
Tired, Worried and Burned Out, but Still Resilient: A Cross-Sectional Study of Mental Health Workers in the UK during the COVID-19 Pandemic


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Questionnaire
- Socio-demographic: age, gender, ethnicity, home living situation, occupation, area of occupation (community, forensic, inpatient, COVID-19 ward etc.).
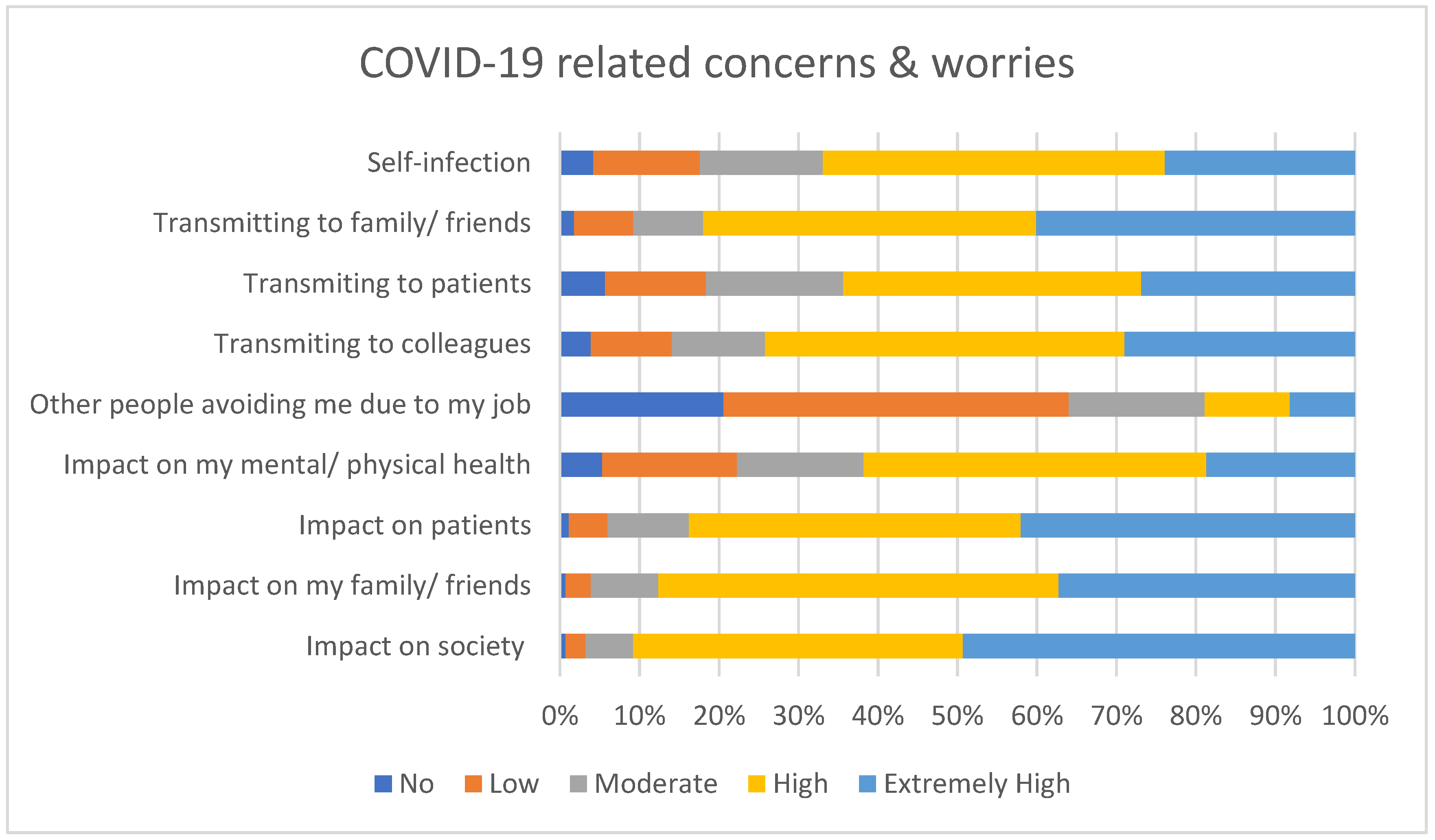
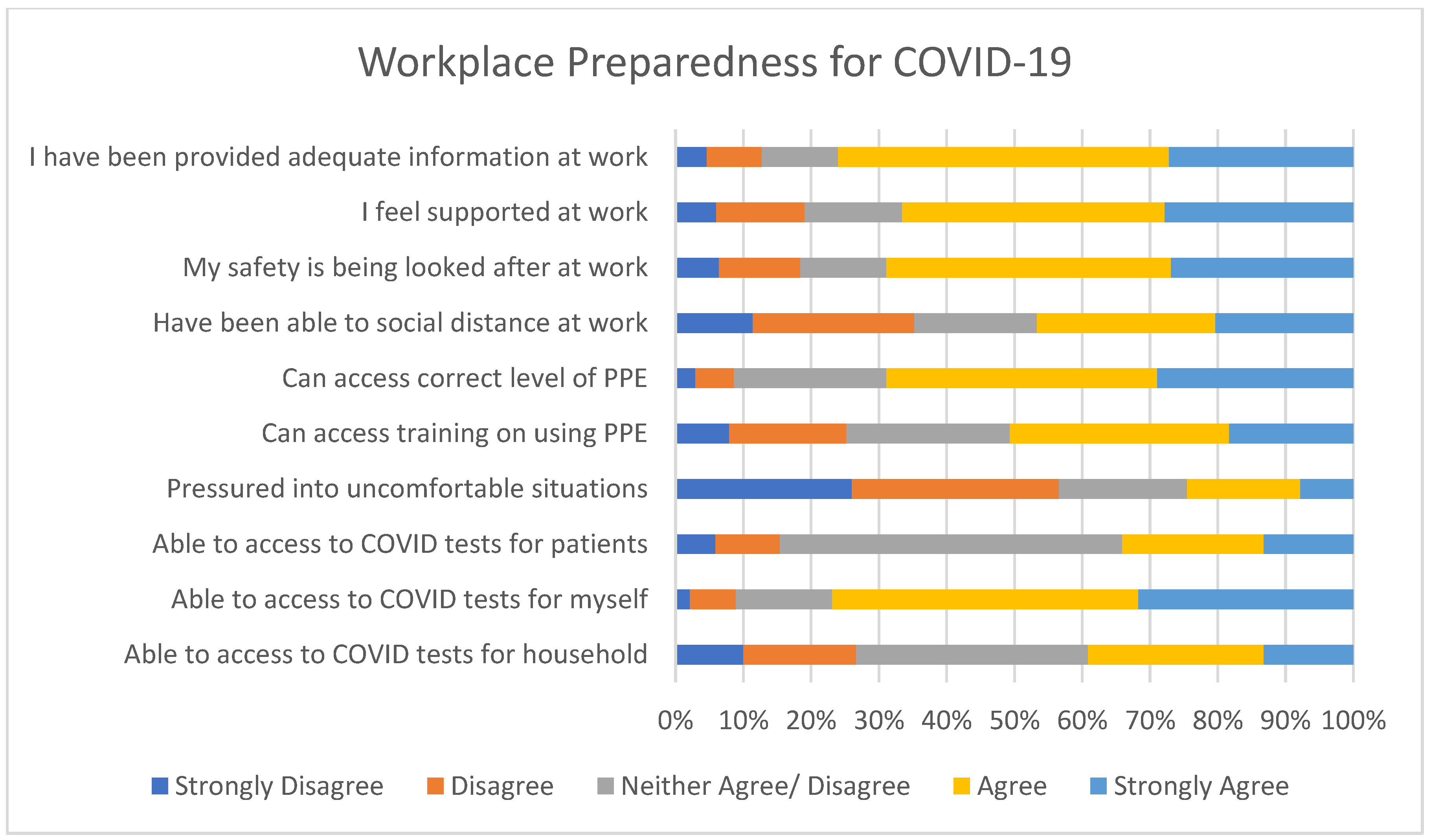
- Personal and work-related effects of COVID-19: Determining if participants are “high risk”, if they/members of their household had contracted the virus, if they have had to self-isolate or “shield”, how much face-to-face contact they