
Effects of Focal Knee Joint Cooling on Static and Dynamic Strength of the Quadriceps: Innovative Approach to Muscle Conditioning


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
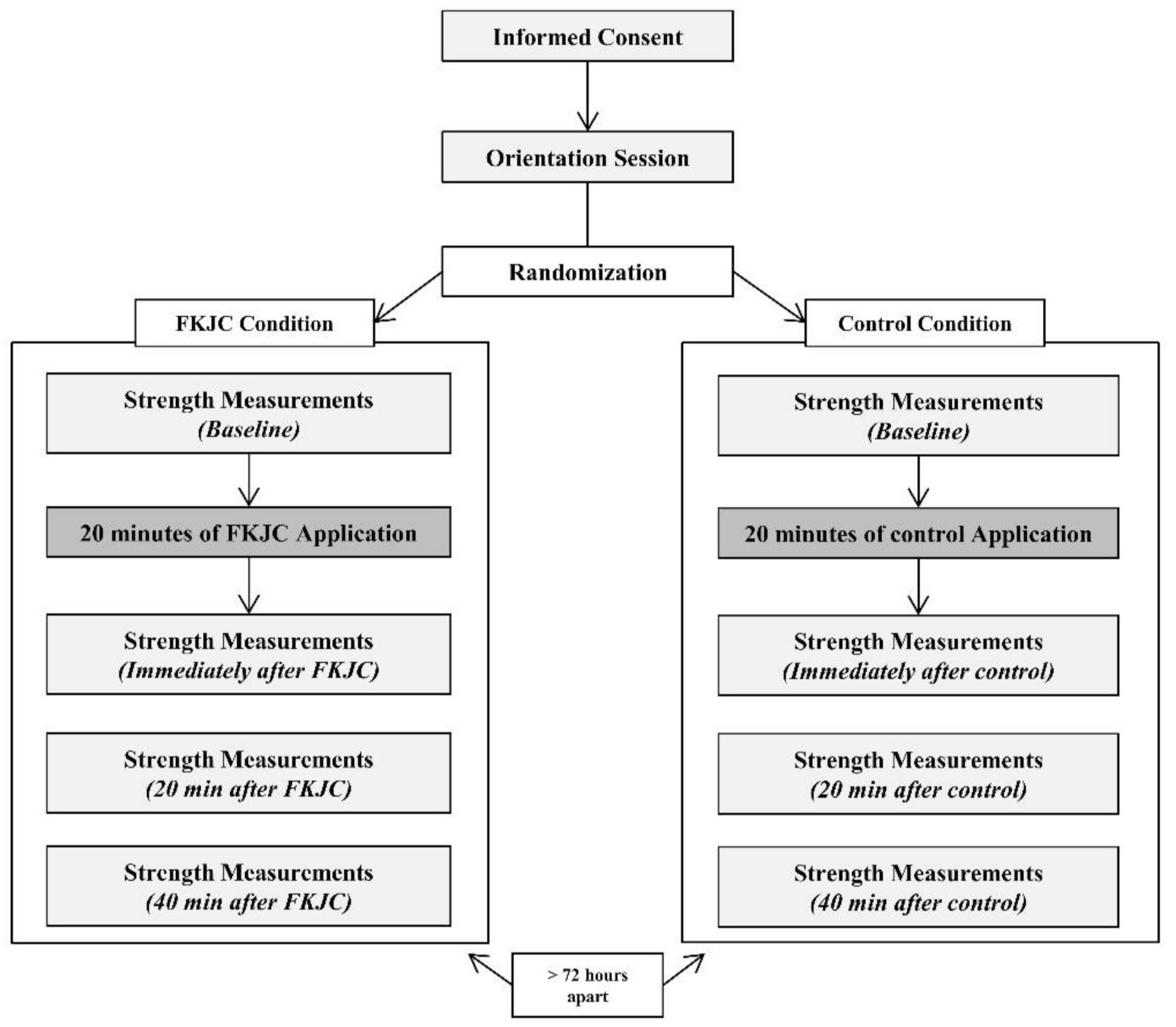
2.1. Design
2.2. Participants
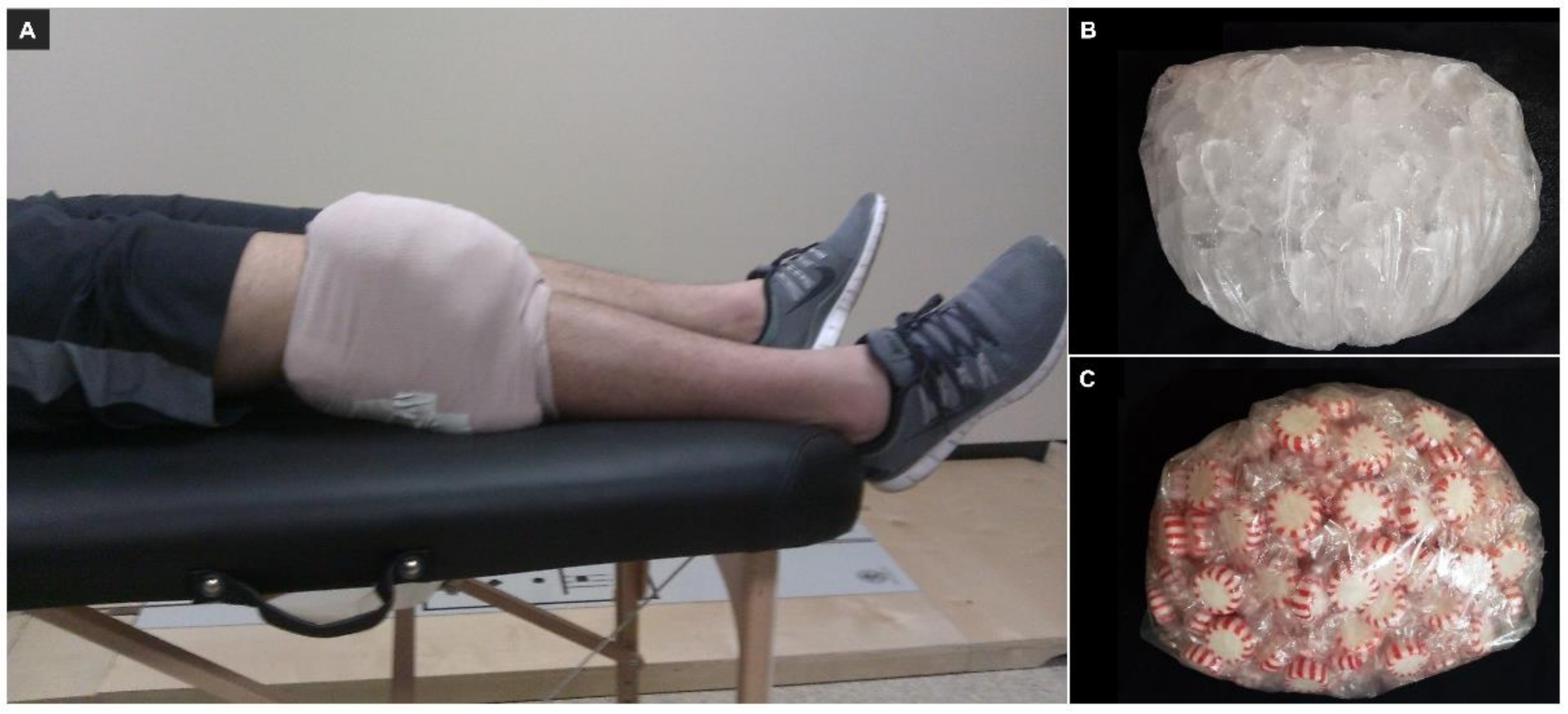
2.3. Procedures
2.4. Statistical Analysis
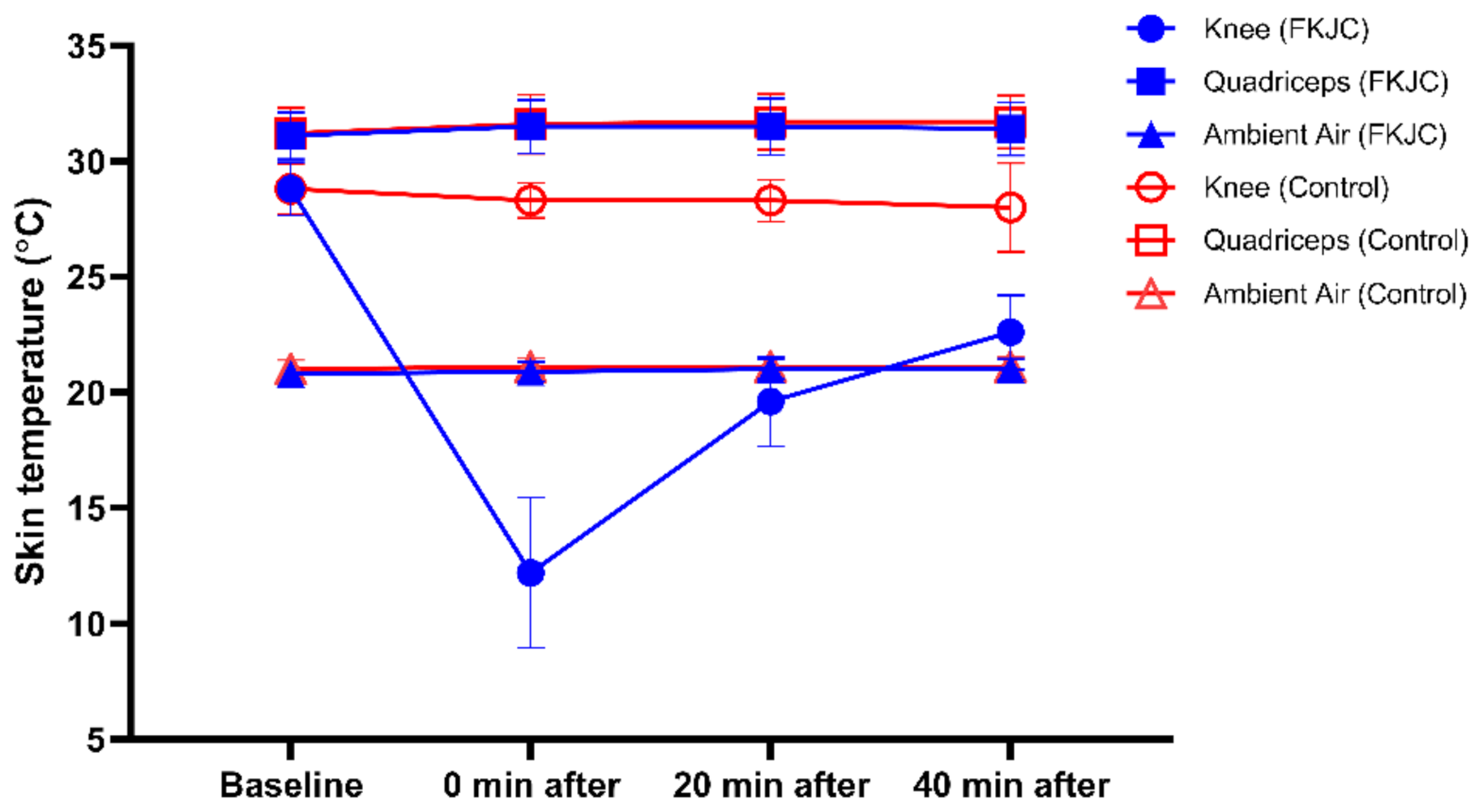
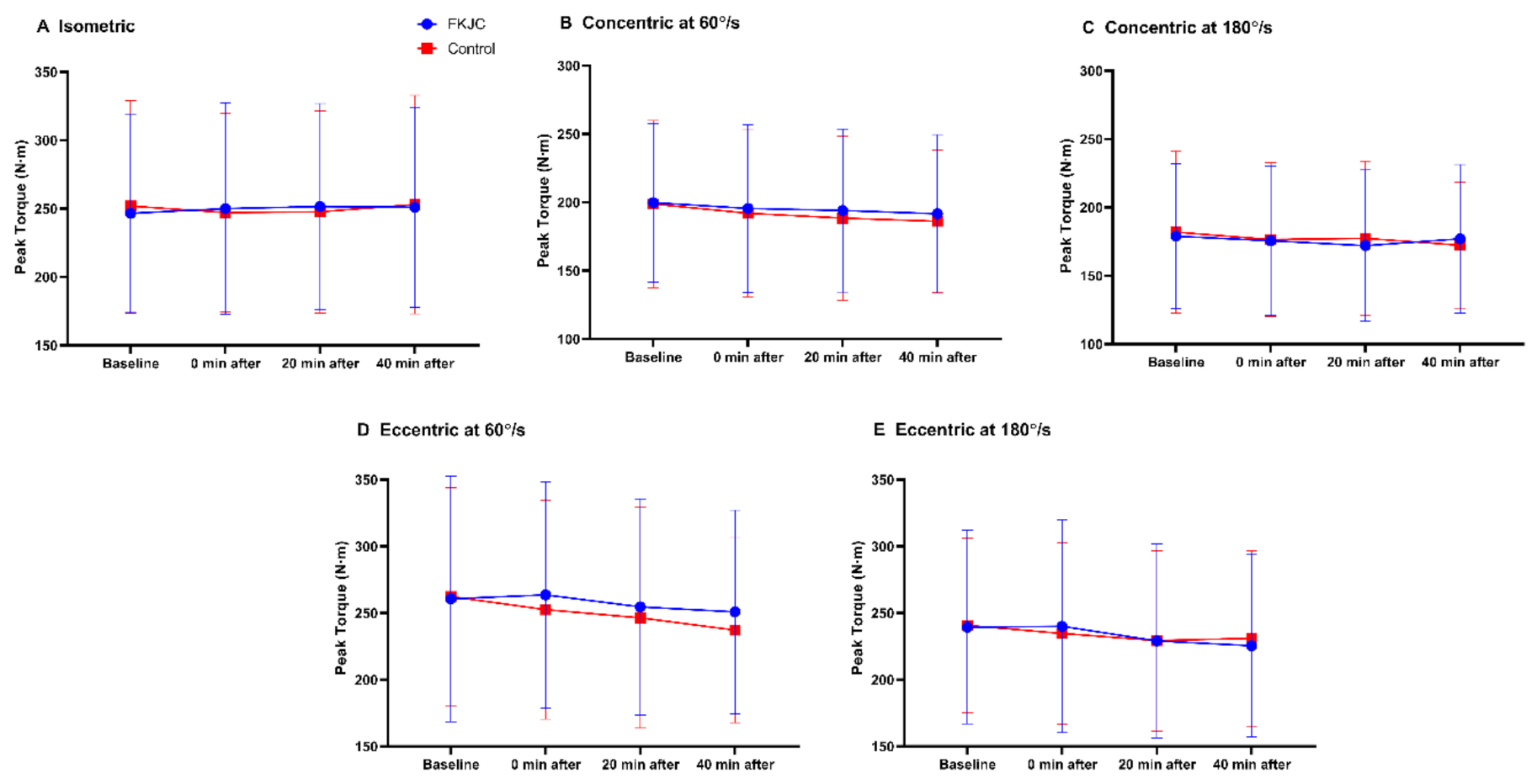
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harkey, M.S.; Gribble, P.A.; Pietrosimone, B.G. Disinhibitory Interventions and Voluntary Quadriceps Activation: A Systematic Review. J. Athl. Train. 2014, 49, 411–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, J.A.; Chaudhari, A.M.W.; Schmitt, L.C.; Best, T.M.; Siston, R.A. Gluteus Maximus and Soleus Compensate for Simulated Quadriceps Atrophy and Activation Failure during Walking. J. Biomech. 2013, 46, 2165–2172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeow, C.H. Hamstrings and Quadriceps Muscle Contributions to Energy Generation and Dissipation at the Knee Joint during Stance, Swing and Flight Phases of Level Running. Knee 2013, 20, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Fischer, F.; Blank, C.; Dunnwald, T.; Gfoller, P.; Herbst, E.; Hoser, C.; Fink, C. Isokinetic Extension Strength Is Associated With Single-Leg Vertical Jump Height. Orthop. J. Sports Med. 2017, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrissey, M.C.; Harman, E.A.; Johnson, M.J. Resistance Training Modes: Specificity and Effectiveness. Med. Sci. Sports Exerc. 1995, 27, 648–660. [Google Scholar] [CrossRef] [PubMed]
