
First Data in the Process of Validating a Tool to Evaluate Knowledge, Attitude, and Practice of Healthcare Providers in Oral Care of Institutionalized Elderly Residents: Content Validity, Reliability and Pilot Study

Abstract
:1. Introduction
1.1. Background
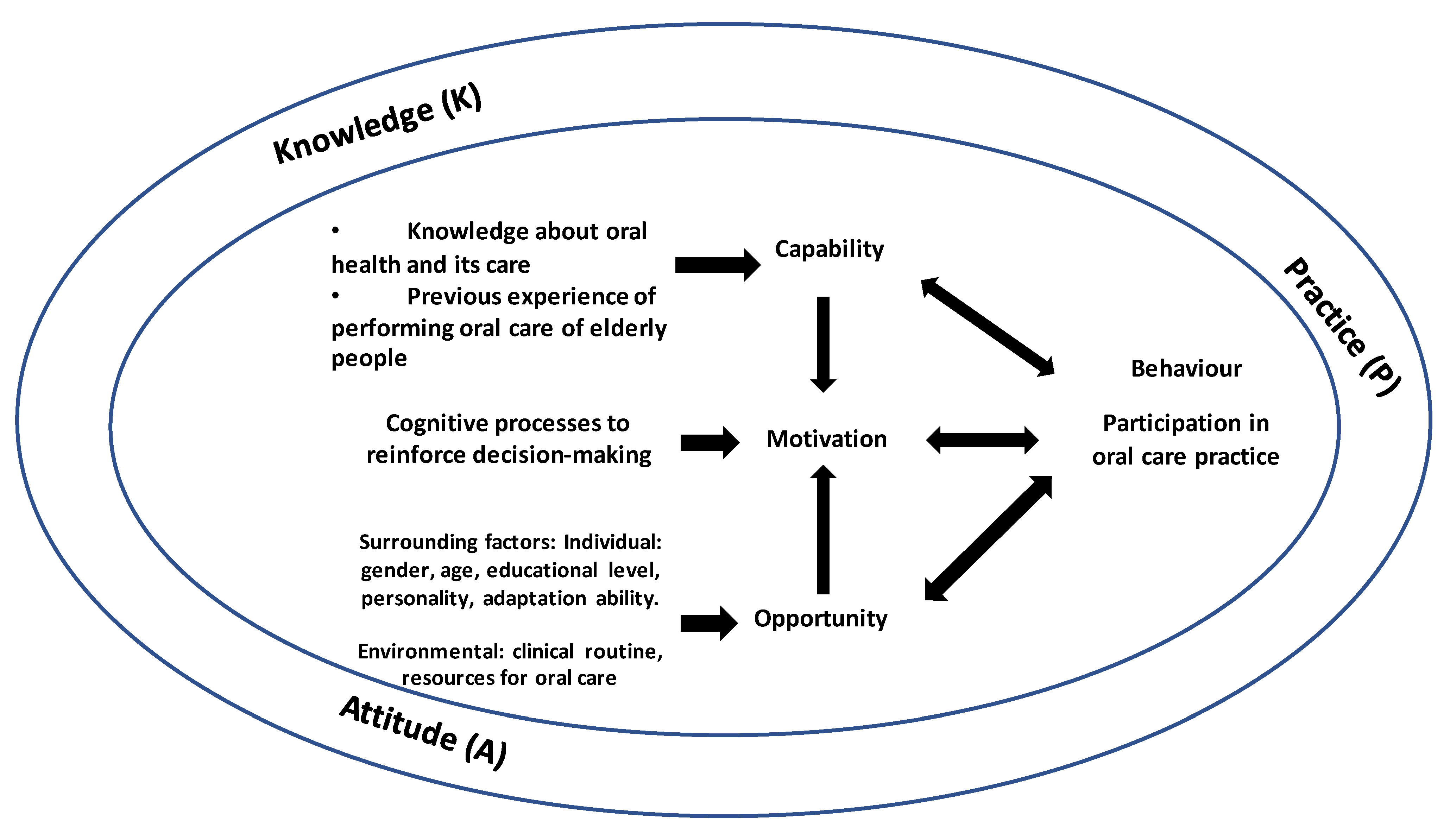
1.2. Operational Definition
1.3. Aims
2. Materials and Methods
2.1. Design
2.2. Literature Review
2.3. Consultation from Experts in Two Stages
2.4. Tool Translation and Interviews
2.5. Content Validity
2.6. A Pilot Study
2.7. Ethical Considerations
3. Results
3.1. Content and Domain Specification and Item Generation
3.2. Expert Review in Two Stages and CVI Results
3.3. Tool Refinement
3.4. A Pilot Study
4. Discussion
Strengths and Weaknesses
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Oral Health. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/oral-health (accessed on 18 January 2021).