have with patients (none, occasional, regular). How well supported and informed they are at work, worries about becoming infected or infecting others with COVID-19 and the consequences of this—these items were rated on a 5 = point Likert type scale; participants were asked how much they agreed with the statements presented, with answers ranging from strongly agree to strongly disagree.
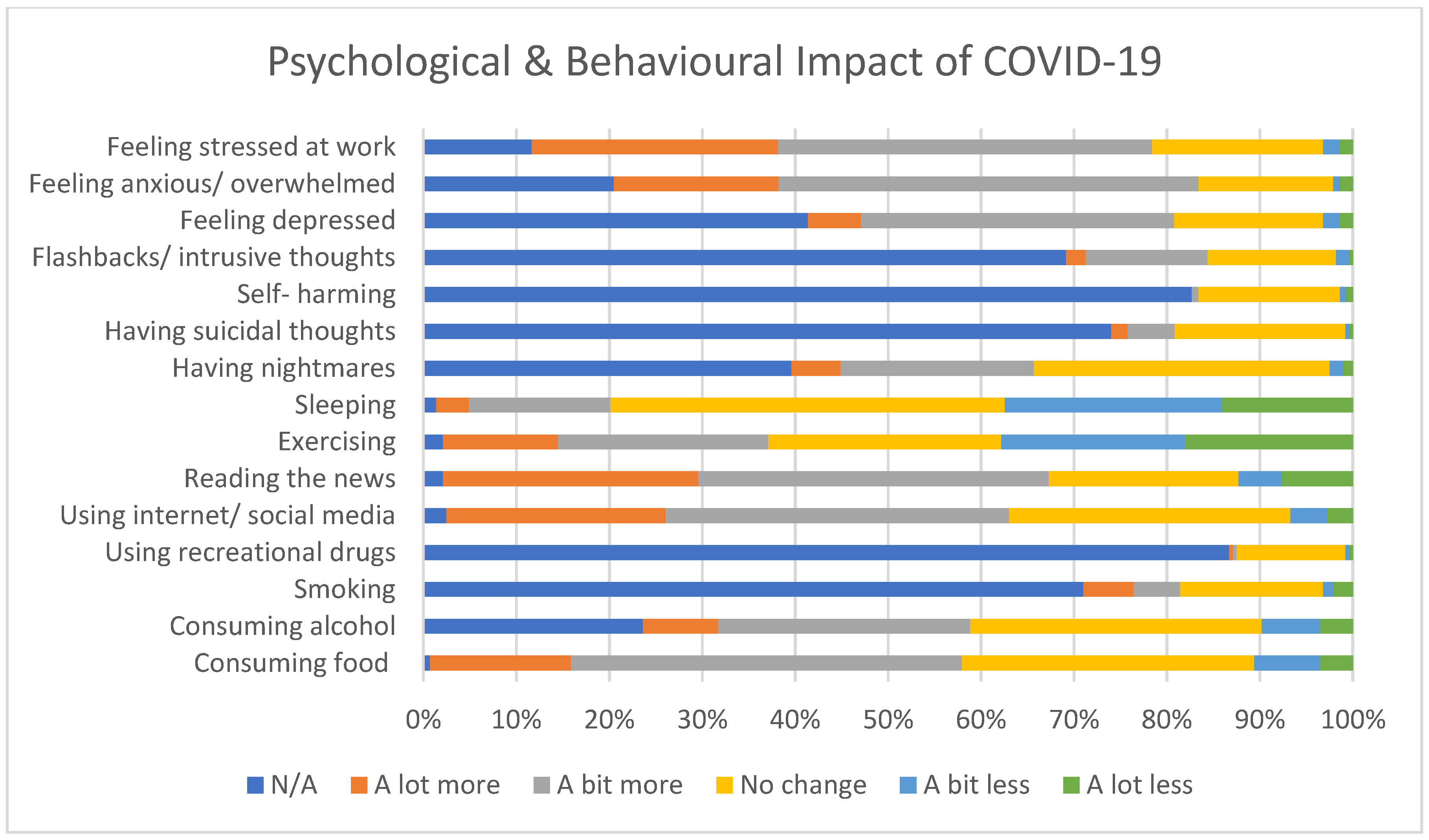
- Mental health and lifestyle-related effects of COVID-19: Pre-existing mental health diagnoses, changes to lifestyle (alcohol/tobacco/drug use, exercise), as well as psychological impact (perceived stress, sleep, nightmares, self-harm/suicidal