
Psychological First Aid Training: A Scoping Review of Its Application, Outcomes and Implementation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Identifying the Research Question
2.2. Identifying Relevant Studies
2.3. Study Selection
2.4. Charting of Information and Data within the Included Studies
2.5. Collating, Summarising and Reporting Results
3. Result
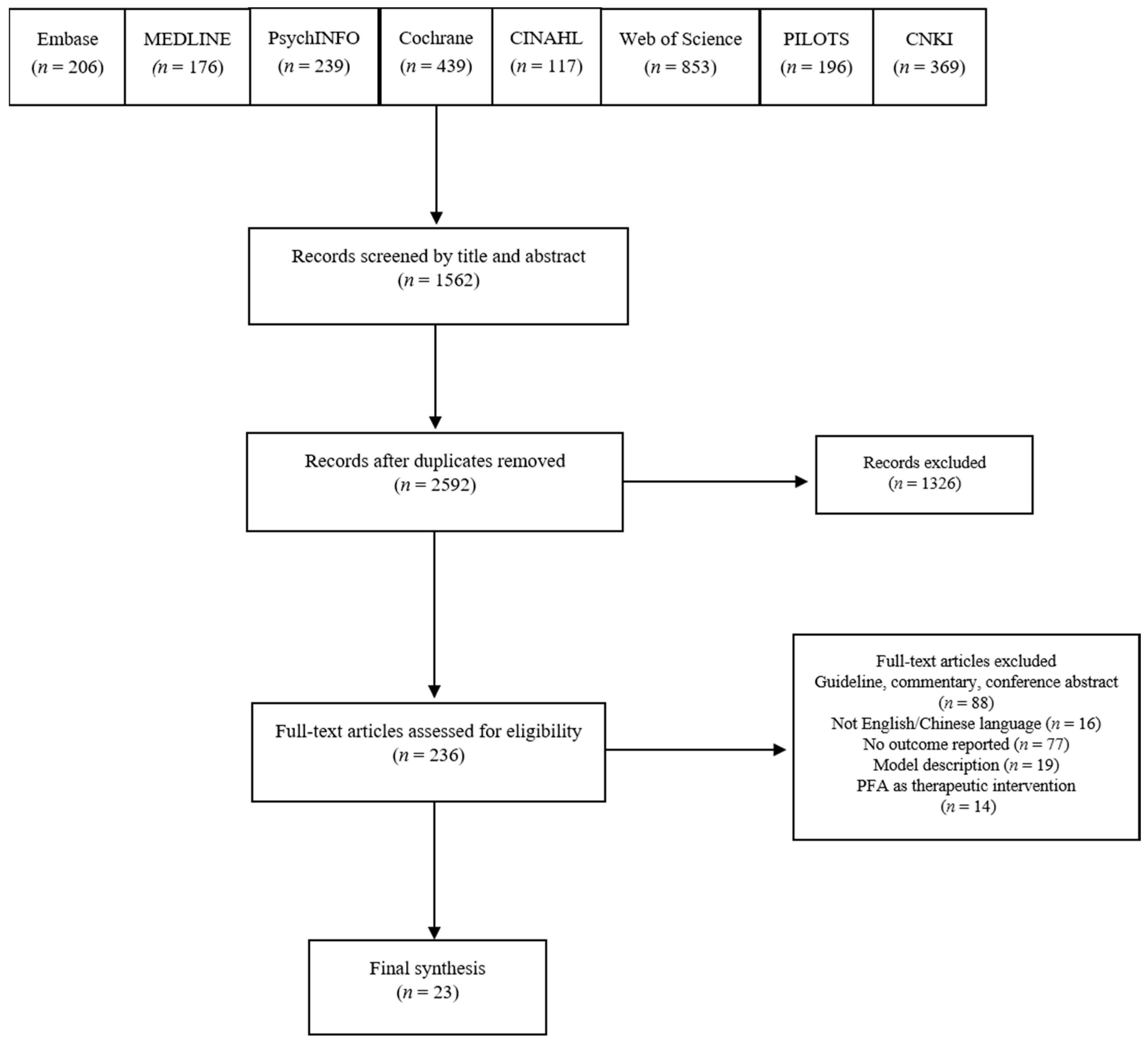
3.1. Study Selection
3.2. PFA Models
3.2.1. Psychological First Aid: Guide for Field Workers
3.2.2. Psychological First Aid: Field Operations Guide
3.2.3. The Johns Hopkins Guide to Psychological First Aid
3.2.4. Mixed Models
3.3. Characteristics of Included Studies
3.4. The Characteristics of PFA Training Delivery
3.4.1. Theory (Why?)
3.4.2. Material and Procedures (What?)
3.4.3. Training Provider (Who?)
3.4.4. Mechanism of Delivery and Location (How and Where?)
3.4.5. Training Schedule and Intensity (When and How Much?)
3.4.6. Adaptations (Tailoring)
3.4.7. Adherence and Fidelity (How Well)
3.5. Outcomes of PFA Training
3.5.1. Effect on Learning
3.5.2. Effect on Behaviour
3.5.3. Effect on Practice
3.5.4. Effect on Satisfaction
3.5.5. Effect on System Changes
3.6. PFA Training Implementation Barriers and Enablers
3.6.1. Potential Risks
3.6.2. Barriers and Enablers Factors to the PFA Training
4. Discussion
4.1. Lack Guidance on PFA Training Application and Adaptation
4.2. Significant Shortcomings in Reporting PFA Training Intervention
4.3. Unintended Potential Harms from Inappropriate Training Delivery
4.4. Limited Efforts in Evaluation of PFA Training
4.5. Less Defined Clear Outcomes for Evaluating the PFA Training
4.6. Implications for Research and Policy
- What are the ‘core’ and ‘adaptable periphery’ components of PFA?