- De Ruiter, C.J.; Van Leeuwen, D.; Heijblom, A.; Bobbert, M.F.; de Haan, A. Fast Unilateral Isometric Knee Extension Torque Development and Bilateral Jump Height. Med. Sci. Sports Exerc. 2006, 38, 1843–1852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dowson, M.N.; Nevill, M.E.; Lakomy, H.K.; Nevill, A.M.; Hazeldine, R.J. Modelling the Relationship between Isokinetic Muscle Strength and Sprint Running Performance. J. Sports Sci. 1998, 16, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Cometti, G.; Maffiuletti, N.A.; Pousson, M.; Chatard, J.C.; Maffulli, N. I Isokinetic Strength and Anaerobic Power of Elite, Subelite and Amateur French Soccer Players. Int. J. Sports Med. 2001, 22, 45–51. [Google Scholar] [CrossRef]
- Lee, S.E.K.; Lira, C.A.B.; Nouailhetas, V.L.A.; Vancini, R.L.; Andrade, M.S. Do Isometric, Isotonic and/or Isokinetic Strength Trainings Produce Different Strength Outcomes? J. Bodyw. Mov. 2018, 22, 430–437. [Google Scholar] [CrossRef]
- Keays, S.L.; Bullock-Saxton, J.E.; Newcombe, P.; Keays, A.C. The Relationship between Knee Strength and Functional Stability before and after Anterior Cruciate Ligament Reconstruction. J. Orthop. Res. 2003, 21, 231–237. [Google Scholar] [CrossRef]
- Knoll, Z.; Kiss, R.M.; Kocsis, L. Gait adaptation in ACL Deficient Patients before and after Anterior Cruciate Ligament Reconstruction Surgery. J. Electromyogr. Kinesiol. 2004, 14, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Hausswirth, C.; Louis, J.; Bieuzen, F.; Pournot, H.; Fournier, J.; Filliard, J.R.; Brisswalter, J. Effects of Whole-Body Cryotherapy vs. Far-Infrared vs. Passive Modalities on Recovery from Exercise-Induced Muscle Damage in Highly-Trained Runners. PLoS ONE 2011, 6, e27749. [Google Scholar] [CrossRef] [Green Version]
