois.go.kr/frt/bbs/type001/commonSelectBoardArticle.do?bbsId=BBSMSTR_000000000014&nttId=73857 (accessed on 21 October 2020).
- World Health Organization. Orientation Programme on Adolescent Health for Health Care Providers. Commonwealth Medical Association Trust and UNICEF. 2006. Available online: https://www.who.int/maternal_child_adolescent/documents/9241591269/en/ (accessed on 19 March 2021).
- Edelman, C.L.; Mandle, C.L.; Kudzma, E.C. Health Promotion Throughout the Life Span; Elsevier Health Science: Amsterdam, The Netherlands, 2017; pp. 535–556. [Google Scholar]
- Salam, R.A.; Das, J.K.; Lassi, Z.S.; Bhutta, Z.A. Adolescent health and well-being: Background and methodology for review of potential interventions. J. Adolesc. Health 2016, 59, S4–S10. [Google Scholar] [CrossRef] [Green Version]
- Ayranci, U.; Erenoglu, N.; Son, O. Eating habits, lifestyle factors, and body weight status among Turkish private educational institution students. Nutrition 2010, 26, 772–778. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; You, S. Study on skipping breakfast in adolescents classified by household type. Korean J. Community Living Sci. 2017, 28, 329–340. [Google Scholar] [CrossRef] [Green Version]
- Astbury, N.M.; Taylor, M.A.; Macdonald, I.A. Breakfast consumption affects appetite, energy intake, and the metabolic and endocrine responses to foods consumed later in the day in male habitual breakfast eaters. J. Nutr. 2011, 141, 1381–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruening, M.; Larson, N.; Story, M.; Neumark-Sztainer, D.; Hannan, P. Predictors of adolescent breakfast consumption: Longitudinal findings from Project EAT. J. Nutr. Educ. Behav. 2011, 43, 390–395. [Google Scholar] [CrossRef]
- Choi, C.; Hwang, S.; Yoo, M.; Lee, M.; Kim, J.; Moon, J. A Study on the Implementation of International Convention on Child-Youth Rights Korean Child-Youth Human Rights Report 2018. National Youth Policy Institute 2018, 1–778. Available online: https://www.nypi.re.kr/brdrr/boardrrView.do?menu_nix=4o9771b7&brd_id=BDIDX_PJk7xvf7L096m1g7Phd3YC&cont_idx=634&seltab_idx=0&edomweivgp=R (accessed on 21 October 2020).
- Park, H.-S.; Han, J.-Y.; Lee, N.-Y. The association of health behaviors with stress perception among high school students in Korea: Based on 2015 Korean Youth Risk Behavior Survey. J. Korean Acad. Community Health Nurs. 2018, 29, 87–96. [Google Scholar] [CrossRef]
- Gu, H. Influence of perceived stress on obesity in South Korean adolescents using data from the 13th 2017 Korea Youth Risk Behavior Web-Based Survey. Korean J. Health Educ. Promot. 2019, 36, 29–41. [Google Scholar] [CrossRef]
- Lee, B.; Kim, J.-S.; Kim, K. Factors that affect the subjective health status of adolescents in multicultural families. J. Korean Public Health Nurs. 2013, 27, 64–75. [Google Scholar] [CrossRef] [Green Version]
- Goodman, E.; Huang, B.; Schafer-Kalkhoff, T.; Adler, N.E. Perceived socioeconomic status: A new type of identity that influences adolescents’ self-rated health. J. Adolesc. Health. 2007, 41, 479–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinberg, L.; Morris, A.S. Adolescent development. Annu. Rev. Psychol. 2001, 52, 83–110. [Google Scholar] [CrossRef]
- Haddad, M.R.; Sarti, F.M. Sociodemographic determinants of health behaviors among Brazilian adolescents: Trends in physical activity and food consumption, 2009–2015. Appetite 2020, 144, 104454. [Google Scholar] [CrossRef]
- Jang, I. Comparative study of health risk behaviors, mental health and subjective health status of adolescents in multicultural and monocultural families. J. Korean Soc. School Health 2020, 33, 115–124. [Google Scholar] [CrossRef]
- Hayes, A.F. An index and test of linear moderated mediation. Multivar. Behav. Res. 2015, 50, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Ferrer-Cascales, R.; Sánchez-SanSegundo, M.; Ruiz-Robledillo, N.; Albaladejo-Blázquez, N.; Laguna-Pérez, A.; Zaragoza-Martí, A. Eat or skip breakfast? The important role of breakfast quality for health-related quality of life, stress and depression in Spanish adolescents. Int. J. Environ. Res. Public Health 2018, 15, 1781. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.J.; Lee, S.S.; Kim, D.H.; Ham, K.A.; Lee, D.H. The differences of depression, anxiety, and stress according to academic performance and home economic status among elementary and middle school students. J. Educ. Res. 2014, 12, 29–50. Available online: https://intereri.org/k/bbs/board.php?bo_table=thesis&wr_id=30&page=2 (accessed on 15 October 2020).