- Is PFA training sufficient to avoid unintended harms and should trainees be given supervision whilst they learn to put training into practice?
- Is PFA training effective and at what levels and which population?
4.7. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Silver, R.C.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Bryant, R.A.; Litz, B. Mental Health Treatments in the Wake of Disaster. Ment. Health Disasters 2010, 321–335. [Google Scholar] [CrossRef]
- Greenberg, N.; Docherty, M.; Gnanapragasam, S.; Wessely, S. Managing mental health challenges faced by healthcare workers during covid-19 pandemic. BMJ 2020, 368, m1211. [Google Scholar] [CrossRef] [Green Version]
- Čartolovni, A.; Stolt, M.; Scott, P.A.; Suhonen, R. Moral injury in healthcare professionals: A scoping review and discussion. Nurs. Ethics 2021. [Google Scholar] [CrossRef]
- Policy Brief: COVID-19 and the Need for Action on Mental Health. Available online: https://unsdg.un.org/sites/default/files/2020-05/UN-Policy-Brief-COVID-19-and-mental-health.pdf (accessed on 12 December 2020).
- Psychological First Aid in Emergencies Training for Frontline Staff and Volunteers. Available online: https://www.gov.uk/government/news/psychological-first-aid-in-emergencies-training-for-frontline-staff-and-volunteers (accessed on 12 December 2020).
- Choong, T.C.; Chai, Y.C.; Huri, S.Z.; Nawawi, W.Z.W.; Ibrahim, N. Innovative psychological first aid (PFA) in the new normal for frontliners. Perspect. Psychiatr. Care 2020. [Google Scholar] [CrossRef]
- Daniel, B.; Hoch, P.; Ryan, V.G. A course in psychological first aid and prevention: A preliminary report. Am. J. Psychiatry 1945, 101, 629–634. [Google Scholar]
- Raphael, B. When Disaster Strikes; Basic Books: New York, NY, USA, 1986; p. 257. [Google Scholar]
- Church of Sweden. Psychological First Aid: Five Year Retrospective (2011–2016) Uppsala: Church of Sweden. 2018. Available online: https://www.svenskakyrkan.se/internationelltarbete/reports-policy-documents–and-positions-on-church-of-swedens-international-work (accessed on 12 December 2020).
- Shultz, J.M.; Forbes, D. Psychological first aid: Rapid proliferation and the search for evidence. Disaster Health 2014, 2, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Rose, S.C.; Bisson, J.; Churchill, R.; Wessely, S. Psychological debriefing for preventing post traumatic stress disorder (PTSD). Cochrane Database Syst. Rev. 2002. [Google Scholar] [CrossRef]
- Hobfoll, S.E.; Watson, P.; Bell, C.C.; Bryant, R.A.; Brymer, M.J.; Friedman, M.J.; Friedman, M.; Gersons, B.P.; De Jong, J.T.; Layne, C.M.; et al. Five Essential Elements of Immediate and Mid–Term Mass Trauma Intervention: Empirical Evidence. Psychiatry 2007, 70, 283–315. [Google Scholar] [CrossRef]
- World Health Organization. War Trauma Foundation and World Vision International. Psychological First Aid: Guide for Fieldworkers; WHO: Geneva, Switzerland, 2011; Available online: https://www.who.int/publications/i/item/9789241548205 (accessed on 12 December 2020).
- Everly, G.S.; Lating, J.M. The Johns Hopkins Guide to Psychological First Aid; JHU Press: Baltimore, MD, USA, 2017. [Google Scholar]
- Dieltjens, T.; Moonens, I.; Van Praet, K.; De Buck, E.; Vandekerckhove, P. A Systematic Literature Search on Psychological First Aid: Lack of Evidence to Develop Guidelines. PLoS ONE 2014, 9, e114714. [Google Scholar] [CrossRef] [PubMed]
- North, C.S.; Pfefferbaum, B. Mental health response to community disasters: A systematic review. JAMA 2013, 310, 507–518. [Google Scholar] [CrossRef]
- Fox, J.H.; Burkle, F.M.; Bass, J.; Pia, F.A.; Epstein, J.L.; Markenson, D. The effectiveness of psychological first aid as a disaster intervention tool: Eesearch analysis of peer-reviewed literature from 1990–2010. Disaster Med. Public Health Prep. 2012, 6, 247–252. [Google Scholar] [CrossRef]
- Ruzek, J.I.; Brymer, M.J.; Jacobs, A.K.; Layne, C.M.; Vernberg, E.M.; Watson, P.J. Psychological first aid. J. Ment. Health Couns. 2007, 29, 17–49. [Google Scholar] [CrossRef] [Green Version]
- Brymer, M.; Jacobs, A.; Layne, C.; Pynoos, R.; Ruzek, J.; Steinberg, A.; Vernberg, E.; Watson, P. Psychological First Aid: Field Operations Guide, 2nd ed.; 2006. Available online: https://www.nctsn.org/resources/psychological-first-aid-pfa-field-operations-guide-2nd-edition. (accessed on 12 December 2020).
