
Climate Change, Health Risks, and Vulnerabilities in Burkina Faso: A Qualitative Study on the Perceptions of National Policymakers

 , ,
, , 
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
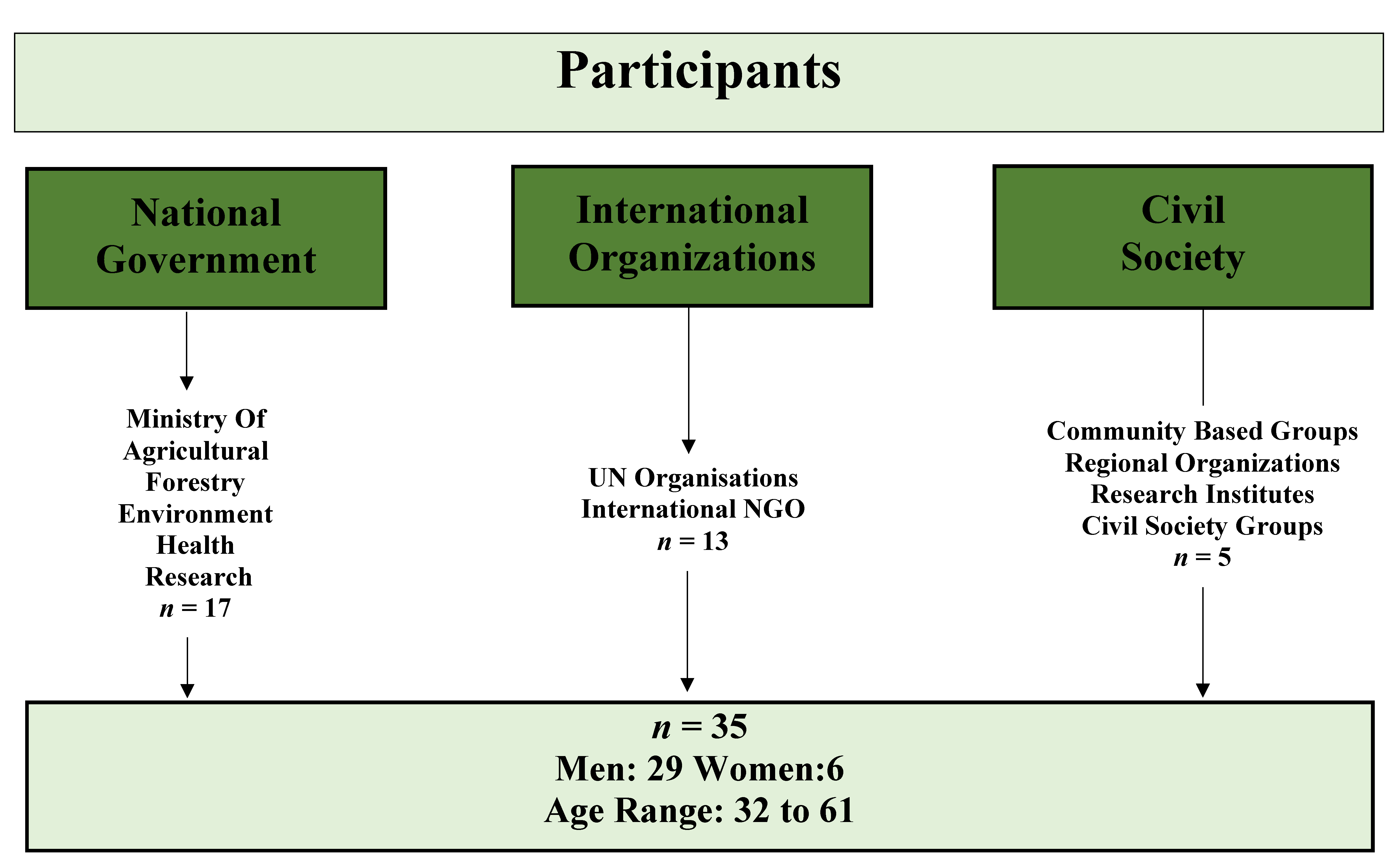
2. Materials and Methods
2.1. Data Collection
2.2. Data Analysis
2.3. Data Validation
- (1)
- To enhance the validity of the data, the investigator conducted a dissemination trip to Burkina Faso before publishing study results [46], presenting preliminary results to half of the study participants individually or in pairs and allowing them to provide feedback on the accurate representation of findings. The participants validated the study results prior to publication.
