
Feasibility of an Outpatient Training Program after COVID-19

Abstract
:1. Introduction
2. Materials and Methods
2.1. Management during the Pulmonary Rehabilitation (PR) Program
2.1.1. Determination of Peak Work Rate
2.1.2. Training Intervention
2.2. Statistics
3. Results
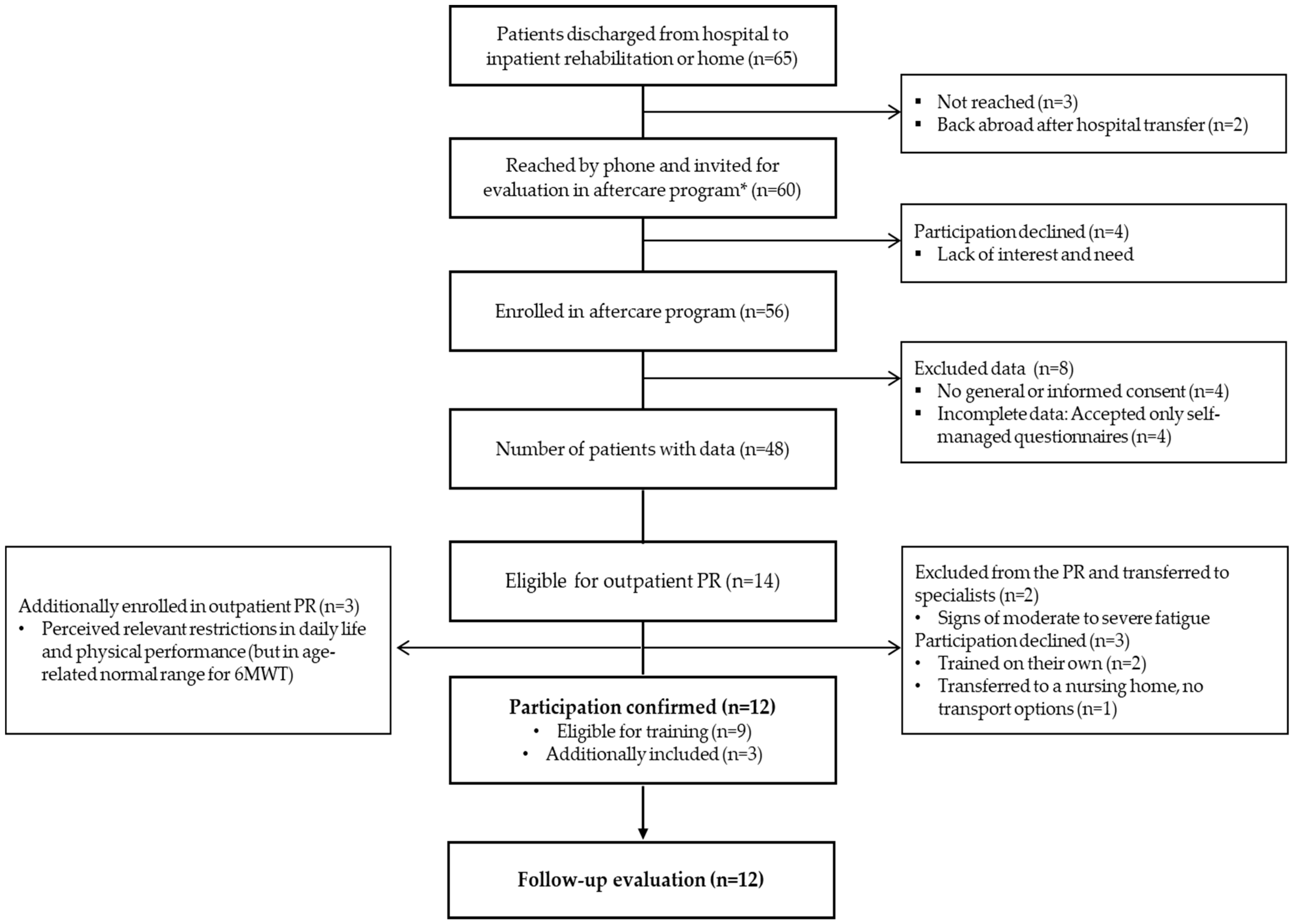
3.1. Participants
3.2. Feasibility Outcomes
3.2.1. Recruitment Rate
3.2.2. Adherence and Tolerability to PR
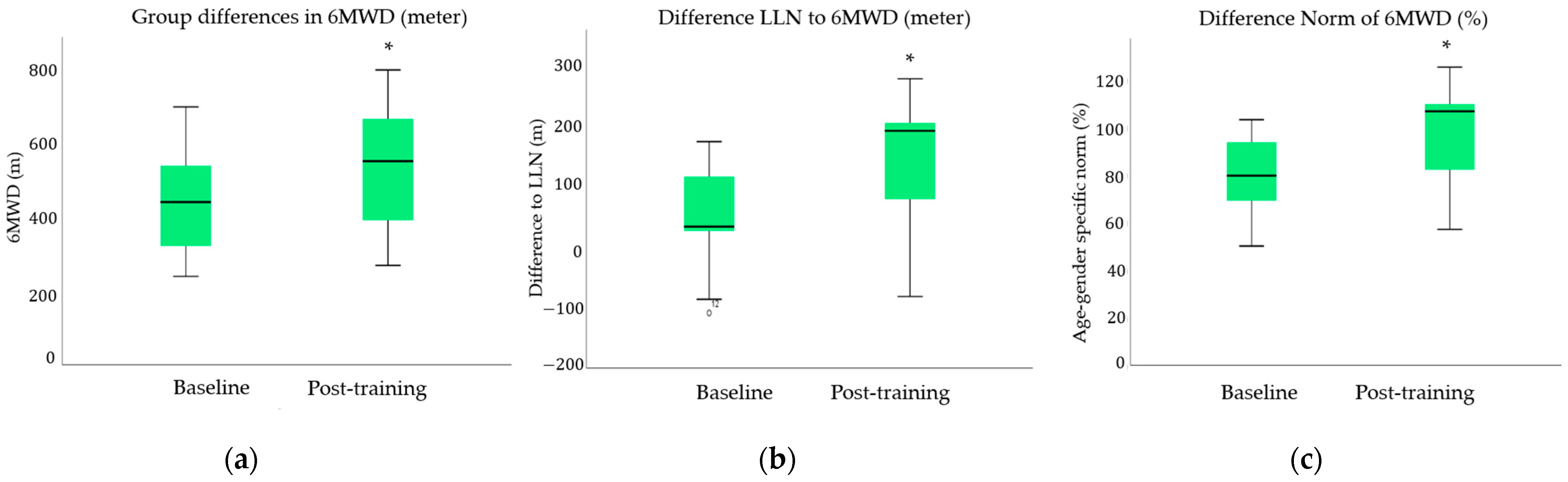
3.3. Clinical Outcomes
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murray, A.; Gerada, C.; Morris, J. We need a Nightingale model for rehab after covid-19. Health Serv. J. 2020. Available online: https://www.hsj.co.uk/commissioning/we-need-a-nightingale-model-for-rehab-after-covid-19-/7027335.article (accessed on 3 February 2021).
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute covid-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef]
- Townsend, L.; Dyer, A.H.; Jones, K.; Dunne, J.; Mooney, A.; Gaffney, F.; O’Connor, L.; Leavy, D.; O’Brien, K.; Dowds, J.; et al. Persistent fatigue following SARS-CoV-2 infection is common and independent of severity of initial infection. PLoS ONE 2020, 15, e0240784. [Google Scholar] [CrossRef] [PubMed]
- van der Sar-van der Brugge, S.; Talman, S.; de Winter, L.B.; de Mol, M.; Hoefman, E.; van Etten, R.; De Backer, I. Pulmonary function and health-related quality of life after COVID-19 pneumonia. Respir. Med. 2021, 176, 106272. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.W.; Shah, A.S.; Johnston, J.C.; Carlsten, C.; Ryerson, C.J. Patient-reported outcome measures after COVID-19: A prospective cohort study. Eur. Respir. J. 2020, 56, 2003276. [Google Scholar] [CrossRef]
- Ahmed, H.; Patel, K.; Greenwood, D.C.; Halpin, S.; Lewthwaite, P.; Salawu, A.; Eyre, L.; Breen, A.; O’Connor, R.; Jones, A.; et al. Long-term clinical outcomes in survivors of severe acute respiratory syndrome and Middle East respiratory syndrome coronavirus outbreaks after hospitalisation or ICU admission: A systematic review and meta-analysis. J. Rehabil. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Belli, S.; Balbi, B.; Prince, I.; Cattaneo, D.; Masocco, F.; Zaccaria, S.; Bertalli, L.; Cattini, F.; Lomazzo, A.; Negro, F.D.; et al. Low physical functioning and impaired performance of activities of daily life in COVID-19 patients who survived hospitalisation. Eur. Respir. J. 2020, 56, 2002096. [Google Scholar] [CrossRef] [PubMed]