- Vernberg, E.M.; Steinberg, A.M.; Jacobs, A.K.; Brymer, M.J.; Watson, P.J.; Osofsky, J.D.; Layne, C.M.; Pynoos, R.S.; Ruzek, J.I. Innovations in disaster mental health: Psychological first aid. Prof. Psychol. Res. Pr. 2008, 39, 381–388. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, G.A.; Gray, B.L.; Erickson, S.E.; Gonzalez, E.D.; Quevillon, R.P. Disaster Mental Health and Community-Based Psychological First Aid: Concepts and Education/Training. J. Clin. Psychol. 2016, 72, 1307–1317. [Google Scholar] [CrossRef] [PubMed]
- Roudini, J.; Khankeh, H.R.; Witruk, E. Disaster mental health preparedness in the community: A systematic review study. Health Psychol. Open 2017, 4, 2055102917711307. [Google Scholar] [CrossRef]
- McCabe, O.L.; Everly, G.S.; Brown, L.M.; Wendelboe, A.M.; Hamid, N.H.A.; Tallchief, V.L.; Links, J.M. Psychological First Aid: A Consensus-Derived, Empirically Supported, Competency-Based Training Model. Am. J. Public Health 2014, 104, 621–628. [Google Scholar] [CrossRef]
- COVID-19: Psychological First Aid. Available online: https://www.futurelearn.com/courses/psychological-first-aid-covid-19. (accessed on 12 December 2020).
- Psychological First Aid. Available online: https://www.coursera.org/learn/psychological-first-aid (accessed on 12 December 2020).
- Dignity in Mental Health. Psychological & Mental Health First Aid for All. Available online: https://www.who.int/mental_health/world-mental-health-day/paper_wfmh_2016.pdf (accessed on 12 December 2020).
- Gispen, F.; Wu, A.W. Psychological first aid: CPR for mental health crises in healthcare. J. Patient Saf. Risk Manag. 2018, 23, 51–53. [Google Scholar] [CrossRef] [Green Version]
- Everly, G.S., Jr. Psychological first aid to support healthcare professionals. J. Patient Saf. Risk Manag. 2020, 25, 159–162. [Google Scholar] [CrossRef]
- Shah, K.; Bedi, S.; Onyeaka, H.; Singh, R.; Chaudhari, G. The Role of Psychological First Aid to Support Public Mental Health in the COVID-19 Pandemic. Cureus 2020, 12, e8821. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Colquhoun, H.; O’Brien, K.K.; Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franks, H.; Hardiker, N.; McGrath, M.; McQuarrie, C. Public health interventions and behaviour change: Reviewing the grey literature. Public Health 2012, 126, 12–17. [Google Scholar] [CrossRef]
- Helmer, D.; Savoie, I.; Green, C.; Kazanjian, A. Evidence-based practice: Extending the search to find material for the systematic review. Bull. Med. Libr. Assoc. 2001, 89, 346–352. [Google Scholar]
- Amir-Behghadami, M.; Janati, A. Population, Intervention, Comparison, Outcomes and Study (PICOS) design as a framework to formulate eligibility criteria in systematic reviews. Emerg. Med. J. 2020, 37, 387. [Google Scholar] [CrossRef]
- Babineau, J. Product Review: Covidence (Systematic Review Software). J. Can. Health Libr. Assoc. J. l’Association bibliothèques de la santé du Can. 2014, 35, 68–71. [Google Scholar]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [Green Version]
- Schafer, A.; Snider, L.; Van Ommeren, M. Psychological first aid pilot: Haiti emergency response. Intervention 2010, 8, 245–254. [Google Scholar] [CrossRef]
- Schafer, A.; Snider, L.; Sammour, R. A reflective learning report about the implementation and impacts of Psychological First Aid (PFA) in Gaza. Disaster Health 2015, 3, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Semlitz, L.; Ogiwara, K.; Weissbecker, I.; Gilbert, E.; Sato, M.; Taniguchi, M.; Ishii, C.; Sawa, C. Psychological first aid training after Japan’s triple disaster: Changes in perceived self competency. Int. J. Emerg. Ment. Health Hum. Resil. 2013, 15, 181–196. [Google Scholar]
- Sijbrandij, M.; Horn, R.; Esliker, R.; O’May, F.; Reiffers, R.; Ruttenberg, L.; Stam, K.; de Jong, J.; Ager, A. The effect of psychological first Aid training on knowledge and understanding about psychosocial support principles: A cluster-randomized controlled trial. Int. J. Environ. Res. Public Health 2020, 17, 484. [Google Scholar] [CrossRef] [Green Version]
- Allen, B.; Brymer, M.J.; Steinberg, A.M.; Vernberg, E.M.; Jacobs, A.; Speier, A.H.; Pynoos, R.S. Perceptions of psychological first aid among providers responding to Hurricanes Gustav and Ike. J. Trauma. Stress 2010, 23, 509–513. [Google Scholar] [CrossRef]