- Fonda, B.; Sarabon, N. Effects of Whole-Body Cryotherapy on Recovery after Hamstring Damaging Exercise: A Crossover Study. Scand. J. Med. Sci. Sports 2013, 23, e270–e278. [Google Scholar] [CrossRef]
- Bailey, D.M.; Erith, S.J.; Griffin, P.J.; Dowson, A.; Brewer, D.S.; Gant, N.; Williams, C. Influence of Cold-Water Immersion on Indices of Muscle Damage following Prolonged Intermittent Shuttle Running. J. Sports Sci. 2007, 25, 1163–1170. [Google Scholar] [CrossRef]
- Banfi, G.; Lombardi, G.; Colombini, A.; Melegati, G. Whole-Body Cryotherapy in Athletes. Sports Med. 2010, 40, 509–517. [Google Scholar] [CrossRef]
- Bleakley, C.M.; McDonough, S.M.; MacAuley, D.C.; Bjordal, J. Cryotherapy for Acute Ankle Sprains: A Randomised Controlled Study of Two Different Icing Protocols. Br. J. Sports Med. 2006, 40, 700–705. [Google Scholar] [CrossRef]
- Lessard, L.A.; Scudds, R.A.; Amendola, A.; Vaz, M.D. The Efficacy of Cryotherapy Following Arthroscopic Knee Surgery. J. Orthop. Sports Phys. Ther. 1997, 26, 14–22. [Google Scholar] [CrossRef] [Green Version]
- Swenson, C.; Sward, L.; Karlsson, J. Cryotherapy in Sports Medicine. Scand. J. Med. Sci. Sports 1996, 6, 193–200. [Google Scholar] [CrossRef]
- Bleakley, C.M.; Costello, J.T.; Glasgow, P.D. Should Athletes Return to Sport After Applying Ice? A Systematic Review of the Effect of Local Cooling on Functional Performance. Sports Med. 2012, 42, 69–87. [Google Scholar] [CrossRef] [Green Version]