- Gao, S.S.; Chen, K.J.; Duangthip, D.; Lo, E.C.M.; Chu, C.H. Oral health care in Hong Kong. Healthcare 2018, 6, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopcraft, M.S.; Morgan, M.V.; Satur, J.G.; Wright, C.; Darby, I.B. Oral hygiene and periodontal disease in Victorian nursing homes. Gerodontology 2012, 29, e220–e228. [Google Scholar] [CrossRef]
- Li, X.L.; Liu, M.Y.; Cheng, L.; Zhu, H.F.; Shang, S.H.; Cui, D. Impact of comprehensive health education on oral care knowledge, attitude and practice in the elderly in long-term care institutions. SJS 2018, 27, 181–184. [Google Scholar]
- Lin, H.C.; Wong, M.C.M.; Wang, Z.J.; Lo, E.C.M. Oral health knowledge, attitudes, and practices of Chinese Adults. J. Dent. Res. 2001, 80, 1466–1470. [Google Scholar] [CrossRef]
- Chalmers, J.; Pearson, A. Oral hygiene care for residents with dementia: A literature review. JAN 2005, 52, 410–419. [Google Scholar] [CrossRef]
- Zhu, L.; Petersen, P.E.; Wang, H.Y.; Bian, J.Y.; Zhang, B.X. Oral Health Knowledge, Attitudes and Behaviour of Adults in China. Int. Dent. J. 2005, 55, 231–241. [Google Scholar] [CrossRef]
- Zuluaga, D.J.M.; Ferreira, J.; Montoya, J.A.; Willumsen, T. Oral health in institutionalised elderly people in Oslo, Norway and its relationship with dependence and cognitive impairment. Gerodontology 2012, 29, 420–426. [Google Scholar] [CrossRef] [Green Version]
- Barrios, R.; Tsakos, G.; Garcia-Medina, B.; Martinez-Lara, I.; Bravo, M. Oral health-related quality of life and malnutrition in patients treated for oral cancer. Support. Care Cancer 2014, 22, 2927–2933. [Google Scholar] [CrossRef] [Green Version]
- Dharamsi, S.; Jivani, K.; Dean, C.; Wyatt, C. Oral care for frail elders: Knowledge, attitudes, and practices of long-term care staff. J. Dent. Educ. 2009, 73, 581–588. [Google Scholar] [CrossRef]
- Lo, E.C.; Luo, Y.; Dyson, J.E. Oral health status of institutionised elderly in Hong Kong. Community Dent. Health 2004, 21, 224–226. [Google Scholar]
- Wiener, R.C.; Meckstroth, R. The Oral Health Self-Care Behavior and Dental Attitudes among Nursing Home Personnel. J. Stud. Soc. Sci. 2014, 6, 1–12. [Google Scholar] [PubMed]
- Porter, J.; Ntouva, A.; Read, A.; Murdoch, M.; Ola, D.; Tsakos, G. The impact of oral health on the quality of life of nursing home residents. Health Qual. Life Outcomes 2015, 13, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atchison, K.A.; Dolan, T.A. Development of the geriatric oral health assessment index. J. Dent. Educ. 1990, 54, 680–687. [Google Scholar] [CrossRef]
- Maille, G.; Saliba-Serre, B.; Ferrandez, A.M.; Ruquet, M. Use of care and the oral health status of people aged 60 years and older in France: Results from the National Health and Disa-bility Survey. Clin. Interv. Aging 2017, 12, 1159–1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, M.F.F.; Ng, T.Y.Y.; Leung, W.K. Oral health and its associated factors among older institutionalized residents—A systematic review. IJERPH 2019, 16, 4132. [Google Scholar] [CrossRef] [Green Version]
- Arpin, S.; Brodeur, J.M.; Corbeil, P. Dental caries, problems perceived and use of services among institutionalized elderly in 3 regions of Quebec, Canada. JCDA 2008, 74, 807. [Google Scholar] [PubMed]
- Hearn, L.; Slack-Smith, L. Oral health care in residential aged care services: Barriers to engaging health-care providers. Aust. J. Prim. Health 2014, 21, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Stančić, I.; Petrović, M.; Popovac, A.; Vasović, M.; Despotović, N. Caregivers’ attitudes, knowledge and practices of oral care at nursing homes in Serbia. Vojnosanit. Pregl. 2016, 73, 668–673. [Google Scholar] [CrossRef]