- Akoury-Dirani, L.; Sahakian, T.S.; Hassan, F.Y.; Hajjar, R.V.; El Asmar, K. Psychological First Aid Training for Lebanese Field Workers in the Emergency Context of the Syrian Refugees in Lebanon. Psychol. Trauma Theory Res. Pr. Policy 2015, 7, 533–538. [Google Scholar] [CrossRef]
- Brown, L.M.; Bruce, M.L.; Hyer, K.; Mills, W.L.; Vongxaiburana, E.; Polivka-West, L. A Pilot Study Evaluating the Feasibility of Psychological First Aid for Nursing Home Residents. Clin. Gerontol. 2009, 32, 293–308. [Google Scholar] [CrossRef] [Green Version]
- Chandra, A.; Kim, J.; Pieters, H.C.; Tang, J.; McCreary, M.; Schreiber, M.; Wells, K. Implementing psychological first-aid training for medical reserve corps volunteers. Disaster Med. Public Health Prep. 2014, 8, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Cheung, Y.L. Psychological First Aid as a Public Health Disaster Response Preparedness Strategy for Responders in Critical Incidents and Disasters. Ph.D. Thesis, The Chinese University of Hong Kong, Hong Kong, China, 2014. [Google Scholar]
- Everly, G.S., Jr.; Barnett, D.J.; Links, J.M. The Johns Hopkins model of psychological first aid (RAPID—PFA): Curriculum development and content validation. Int. J. Emerg. Ment. Health 2012, 14, 95–103. [Google Scholar] [PubMed]
- Everly, G.S., Jr.; McCabe, O.L.; Semon, N.L.; Thompson, C.B.; Links, J.M. The development of a model of psychological first aid for non–mental health trained public health personnel: The Johns Hopkins RAPID-PFA. J. Public Health Manag. Pract. 2014, 20, S24–S29. [Google Scholar] [CrossRef] [PubMed]
- Despeaux, K.E.; Lating, J.M.; Everly, G.S.; Sherman, M.F.; Kirkhart, M.W. A Randomized Controlled Trial Assessing the Efficacy of Group Psychological First Aid. J. Nerv. Ment. Dis. 2019, 207, 626–632. [Google Scholar] [CrossRef]
- Everly, G.S., Jr.; Lating, J.M.; Sherman, M.F.; Goncher, I. The potential efficacy of psychological first aid on self-reported anxiety and mood: A pilot study. J. Nerv. Ment. Dis. 2016, 204, 233–235. [Google Scholar] [CrossRef] [PubMed]
- Kılıç, N.; Şimşek, N. The effects of psychological first aid training on disaster preparedness perception and self-efficacy. Nurse Educ. Today 2019, 83, 104203. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-S.; You, S.; Choi, Y.-K.; Youn, H.-Y.; Shin, H.S. A preliminary evaluation of the training effects of a didactic and simulation-based psychological first aid program in students and school counselors in South Korea. PLoS ONE 2017, 12, e0181271. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, J.; Xue, Z.; Xue, Y. Effect of psychological first aid training on medical students’ cognitive appraisal about sudden events. Chin. J. Behav. Med. Brain Sci. 2016, 25, 838–841. [Google Scholar]
- Farchi, M.; Ben Hirsch-Gornemann, M.; Whiteson, A.; Gidron, Y. The SIX Cs model for Immediate Cognitive Psychological First Aid: From Helplessness to Active Efficient Coping. Int. J. Emerg. Ment. Health Hum. Resil. 2018, 20, 1–12. [Google Scholar] [CrossRef]
- McCabe, O.L.; Semon, N.L.; Thompson, C.B.; Lating, J.M.; Everly, G.S.; Perry, C.J.; Moore, S.S.; Mosley, A.M.; Links, J.M. Building a National Model of Public Mental Health Preparedness and Community Resilience: Validation of a Dual-Intervention, Systems-Based Approach. Disaster Med. Public Health Prep. 2014, 8, 511–526. [Google Scholar] [CrossRef]
- Kantaris, X.; Radcliffe, M.; Acott, K.; Hughes, P.; Chambers, M. Training healthcare assistants working in adult acute inpatient wards in Psychological First Aid: An implementation and evaluation study. J. Psychiatr. Ment. Health Nurs. 2020, 27, 742–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosley, A.; Marum, F.; Gwon, H.S.; McCabe, O.L.; Kaminsky, M.J.; George, S.; Links, E.J.M., Jr.; Langlieb, A. Community capacity-building in disaster mental health resilience: A pilot study of an academic/faith partnership model. Int. J. Emerg. Ment. Health 2012, 14, 112–122. [Google Scholar]
- Hambrick, E.P.; Rubens, S.L.; Vernberg, E.M.; Jacobs, A.K.; Kanine, R.M. Towards successful dissemination of psychological first aid: A study of provider training preferences. J. Behav. Health Serv. Res. 2014, 41, 203–215. [Google Scholar] [CrossRef]
- Horn, R.; O’May, F.; Esliker, R.; Gwaikolo, W.; Woensdregt, L.; Ruttenberg, L.; Ager, A. The myth of the 1-day training: The effectiveness of psychosocial support capacity-building during the Ebola outbreak in West Africa. Glob. Ment. Health 2019, 6. [Google Scholar] [CrossRef] [Green Version]
