
Current Practice of Physical Activity Counselling within Physiotherapy Usual Care and Influences on Its Use: A Cross-Sectional Survey

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
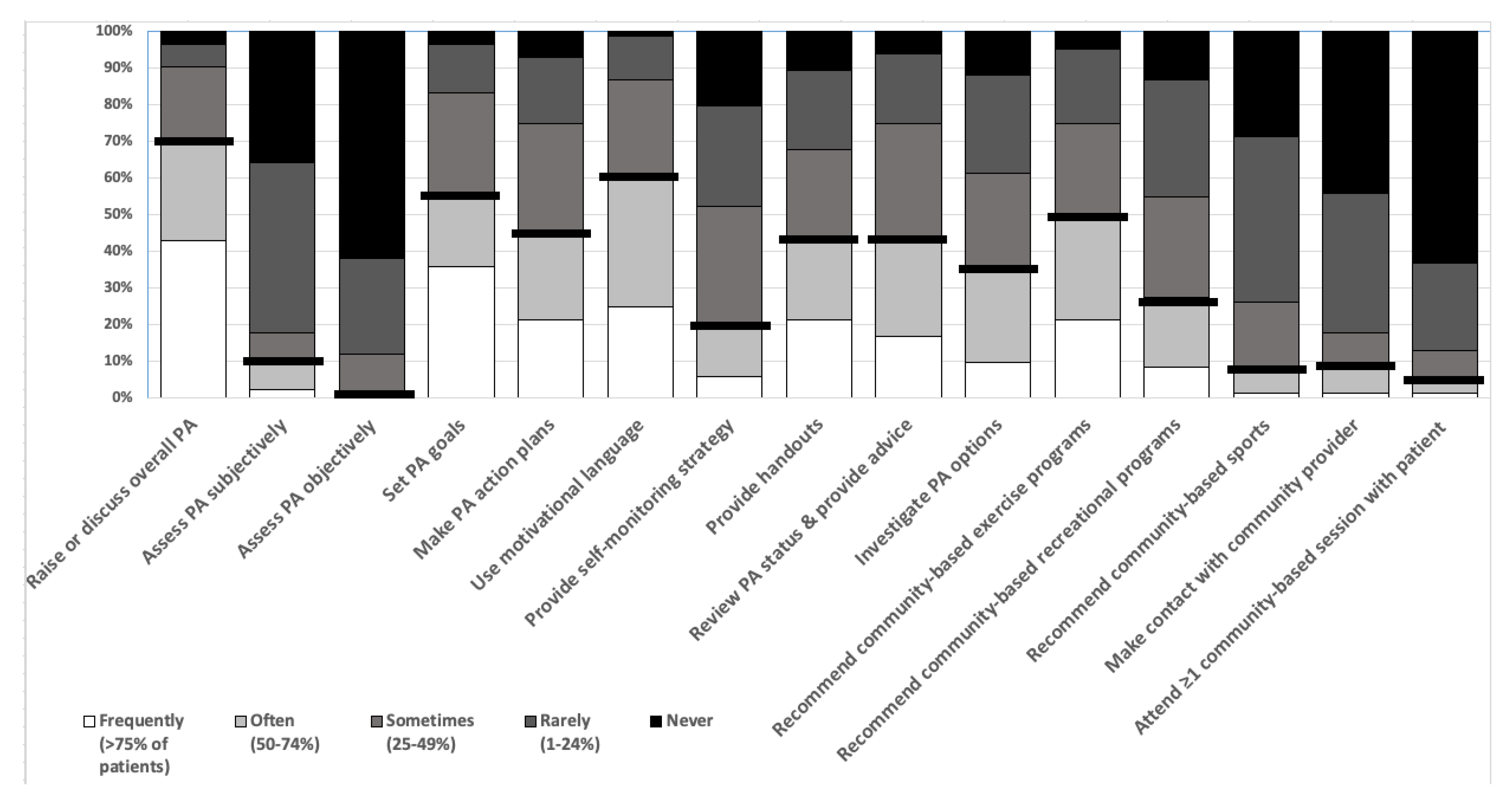
- What elements of physical activity counselling are currently incorporated in routine healthcare interactions by physiotherapists working in a local health district in Australia?
- What are physiotherapists’ perceptions of their patients’ readiness for structured community-based physical activity on discharge from physiotherapy care?