- (2)
- The implementation of the 32-item checklist of the Consolidated Criteria for Reporting Qualitative Research (COREQ) (Supplementary Material 1) ensured that key information about the study (research team, study design, participants, data analysis, reporting) was provided to the reader [47,48]. This information is essential for readers and scientists to assess the transferability of our study to other contexts. Data source comparison was conducted using interviews, daily observations, and weekly memos, in combination with researcher investigator triangulation (between RSo and MJ) through the first cycle coding of the transcripts, to bring together differing perspectives [49,50] and further ensure transferability [51].
3. Results
3.1. Perceptions of Climate Change
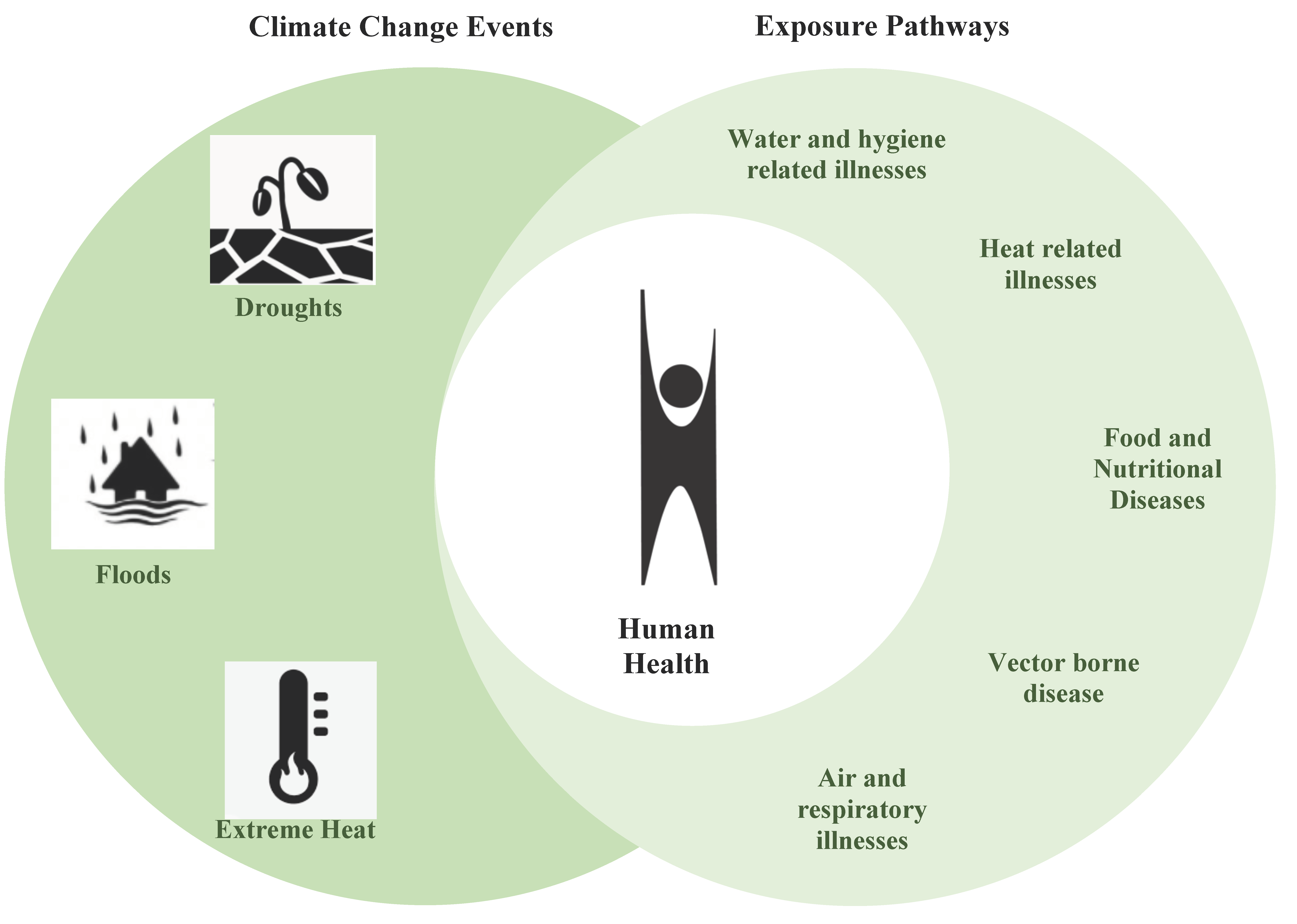
3.2. Perceptions of Climate Change: Health Risks and Vulnerabilities
3.3. Perceptions of Climate Change: Agricultural and Food Security Impacts
3.3.1. Agriculture
3.3.2. Food Security
4. Discussion
4.1. Perceptions of Climate Change
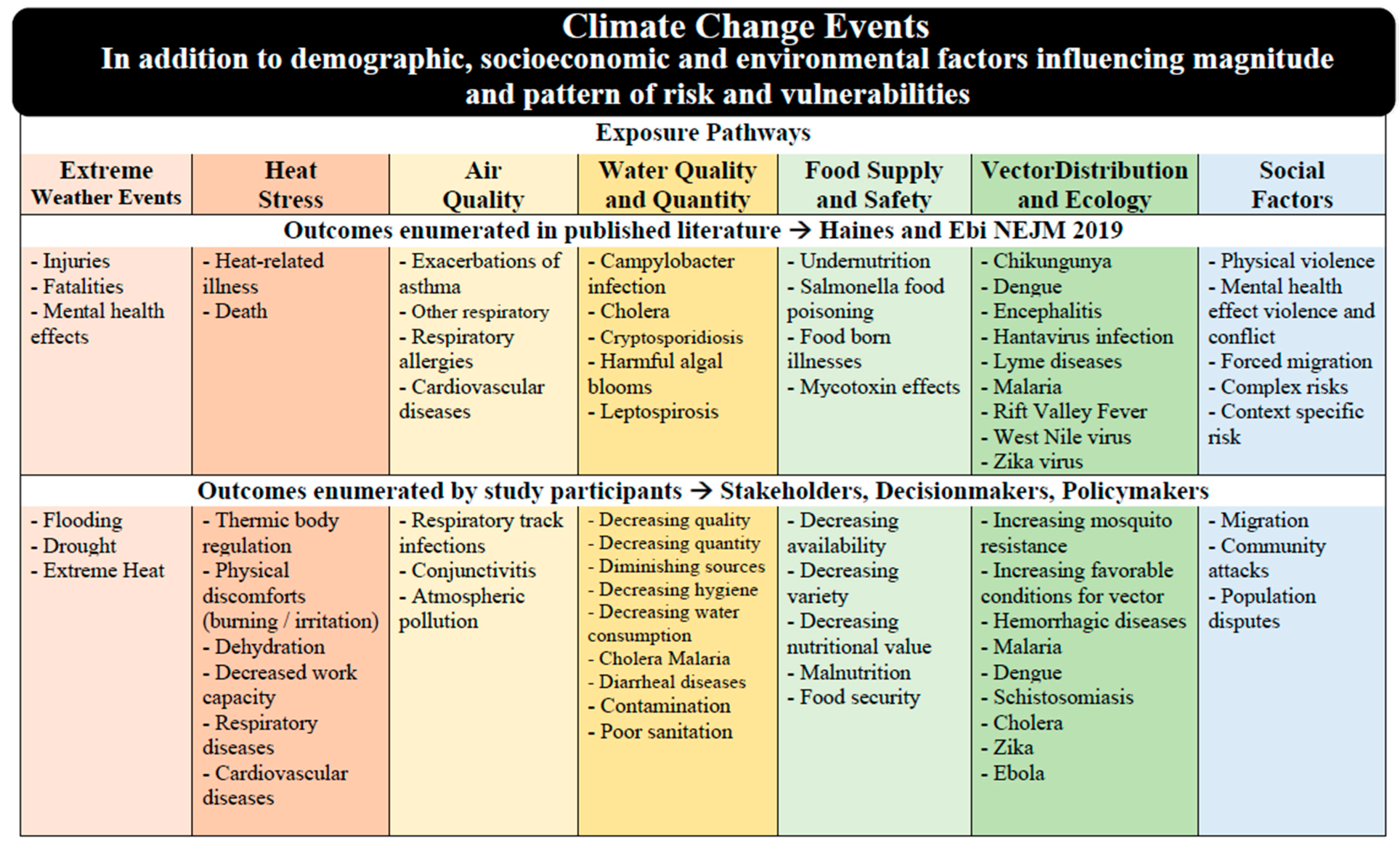
4.2. Perceptions of Climate Change, Health Risks and Vulnerabilities: Congruence with Scientific Evidence?
4.3. Perceptions of Climate Change: Agriculture and Food Security Impacts
4.4. Recommendation for Research and Policy
- (i)
- Identifying and surveilling vulnerable groups to CC hazards and health outcomes through a two-tier system. Our study highlighted the vulnerability of particular groups to CC hazards and resulting health outcomes, notably the elderly and young children. SDPs discussed the lack of information, data, and statistics collected around the outcomes of CC on the health of the population. We recommend the implementation of a climate-health impact surveillance system with a two-part focus (a) identifying and assisting vulnerable populations in times of CC events such as heat waves and (b) collecting information, data, and statistics on the health outcomes at the populations level, so the relevant institutions can better understand, learn, adapt and react to safeguard human health during future CC events.
- (ii)