- Lewis, V.; Varker, T.; Phelps, A.; Gavel, E.; Forbes, D. Organizational implementation of psychological first aid (PFA): Training for managers and peers. Psychol. Trauma Theory Res. Pract. Policy 2014, 6, 619. [Google Scholar] [CrossRef]
- McCabe, O.L.; Mosley, A.M.; Gwon, H.S.; Everly, G.S.; Lating, J.M.; Links, J.M.; Kaminsky, M.J. The tower of ivory meets the house of worship: Psychological first aid training for the faith community. Int. J. Emerg. Ment. Health Hum. Resil. 2007, 9, 171–180. [Google Scholar]
- McCabe, O.L.; Perry, C.; Azur, M.; Taylor, H.G.; Bailey, M.; Links, J.M. Psychological First-Aid Training for Paraprofessionals: A Systems-Based Model for Enhancing Capacity of Rural Emergency Responses. Prehosp. Disaster Med. 2011, 26, 251–258. [Google Scholar] [CrossRef] [PubMed]
- McCabe, O.L.; Semon, N.L.; Lating, J.M.; Everly, J.G.S.; Perry, C.J.; Moore, S.S.; Mosley, A.M.; Thompson, C.B.; Links, J.M. An Academic-Government-Faith Partnership to Build Disaster Mental Health Preparedness and Community Resilience. Public Health Rep. 2014, 129, 96–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkes, M.; Bligh, J. Evaluating educational interventions. BMJ 1999, 318, 1269–1272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bisson, J.I.; Lewis, C. Systematic Review of Psychological First Aid; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Baron, N. The’TOT’: A Global Approach for the Training of Trainers for Psychosocial and Mental Health Interventions in Countries Affected by War, Violence and Natural Disasters; National Emergency Training Center: Emmitsburg, MD, USA, 2006.
- Simmons, R.; Fajans, P.; Ghiron, L. (Eds.) Scaling up Health Service Delivery: From Pilot Innovations to Policies and Programmes; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Généreux, M.; Schluter, P.J.; Takahashi, S.; Usami, S.; Mashino, S.; Kayano, R.; Kim, Y. Psychosocial Management Before, During, and After Emergencies and Disasters—Results from the Kobe Expert Meeting. Int. J. Environ. Res. Public Health 2019, 16, 1309. [Google Scholar] [CrossRef] [Green Version]
- Javadi, D.; Feldhaus, I.; Mancuso, A.; Ghaffar, A. Applying systems thinking to task shifting for mental health using lay providers: A review of the evidence. Glob. Ment. Health 2017, 4, e14. [Google Scholar] [CrossRef]
- Caulfield, A.; Vatansever, D.; Lambert, G.; Van Bortel, T. WHO guidance on mental health training: A systematic review of the progress for non-specialist health workers. BMJ Open 2019, 9, e024059. [Google Scholar] [CrossRef]
- Gray, B.; Hanna, F.; Reifels, L. The Integration of Mental Health and Psychosocial Support and Disaster Risk Reduction: A Mapping and Review. Int. J. Environ. Res. Public Health 2020, 17, 1900. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population | Any studies that sampled PFA trainees. e.g., disaster responders, health professionals, decision-makers. | None. |
| Intervention | PFA training models which adhered to the five Hobfoll’s principles of an immediate mass trauma intervention to improve: safety, calming, efficacy, connectedness and hope [13]. | None. |
| Comparison | Studies were not required to have a control or comparison group, due to the exploratory nature of the scoping review. | None. |
| Outcomes | All outcomes investigated by the training courses, delivered at all intervention levels: individuals, organisation and system. | None. |
| Studies | All study designs evaluating PFA training, e.g., qualitative, quantitative and mixed-method studies. | Non-English and Chinese language sources. |
 ⟪Psychological First Aid Guide for Field workers⟫ ⟪Psychological First Aid Guide for Field workers⟫ |  ⟪Psychological First Aid: Field Operations Guide⟫ ⟪Psychological First Aid: Field Operations Guide⟫ |  ⟪The Johns Hopkins Guide to Psychological First Aid⟫ ⟪The Johns Hopkins Guide to Psychological First Aid⟫ | Immediate Cognitive-Functional Psychological First Aid (ICF-PFA): The SIX-Cs PFA Model | |
|---|---|---|---|---|
| Developer | World Health Organization War Trauma Foundation World Vision International | National Child Traumatic Stress Network National Centre for PTSD | Johns Hopkins University | / |
| Intended purpose | Humanitarian aid in low- and middle-income countries | Common disaster mental health response and research | Mental health preparedness and community resilience initiatives | Nonprofessional community, Professionals and first responders |
| Approach |
Check for serious distressed people Approach people who may need help |