thoughts), awareness and access of wellbeing support within the organization, and psychometric scales as detailed below.
2.3. Psychometric Scales
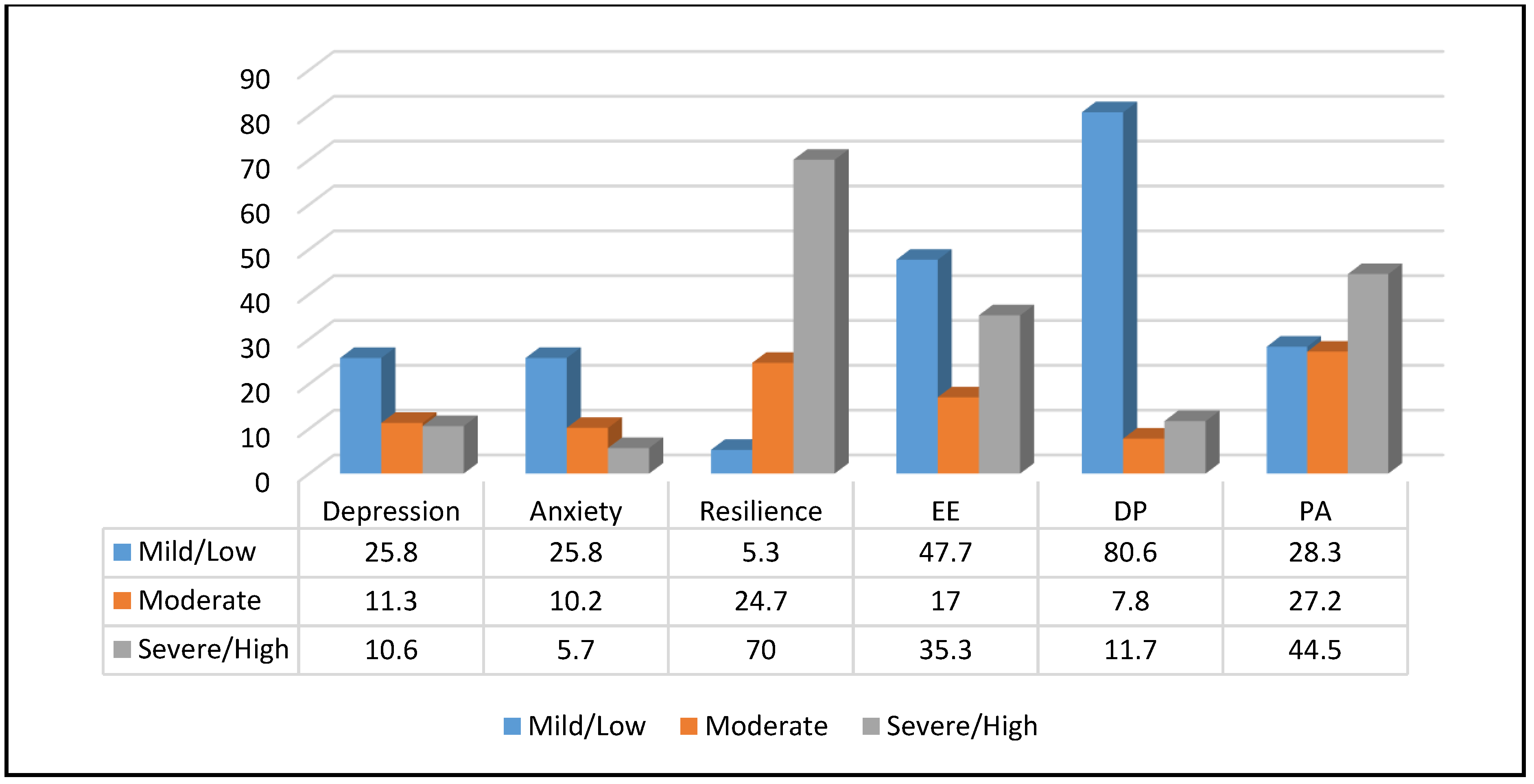
- Burnout: Maslach Burnout Inventory (MBI) is a 22-item questionnaire which assesses three dimensions: emotional exhaustion (EE, 9 items), depersonalization (DP, 5 items), and personal accomplishment (PA, 8 items) [26]. Higher scores in the EE and DP dimensions indicate more severe burnout, whereas higher scores in the PA subscale indicate less burnout. Cut-offs for moderate and severe EE were ≥17 and ≥27, for moderate and severe DP ≥ 7 and ≥ 13, and for moderate and severe reduced PA ≤ 38 and ≤21.