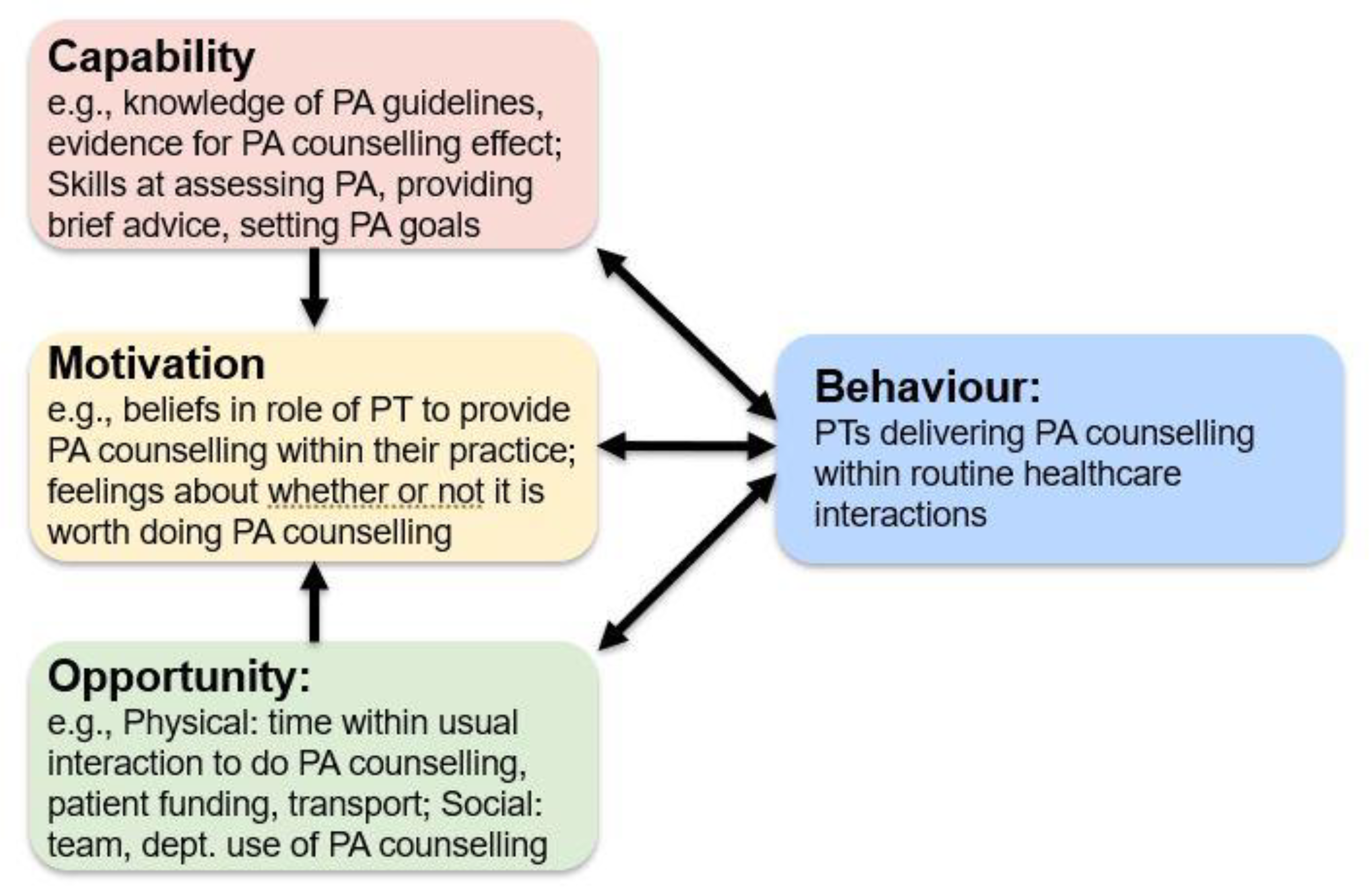
- Which influences do physiotherapists report to affect incorporation of physical activity counselling into routine healthcare interactions?
- Is there a relationship between the incorporation of physical activity counselling within routine care, physiotherapist characteristics and influences reported by physiotherapists?