- Vasudevan, V.; Rimmer, J.H.; Kviz, F. Development of the barriers to physical activity questionnaire for people with mobility impairments. Disabil. Health J. 2015, 8, 547–556. [Google Scholar] [CrossRef] [Green Version]
- Collins, D. Pretest survey instruments: An overview of cognitive methods. Qual. Life Res. 2003, 12, 229–238. [Google Scholar] [CrossRef]
- Paryag, A.; Rafeek, R.; Lewis, D. Knowledge, Attitudes, Beliefs and Training of Care Givers and Nursing Staff in Relation to Oral Care in Institutions for Older People in Trinidad. Int. J. Dent. Oral. Health 2016, 2. [Google Scholar] [CrossRef]
- Sinavarat, P.; Manosoontorn, S.; Anunmana, C. Knowledge, attitudes, and behavior towards oral health among a group of staff caring for elderly people in long-term care facilities in Bangkok, Thailand. M Dent. J. 2018, 38, 23–38. [Google Scholar]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterizing and designing behavior change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, T.S.; Cohen, M.Z.; Eriksen, L.; Cleeland, C. Content validity of selfreport measurement instruments: An illustration from the development of the brain tumor module of the M.D. Anderson symptom inventory. Oncol. Nurs. Forum. 2005, 32, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Zamanzadeh, V.; Ghahramanian, A.; Rassouli, M.; Abbaszadeh, A.; Alavi, H. Design and implementation content validity Study: Development of an instrument for measuring patient-centered communication. J. Caring Sci. 2015, 4, 165–178. [Google Scholar] [CrossRef] [PubMed]
- Yamada, J.; Stevens, B.; Sidani, S.; Watt-Watson, J.; De Silva, N. Content validity of a process evaluation checklist to measure intervention implementation fidelity of the EPIC intervention. Worldviews Evid. Based Nurs. 2010, 7, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Khanagar, S.; Naganandini, S.; Tuteja, J.S.; Naik, S.; Satish, G.; Divya, K.T. Improving oral hygiene in institutionalized elderly by educating their caretakers in Bangalore city, India: A randomized control trial. Can. Geriatr. J. 2015, 18, 136–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Unfer, B.; Braun, K.O.; De Oliveira Ferreira, A.C.; Ruat, G.R.; Batista, A.K. Challenges and barriers to quality oral care as perceived by caregivers in long-stay institutions in Brazil. Gerodontology 2012, 29, 324–330. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| No. | Item Questions | Interpretation | Recommendations |
|---|---|---|---|
| KQ1 | Oral health is directly related to general health. | Relevant | Included |
| KQ2 | Fluorides can help protect dental health. | Relevant | Included |
| KQ3 | Toothbrushing should be done in the morning after waking up and before bed at night every day. | Relevant | Rephrased |
| KQ4 | Sugary food, e.g., candy, increases the risk of tooth decay in residents. | Relevant | Included |
| KQ5 | Dental plaque can cause gum diseases and dental caries. | Relevant | Rephrased |
| KQ6 | Medication is one of the common reasons for dry mouth. | Relevant | Included |
| KQ7 | Dry mouth increases the risk of oral problems. | Relevant | Rephrased |
| KQ8 | Interdental cleaning aids, such as dental floss and interdental brush, can be used to clean the adjacent tooth surfaces. | Relevant | Included |
| KQ9 | Mouth rinsing can replace toothbrushing. | Relevant | Included |
| KQ10 | It is normal that the residents feel toothache and sores in their mouth. | Relevant | Included |
| KQ11 | Denture can totally replace natural teeth. | Relevant | Included |