- Resilience Scale-14 (RS-14) is a modified, consistent, and validated version of the RS-25 questionnaire [27], consisting of 14 self-reported items which are measured on a 7-point Likert-type rating scale ranging from 1 (strongly disagree) to 7 (strongly agree). Scores range from 14 to 98 in total; <65 indicate “low resilience”, 65–81 “moderate resilience” and >81 “high levels of resilience” [28].
- Patient Health Questionnaire-9 (PHQ-9) is a nine-item self-administered screening tool for depression [29]. The scale investigates symptom severity over the past two weeks. Items are rated on a 4-point Likert type scale, ranging from 0 (not at all) to 3 (nearly every day). Total scores range between 0 and 27; scores of 0–4 are regarded as “minimal or none,” 5–9 as “mild,” 10–14 as “moderate,” 15–19 as “moderately severe,” and 20–27 as “severe”. The recognized cut-off point of 10 or greater corresponds to moderate to severe symptomatology indicative of a clinically significant problem.
- General Anxiety Disorder-7 (GAD-7) is a seven-item self-reported anxiety scale evaluating symptom severity in the preceding two weeks [30]. Items are rated on a 4-point Likert-type scale, ranging from 0 (not at all) to 3 (nearly every day). Total scores range between 0 and 21. Total scores of 0–4 were regarded as “not at all,” 5–9 as “mildly,” 10–14 as “moderately,” and 15 as “severely”. A cut-off point of 10 or greater is commonly used for case definition.
- Athens Insomnia Scale (AIS) is an eight-item self-reported questionnaire designed for quantifying sleep difficulty based on the ICD-10 criteria over the last month, which has shown good consistency, reliability, and validity [31]. The items are rated on a 4-point Likert-type scale, ranging from 0 (no problem or equivalent meaning) to 3 (severe problem or equivalent meaning). The commonly accepted cut off score is 6, with higher scores indicating more severe insomnia [32].
- A numerical fear rating scale (NFRS) was used to measure the level of fear in the study which has been reported to have good reliability and validity [33]. It is a segmented numeric version of the visual analogue scale (VAS) in which a respondent selects a whole number (0–10 integers) that best reflects the intensity of their fear. Higher scores indicate greater fear as follows: 0 for no fear, 1–3 for mild fear, 4–6 for moderate fear, 7–9 for severe fear, 10 for extreme fear.
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Psychometric Scales Outcomes
4. Discussion
4.1. Mood and Sleep
4.2. Lifestyle Changes
4.3. Burnout
4.4. Resilience
4.5. Strengths & Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Pneumonia of Unknown Cause-China. Available online: https://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-cause-china/en/ (accessed on 24 March 2021).
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- The New York Times. Coronavirus World Map: Tracking the Global Outbreak. Available online: https://www.nytimes.com/interactive/2020/world/coronavirus-maps.html (accessed on 16 April 2021).
- National AIDS Trust: HIV in the UK Statistics. Available online: https://www.nat.org.uk/about-hiv/hiv-statistics (accessed on 24 March 2021).