2. Materials and Methods
2.1. Study Design
2.2. Context
2.3. Participants
2.4. Data Collection Measures and Tools
| In a Typical Week, How Frequently Do You Undertake Each of the Below for Your Patients Who Could Be More Active: | ||
| Raise or discuss overall PA | Use motivational language | Recommend community-based exercise programs |
| Assess PA subjectively | Provide self-monitoring strategy | Recommend community-based recreation programs |
| Assess PA objectively | Provide handouts | Recommend community-based sports |
| Set PA goals | Review PA status & provide advice | Make contact with community provider |
| Make PA action plans | Investigate PA options | Attend ≥1 community-based session with patient |
2.5. Procedure
2.6. Sample Size
2.7. Data Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Current Practice of Physical Activity Counselling by Physiotherapists within Routine Care
3.3. Physiotherapist Perceptions of Their Patients’ Readiness for Structured Community Based Physical Activity
3.4. Influences on Physiotherapists’ Ability to Incorporate PA Counselling into Practice within the COM-B Framework, and Its Relationship with Total Number of PA Counselling Elements
3.5. Relationship between PA Counselling Skills and Incorporating Elements
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Disclosure Statement
Conflicts of Interest
References
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour: Web Annex. Evidence Profiles; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Australian Health Policy Collaboration. Australia’s Health Tracker by Area. 2017. Available online: Atlasesaustralia.com.au (accessed on 22 May 2017).
- Australian Bureau of Statistics (ABS). Australian Health Survey: Physical Activity, 2011–2012; Australian Bureau of Statistics (ABS), Ed.; ABS: Canberra, Australia, 2013. [Google Scholar]
- Hassett, L.; Shields, N.; Cole, J.; Owen, K.; Sherrington, C. Comparisons of leisure-time physical activity participation by adults with and without a disability: Results of an Australian cross-sectional national survey. BMJ Open Sport Exerc. Med. 2021, 7, e000991. [Google Scholar] [CrossRef]
- Reis, R.S.; Salvo, D.; Ogilvie, D.; Lambert, E.V.; Goenka, S.; Brownson, R.C. Lancet Physical Activity Series 2 Executive Committee. Scaling up physical activity interventions worldwide: Stepping up to larger and smarter approaches to get people moving. Lancet 2016, 388, 1337–1348. [Google Scholar] [PubMed] [Green Version]
- Estabrooks, P.A.; Glasgow, R.E.; Dzewaltowski, D.A. Physical activity promotion through primary care. JAMA 2003, 289, 2913–2916. [Google Scholar] [CrossRef] [PubMed]
- Richards, J.; Hillsdon, M.; Thorogood, M.; Foster, C. Face-to-face interventions for promoting physical activity. Cochrane Database Syst Rev. 2013, 9. [Google Scholar] [CrossRef]
- Foster, C.; Richards, J.; Thorogood, M.; Hillsdon, M. Remote and web 2.0 interventions for promoting physical activity. Cochrane Database Syst Rev. 2013, 9. [Google Scholar] [CrossRef]
- Michie, S.; Abraham, C.; Whittington, C.; McAteer, J.; Gupta, S. Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychol. 2009, 28, 690–701. [Google Scholar] [CrossRef] [Green Version]
- van der Ploeg, H.P.; Streppel, K.R.M.; van der Beek, A.J.; van der Woude, L.H.V.; Vollenbroek-Hutten, M.M.R.; van Harten, W.H.; van Mechelen, W. Successfully improving physical activity behavior after rehabilitation. Am. J. Health Promot. 2007, 21, 153–159. [Google Scholar] [CrossRef]
- Orrow, G.; Kinmonth, A.-L.; Sanderson, S.; Sanderson, S.; Sutton, S. Effectiveness of physical activity promotion based in primary care: Systematic review and meta-analysis of randomised controlled trials. BMJ 2012, 344, e1389. [Google Scholar] [CrossRef] [Green Version]