| KQ12 | Denture should be taken out at night, cleaned and soaked. | Relevant | Included |
| KQ13 | It is normal to lose teeth as one gets old. | Relevant | Rephrased |
| KQ14 | Residents with full denture do not need to see a dentist. | Duplicatedwith KQ19 | Deleted |
| KQ15 | Unfit denture may indicate serious oral problems. | Relevant | Rephrased |
| KQ16 | Annual dental check is as important as body check. | Relevant | Included |
| KQ17 | Dental plaque does not form on denture. | Relevant | Rephrased |
| KQ18 | Residents with denture need to have regular dental check. | Duplicated with KQ 19 | Deleted |
| KQ19 | Residents with no teeth need to have dental check regularly. | Relevant | Included |
| KQ20 | The residents with full denture only need mouth rinsing. | Relevant | Included |
| KQ21 | Residents with tubing for feeding need oral care. | Relevant | Added |
| AQ1 | Daily oral care is an essential procedure. | Relevant | Rephrased |
| AQ2 | I will perform oral care for residents at least once in my shift. | Relevant | Moved to P (PQ15) |
| AQ3 | Independent residents should clean their dentures by themselves. | Relevant | Rephrased |
| AQ4 | When I am busy, I tend to ignore oral care to residents. | Relevant | Included |
| AQ5 | Oral care is an unpleasant task. | Relevant | Included |
| AQ6 | Oral care training for residents can improve my practice skills. | Relevant | Included |
| AQ7 | Oral care is not dentist’s duty. | Not essential | Deleted |
| AQ8 | I would perform other care procedures instead of oral care procedures to the residents. | Relevant | Rephrased and moved from P (PQ14) |
| AQ9 | It is normal if the gum bleeds while doing oral care to a resident. There is usually no need to follow up. | Relevant | Rephrased |
| AQ10 | I will only perform oral care to residents who are willing to open their mouth. | Relevant | Rephrased |
| AQ11 | Oral care to residents is my duty. | Relevant | Included |
| AQ12 | I will assist residents to perform oral care only if they have difficulty. | Relevant | Included |
| AQ13 | I am willing to spend time on oral care for each resident. | Relevant | Rephrased |
| AQ14 | If a resident requests to see a dentist, I am responsible to arrange for making corresponding arrangements. | Relevant | Included |
| AQ15 | The outreach dentist programme is helpful in assisting us to deliver oral care to the residents. | Relevant | Added |
| PQ1 | I will assist all residents in their toothbrushing or wiping their mouths at least once in my shift. | Relevant | Rephrased |
| PQ2 | I will not give junk foods to residents. | Not essential | Deleted |
| PQ3 | I will position the resident for oral care. | Not essential | Deleted |
| PQ4 | While I am performing oral care, I will brush the resident’s teeth. | Relevant | Rephrased |
| PQ5 | While I am performing oral care, I will brush the margin between teeth and gum. | Relevant | Included |
| PQ6 | While I am performing oral care, I will brush the resident’s tongue. | Relevant | Rephrased |
| PQ7 | I use interdental brush to clean adjacent tooth surfaces for residents with large space between teeth. | Relevant | Included |
| PQ8 | I will not perform oral care to residents if there is a risk of choking during the procedure. | Relevant | Rephrased |
| PQ9 | I always perform oral care according to the instruction of my unit head or the protocol at my workplace. | Relevant | Included |
| PQ10 | While performing oral care, I will do oral assessment for the resident. | Relevant | Included |
| PQ11 | I will refer residents with oral problems to a dentist. | Relevant | Included |