- Kim, S.; Kim, Y. A study on the health inequality in childhood: The moderating effects of social support between the social economic level and health problems. Res. Cent. Korea Youth Cult 2017, 50, 7–30. [Google Scholar] [CrossRef]
- Lee, H.A.; Park, H. The mediation effect of individual eating behaviours on the relationship between socioeconomic status and dietary quality in children: The Korean National Health and Nutrition Examination Survey. Eur. J. Nutr. 2017, 56, 1339–1346. [Google Scholar] [CrossRef] [Green Version]
- Osera, T.; Awai, M.; Kobayashi, M.; Tsutie, S.; Kurihara, N. Relationship between self-rated health and lifestyle and food habits in Japanese high school students. Behav. Sci. 2017, 7, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marques, A.; Peralta, M.; Santos, T.; Martins, J.; de Matos, M.G. Self-rated health and health-related quality of life are related with adolescents’ healthy lifestyle. Public Health 2019, 170, 89–94. [Google Scholar] [CrossRef]
- Caro, D.H.; Cortés, D. Measuring family socioeconomic status: An illustration using data from PIRLS 2006. IERI Monogr. Ser. Issues Methodol. Large-Scale Assess. 2012, 5, 9–33. Available online: https://www.ierinstitute.org/fileadmin/Documents/IERI_Monograph/IERI_Monograph_Volume_05_Chapter_1.pdf (accessed on 30 October 2020).
- Svedberg, P.; Nygren, J.; Staland-Nyman, C.; Nyholm, M. The validity of socioeconomic status measures among adolescents based on self-reported information about parents’ occupations, FAS and perceived SES; implication for health related quality of life studies. BMC Med. Res. Methodol. 2016, 16, 48. [Google Scholar] [CrossRef] [Green Version]
- Korean Ministry of Health and Welfare. 5th Korean National Health Plan 2030 (2021–2030). Seoul: Korean Health Promotion Institute. 2020. Available online: https://www.khealth.or.kr/board?menuId=MENU00783&siteId=null (accessed on 13 January 2021).
- Ma, X.; Chen, Q.; Pu, Y.; Guo, M.; Jiang, Z.; Huang, W.; Long, Y.; Xu, Y. Skipping breakfast is associated with overweight and obesity: A systematic review and meta-analysis. Obes. Res. Clin. Pract. 2020, 14, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Babaeer, L.Y.; Wraith, D. A systematic review of the effect of habitual breakfast for adolescents aged 11–19 years on academic performance. J. Adolesc. Family Health 2018, 29, 7. Available online: https://scholar.utc.edu/jafh/vol9/iss1/7 (accessed on 7 November 2020).
- Lee, H.J.; Kim, C.H.; Han, I.; Kim, S.H. Emotional state according to breakfast consumption in 62276 South Korean adolescents. Iran. J. Pediatr. 2019, 29, e92193. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.-K.; Chung, W.-J.; Lim, S.-J.; Yoon, S.; Lee, J.; Kim, E.; Ko, L. Socioeconomic inequity in self-rated health status and contribution of health behavioral factors in Korea. J. Prev. Med. Public Health 2010, 43, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Park, H.-R.; Lee, J.-S. The relationship between evaluative concerns perfectionism, and speech anxiety in college students: The serial multiple mediation effects of internalized shame and intolerance of uncertainty. Korean J. Stress Res. 2017, 25, 246–254. [Google Scholar] [CrossRef] [Green Version]
- Judd, C.M.; Kenny, D.A. Process analysis: Estimating mediation in treatment evaluations. Evaluation review 1981, 5, 602–619. [Google Scholar] [CrossRef]
- Joffer, J.; Flacking, R.; Bergström, E.; Randell, E.; Jerdén, L. Self-rated health, subjective social status in school and socioeconomic status in adolescents: A cross-sectional study. BMC Public Health 2019, 19, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Okeyo, A.P.; Seekoe, E.; de Villiers, A.; Faber, M.; Nel, J.H.; Steyn, N.P. Dietary practices and adolescent obesity in secondary school learners at disadvantaged schools in South Africa: Urban-rural and gender differences. Int. J. Environ. Res. Public Health 2020, 17, 5864. [Google Scholar] [CrossRef] [PubMed]