- Simons-Morton, D.G.; Blair, S.N.; King, A.C.; Morgan, T.M.; Applegate, W.B.; O’Toole, M.; Haskell, W.L.; Albright, C.L.; Cohen, S.J.; Ribisl, P.M.; et al. Effects of physical activity counseling in primary care: The Activity Counseling Trial: A randomized controlled trial. JAMA 2001, 286, 677–687. [Google Scholar]
- Short, C.E.; Hayman, M.; Rebar, A.L.; Gunn, K.M.; de Cocker, K.; Duncan, M.J.; Turnbull, D.; Dollman, J.; van Uffelen, J.G.Z.; Vandelanotte, C. Physical activity recommendations from general practitioners in Australia. Results from a national survey. Aust. N. Z. J. Public Health 2016, 40, 83–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carroll, D.D.; Courtney-Long, E.A.; Stevens, A.C.; Sloan, M.L.; Lullo, C.; Visser, S.N.; Fox, M.H.; Armour, B.S.; Campbell, V.A.; Brown, D.R.; et al. Vital signs: Disability and physical activity—United States, 2009–2012. MMWR Morb. Mortal. Wkly. Rep. 2014, 63, 407–413. [Google Scholar]
- Letts, L.; Martin Ginis, K.A.; Faulkner, G.; Colquhoun, H.; Levac, D.; Gorczynski, P. Preferred methods and messengers for delivering physical activity information to people with spinal cord injury: A focus group study. Rehabil. Psychol. 2011, 56, 128–137. [Google Scholar] [CrossRef]
- Freene, N.; Cools, S.; Bissett, B. Are we missing opportunities? Physiotherapy and physical activity promotion: A cross-sectional survey. BMC Sports Sci. Med. Rehabil. 2017, 9, 19. [Google Scholar]
- Shirley, D.; van der Ploeg, H.P.; Bauman, A.E. Physical Activity Promotion in the Physical Therapy Setting: Perspectives from Practitioners and Students. Phys. Ther. 2010, 90, 1311–1322. [Google Scholar] [CrossRef] [Green Version]
- Aweto, H.A.; Oligbo, C.N.; Fapojuwo, O.A.; Olawale, O.A. Knowledge, attitude and practice of physiotherapists towards promotion of physically active lifestyles in patient management. BMC Health Serv. Res. 2013, 13, 21. [Google Scholar] [CrossRef] [Green Version]
- Mouton, A.; Mugnier, B.; Demoulin, C.; Cloes, M. Physical therapists’ knowledge, attitudes, and beliefs about physical activity. J. Phys. Ther. Educ. 2014, 28, 120–127. [Google Scholar] [CrossRef]
- Lowe, A.; Littlewood, C.; McLean, S.; Kilner, K. Physiotherapy and physical activity: A cross-sectional survey exploring physical activity promotion, knowledge of physical activity guidelines and the physical activity habits of UK physiotherapists. BMJ Open Sport Exerc. Med. 2017, 3, e000290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, M.S.; Damschroder, L.; Hagedorn, H.; Smith, J.; Kilbourne, A.M. An introduction to implementation science for the non-specialist. BMC Psychol. 2015, 3, 32. [Google Scholar] [CrossRef] [Green Version]
- Powell, B.J.; Waltz, T.J.; Chinman, M.J.; Damschroder, L.J.; Smith, J.L.; Matthieu, M.M.; Proctor, E.K.; Kirchner, J.E. A refined compilation of implementation strategies: Results from the Expert Recommendations for Implementing Change (ERIC) project. Implement. Sci. 2015, 10, 21. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Atkins, L.; West, R. The Behaviour Change Wheel: A Guide to Designing Interventions; Silverback Publishing: Sutton, UK, 2014. [Google Scholar]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- Holt, R.G. Declaration of Helsinki—The World’s Document of Conscience and Responsibility. South. Med. J. 2014, 107, 407. [Google Scholar] [CrossRef]
- Grimshaw, J. SURGE (The SUrvey Reporting GuidelinE). In Guidelines for Reporting Health Research: A User’s Manual; Moher, D., Altman, D.G., Schulz, K.F., Simera, I., Wager, E., Eds.; John Wiley & Sons, Ltd.: West Sussex, UK, 2014; pp. 206–213. [Google Scholar]
- South Western Sydney Local Health District. Year in Review 2018–2019. 2019. Available online: https://www.swslhd.health.nsw.gov.au/pdfs/2019Review.pdf (accessed on 13 October 2020).
- South West Sydney Local Health District Planning Unit. SWSLHD: Key Health Challenges 2020. Available online: https://www.swslhd.health.nsw.gov.au/planning/content/pdf/Current%20Documents/SWSLHD_Key_Health_Challenges_March_2020-v3.pdf (accessed on 29 January 2021).