| PQ12 | I will inform my senior when I have found oral problems in the resident. | Relevant | Included |
| PQ13 | I can find adequate equipment to perform oral care to residents in my workplace. | Relevant | Included |
| PQ14 | I would perform other care procedures instead of oral care procedures to the residents. | Relevant | Moved from A (AQ8) |
| PQ15 | I will perform oral care for residents at least once in my shift. | Not essential | Moved from A (AQ2)but deleted |
| No. | Item Questions | I-CVI | Interpretation | Recommendations | CVR | Interpretation |
|---|---|---|---|---|---|---|
| KQ1 | Oral health is directly related to general health. | 1.00 | Relevant | Included | 1.00 | Included |
| KQ2 | Fluorides can help protect dental health. | 1.00 | Relevant | Included | 1.00 | Included |
| KQ3 | Toothbrushing should be done in the morning after waking up and before bed at night every day. | 1.00 | Relevant | Included | 1.00 | Included |
| KQ4 | Sugary food, e.g., candy, increases the risk of tooth decay in residents. | 1.00 | Relevant | Rephrased | 1.00 | Included |
| KQ5 | Dental plaque can cause gum diseases and dental caries. | 1.00 | Relevant | Included | 1.00 | Included |
| KQ6 | Medication is one of the common reasons for dry mouth. | 1.00 | Relevant | Included | 1.00 | Included |
| KQ7 | Dry mouth increases the risk of oral problems. | 1.00 | Relevant | Rephrased | 1.00 | Included |
| KQ8 | Interdental cleaning aids, such as dental floss and interdental brush, can be used to clean the adjacent tooth surfaces. | 1.00 | Relevant | Included | 1.00 | Included |
| KQ9 | Mouth rinsing can replace toothbrushing. | 1.00 | Relevant | Rephrased | 1.00 | Included |
| KQ10 | It is normal that the residents feel toothache and sores in their mouth. | 1.00 | Relevant | Included | 1.00 | Included |
| KQ11 | Denture can totally replace natural teeth. | 1.00 | Relevant | Included | 1.00 | Included |
| KQ12 | Denture should be taken out at night, cleaned and soaked. | 1.00 | Relevant | Included | 1.00 | Included |
| KQ13 | It is normal to lose teeth as one gets old. | 1.00 | Relevant | Included | 1.00 | Included |
| KQ15 | Unfit denture may indicate serious oral problems. | 1.00 | Relevant | Included | 1.00 | Included |
| KQ16 | Annual dental check is as important as body check. | 1.00 | Relevant | Included | 1.00 | Included |
| KQ17 | Dental plaque does not form on denture. | 1.00 | Relevant | Included | 1.00 | Included |
| KQ19 | Residents with no teeth need to have dental check regularly. | 1.00 | Relevant | Included | 1.00 | Included |
| KQ20 | The residents with full denture only need mouth rinsing. | 1.00 | Relevant | Included | 1.00 | Included |
| KQ21 | Residents with tubing for feeding need oral care. | 1.00 | Relevant | Included | 1.00 | Included |
| AQ1 | Daily oral care is an essential procedure. | 1.00 | Relevant | Added | 1.00 | Included |
| AQ3 | Independent residents should clean their dentures by themselves. | 1.00 | Relevant | Rephrased | 1.00 | Included |
| AQ4 | When I am busy, I tend to ignore oral care to residents. | 1.00 | Relevant | Included | 1.00 | Included |
| AQ5 | Oral care is an unpleasant task. | 1.00 | Relevant | Included | 1.00 | Included |
| AQ7 | Oral care training for residents can improve my practice skills. | 1.00 | Relevant | Included | 1.00 | Included |
| AQ8 | I would perform other care procedures instead of oral care procedures to the residents. | 1.00 | Relevant | Included | 1.00 | Included |