- Public Health England. Trends in HIV Testing, New Diagnoses and People Receiving HIV-Related Care in the United Kingdom: Data to the end of December 2019. Health Prot. Rep. 2020, 14, 3. [Google Scholar]
- Smith, R. Responding to global infectious disease outbreaks: Lessons from SARS on the role of risk perception, communication and management. Soc. Sci. Med. 2006, 63, 3113–3123. [Google Scholar] [CrossRef]
- Donaldson, L.; Rutter, P.; Ellis, B.; Greaves, F.; Mytton, O.; Pebody, R.; Yardley, I. Mortality from pandemic A/H1N1 2009 influenza in England: Public health surveillance study. BMJ 2009, 339, b5213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goulia, P.; Mantas, C.; Dimitroula, D.; Mantis, D.; Hyphantis, T. General hospital staff worries, perceived sufficiency of information and associated psychological distress during the A/H1N1 influenza pandemic. BMC Infect. Dis. 2010, 322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Jia, R.; Ayling, K.; Chalder, T.; Massey, A.; Broadbent, E.; Coupland, C.; Vedhara, K. Mental health in the UK during the COVID-19 pandemic: Cross-sectional analyses from a community cohort study. BMJ Open 2020, 10, e040620. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, R.C.; Wetherall, K.; Cleare, S.; McClelland, H.; Melson, A.J.; Niedzwiedz, C.L.; O’Carroll, R.E.; O’Connor, D.B.; Platt, S.; Scowcroft, E.; et al. Mental Health and Well-Being during the COVID-19 Pandemic: Longitudinal Analyses of Adults in the UK COVID-19 Mental Health & Wellbeing Study. Br. J. Psychiatry 2020, 1–8. [Google Scholar] [CrossRef]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Deng, J.; Zhou, F.; Hou, W.; Silver, Z.; Wong, C.Y.; Chang, O.; Huang, E.; Zuo, Q.K. The prevalence of depression, anxiety, and sleep disturbances in COVID-19 patients: A meta-analysis. Ann. N. Y. Acad. Sci. 2020, 1486, 90–111. [Google Scholar] [CrossRef]
- Choudhury, T.; Debski, M.; Wiper, A.; Abdelrahman, A.; Wild, S.; Chalil, S.; More, R.; Goode, G.; Patel, B.; Abdelaziz, H. COVID-19 Pandemic: Looking After the Mental Health of Our Healthcare Workers. J. Occup. Environ. Med. 2020, 62, e373–e376. [Google Scholar] [CrossRef]
- Wanigasooriya, K.; Palimar, P.; Naumann, D.N.; Ismail, K.; Fellows, J.L.; Logan, P.; Thompson, C.V.; Bermingham, H.; Beggs, A.D.; Ismail, T. Mental Health Symptoms in a Cohort of Hospital Healthcare Workers Following the First Peak of the COVID-19 Pandemic in the UK. BJPsych Open 2021, 7, e24. [Google Scholar] [CrossRef]
- Roberts, N.; McAloney-Kocaman, K.; Lippiett, K.; Ray, E.; Welch, L.; Kelly, C. Levels of resilience, anxiety and depression in nurses working in respiratory clinical areas during the COVID pandemic. Respir. Med. 2021, 176, 106219. [Google Scholar] [CrossRef]
- Vindrola-Padros, C.; Andrews, L.; Dowrick, A.; Djellouli, N.; Fillmore, H.; Gonzalez, E.B.; Javadi, D.; Lewis-Jackson, S.; Manby, L.; Mitchinson, L.; et al. Perceptions and experiences of healthcare workers during the COVID-19 pandemic in the UK. BMJ Open 2020, 10, e040503. [Google Scholar] [CrossRef]
- Nyashanu, M.; Pfende, F.; Ekpenyong, M. Exploring the challenges faced by frontline workers in health and social care amid the COVID-19 pandemic: Experiences of frontline workers in the English Midlands region, UK. J. Interprofessional Care 2020, 34, 655–661. [Google Scholar] [CrossRef] [PubMed]
- Papoutsi, G.; Giannakoulis, V.; Ntella, V.; Pappa, S.; Katsaounou, P. Global burden of COVID-19 pandemic on healthcare workers. ERJ Open Res. 2020, 6, 00195-2020. [Google Scholar] [CrossRef] [PubMed]
- Lemaire, J.; Wallace, J. Burnout among doctors. BMJ 2017, 358, j3360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orton, P.; Gray, D. Burnout in NHS staff. Lancet 2015, 385, 1831. [Google Scholar] [CrossRef]
- Sumner, R.; Kinsella, E. Grace under pressure: Resilience, burnout, and wellbeing in frontline workers in the UK and Republic of Ireland during the SARS-Cov-2 pandemic. Front. Psychol. 2021, 11, 576229. [Google Scholar] [CrossRef] [PubMed]
- West, C.; Dyrbye, L.; Erwin, P.; Shanafelt, T. Interventions to prevent and reduce physician burnout: A systematic review and meta-analysis. Lancet 2016, 388, 2272–2281. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.; Leiter, M. The Maslach Burnout Inventory Manual. In Evaluating Stress: A Book of Resources; Consulting Psychologists Press: Palo Alto, CA, USA, 1997; pp. 191–218. [Google Scholar]
- Wagnild, G.; Young, H. Development and psychometric evaluation of the Resilience Scale. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar]
- Wagnild, G. The Resilience Scale User’s Guide for the US English Version of the Resilience Scale and the 14-Item Resilience Scale (RS-14); The Resilience Centre: Worden, MT, USA, 2009; pp. 26–33. [Google Scholar]
- Kroenke, K.; Spitzer, R.; Williams, J. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.; Kroenke, K.; Williams, J.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soldatos, C.; Dikeos, D.; Paparrigopoulos, T. Athens Insomnia Scale: Validation of an instrument based on ICD-10 criteria. J. Psychosom. Res. 2000, 48, 555–560. [Google Scholar] [CrossRef]