- Loro, W.A.; Thelen, M.D.; Rosenthal, M.D.; Stoneman, P.D.; Ross, M.D. Effects of Cryotherapy on Quadriceps Electromyographic Activity and Isometric Strength in Patient in the Early Phases following Knee Surgery. J. Orthop. Surg. 2019, 27. [Google Scholar] [CrossRef]
- Rice, D.; McNair, P.J.; Dalbeth, N. Effects of Cryotherapy on Arthrogenic Muscle Inhibition Using an Experimental Model of Knee Swelling. Arthritis Rheum. 2009, 61, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Pietrosimone, B.G.; Ingersoll, C.D. Focal Knee Joint Cooling Increases the Quadriceps Central Activation Ratio. J. Sports Sci. 2009, 27, 873–879. [Google Scholar] [CrossRef] [PubMed]
- Hart, J.M.; Kuenze, C.M.; Diduch, D.R.; Ingersoll, C.D. Quadriceps Muscle Function after Rehabilitation with Cryotherapy in Patients with Anterior Cruciate Ligament Reconstruction. J. Athl. Train. 2014, 49, 733–739. [Google Scholar] [CrossRef] [Green Version]
- Pietrosimone, B.G.; Hart, J.M.; Saliba, S.A.; Hertel, J.; Ingersoll, C.D. Immediate Effects of Transcutaneous Electrical Nerve Stimulation and Focal Knee Joint Cooling on Quadriceps Activation. Med. Sci. Sports Exerc. 2009, 41, 1175–1181. [Google Scholar] [CrossRef]
- Hopkins, J.T.; Ingersoll, C.D.; Edwards, J.; Klootwyk, T.E. Cryotherapy and Transcutaneous Electric Neuromuscular Stimulation Decrease Arthrogenic Muscle Inhibition of the Vastus Medialis after Knee Joint Effusion. J. Athl. Train. 2002, 37, 125. [Google Scholar]
- Alegre, L.M.; Hasler, M.; Wenger, S.; Nachbauer, W.; Csapo, R. Does Knee Joint Cooling Change in Vivo Patellar Tendon Mechanical Properties? Eur. J. Appl. Physiol. 2016, 116, 1921–1929. [Google Scholar] [CrossRef] [Green Version]