| AQ9 | It is normal if the gum bleeds while doing oral care to a resident. There is usually no need to follow up. | 1.00 | Relevant | Included | 1.00 | Included |
| AQ10 | I will only perform oral care to residents who are willing to open their mouth. | 1.00 | Relevant | Included | 1.00 | Included |
| AQ11 | Oral care to residents is my duty. | 1.00 | Relevant | Rephrased | 1.00 | Included |
| AQ12 | I will assist residents to perform oral care only if they have difficulty. | 1.00 | Relevant | Included | 1.00 | Included |
| AQ13 | I am willing to spend time on oral care for each resident. | 1.00 | Relevant | Added | 1.00 | Included |
| AQ14 | If a resident requests to see a dentist, I am responsible to arrange for making corresponding arrangements. | 1.00 | Relevant | Included | 1.00 | Included |
| AQ15 | The outreach dentist programme is helpful in assisting us to deliver oral care to the residents. | 1.00 | Relevant | Included | 1.00 | Included |
| PQ1 | I will assist all residents in their toothbrushing or wiping their mouths at least once in my shift. | 1.00 | Relevant | Included | 1.00 | Included |
| PQ4 | While I am performing oral care, I will brush the resident’s teeth. | 1.00 | Relevant | Included | 1.00 | Included |
| PQ5 | While I am performing oral care, I will brush the margin between teeth and gum. | 1.00 | Relevant | Included | 1.00 | Included |
| PQ6 | While I am performing oral care, I will brush the resident’s tongue. | 0.80 | Relevant | Included | 0.71 | Included |
| PQ7 | I use interdental brush to clean adjacent tooth surfaces for residents with large space between teeth. | 1.00 | Relevant | Included | 1.00 | Included |
| PQ8 | I will not perform oral care to residents if there is a risk of choking during the procedure. | 1.00 | Relevant | Included | 1.00 | Included |
| PQ9 | I always perform oral care according to the instruction of my unit head or the protocol at my workplace. | 1.00 | Relevant | Included | 1.00 | Included |
| PQ10 | While performing oral care, I will do oral assessment for the resident. | 1.00 | Relevant | Included | 1.00 | Included |
| PQ11 | I will refer residents with oral problems to a dentist. | 0.80 | Relevant | Included | 0.71 | Included |
| PQ12 | I will inform my senior when I have found oral problems in the resident. | 1.00 | Relevant | Included | 1.00 | Included |
| PQ13 | I can find adequate equipment to perform oral care to residents in my workplace. | 1.00 | Relevant | Included | 1.00 | Included |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, F.M.F. First Data in the Process of Validating a Tool to Evaluate Knowledge, Attitude, and Practice of Healthcare Providers in Oral Care of Institutionalized Elderly Residents: Content Validity, Reliability and Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 4145. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084145
Wong FMF. First Data in the Process of Validating a Tool to Evaluate Knowledge, Attitude, and Practice of Healthcare Providers in Oral Care of Institutionalized Elderly Residents: Content Validity, Reliability and Pilot Study. International Journal of Environmental Research and Public Health. 2021; 18(8):4145. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084145
Chicago/Turabian StyleWong, Florence M. F. 2021. "First Data in the Process of Validating a Tool to Evaluate Knowledge, Attitude, and Practice of Healthcare Providers in Oral Care of Institutionalized Elderly Residents: Content Validity, Reliability and Pilot Study" International Journal of Environmental Research and Public Health 18, no. 8: 4145. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084145