- Voitsidis, P.; Gliatas, O.; Bairachtari, V.; Papadopoulou, K.; Papageorgiou, G.; Parlapani, E.; Syngelakis, M.; Holeva, V.; Diakogiannis, I. Insomnia during the COVID-19 pandemic in a Greek population. Psychiatry Res. 2020, 289, 113076. [Google Scholar] [CrossRef] [PubMed]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.; Pakpour, A.H. The fear of COVID-19 scale: Development and initial validation. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Dreary, I.; Agius, R.; Sadler, A. Personality and Stress in Consultant Psychiatrists. Int. J. Soc. Psychiatry 1996, 42, 112–123. [Google Scholar] [CrossRef]
- Kumar, S.; Hatcher, S.; Huggard, P. Burnout in Psychiatrists: An Etiological Model. Int. J. Psychiatry Med. 2005, 35, 405–416. [Google Scholar] [CrossRef]
- Firth-Cozens, J. Improving the Health of Psychiatrists. Adv. Psychiatr. Treat. 2007, 13, 161–168. [Google Scholar] [CrossRef] [Green Version]
- Di Filippo, P.; Attanasi, M.; Dodi, G.; Porreca, A.; Raso, M.; Di Pillo, S.; Chiarelli, F. A Survey on Mental Health Impact Caused by COVID-19 Pandemic in Italian Pediatric Healthcare Workers. 2020. preprint available at Research Square. [Google Scholar] [CrossRef]
- Pappa, S.; Athanasiou, N.; Sakkas, N.; Patrinos, S.; Sakka, E.; Barmparessou, Z.; Tsikrika, S.; Adraktas, A.; Pataka, A.; Migdalis, I.; et al. From Recession to Depression? Prevalence and Correlates of Depression, Anxiety, Traumatic Stress and Burnout in Healthcare Workers during the COVID-19 Pandemic in Greece: A Multi-Center, Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 2390. [Google Scholar] [CrossRef]
- Pappa, S.; Giannakoulis, V.; Papoutsi, E.; Katsaounou, P. Author reply–Letter to the editor “The challenges of quantifying the psychological burden of COVID-19 on healthcare workers”. Brain Behav. Immun. 2020, 92, 209–210. [Google Scholar] [CrossRef]
- Shevlin, M.; McBride, O.; Murphy, J.; Miller, J.G.; Hartman, T.K.; Levita, L.; Mason, L.; Martinez, A.P.; McKay, R.; Stocks, T.V.A.; et al. Anxiety, Depression, Traumatic Stress and COVID-19-Related Anxiety in the UK General Population during the COVID-19 Pandemic. BJPsych Open 2020, 6, e125. [Google Scholar] [CrossRef]
- Muller, A.; Hafstad, E.; Himmels, J.; Smedslund, G.; Flottorp, S.; Stensland, S.; Stroobants, S.; Van de Velde, S.; Vist, G. The mental health impact of the covid-19 pandemic on healthcare workers, and interventions to help them: A rapid systematic review. Psychiatry Res. 2020, 293, 113441. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Xie, L.; Xu, Y.; Yu, S.; Yao, B.; Xiang, D. Sleep disturbances among medical workers during the outbreak of COVID-2019. Occup. Med. 2020, 70, 364–369. [Google Scholar] [CrossRef]
- Zhang, C.; Yang, L.; Liu, S.; Ma, S.; Wang, Y.; Cai, Z.; Du, H.; Li, R.; Kang, L.; Su, M.; et al. Survey of Insomnia and Related Social Psychological Factors Among Medical Staff Involved in the 2019 Novel Coronavirus Disease Outbreak. Front. Psychiatry 2020, 11, 306. [Google Scholar] [CrossRef] [Green Version]
- Stubbs, B.; Veronese, N.; Vancampfort, D.; Prina, A.M.; Lin, P.Y.; Tseng, P.T.; Evangelou, E.; Solmi, M.; Kohler, C.; Carvalho, A.F.; et al. Perceived stress and smoking across 41 countries: A global perspective across Europe, Africa, Asia and the Americas. Sci. Rep. 2017, 7, 7597. [Google Scholar] [CrossRef] [PubMed]
- Grogan, S.; Walker, L.; McChesney, G.; Gee, I.; Gough, B.; Cordero, M. How has COVID-19 lockdown impacted smoking? A thematic analysis of written accounts from UK smokers. Psychol. Health 2020, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Boyland, E.; Chisholm, A.; Harrold, J.; Maloney, N.; Marty, L.; Mead, B.; Noonan, R.; Hardman, C. Obesity, eating behavior and physical activity during COVID-19 lockdown: A study of UK adults. Appetite 2021, 156, 104853. [Google Scholar] [CrossRef] [PubMed]
- Niedzwiedz, C.L.; Green, M.J.; Benzeval, M.; Campbell, D.; Craig, P.; Demou, E.; Leyland, A.; Pearce, A.; Thomson, R.; Whitley, E.; et al. Mental health and health behaviours before and during the initial phase of the COVID-19 lockdown: Longitudinal analyses of the UK Household Longitudinal Study. J. Epidemiol. Community Health 2021, 75, 224–231. [Google Scholar]
- Jacka, F.; Berk, M. Depression, diet and exercise. Med. J. Aust. 2013, 199, 21–23. [Google Scholar] [CrossRef] [PubMed]
- Gibson, E. The psychobiology of comfort eating implications for neuropharmacological interventions. Behav. Pharmacol. 2012, 23, 442–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herle, M.; Smith, A.; Bu, F.; Steptoe, A.; Fancourt, D. Trajectories of eating behavior during COVID-19 lockdown: Longitudinal analyses of 22,374 adults. Clin. Nutr. Espen. 2021, 42, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Imo, U. Burnout and psychiatric morbidity among doctors in the UK: A systematic literature review of prevalence and associated factors. BJPsych Bull. 2017, 41, 197–204. [Google Scholar] [CrossRef] [PubMed]
- BMA Covid-19 Tracker Survey. Available online: https://www.bma.org.uk/media/2315/bma-ppe-survey-results-for-wellbeing-april-2020.pdf (accessed on 27 March 2021).
