
Radiation-Induced Recurrent Vesicovaginal Fistula—Treatment with Adjuvant Platelet-Rich Plasma Injection and Martius Flap Placement—Case Report and Review of Literature

 , and
, and {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
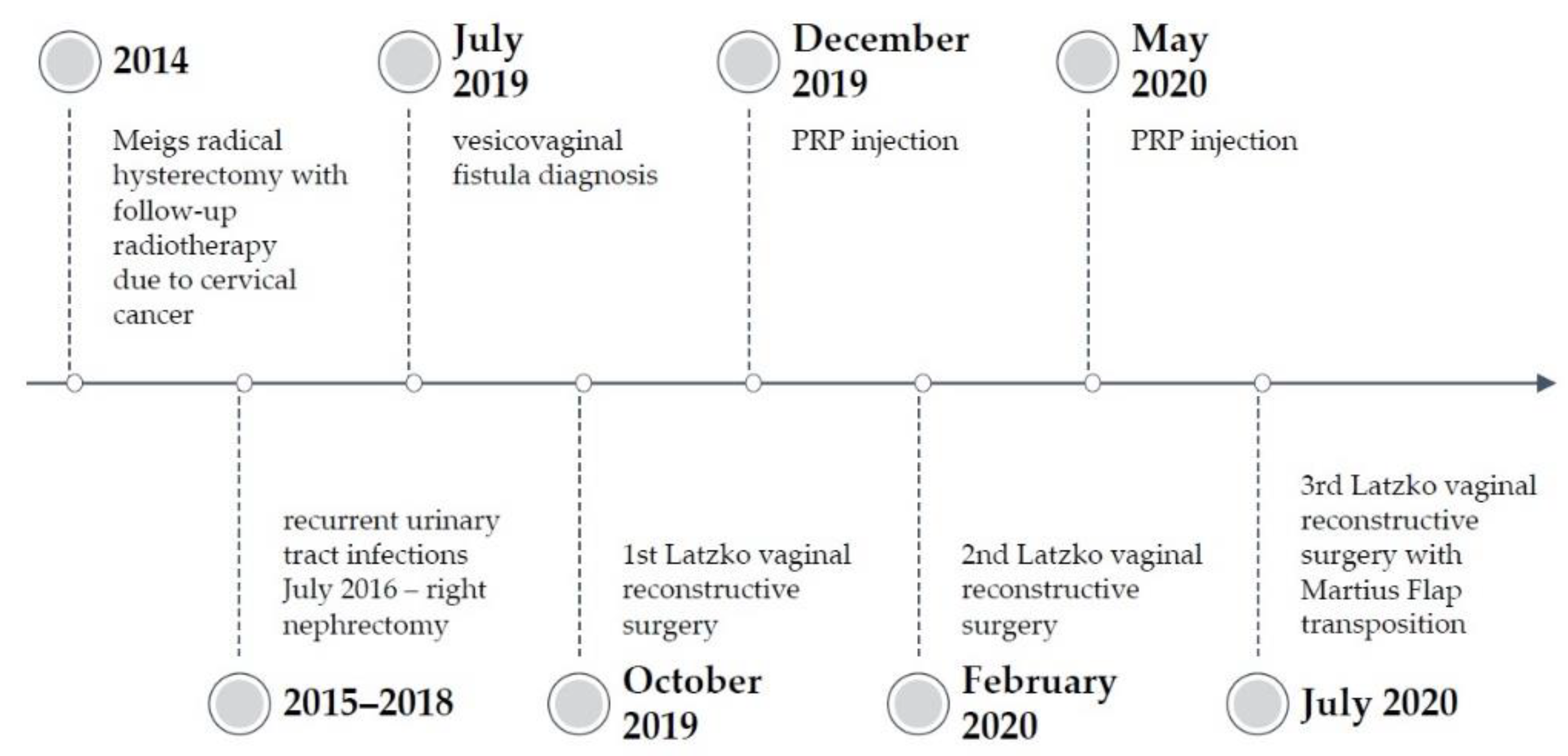
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Abrams, P.; Cardozo, L.; Khoury, S.; Wein, A. Incontinence, 5th ed.; International Consultation on Urological Diseases: Bristol, UK, 2013.