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burns, K.E.; Duffett, M.; Kho, M.E.; Meade, M.O.; Adhikari, N.K.; Sinuff, T.; Cook, D.J. A guide for the design and conduct of self-administered surveys of clinicians. CMAJ 2008, 179, 245–252. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.K.; Ginis, K.A.M. A meta-analysis of physical activity interventions in people with physical disabilities: Content, characteristics, and effects on behaviour. Psychol. Sport Exerc. 2018, 37, 262–273. [Google Scholar] [CrossRef]
- Kunstler, B.E.; Cook, J.L.; Freene, N.; Finch, C.F.; Kemp, J.L.; O’Halloran, P.D.; Gaida, J.E. Physiotherapists use a small number of behaviour change techniques when promoting physical activity: A systematic review comparing experimental and observational studies. J. Sci. Med. Sport 2018, 21, 609–615. [Google Scholar] [CrossRef]
- Rimmer, J.; Lai, B. Framing new pathways in transformative exercise for individuals with existing and newly acquired disability. Disabil. Rehabil. 2017, 39, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Rimmer, J.H.; Henley, K.Y. Building the crossroad between inpatient/outpatient rehabilitation and lifelong community-based fitness for people with neurologic disability. J. Neurol. Phys. Ther. 2013, 37, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Hanson, C.L.; Oliver, E.J.; Dodd-Reynolds, C.J.; Pearsons, A.; Kelly, P. A modified Delphi study to gain consensus for a taxonomy to report and classify physical activity referral schemes (PARS). Int. J. Behav. Nutr. Phys. Act. 2020, 17, 158. [Google Scholar] [CrossRef]
- Raphael, K. Recall bias: A proposal for assessment and control. Int. J. Epidemiol. 1987, 16, 167–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomson, D. An ethnographic study of physiotherapists’ perceptions of their interactions with patients on a chronic pain unit. Physiother. Theory Pract. 2008, 24, 408–422. [Google Scholar] [CrossRef] [PubMed]
- Liberati, E.G. What Is the Potential of Patient Shadowing as a Patient-Centred Method? BMJ. Qual. Saf. 2017, 26, 343–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristic | n = 84 | |
|---|---|---|
| Age (yr), n (%) | ||
| <25 | 19 (23) | |
| 25–34 | 40 (48) | |
| 35–44 | 18 (22) | |
| 45 and over | 6 (7) | |
| Gender, number female, n (%) | 66 (79) | |
| Years practised as a physiotherapist (years) | ||
| 0–2 | 17 (20) | |
| 2–5 | 23 (28) | |
| 5–8 | 13 (16) | |
| 8–12 | 10 (12) | |
| >12 | 20 (24) | |
| Hospital, n (%) | ||
| Hospital 1 | 44 (52) | |
| Hospital 2 | 18 (21) | |
| Hospital 3 | 14 (17) | |
| Hospital 4 | 7 (8) | |
| Hospital 5 | 1 (1) | |
| Employment status, n (%) | ||
| Permanent staff | 55 (67) | |
| Contract staff | 17 (21) | |
| First year graduate program | 10 (12) | |
| Full time equivalent, n (%) | ||
| Full-time | 65 (78) | |
| Part-time | 18 (22) | |
| Classification of position, n (%) | ||
| Level 1–2: Junior clinician | 47 (57) | |
| Level 3–4: Senior clinician | 26 (32) | |
| Level 5–6: Health Professional Educator/Clinical Specialist | 5 (6) | |
| Manager | 4 (5) | |
| Position, n (%) | ||
| Rotational position | 43 (53) | |
| Non-rotating position | 38 (47) | |
| Practice setting, n (%) | ||
| Inpatient | 43 (51) | |
| Outpatient/Community | 29 (35) | |
| Mixed inpatient and outpatient | 12 (14) | |
| Area of physiotherapy, n (%) * | ||
| Musculoskeletal/Rheumatology/Hands | 23 (27) | |
| Rehabilitation | 21 (25) | |
| Orthopaedics | 17 (20) | |
| Aged Care | 17 (20) | |
| Cardiopulmonary | 14 (17) | |
| Intensive Care | 11 (13) | |
| Emergency Department | 10 (12) | |
| Surgical | 10 (12) | |
| Medical | 10 (12) | |
| Cancer | 6 (7) | |
| Women & Men’s health | 6 (7) | |
| Acute Neurological | 6 (7) | |
| Other (e.g., paediatrics, renal, chronic disease, palliative care) | 8 (10) | |
| Current workload | ||
| Mean (SD) number of patients seen in a typical workday | Inpatient | 10.2 (2.6) |
| Outpatient | 8.0 (4.5) | |
| Mixed | 6.5 (2.3) | |