- Borst, B.V.D.; Peters, J.B.; Brink, M.; Schoon, Y.; Bleeker-Rovers, C.P.; Schers, H.; Van Hees, H.W.H.; Van Helvoort, H.; Boogaard, M.V.D.; Van Der Hoeven, H.; et al. Comprehensive health assessment three months after recovery from acute COVID-19. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Guler, S.A.; Ebner, L.; Beigelman, C.; Bridevaux, P.-O.; Brutsche, M.; Clarenbach, C.; Garzoni, C.; Geiser, T.K.; Lenoir, A.; Mancinetti, M.; et al. Pulmonary function and radiological features four months after COVID-19: First results from the national prospective observational Swiss COVID-19 lung study. Eur. Respir. J. 2021, 2003690. [Google Scholar] [CrossRef]
- Zhu, Y.; Wang, Z.; Zhou, Y.; Onoda, K.; Maruyama, H.; Hu, C.; Liu, Z. Summary of respiratory rehabilitation and physical therapy guidelines for patients with COVID-19 based on recommendations of World Confederation for Physical Therapy and National Association of Physical Therapy. J. Phys. Ther. Sci. 2020, 32, 545–549. [Google Scholar] [CrossRef]
- Sheehy, L.M. Considerations for Postacute Rehabilitation for Survivors of COVID-19. JMIR Public Health Surveill. 2020, 6, e19462. [Google Scholar] [CrossRef] [PubMed]
- Spruit, M.A.; Holland, A.E.; Singh, S.J.; Troosters, T. Report of an Ad-Hoc International Task Force to Develop an Expert-Based Opinion on Early and Short-Term Rehabilitative Interventions (After the Acute Hospital Setting) in Covid-19 Survivors, version April 3rd 2020; European Respiratory Society: Lausanne, Switzerland; Available online: https://www.ersnet.org/news-and-features/covid-19-blog/covid-19-and-rehabilitation/ (accessed on 25 March 2021).
- Thornton, J. Covid-19: The challenge of patient rehabilitation after intensive care. BMJ 2020, 369, m1787. [Google Scholar] [CrossRef] [PubMed]
- Polastri, M.; Nava, S.; Clini, E.; Vitacca, M.; Gosselink, R. COVID-19 and pulmonary rehabilitation: Preparing for phase three. Eur. Respir. J. 2020, 55, 2001822. [Google Scholar] [CrossRef]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.-C.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Key Concepts and Advances in Pulmonary Rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef]