- Harkki-Siren, P.; Sjoberg, J.; Tiitinen, A. Urinary Tract Injuries after Hysterectomy. Obstet. Gynecol. Surv. 1998, 92, 113–118. [Google Scholar] [CrossRef]
- Stamatakos, M.; Sargedi, C.; Stasinou, T.; Kontzoglou, K. Vesicovaginal Fistula: Diagnosis and Management. Indian J. Surg. 2014, 76, 131–136. [Google Scholar] [CrossRef] [Green Version]
- Streit–Ciećkiewicz, D.; Nowakowski, Ł.; Grzybowska, M.E.; Futyma, K. Predictive Value of Classification Systems and Single Fistula-Related Factors in Surgical Management of Vesicovaginal Fistula. Neurourol. Urodyn. 2021, 40, 529–537. [Google Scholar] [CrossRef]
- Maier, U.; Ehrenböck, P.M.; Hofbauer, J. Late Urological Complications and Malignancies after Curative Radiotherapy for Gynecological Carcinomas: A Retrospective Analysis of 10,709 Patients. J. Urol. 1997, 158, 814–817. [Google Scholar] [CrossRef]
- Bhatla, N.; Berek, J.S.; Cuello Fredes, M.; Denny, L.A.; Grenman, S.; Karunaratne, K.; Kehoe, S.T.; Konishi, I.; Olawaiye, A.B.; Prat, J.; et al. Revised FIGO Staging for Carcinoma of the Cervix Uteri. Int. J. Gynecol. Obstet. 2019, 145, 129–135. [Google Scholar] [CrossRef]
- Streit-Ciećkiewicz, D.; Futyma, K.; Miotła, P.; Grzybowska, M.E.; Rechberger, T. Platelet-Rich Plasma as Adjuvant Therapy for Recurrent Vesicovaginal Fistula: A Prospective Case Series. J. Clin. Med. 2019, 8, 2122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moses, R.A.; Ann Gormley, E. State of the Art for Treatment of Vesicovaginal Fistula. Curr. Urol. Rep. 2017, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kopp, D.M.; Tang, J.H.; Bengtson, A.M.; Chi, B.H.; Moyo, M.; Wilkinson, J. Continence, Quality of Life, and Depression Following Surgical Repair of Obstetric Vesicovaginal Fistula: A Cohort Study. BJOG 2020, 126, 926–934. [Google Scholar] [CrossRef]
- Singh, V.; Mehrotra, S.; Bansal, A.; Akhtar, A.; Sinha, R.J. Prospective Randomized Comparison of Repairing Vesicovaginal Fistula with or without the Interposition Flap: Result from a Tertiary Care Institute in Northern India. Turkish J. Urol. 2019, 45, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Rangnekar, N.P.; Imdad Ali, N.; Kaul, S.A.; Pathak, H.R. Role of the Martins Procedure in the Management of Urinary-Vaginal Fistulas. J. Am. Coll. Surg. 2000, 191, 259–263. [Google Scholar] [CrossRef]
- Ghosh, B.; Wats, V.; Pal, D.K. Comparative Analysis of Outcome between Laparoscopic versus Open Surgical Repair for Vesico-Vaginal Fistula. Obstet. Gynecol. Sci. 2016, 59, 525. [Google Scholar] [CrossRef] [Green Version]
- Lobo, N.; Kulkarni, M.; Hughes, S.; Nair, R.; Khan, M.S.; Thurairaja, R. Urologic Complications Following Pelvic Radiotherapy. Urology 2018, 122, 1–9. [Google Scholar] [CrossRef]
- Pushkar, D.Y.; Dyakov, V.V.; Kasyan, G.R. Management of Radiation-Induced Vesicovaginal Fistula. Eur. Urol. 2009, 55, 131–138. [Google Scholar] [CrossRef]