- Giusti, E.M.; Pedroli, E.; D’Aniello, G.E.; Stramba Badiale, C.; Pietrabissa, G.; Manna, C.; Stramba Badiale, M.; Riva, G.; Castelnuovo, G.; Molinari, E. The Psychological Impact of the COVID-19 Outbreak on Health Professionals: A Cross-Sectional Study. Front. Psychol. 2020, 11, 1684. [Google Scholar] [CrossRef]
- Scott, G. Goodwill in the NHS is a one-way street. Nurs. Stand. 2015, 29, 3. [Google Scholar] [CrossRef] [Green Version]
- Jones-Berry, S. Nurses’ goodwill keeping NHS afloat, RCN warns. Nurs. Stand. 2017, 31, 9. [Google Scholar] [CrossRef] [PubMed]
- Hiam, L.; McKee, M.; Dorling, D. The NHS has Been Run on the Goodwill of Its Staff for too Long. 2020. Available online: https://0-blogs-bmj-com.brum.beds.ac.uk/bmj/2020/04/07/the-nhs-has-been-run-on-the-goodwill-of-its-staff-for-too-long/ (accessed on 27 March 2021).
- West, C.; Dyrbye, L.; Shanafelt, T. Physician burnout: Contributors, consequences and solutions. J. Intern. Med. 2018, 283, 516–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montemurro, N. The emotional impact of COVID-19: From medical staff to common people. Brain Behav. Immun. 2020, 87, 23–24. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.; Noseworthy, J. Executive Leadership and Physician Well-being: Nine Organizational Strategies to Promote Engagement and Reduce Burnout. Mayo Clin. Proc. 2017, 92, 129–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofmeyer, A.; Taylor, R.; Kennedy, K. Fostering compassion and reducing burnout: How can health system leaders respond in the Covid-19 pandemic and beyond? Nurse Educ. Today 2020, 94, 104502. [Google Scholar] [CrossRef] [PubMed]
- Medscape: ‘Death by 1000 Cuts’: Medscape National Physician Burnout & Suicide Report 2021. Available online: https://www.medscape.com/slideshow/2021-lifestyle-burnout-6013456 (accessed on 27 March 2021).
- BJGP Life: Pandemic Burnout in Frontline Heathcare Workers: Can Meditation Help? 2020. Available online: https://bjgplife.com/2020/11/17/pandemic-burnout-in-frontline-healthcare-workers-can-meditation-help/ (accessed on 26 March 2021).
- McCann, C.; Beddoe, E.; McCormick, K.; Huggard, P.; Kedge, S.; Adamson, C.; Huggard, J. Resilience in the health professions: A review of recent literature. Int. J. Wellbeing 2013, 3, 60–81. [Google Scholar] [CrossRef]
- Sull, A.; Harland, N.; Moore, A. Resilience of health-care workers in the UK; a cross-sectional survey. J. Occup. Med. Toxicol. 2015, 10, 20. [Google Scholar] [CrossRef] [Green Version]
- Balme, E.; Gerada, C.; Page, L. Doctors need to be supported, not trained in resilience. BMJ 2015, 351, 4709. [Google Scholar] [CrossRef]
- Howe, A.; Smajdor, A.; Stockl, A. Towards an understanding of resilience and its relevance to medical training. Med. Educ. 2012, 46, 349–356. [Google Scholar] [CrossRef]
- Jackson, D.; Firtko, A.; Edenborough, M. Personal resilience as a strategy for surviving and thriving in the face of workplace adversity: A literature review. J. Adv. Nurs. 2007, 60, 1–9. [Google Scholar] [CrossRef]
- DeChant, P.; Acs, A.; Rhee, K.; Boulanger, T.; Snowdon, J.; Tutty, M.; Sinsky, C.; Thomas Craig, K. Effect of Organization-Directed Workplace Interventions on Physician Burnout: A Systematic Review. Mayo Clin. Proc. Innov. Qual. Outcomes 2019, 3, 384–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillespie, B.; Chaboyer, W.; Wallis, M. Development of a theoretically derived model of resilience through concept analysis. Contemp. Nurse 2007, 25, 124–135. [Google Scholar] [CrossRef]
- Denkova, E.; Zanesco, A.; Rogers, S.; Jha, A. Is resilience trainable? An initial study comparing mindfulness and relaxation training in firefighters. Psychiatry Res. 2020, 285, 112794. [Google Scholar] [CrossRef]
- Tregoning, C.; Remington, S.; Agius, S. Facing change: Developing resilience for staff, associate specialist, and specialty doctors. BMJ 2014, 348, 251. [Google Scholar] [CrossRef]
- GOV.uk: Ethnicity Facts and Figures. Available online: https://www.ethnicity-facts-figures.service.gov.uk/workforce-and-business/workforce-diversity/nhs-workforce/latest (accessed on 29 March 2021).