| Mean (SD) time spent with patient per session (min) | Inpatient | 32.8 (11.6) |
| Outpatient | 46.7 (20.3) | |
| Mixed | 46.8 (11.7) | |
| Mean (SD) number of occasions of service before discharged | Inpatient | 8.8 (12.8) |
| Outpatient | 6.4 (3.9) | |
| Mixed | 8.4 (14.1) | |
| Mean (SD) number of new patients seen per week | Inpatient | 10.8 (7.2) |
| Outpatient | 9.2 (11.3) | |
| Mixed | 9.6 (8.7) | |
| Training | ||
| Attended training on behaviour change/ motivational interviewing/ health coaching, yes, n (%) | 30 (36) | |
| Demographic Categories | Mean (SD) Number of PA Counselling Elements Used |
|---|---|
| PT years of experience | |
| <2 years (n = 17) | 4.0 (3.0) |
| 2 ≤ 5yrs (n = 23) | 5.0 (3.6) |
| 5 ≤ 8yrs (n = 13) | 5.7 (3.5) |
| 8 ≤ 12yrs (n = 10) | 3.8 (3.4) |
| >12 years (n = 20) | 5.1 (3.6) |
| Setting | |
| Inpatient (n = 43) | 3.6 (3.0) |
| Outpatient/community (n = 29) | 6.6 (3.5) |
| Mixed inpatient/outpatient (n = 12) | 5.3 (2.7) |
| Area of physio practice * | |
| MSK; Rheum; Hands (n = 19) | 5.1 (2.9) |
| Orthopaedics (n = 17) | 4.8 (3.2) |
| Rehabilitation (n = 21) | 5.7 (3.8) |
| Aged care (n = 17) | 5.5 (4.1) |
| Cardiopulmonary (n = 14) | 4.9 (3.2) |
| ED (n = 10) | 6.7 (3.5) |
| Cancer (n = 6) | 4.2 (3.4) |
| Medical (n = 10) | 2.7 (1.7) |
| Women and Men’s Health (n = 6) | 5.3 (3.6) |
| Surgical (n = 10) | 3.7 (2.9) |
| ICU (n = 11) | 4.5 (3.2) |
| Neuro (n = 6) | 4 (3.3) |
| Other: Paediatrics, Renal, Palliative (n = 8) | 3.5 (2.4) |
| Yes n (%) | No n (%) | Unsure n (%) | |
|---|---|---|---|
| Ready to be referred directly to community PA programs | 26 (32) | 44 (54) | 12 (15) |
| Would benefit from a transitional stage with a health professional-led program | 76 (90) | 2 (2) | 6 (7) |
| Require further treatment from a health professional prior to referral | 59 (71) | 12 (14) | 12 (14) |
| Benefit from supported introduction or extra advice about community PA programs from a health professional | 79 (94) | 2 (2) | 3 (4) |
| Mean (SD) | Percentage of Total Barriers Reported in Each Category | |
|---|---|---|
| Total barriers reported (0–53) | 25.1 (8.7) | 47 |
| Capability (0–28) | 13.3 (5.7) | 47 |
| Knowledge (0–14) | 7.6 (2.6) | 54 |
| Cognition (0–13) | 5.0 (3.8) | 39 |
| Opportunity (0–12) | 7.1 (2.9) | 59 |
| Physical (0–7) | 4.7 (1.8) | 67 |
| Social (0–5) | 2.4 (1.7) | 47 |
| Motivation (0–13) | 4.8 (2.9) | 37 |
| Number (95% CI) PA counselling elements * | p value | |
| Total barriers | −0.3 (−0.3 to −0.2) | <0.01 |
| Barriers in Capability | −0.3 (−0.4 to −0.2) | <0.01 |
| Barriers in Opportunity | −0.2 (−0.4 to 0.1) | 0.21 |
| Barriers in Motivation | −0.2 (−0.4 to 0.1) | 0.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, S.; Sherrington, C.; Jennings, M.; Brady, B.; Pinheiro, M.; Dennis, S.; Christie, L.J.; Sidhu, B.; Haynes, A.; Greaves, C.; et al. Current Practice of Physical Activity Counselling within Physiotherapy Usual Care and Influences on Its Use: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2021, 18, 4762. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094762
Zhu S, Sherrington C, Jennings M, Brady B, Pinheiro M, Dennis S, Christie LJ, Sidhu B, Haynes A, Greaves C, et al. Current Practice of Physical Activity Counselling within Physiotherapy Usual Care and Influences on Its Use: A Cross-Sectional Survey. International Journal of Environmental Research and Public Health. 2021; 18(9):4762. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094762
Chicago/Turabian StyleZhu, Shiyi, Catherine Sherrington, Matthew Jennings, Bernadette Brady, Marina Pinheiro, Sarah Dennis, Lauren J. Christie, Balwinder Sidhu, Abby Haynes, Colin Greaves, and et al. 2021. "Current Practice of Physical Activity Counselling within Physiotherapy Usual Care and Influences on Its Use: A Cross-Sectional Survey" International Journal of Environmental Research and Public Health 18, no. 9: 4762. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094762