- Van Droogenbroeck, F.; Spruyt, B.; Keppens, G. Gender differences in mental health problems among adolescents and the role of social support: Results from the Belgian health interview surveys 2008 and 2013. BMC Psychiatry 2018, 18, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Novak, D.; Štefan, L.; Emeljanovas, A.; Mieziene, B.; Milanović, I.; Janić, S.R.; Kawachi, I. Factors associated with good self-rated health in European adolescents: A population-based cross-sectional study. Int. J. Public Health 2017, 62, 971–979. [Google Scholar] [CrossRef]
- Hoffman, J.A.; Miller, E.A. Addressing the consequences of school closure due to COVID-19 on children’s physical and mental well-being. World Med. Health Policy 2020, 12, 300–310. [Google Scholar] [CrossRef]
- Parnham, J.C.; Laverty, A.A.; Majeed, A.; Vamos, E.P. Half of children entitled to free school meals did not have access to the scheme during COVID-19 lockdown in the UK. Public Health 2020, 187, 161–164. [Google Scholar] [CrossRef]
- Morales, D.X.; Morales, S.A.; Beltran, T.F. Racial/ethnic disparities in household food insecurity during the COVID-19 pandemic: A nationally representative study. J. Racial Ethn. Health Di. 2020, 1–15. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Mean ± SD or n (%) |
|---|---|
| Age | 13.31 ± 0.99 |
| Grade | |
| 1st (14 years old) | 206 (41.2) |
| 2nd (15 years old) | 168 (33.6) |
| 3rd (16 years old) | 126 (25.2) |
| Sex | |
| Male | 238 (47.6) |
| Residential area | |
| Rural | 158 (31.6) |
| Suburban | 240 (48.0) |
| Urban | 102 (20.4) |
| Living arrangement | |
| Home with family | 480 (96.0) |
| Home with relatives | 3 (0.6) |
| Dormitory | 8 (1.6) |
| Care facility | 9 (1.8) |
| Subjective Socioeconomic Status | Breakfast Frequency | Perceived Stress | Subjective Health Status | |
|---|---|---|---|---|
| Subjective socioeconomic status | 1 | |||
| Breakfast frequency | 0.104 * | 1 | ||
| Perceived stress | −0.042 | −0.131 ** | 1 | |
| Subjective health status | 0.204 ** | 0.161 ** | −0.323 ** | 1 |
| Pathway | B | SE | t | p | F | ||
|---|---|---|---|---|---|---|---|
| Subjective socioeconomic status | → | Breakfast frequency | 0.318 | 0.104 | 2.328 | 0.020 | 5.419 |
| Subjective socioeconomic status | → | Perceived stress | −0.032 | −0.029 | −0.638 | 0.524 | 4.558 |
| Breakfast frequency | −0.047 | −0.128 | −2.869 | 0.004 | |||
| Subjective socioeconomic status | → | Subjective health status | 0.178 | 0.180 | 4.332 | <0.001 | 29.400 |
| Breakfast frequency | 0.033 | 0.103 | 2.446 | 0.015 | |||
| Perceived stress | −0.266 | −0.302 | −7.242 | <0.001 | |||
| Mediating Pathway | Bootstrapping Estimate | 95% CI | ||
|---|---|---|---|---|
| B | SE | LLCI | ULCI | |
| Subjective socioeconomic status ⇒ Breakfast frequency ⇒ Subjective health status | 0.011 | 0.0070 | 0.0002 | 0.0271 |
| Subjective socioeconomic status ⇒ Perceived stress ⇒ Subjective health status | 0.009 | 0.0143 | −0.0193 | 0.0373 |
| Subjective socioeconomic status ⇒ Breakfast frequency ⇒ Perceived stress ⇒ Subjective health status | 0.004 | 0.0025 | 0.0002 | 0.0098 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Lee, H.; Lee, M.; Lee, H.; Kim, S.; Konlan, K.D. The Sequential Mediating Effects of Dietary Behavior and Perceived Stress on the Relationship between Subjective Socioeconomic Status and Multicultural Adolescent Health. Int. J. Environ. Res. Public Health 2021, 18, 3604. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073604
Kim Y, Lee H, Lee M, Lee H, Kim S, Konlan KD. The Sequential Mediating Effects of Dietary Behavior and Perceived Stress on the Relationship between Subjective Socioeconomic Status and Multicultural Adolescent Health. International Journal of Environmental Research and Public Health. 2021; 18(7):3604. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073604
Chicago/Turabian StyleKim, Youlim, Hyeonkyeong Lee, Mikyung Lee, Hyeyeon Lee, Sookyung Kim, and Kennedy Diema Konlan. 2021. "The Sequential Mediating Effects of Dietary Behavior and Perceived Stress on the Relationship between Subjective Socioeconomic Status and Multicultural Adolescent Health" International Journal of Environmental Research and Public Health 18, no. 7: 3604. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18073604