- Sun, T.; Guo, L.; Tian, F.; Dai, T.; Xing, X.; Zhao, J.; Li, Q. Rehabilitation of patients with COVID-19. Expert Rev. Respir. Med. 2020, 14, 1249–1256. [Google Scholar] [CrossRef]
- Gloeckl, R.; Marinov, B.; Pitta, F. Practical recommendations for exercise training in patients with COPD. Eur. Respir. Rev. 2013, 22, 178–186. [Google Scholar] [CrossRef]
- Puchner, B.; Sahanic, S.; Kirchmair, R.; Pizzini, A.; Sonnweber, B.; Wöll, E.; Mühlbacher, A.; Garimorth, K.; Dareb, B.; Ehling, R.; et al. Beneficial effects of multi-disciplinary rehabilitation in post-acute COVID-19—An observational cohort study. Eur. J. Phys. Rehabil. Med. 2021, 57. [Google Scholar]
- Gloeckl, R.; Leitl, D.; Jarosch, I.; Schneeberger, T.; Nell, C.; Stenzel, N.; Vogelmeier, C.F.; Kenn, K.; Koczulla, A.R. Benefits of pulmonary rehabilitation in COVID-19—a prospective observational cohort study. ERJ Open Res. 2021, in press. [Google Scholar] [CrossRef]
- Thabane, L.; Ma, J.; Chu, R.; Cheng, J.; Ismaila, A.; Rios, L.P.; Robson, R.; Thabane, M.; Giangregorio, L.; Goldsmith, C.H. A tutorial on pilot studies: The what, why and how. BMC Med Res. Methodol. 2010, 10, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsen, T.S.; Scott, J.M.; Michalski, M.; Capaci, C.; Thomas, S.; Herndon, J.E., 2nd; Sasso, J.; Eves, N.D.; Jones, L.W. Novel Methods for Reporting of Exercise Dose and Adherence: An Exploratory Analysis. Med. Sci. Sports Exerc. 2018, 50, 1134–1141. [Google Scholar] [CrossRef]
- Garvey, C.; Bayles, M.P.; Hamm, L.F.; Hill, K.; Holland, A.; Limberg, T.M.; Spruit, M.A. Pulmonary Rehabilitation Exercise Prescription in Chronic Obstructive Pulmonary Disease: Review of Selected Guidelines: An official statement from the american association of cardiovascular and pulmonary rehabilitation. J. Cardiopulm. Rehabil. Prev. 2016, 36, 75–83. [Google Scholar] [CrossRef]
- Office for Human Research Protections. Unanticipated Problems Involving Risks & Adverse Events Guidance (2007). Available online: https://www.hhs.gov/ohrp/regulations-and-policy/guidance/reviewing-unanticipated-problems/index.html (accessed on 27 February 2021).