- Training of SDPs on mental health consequences and social factors influencing and resulting from CC. This study has identified gaps in SDPs’ perceptions of social factors interaction with CC&H, more specifically regarding mental health and complex risks. To address this minor gap, training relevant stakeholders should be offered. While closing this knowledge gap, the training would also draw attention to these issues, strengthen the expertise of key stakeholders, decision-makers and policymakers and increase their awareness further edging them towards action.
- (iii)
- Investigating where Burkina Faso is in the process of creating a CC&H adaptation policy. This study illustrates that SDPs are knowledgeable about CC&H risks and vulnerabilities, therefore, research should look beyond awareness and towards political will. We suggest investigating if and how this SDP awareness is driving policy to address the issue of CC&H by examining where Burkina Faso is in the process of drafting adaptation policies. Future research through a policy frame should investigate the factors, besides knowledge and awareness which will influence the formation of CC&H adaptation policy by determining (1) how the problem of CC&H is framed in the public and political discourse; (2) which political majorities for or against CC&H policies exist; and (3) what CC&H policy alternatives, barriers, and possibilities exist currently in Burkina Faso. This will provide an outlook and overview on the factors already in play in Burkina Faso’s policy process, and how best the process can be moved toward the goal of a formulated and implemented CC&H adaption policy.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- McMichael, A.J.; Friel, S.; Nyong, A.; Corvalan, C. Global environmental change and health: Impacts, inequalities, and the health sector. BMJ 2008, 336, 191–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMichael, A.J.; Woodruff, R.E.; Hales, S. Climate change and human health: Present and future risks. Lancet 2006, 367, 859–869. [Google Scholar] [CrossRef]
- UNFPA. The State of World Population Report 2009: Facing a Changing World: Women, Population and Climate; UNFPA: New York, NY, USA, 2009; pp. 1–104. ISBN 978-0-89714-958-7. [Google Scholar]
- UNDP. Human Development Report 2007: Background Paper on Risks, Vulnerability and Adaptation in Bangladesh; Bangladesh Centre for Advanced Studies : Dhaka, Bangladesh, 2007. [Google Scholar]