- Rossitto, S.; Tsai, D. Annual Workforce Equality and Diversity Report 2016/2017; Imperial College Healthcare NHS Trust: London, UK, 2017. [Google Scholar]
- Korkeila, K.; Suominen, S.; Ahvenainen, J.; Ojanlatva, A.; Rautava, P.; Helenius, H.; Koskenvuo, M. Non-response and related factors in a nation-wide health survey. Eur. J. Epidemiol. 2001, 17, 991–999. [Google Scholar] [CrossRef] [PubMed]
- Sigmon, S.T.; Pells, J.J.; Boulard, N.E.; Whitcomb-Smith, S.; Edenfield, T.M.; Hermann, B.A.; LaMattina, S.M.; Schartel, J.G.; Kubik, E. Gender Differences in Self-Reports of Depression: The Response Bias Hypothesis Revisited. Sex Roles 2005, 53, 401–411. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | N | % |
|---|---|---|
| Age | ||
| 16–20 | 1 | 0.4 |
| 21–30 | 64 | 22.6 |
| 31–40 | 57 | 20.1 |
| 41–50 | 71 | 25.1 |
| 51–65 | 83 | 29.3 |
| 66+ | 7 | 2.5 |
| Gender | ||
| Male | 78 | 26.6 |
| Female | 201 | 71 |
| Prefer not to say | 4 | 1.4 |
| Race and Ethnicity | ||
| All White backgrounds | 189 | 66.8 |
| All Black backgrounds | 27 | 9.5 |
| All Asian backgrounds | 41 | 14.5 |
| Mixed backgrounds | 11 | 3.9 |
| Other | 15 | 5.3 |
| Occupation | ||
| Doctors | 45 | 16 |
| Nurses | 46 | 16.4 |
| Psychologists | 52 | 18.5 |
| Health Care Assistant | 21 | 7.5 |
| Administrative/ Management | 41 | 14.6 |
| Other | 76 | 27 |
| High-risk group for COVID-19 | ||
| Yes | 68 | 24 |
| No | 215 | 76 |
| Current Contact with Patients | ||
| No | 104 | 39.2 |
| Yes, occasionally | 72 | 27.2 |
| Yes, regularly | 89 | 33.6 |
| Pre-existing Mental Health Condition | ||
| Yes | 60 | 78.8 |
| No | 223 | 21.2 |
| Adequacy of support offered at work | ||
| Yes | 104 | 37.3 |
| Yes, to some extent | 115 | 41.2 |
| No | 60 | 21.5 |
| Insomnia | Emotional Exhaustion | ||
|---|---|---|---|
| No Insomnia | 48.4% | Low | 47.7% |
| Insomnia | 51.6% | Moderate | 17% |
| High | 35.3% | ||
| Depression | Depersonalisation | ||
| Mild | 25.8% | Low | 80.6% |
| Moderate | 11.3% | Moderate | 7.8% |
| Severe | 10.6% | High | 11.7% |
| Anxiety | Personal Accomplishment | ||
| Mild | 25.8% | Low | 28.3% |
| Moderate | 10.2% | Moderate | 27.2% |
| Severe | 5.7% | High | 44.5% |
| Resilience | |||
| Low | 5.3% | ||
| Moderate | 24.7% | ||
| High | 70% | ||
| Domain | Mean ± Std. Error | df | P-Value | Cohen’s d | ||
|---|---|---|---|---|---|---|
| Male | Female | t | ||||
| PHQ-9 | 4.72 ± 0.70 | 6.31 ± 0.40 | 1.98 | 129.68 | 0.05 * | 0.27 |
| GAD-7 | 3.82 ± 0.57 | 5.06 ± 0.34 | 1.87 | 135.50 | 0.064 | 0.25 |
| AIS | 5.95 ± 0.63 | 7.11 ± 0.40 | 1.57 | 139.08 | 0.119 | 0.21 |
| MBI_EE | 18.35 ±1.47 | 22.38 ± 0.94 | 2.32 | 143.66 | 0.022 * | 0.31 |
| MBI_PA | 31.15 ± 1.29 | 32.81 ± 0.70 | 1.13 | 124.66 | 0.262 | 0.16 |
| MBI_DE | 4.32 ± 0.54 | 3.61 ± 0.31 | −1.14 | 130.77 | 0.709 | 0.15 |
| RS_14 | 83.05 ± 1.34 | 83.65 ± 0.72 | 0.40 | 123.26 | 0.694 | 0.05 |
| No Pre-existing MH diagnosis | Pre-existing MH diagnosis | t | df | p-Value | Cohen’s d | |
| PHQ-9 | 4.75 ± 0.33 | 5.01 ± 0.39 | −5.38 | 75.81 | <0.001 * | 0.85 |
| GAD-7 | 3.81 ± 0.28 | 8.08 ± 0.74 | −5.38 | 77.10 | <0.001 * | 0.85 |
| AIS | 5.98 ± 0.34 | 9.72 ± 0.78 | −4.40 | 83.03 | <0.001 * | 0.67 |
| MBI_EE | 20.12 ± 0.89 | 24.98 ± 1.67 | −2.57 | 95.18 | 0.012 * | 0.37 |
| MBI_PA | 32.01 ± 0.71 | 33.83 ± 1.19 | −1.31 | 104.54 | 0.192 | 0.18 |
| MBI_DE | 3.53 ± 0.29 | 4.68 ± 0.62 | −1.69 | 87.75 | 0.094 | 0.25 |
| RS_14 | 84.44 ± 0.68 | 80.07 ± 1.54 | 2.60 | 83.20 | 0.011 * | 0.39 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pappa, S.; Barnett, J.; Berges, I.; Sakkas, N. Tired, Worried and Burned Out, but Still Resilient: A Cross-Sectional Study of Mental Health Workers in the UK during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 4457. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094457
Pappa S, Barnett J, Berges I, Sakkas N. Tired, Worried and Burned Out, but Still Resilient: A Cross-Sectional Study of Mental Health Workers in the UK during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(9):4457. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094457
Chicago/Turabian StylePappa, Sofia, Joshua Barnett, Ines Berges, and Nikolaos Sakkas. 2021. "Tired, Worried and Burned Out, but Still Resilient: A Cross-Sectional Study of Mental Health Workers in the UK during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 9: 4457. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094457