- Bojsen-Moller, J.; Magnusson, S.P.; Rasmussen, L.R.; Kjaer, M.; Aagaard, P. Muscle Performance during Maximal Isometric and Dynamic Contractions is Influenced by the Stiffness of the Tendinous Structures. J. Appl. Physiol. 2005, 99, 986–994. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, J.T.; Stencil, R. Ankle Cryotherapy Facilitates Soleus Function. J. Orthop. Sports Phys. 2002, 32, 622–627. [Google Scholar] [CrossRef] [Green Version]
- Alexander, J.; Rhodes, D. Temporal Patterns of Knee-Extensor Isokinetic Torque Strength in Male and Female Athletes Following Comparison of Anterior Thigh and Knee Cooling Over a Rewarming Period. J. Sport Rehabil. 2019, 29, 723–729. [Google Scholar] [CrossRef]
- Rhodes, D.; Alexander, J. The Effect of Knee Joint Cooling on Isokinetic Torque Production of the Knee Extensors: Considerations for Application. Int. J. Sports Phys. Ther. 2018, 13, 985–992. [Google Scholar] [CrossRef] [Green Version]
- Negrete, R.; Brophy, J. The Relationship Between Isokinetic Open and Closed Chain Lower Extremity Strength and Functional Performance. J. Sport Rehabil. 2000, 9, 46–61. [Google Scholar] [CrossRef]
- Atabek, H.Ç.; Sönmez, G.A.; Yılmaz, İ. The Relationship between Isokinetic Strength of Knee Extensors/Flexors, Jumping and Anaerobic Performance. Isokinet. Exerc. Sci. 2009, 17, 79–83. [Google Scholar] [CrossRef]
- Warner, B.; Kim, K.M.; Hart, J.M.; Saliba, S. Lack of Effect of Superficial Heat to the Knee on Quadriceps Function in Individuals With Quadriceps Inhibition. J. Sport Rehabil. 2013, 22, 93–99. [Google Scholar] [CrossRef]
- Marginson, V.; Eston, R. The Relationship between Torque and Joint Angle during Knee Extension in Boys and Men. J. Sports Sci. 2001, 19, 875–876. [Google Scholar] [CrossRef] [PubMed]