- Haines, A.; Kovatsa, R.S.; Campbell-Lendrumb, D.; Corvalanb, C. Climate change and human health: Impacts, vulnerability and public health. J. R. Inst. Public Health 2006, 7, 585–596. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, J.; Newman, K.; Mayhew, S. Population dynamics and climate change: What are the links? J. Public Health 2010, 32, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Barnett, J. Security and climate change. Glob. Environ. Chang. 2003, 13, 7–17. [Google Scholar] [CrossRef] [Green Version]
- Tyagi, S.; Garg, N.; Paudel, R. Environmental degradation: Causes and consequences. Eur. Res. 2014, 81, 1491. [Google Scholar]
- Woodward, A.; Smith, K. Chapter 11. Human Health: Impacts, Adaptation, and Co-Benefits. IPCC WGII AR5 2014, 69. [Google Scholar] [CrossRef]
- IPCC. Summary for Policymakers. In Global Warming of 1.5 °C. An IPCC Special Report on the Impacts of Global Warming of 1.5 °C above Pre-Industrial Levels and Related Global Greenhouse Gas Emission Pathways, in the Context of Strengthening the Global Response to the Threat of Climate Change, Sustainable Development, and Efforts to Eradicate Poverty; IPCC: New York, NY, USA, 2018. [Google Scholar]
- IPCC. Glossary of terms. In Managing the Risks of Extreme Events and Disasters to Advance Climate Change Adaptation; Intergovermental Panel on Climate Change; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2012; pp. 555–564. [Google Scholar]
- Wittig, R.; König, K.; Schmidt, M.; Szarzynski, J. A study of climate change and anthropogenic impacts in West Africa. Environ. Sci. Pollut. Res.-Int. 2007, 14, 182–189. [Google Scholar] [CrossRef]
- Kotir, J.H. Climate change and variability in Sub-Saharan Africa: A review of current and future trends and impacts on agriculture and food security. Environ. Dev. Sustain. 2011, 13, 587–605. [Google Scholar] [CrossRef]
- UNFCCC. United Nations Framework Convention On Climate Change Parties & Observers. Available online: https://unfccc.int/parties-observers (accessed on 8 September 2020).