|
|
|
| Listen |
|
|
| Listening the answers to the above cognitive questions |
| Assessment |
|
|
| Set priorities and make effective decisions |
| Support |
Help people cope with problems Give information Protecting people from further harm |
|
|
|
| Referral |
|
|
|
Synchronisation of the event: underline the ending of the event |
| Self-care | Caring for yourself and your colleagues | Provider care |
| / |
| Available resources |
31 languages |
6 languages | Book The Johns Hopkins guide to psychological first aid. Online course: Coursera | / |
| Evaluation evidence support | Earthquake, Conflict, Triple Disasters, Refugee, Ebola, Acute wards | Hurricane, Flood, Fire, Typhoon, Refugee, Crime, Nursing Home staff | Emergency response, Mental health preparedness capacity building, College student | War crisis, High school student |
| First Author/Year/Country | Aim/s | Sample/Context | Methodology | Outcomes | Key Findings |
| Allen et al. [43] (2010) USA | To examine the perceptions of the providers after PFA training | Disaster workers (n = 50) Hurricane | Cross-sectional post-test study |
scale 2 on perceptions of PFA core actions |
|
| Akoury et al. [44] (2015) Lebanon | To examine the efficacy of a national PFA training program to enhance the readiness of mental health field workers in Syrian refugee response | Government, NGO workers (n = 60) | Pre- and post-control study |
evaluation form B on readiness of the trainees |
|
| Brown et al. [45] (2009) USA | To evaluate the feasibility of a modified PFA training intervention among nursing home staff. | Nursing home staff (n = 22) | Mixed methods study |
|
|
| Chandra et al. [46] (2014) USA | To assess the feasibility and impact on knowledge, attitudes; To explore perceived facilitators and barriers to improve PFA training | Medical response corps volunteer (n = 76) | Mixed methods study |
|
perceived confidence and capability in using PFA increases from 71% to 90% (p < 0.01); no significant increase in PFA-related knowledge;
|
| Cheung Y.L. [47] (2014) China | To investigate the effectiveness of pre-disaster training of PFA among first responders in enhancing PFA provision to survivors of disasters | First responders from Auxiliary Medical Service (n = 624) | Randomised controlled trial |
Secondary outcome: psychological distress; coping and social support; life satisfaction and resilience |
|
| Everly et al. [48] (2012) USA | To evaluate the attitudes, knowledge and behaviour towards the content. validation of the PFA training | Community citizens (n = 252) Mental health preparedness | Pre-/post-test study |
|
|
| Everly et al. [49] (2014) USA | To determine whether relevant knowledge, skills, and attitudes are imparted to trainees to support the effectiveness of PFA training | Public health personnel (n = 1500) Mental health preparedness | Pre-/post-test design study |
|
|
| Farchi et al. [55] (2018) Israel | To evaluate general self-efficacy, self-efficacy, resilience and perceived stress using the training among students | High school students (n = 232) | Pre-/post-test, controlled study |
Resilience The Perceived Stress Scale (PSS) |
|
| Hambrick et al. [59] (2014) USA | To gain understanding of training needs and preferences; To identify challenges and facilitators towards successful dissemination. | Disaster mental health providers (n = 9) | Qualitative study |
mental health team and resources Training nuts and bolts Desired training focus Training sustainability |
|
| Horn et al. [60] (2019) Sierra Leone | To understand whether the training provided enabled non-specialists to incorporate the key principles into their practice. | PFA trainers (n = 24) PFA trainees (n = 36) Key informants (n = 12) | Qualitative study |
Rolling out PFA training Effectiveness of the PFA training Factors contributing to effectiveness of PFA capacity-building |
Only terms of language and role play were modified based on the PFA manual (Ebola version), training greatly reduced into a 95-min time slot; (2) Rolling out training “Emergency” result in confusion: poor-quality of training (diluted), multiple trainings, short train-of-trainers rarely included training skills; Varied in nature and quality of the refresher training and supervision; (3) Effectiveness of training: responses were less consistent with the guidance, e.g., calming people or promoting hope by reassuring them and making false promises; challenging by helping them to promote self-and collective efficacy and connectedness; (4) Challenges to the effectiveness of PFA capacity-building: difficulties in coordinating training activities; confusion of the purpose and limitations of PFA; unavailable supervision result in diluted PFA delivery. |