- Pincivero, D.M.; Salfetnikov, Y.; Campy, R.M.; Coelho, A.J. Angle- and Gender-Specific Quadriceps Femoris Muscle Recruitment and Knee Extensor Torque. J. Biomech. 2004, 37, 1689–1697. [Google Scholar] [CrossRef] [PubMed]
- Roberts, T.J. Contribution of Elastic Tissues to the Mechanics and Energetics of Muscle Function during Movement. J. Exp. Biol. 2016, 219, 266–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rice, D.A.; McNair, P.J. Quadriceps Arthrogenic Muscle Inhibition: Neural Mechanisms and Treatment Perspectives. Semin. Arthritis Rheum. 2010, 40, 250–266. [Google Scholar] [CrossRef] [PubMed]
- Furmanek, M.P.; Slomka, K.J.; Sobiesiak, A.; Rzepko, M.; Juras, G. The Effects of Cryotherapy on Knee Joint Position Sense and Force Production Sense in Healthy Individuals. J. Hum. Kinet. 2018, 61, 39–51. [Google Scholar] [CrossRef] [Green Version]
- Kimura, I.F.; Thompson, G.T.; Gulick, D.T. The Effect of Cryotherapy on Eccentric Plantar Flexion Peak Torque and Endurance. J. Athl. Train. 1997, 32, 124–126. [Google Scholar]
- Kim, H.; Lee, D.; Choi, H.M.; Park, J. Joint Cooling does not Hinder Athletic Performance during High-intensity Intermittent Exercise. Int. J. Sports Med. 2016, 37, 641–646. [Google Scholar] [CrossRef]
- Oosterveld, F.G.; Rasker, J.J.; Jacobs, J.W.; Overmars, H.J. The Effect of Local Heat and Cold Therapy on the Intraarticular and Skin Surface Semperature of the Knee. Arthritis Rheum. 1992, 35, 146–151. [Google Scholar] [CrossRef]