- Sorgho, R.; Mank, I.; Kagoné, M.; Souares, A.; Danquah, I.; Sauerborn, R. We will always ask ourselves the question of how to feed the family: Subsistence farmers perceptions on adaptation to climate change in Burkina Faso. Int. J. Environ. Res. Public Health 2020, 17, 7200. [Google Scholar] [CrossRef]
- Laux, P.W.S.; Wagner, A.; Jacobeit, J.; Bardossy, A.; Kunstmann, H. Modelling daily precipitation features in the Volta basin of West Africa. Int. J. Climatol. 2009, 29, 937–954. [Google Scholar] [CrossRef] [Green Version]
- Barry, A.A.; Caesar, J.; Klein Tank, A.M.G.; Aguilar, E.; McSweeney, C.; Cyrille, A.M.; Nikiema, M.P.; Narcisse, K.B.; Sima, F.; Stafford, G.; et al. West Africa climate extremes and climate change indices. Int. J. Climatol. 2018, 38, e921–e938. [Google Scholar] [CrossRef]
- Ibrahim, B.; Karambiri, H.; Polcher, J.; Yacouba, H.; Ribstein, P. Changes in rainfall regime over Burkina Faso under the climate change conditions simulated by 5 regional climate models. Clim. Dyn. 2014, 42, 1363–1381. [Google Scholar] [CrossRef] [Green Version]
- Hondula, D.M.; Rocklöv, J.; Sankoh, O.A. Past, present and future climate at select INDEPTH member Health and Demographic Surveillance Systems in Africa and Asia. Glob. Health Action 2012, 5, 19083. [Google Scholar] [CrossRef]
- Ministry of Environment. DECRET N° 2016383/PRES/PM/MEEVCC. In N° 2016383; Burkina Faso, Ed.; Cabinet of the President of Burkina Faso: Ouagadougou, Burkina Faso, 2016. [Google Scholar]
- Rowhani, P.; Lobell, D.B.; Linderman, M.; Ramankutty, N. Climate variability and crop production in Tanzania. Agric. For. Meteorol. 2011, 151, 449–460. [Google Scholar] [CrossRef]
- Haines, A.; Ebi, K. The Imperative for Climate Action to Protect Health. N. Engl. J. Med. 2019, 380, 263–273. [Google Scholar] [CrossRef]
- Watts, N.; Amann, M.; Arnell, N.; Ayeb-Karlsson, S.; Belesova, K.; Berry, H.; Bouley, T.; Boykoff, M.; Byass, P.; Cai, W. The 2018 report of the Lancet Countdown on health and climate change: Shaping the health of nations for centuries to come. Lancet 2018, 392, 2479–2514. [Google Scholar] [CrossRef]
- Bunker, A. Effects of ambient temperature on non-communicable disease health outcomes in vulnerable populations. Heidelberg University 2018. Available online: https://archiv.ub.uni-heidelberg.de/volltextserver/25388/ (accessed on 10 May 2020).