| Kılıç et al. [52] (2019) Turkey | To investigate the impact of PFA training on the perception of disaster preparedness and self-efficacy | Nursing student: Intervention group with PFA training (n = 38) Control group with no training (n = 38) | Randomised controlled trial |
Self-efficacy |
|
| Lewis et al. [61] (2013) Australia | To examine the impact (knowledge, skills and overall understanding of response) of PFA training for both managers and peer supporters in a high-risk organisation | Police force (n = 582) High-risk organisation | Pre-/post-test design study |
self-reported knowledge and skill about response; confidence in emergency response |
|
| Lee et al. [53] (2017) Korea | To examine the training effects of a didactic and simulation based PFA program | College student (n = 37) Counsellor (n = 82) | Quasi-experimental pre-and post-control design |
Perceived competence in PFA skill Perceived willingness, preparedness and confidence |
|
| Mosley et al. [62] (2007) USA | To determine the PFA training model feasibility, perceived effectiveness and prospective translational impact | Faith members (n = 500) Mental health preparedness | Quasi-experimental design |
Effectiveness: self-efficacy; overall impression of the programme |
|
| McCabe et al. [63] (2011) USA | To assess the feasibility and effectiveness of a system based PFA training among lay citizens | Community citizens (n = 178) Mental health preparedness | Quasi-experimental design |
Effectiveness: knowledge; skill; attitudes Impact: policy change |
|
| Mosley et al. [58] (2012) USA | To determine the feasibility of a brief PFA training to enhance the perceived self-efficacy among faith leaders | Faith leader (n = 72) Mental health preparedness | Quasi-experimental design |
Effectiveness: knowledge, perceived self-efficacy; impression of the programme |
|
| McCabe et al. [56] (2014) USA | To evaluate the feasibility and the effectiveness of PFA training among lay citizens | Lay citizens (n = N/A) Mental health preparedness | Pre- and post-training, mixed methods study |
Impact | Significantly improved knowledge and skills in technical or practical PFA content (p < 0.001); Changes in policy of government and faith partners to sustain the training to promote public health preparedness and community resilience. |
| McCabe et al. [64] (2014) USA | To assess the outcomes of 1-day PFA training workshop among urban and rural communities | Urban and rural communities (n = N/A) Mental health preparedness | Pre- and post-training, mixed methods study |
sustainability and model scalability
|
|
| Schafer et al. [39] (2010) Haiti | To understand the experience from the pilot PFA use within the Haiti context | NGO staff (n = 119) earthquake | Qualitative study |
the application of the PFA approach; contextual lessons and the limitations. |
|
| Semlitz et al. [41] (2013) Japan | To examine the utility and effectiveness of a culturally adapted PFA training | NGO staff (n = 463) Triple disaster | Mixed methods study |
Qualitative discussions: qualitative questions in acquisition of training and specific issues. |
|
| Sijbrandij et al. [42] (2020) Sierra Leone | To extend the evidence base concerning PFA by evaluating the effectiveness of a one-day PFA training in the acute aftermath of adversity. | Primary health workers Ebola Intervention group with PFA training (n = 206) Control group without training (n = 202) | Cluster-randomised controlled trial |
|
|
| Xenya et al. [57] (2020) UK | To introduce and evaluate first aid training for healthcare assistants | Healthcare assistant (n = 16) Acute inpatient wards | Mixed methods, pre-and post-test study |
|
Significantly increased healthcare assistants’ self-efficacy and confidence, “untoward” incidents decreased;
|
| Zhang et al. [54] (2016) China | To explore the influence of PFA training on cognitive appraisal of sudden events in medical students | College students Intervention group with PFA training (n = 42) Control group without training (n = 53) | Randomised controlled study |
Looming maladaptive style questionnaire |
|