- Hohenauer, E.; Stoop, R.; Clarys, P.; Clijsen, R.; Deliens, T.; Taeymans, J. The Effect of Pre-Exercise Cooling on Performance Characteristics: A Systematic Review and Meta-Analysis. Int. J. Clin. Med. 2018, 9, 117–141. [Google Scholar] [CrossRef] [Green Version]
- Banfi, G.; Melegati, G.; Barassi, A.; Dogliotti, G.; d’Eril, G.M.; Dugue, B.; Corsi, M.M. Effects of Whole-Body Cryotherapy on Serum Mediators of Inflammation and Serum Muscle Enzymes in Athletes. J. Biol. 2009, 34, 55–59. [Google Scholar] [CrossRef]
- Partridge, E.M.; Cooke, J.; McKune, A.; Pyne, D.B. Whole-Body Cryotherapy: Potential to Enhance Athlete Preparation for Competition? Front. Physiol. 2019, 10, 1007. [Google Scholar] [CrossRef] [Green Version]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-S.; Mettler, J.A.; McCurdy, K.; Kim, K.-M. Effects of Focal Knee Joint Cooling on Static and Dynamic Strength of the Quadriceps: Innovative Approach to Muscle Conditioning. Int. J. Environ. Res. Public Health 2021, 18, 4890. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094890
Kim J-S, Mettler JA, McCurdy K, Kim K-M. Effects of Focal Knee Joint Cooling on Static and Dynamic Strength of the Quadriceps: Innovative Approach to Muscle Conditioning. International Journal of Environmental Research and Public Health. 2021; 18(9):4890. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094890
Chicago/Turabian StyleKim, Joo-Sung, Joni A. Mettler, Kevin McCurdy, and Kyung-Min Kim. 2021. "Effects of Focal Knee Joint Cooling on Static and Dynamic Strength of the Quadriceps: Innovative Approach to Muscle Conditioning" International Journal of Environmental Research and Public Health 18, no. 9: 4890. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094890