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Mahler, D.A.; Wells, C.K. Evaluation of Clinical Methods for Rating Dyspnea. Chest 1988, 93, 580–586. [Google Scholar] [CrossRef] [Green Version]
- Klok, F.A.; Boon, G.J.; Barco, S.; Endres, M.; Geelhoed, J.M.; Knauss, S.; Rezek, S.A.; Spruit, M.A.; Vehreschild, J.; Siegerink, B. The Post-COVID-19 Functional Status scale: A tool to measure functional status over time after COVID-19. Eur. Respir. J. 2020, 56, 2001494. [Google Scholar] [CrossRef]
- Valko, P.O.; Bassetti, C.L.; Bloch, K.E.; Held, U.; Baumann, C.R. Validation of the Fatigue Severity Scale in a Swiss Cohort. Sleep 2008, 31, 1601–1607. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bienvenu, O.J.; Williams, J.B.; Yang, A.; Hopkins, R.O.; Needham, D.M. Posttraumatic stress disorder in survivors of acute lung injury: Evaluating the Impact of Event Scale-Revised. Chest 2013, 144, 24–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spruit, M.A.; Wouters, E.F. Organizational aspects of pulmonary rehabilitation in chronic respiratory diseases. Respirology 2019, 24, 838–843. [Google Scholar] [CrossRef] [PubMed]
- Heisler, M.; Vijan, S.; Anderson, R.M.; Ubel, P.A.; Bernstein, S.J.; Hofer, T.P. When do patients and their physicians agree on diabetes treatment goals and strategies, and what difference does it make? J. Gen. Intern. Med. 2003, 18, 893–902. [Google Scholar] [CrossRef]
- Bovend’Eerdt, T.J.H.; Botell, R.E.; Wade, D.T. Writing SMART rehabilitation goals and achieving goal attainment scaling: A practical guide. Clin. Rehabil. 2009, 23, 352–361. [Google Scholar] [CrossRef]
- Chura, R.L.; Marciniuk, D.D.; Clemens, R.; Butcher, S.J. Test-Retest Reliability and Physiological Responses Associated with the Steep Ramp Anaerobic Test in Patients with COPD. Pulm. Med. 2012, 2012, 1–6. [Google Scholar] [CrossRef]
- De Backer, I.C.; Schep, G.; Hoogeveen, A.; Vreugdenhil, G.; Kester, A.D.; Van Breda, E. Exercise Testing and Training in a Cancer Rehabilitation Program: The Advantage of the Steep Ramp Test. Arch. Phys. Med. Rehabil. 2007, 88, 610–616. [Google Scholar] [CrossRef]
- Meyer, K. Exercise training in heart failure: Recommendations based on current research. Med. Sci. Sports Exerc. 2001, 33, 525–531. [Google Scholar] [CrossRef]
- Bongers, B.C.; Werkman, M.S.; Arets, H.G.; Takken, T.; Hulzebos, H.J. A possible alternative exercise test for youths with cystic fibrosis: The steep ramp test. Med. Sci. Sports Exerc. 2015, 47, 485–492. [Google Scholar] [CrossRef] [Green Version]
- American Thoracic Society; American College of Chest Physicians. ATS/ACCP Statement on cardiopulmonary exercise testing. Am. J. Respir. Crit Care Med. 2003, 167, 211–277. [Google Scholar]
- Borg, G. Ratings of Perceived Exertion and Heart Rates During Short-Term Cycle Exercise and Their Use in a New Cycling Strength Test. Int. J. Sports Med. 1982, 3, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Nici, L.; ZuWallack, R.; Wouters, E.; Donner, C.F. On pulmonary rehabilitation and the flight of the bumblebee: The ATS/ERS Statement on Pulmonary Rehabilitation. Eur. Respir. J. 2006, 28, 461–462. [Google Scholar] [CrossRef]
- Enright, P.L.; Sherrill, D.L. Reference Equations for the Six-Minute Walk in Healthy Adults. Am. J. Respir. Crit. Care Med. 1998, 158, 1384–1387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. Clinical Management of COVID-19: Intermim Guidance, 27 May 2020. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-1 (accessed on 26 January 2021).