| Study | Ix | Outcome Measures | Why | Who | How and Where | When and How Much | Tailoring | How Well? | Total | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Learning | Behavior | Practice | Satisfaction | Theory | From | To | Deliver | Site | Duration | Number of Sessions | Attrition | Adherence | ||||||||||||
| pm | nw | p | np | lec- | com | sup | cl | Short ≤1/2 d | Med 1 d | Long >1 d | Low ≤4 se | Med 4–8 se | Long >8 se | |||||||||||
| Allen [43] | NCTSN | √ | √ | ⊘ | ● | ● | ● | ● | − | ◉ | ⊘ | ⊘ | 4 | |||||||||||
| Akoury [44] | NCTSN | √ | √ | ⊘ | ● | ● | ● | ● | ● | ● | ● | ⊘ | ⊘ | 7 | ||||||||||
| Brown [45] | NCTSN | √ | √ | ⊘ | ● | ● | ● | ● | ● | − | ● | ⊘ | ⊘ | 6 | ||||||||||
| Chandra [46] | NCTSN | X | √ | ⊘ | ⊖ | ● | ● | ● | ● | − | ● | ⊘ | ⊘ | 5 | ||||||||||
| Cheung [47] | NCTSN | √ | √ | √ | ⊘ | ● | ● | ● | ● | ● | ◉ | ⊘ | ⊘ | 5 | ||||||||||
| Everly [48] | RAPID | √ | √ | ● | ● | ● | ● | ● | ● | − | ◉ | ⊘ | ⊘ | 6 | ||||||||||
| Everly [49] | RAPID | √ | √ | ⊘ | ● | ● | ● | ● | ● | − | ◉ | ⊘ | ⊘ | 5 | ||||||||||
| Farchi [55] | ICF-PFA | √ | ● | ⊘ | ● | ● | − | ⊖ | ⊘ | ⊘ | 3 | |||||||||||||
| Kılıç [52] | Mixed | √ | ⊘ | ● | ● | ● | ● | ● | ● | ⊖ | ⊘ | ⊘ | 6 | |||||||||||
| Lee [53] | Mixed | √ | √ | ⊘ | ● | ● | ● | ● | ● | − | ● | ⊘ | ⊘ | 6 | ||||||||||
| Lewis [61] | NCTSN | √ | √ | ⊘ | ● | ● | ● | ● | − | ⊖ | ⊘ | ⊘ | 4 | |||||||||||
| McCabe [63] | RAPID | √ | √ | ⊘ | ● | ● | ● | ● | ● | ● | ◉ | ⊘ | ⊘ | 6 | ||||||||||
| McCabe [64] | RAPID | √ | ⊘ | ⊘ | ● | ● | ● | ● | ● | ◉ | ⊘ | ⊘ | 6 | |||||||||||
| McCabe [56] | RAPID | √ | √ | √ | ⊘ | ● | ● | ● | ● | ● | ● | ◉ | ⊘ | ⊘ | 6 | |||||||||
| Mosley [62] | RAPID | √ | √ | √ | ⊘ | ● | ● | ● | ● | ● | ● | ◉ | ⊘ | ⊘ | 6 | |||||||||
| Mosley [58] | RAPID | √ | √ | ⊘ | ● | ● | ● | ● | ● | ● | ◉ | ⊘ | ⊘ | 6 | ||||||||||
| Semlitz [41] | WHO | √ | √ | √ | ⊘ | ● | ● | ● | ● | ● | − | ● | ⊘ | ⊘ | 6 | |||||||||
| Sijbrandij [42] | WHO | √ | X | √ | ⊘ | ● | ● | ● | ● | ● | − | − | ● | ● | ● | 7 | ||||||||
| Xenya [57] | WHO | √ | √ | √ | √ | ⊘ | ⊘ | ● | ● | ● | ● | − | ◉ | ⊘ | ⊘ | 4 | ||||||||
| Zhang [54] | Mixed | √ | ⊘ | ● | ● | ● | ● | ● | ⊖ | ⊘ | ⊘ | 5 | ||||||||||||
| Total | √ 14; X 1 | √ 17; X 1 | √ 4 | √ 6 | 2 | 12 | 5 | 9 | 11 | 3 | 15 | 1 | 15 | 2 | 11 | 5 | 6 | 2 | 1 | 6 | 1 | 1 | ||
| Outcomes Measures | Learning | Behaviour | Satisfaction | Practice |
|---|---|---|---|---|
| Validated tools | ||||
| The General Self-Efficacy scale (GSE) | +[52] +[55] +[57] +[47] | |||
| The General Health Questionnaire (GHQ) | +[47] | |||
| Depression Anxiety Stress Scales (DASS21) | −[47] | |||
| Brief COPE scale | −[47] | |||
| Professional Self-Efficacy (PSE) | +[55] | |||
| The Connor-Davidson Resilience scale (CD-RISC) | +[55] −[47] | |||
| The Perceived Stress Scale (PSS) | +[55] | |||
| Multidimensional Scale of Perceived Social Support (MSPSS) | −[47] | |||
| Professional Quality of Life Scale (ProQOL-5) | −[42] | |||
| Therapeutic Engagement questionnaire (TEQ) | +[57] | |||
| The Stress Appraisal Measure | +[54] | |||
| Looming maladaptive style questionnaire | +[54] | |||
| Self-designed tools | ||||
| Skill, Knowledge and attitude | +[41] +[42] +[44] −[46] +[49]+[53] +[56] +[58] +[61] +[62] +[63] +[64] | |||
| Ability to recognise clinical markers | +[48] | |||
| Perceived competence | +[40] +[48] | |||
| Scales on willingness, preparedness and confidence | +[44] +[45] +[49] +[52] +[53] +[58] +[61]+[62] +[63] | +[62] | +[49] +[56] | |
| Scale on perceptions of PFA utilisation and satisfaction on PFA training | +[43] | |||
| Programme Evaluation | +[45] +[47] +[55] +[57] | +[43] | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, L.; Norman, I.; Xiao, T.; Li, Y.; Leamy, M. Psychological First Aid Training: A Scoping Review of Its Application, Outcomes and Implementation. Int. J. Environ. Res. Public Health 2021, 18, 4594. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094594
Wang L, Norman I, Xiao T, Li Y, Leamy M. Psychological First Aid Training: A Scoping Review of Its Application, Outcomes and Implementation. International Journal of Environmental Research and Public Health. 2021; 18(9):4594. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094594
Chicago/Turabian StyleWang, Ling, Ian Norman, Tao Xiao, Yamin Li, and Mary Leamy. 2021. "Psychological First Aid Training: A Scoping Review of Its Application, Outcomes and Implementation" International Journal of Environmental Research and Public Health 18, no. 9: 4594. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094594