- Barone, M.A.; Frajzyngier, V.; Ruminjo, J.; Asiimwe, F.; Barry, T.H.; Bello, A.; Danladi, D.; Ganda, S.O.; Idris, S.A.; Inoussa, M.; et al. Determinants of Postoperative Outcomes of Female Genital Fistula Repair Surgery. Obs. Gynecol. 2012, 120, 524–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bengtson, A.M.; Kopp, D.; Tang, J.H.; Chipungu, E.; Moyo, M.; Wilkinson, J. Identifying Patients with Vesicovaginal Fistula at High Risk of Urinary Incontinence After Surgery. Obs. Gynecol. 2016, 128, 945–953. [Google Scholar] [CrossRef]
- Reiss, R.F.; Oz, M.C. Autologous Fibrin Glue: Production and Clinical Use. Transfus. Med. Rev. 1996, 10, 85–92. [Google Scholar] [CrossRef]
- Sierra, D.H. Fibrin Sealant Adhesive Systems: A Review of Their Chemistry, Material Properties and Clinical Applications. J. Biomater. Appl. 1993, 7, 309–352. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.K.; Perry, K.T.; Turk, T.M.T. Endoscopic Injection of Fibrin Glue for the Treatment of Urinary-Tract Pathology. J. Endourol. 2005, 19, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Lubkowska, A.; Dolegowska, B.; Banfi, G. Growth Factor Content in PRP and Their Applicability in Medicine. J. Biol. Regul. Homeost. Agents 2012, 26(2 Suppl. 1), 3S–22S. [Google Scholar]
- Dawood, A.S.; Salem, H.A. Current Clinical Applications of Platelet-Rich Plasma in Various Gynecological Disorders: An Appraisal of Theory and Practice. Clin. Exp. Reprod. Med. 2018, 45, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Siemińska, L. Adipose tissue. Pathophysiology, distribution, sex differences and the role in inflammation and cancerogenesis. Endokrynol. Polska 2007, 58, 330–342. [Google Scholar]
- Leach, D.A.; Gebhart, J.B. Martius labial fat pad graft (use in rectovaginal fistula repair). Int. Urogynecol. J. 2020. [CrossRef] [PubMed]
- Kasyan, G.; Tupikina, N.; Pushkar, D. Use of Martius flap in the complex female urethral surgery. Cent. Eur. J. Urol. 2014, 67, 202–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kołodyńska, A.; Streit-Ciećkiewicz, D.; Kot, A.; Kuliniec, I.; Futyma, K. Radiation-Induced Recurrent Vesicovaginal Fistula—Treatment with Adjuvant Platelet-Rich Plasma Injection and Martius Flap Placement—Case Report and Review of Literature. Int. J. Environ. Res. Public Health 2021, 18, 4867. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094867
Kołodyńska A, Streit-Ciećkiewicz D, Kot A, Kuliniec I, Futyma K. Radiation-Induced Recurrent Vesicovaginal Fistula—Treatment with Adjuvant Platelet-Rich Plasma Injection and Martius Flap Placement—Case Report and Review of Literature. International Journal of Environmental Research and Public Health. 2021; 18(9):4867. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094867
Chicago/Turabian StyleKołodyńska, Aleksandra, Dominika Streit-Ciećkiewicz, Agata Kot, Iga Kuliniec, and Konrad Futyma. 2021. "Radiation-Induced Recurrent Vesicovaginal Fistula—Treatment with Adjuvant Platelet-Rich Plasma Injection and Martius Flap Placement—Case Report and Review of Literature" International Journal of Environmental Research and Public Health 18, no. 9: 4867. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094867