- NICE Statement about Graded Exercise Therapy in the Context of COVID-19. Available online: https://www.nice.org.uk/guidance/gid-ng10091/documents/interim-findings-2 (accessed on 3 February 2021).
- NIHR Living with Covid-19. Available online: https://evidence.nihr.ac.uk/themedreview/living-with-covid19 (accessed on 3 February 2021).
- Carruthers, B.M.; van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A.C.; Speight, N.; Vallings, R.; et al. Myalgic encephalomyelitis: International Consensus Criteria. J. Intern Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Aerobic Cycle Endurance Training (ACE) | Resistance Training (RT) |
|---|---|
| Duration 30 min | Duration 30–40 min |
| Interval mode (alternating HI and MI) | |
| Warm-up 4 min at 15% peakWR HI 4 min 50% peak WR (4×) Borg 4–6 MI 3 min 20–30% peak WR (3×) Cooling-down 3 min at 15% peakWR | 10–12 repetitions 50–85% of RM 3 rounds per device Adjustment of weight when more or less than 10–12 repetition achieved |
| Continuous mode 30 min, 20–30% peakWR |
| N = 12 | Median (Range); Frequency (Percentage) |
|---|---|
| Age, years | 61 (26–84) |
| Gender, female (%) | 4 (33%) |
| Severity of pneumonia, n (%) | |
| Mild | 1 (8%) |
| Moderate | 8 (67%) |
| Severe | 2 (16%) |
| Critical | 1 (8%) |
| Pre-existing Comorbidities | |
| Cardiovascular disease, n (%) | 6 (50%) |
| Arterial hypertonia, n (%) | 3 (25%) |
| Chronic renal disease, n (%) | 5 (n = 5) |
| Cancerogenous disease, n (%) | 3 (25%) |
| Chronic pulmonary disease, n (%) | 2 (16%) |
| Diabetes mellitus, n (%) | 1 (8%) |
| Adipositas (BMI ≥ 25), n (%) | 1 (8%) |
| Other internal disease, n (%) | 2 (16%) |
| Polyneuropathia, n (%) | 1 (8%) |
| Length of stay at the hospital (days) | 11 (3–24) |
| Duration between COVID-19 diagnosis and PR admission (days) | 41.5 (21–73) |
| Initial 6MWD %Norm, (%) | 79.5 (50–100) |
| Desaturation during 6MWT, yes (%) | 4 (33%) |
| mMRC Dyspnea (0–4) | |
| 0, n (%) | 1 (8%) |
| 1, n (%) | 4 (33%) |
| 2, n (%) | 7 (58%) |
| 3, n (%) | 0 (0%) |
| 4, n (%) | 0 (0%) |
| EQ-5D-5L VAS, 0–100% (%) | 70 (30–85) |
| EQ-5D-5L VAS < 80%, n (%) | 9 (75%) |
| Initial PCFS ≥ 2, n (%) | 10 (83%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Betschart, M.; Rezek, S.; Unger, I.; Beyer, S.; Gisi, D.; Shannon, H.; Sieber, C. Feasibility of an Outpatient Training Program after COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 3978. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083978
Betschart M, Rezek S, Unger I, Beyer S, Gisi D, Shannon H, Sieber C. Feasibility of an Outpatient Training Program after COVID-19. International Journal of Environmental Research and Public Health. 2021; 18(8):3978. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083978
Chicago/Turabian StyleBetschart, Martina, Spencer Rezek, Ines Unger, Swantje Beyer, David Gisi, Harriet Shannon, and Cornel Sieber. 2021. "Feasibility of an Outpatient Training Program after COVID-19" International Journal of Environmental Research and Public Health 18, no. 8: 3978. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18083978