- Bunker, A.; Wildenhain, J.; Vandenbergh, A.; Henschke, N.; Rocklöv, J.; Hajat, S.; Sauerborn, R. Effects of air temperature on climate-sensitive mortality and morbidity outcomes in the elderly; a systematic review and meta-analysis of epidemiological evidence. EBioMedicine 2016, 6, 258–268. [Google Scholar] [CrossRef] [Green Version]
- Kjellstrom, T.; Briggs, D.; Freyberg, C.; Lemke, B.; Otto, M.; Hyatt, O. Heat, Human Performance, and Occupational Health: A Key Issue for the Assessment of Global Climate Change Impacts. Annu. Rev. Public Health 2016, 37, 97–112. [Google Scholar] [CrossRef] [Green Version]
- Williams, M. Putting a Human Face on Climate Change; Feldscher, K., Ed.; Harvard T.H. Chan School of Public Health: Boston, MA, USA, 2016. [Google Scholar]
- Belesova, K.; Gasparrini, A.; Sié, A.; Sauerborn, R.; Wilkinson, P. Household cereal crop harvest and children’s nutritional status in rural Burkina Faso. Environ. Health 2017, 16, 65. [Google Scholar] [CrossRef] [Green Version]
- Belesova, K.; Gasparrini, A.; Sié, A.; Sauerborn, R.; Wilkinson, P. Annual Crop-Yield Variation, Child Survival, and Nutrition Among Subsistence Farmers in Burkina Faso. Am. J. Epidemiol. 2017, 187, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Nelson, G.C.; Rosegrant, M.W.; Palazzo, A.; Gray, I.; Ingersoll, C.; Robertson, R.; Tokgoz, S.; Zhu, T.; Sulser, T.B.; Ringler Msangi, S.; et al. Food Security, Farming, and Climate Change to 2050: Scenarios, Results, Policy Options; The International Food Policy Research Institute (IFPRI): Washington, DC, USA, 2010. [Google Scholar]
- Niang, I.; Ruppel, O.C.; Abdrabo, M.A.; Essel, A.; Lennard, C.; Padgham, J.; Urquhart, P. Africa. In Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part B: Regional Aspects, Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014; pp. 1199–1265. [Google Scholar]
- De Longueville, F.; Hountondji, Y.-C.; Kindo, I.; Gemenne, F.; Ozer, P. Long-term analysis of rainfall and temperature data in Burkina Faso (1950–2013). Int. J. Climatol. 2016, 36, 4393–4405. [Google Scholar] [CrossRef]
- Karst, I.G.; Mank, I.; Traoré, I.; Sorgho, R.; Stückemann, K.-J.; Simboro, S.; Sié, A.; Franke, J.; Sauerborn, R. Estimating yields of household fields in rural subsistence farming systems to study food security in burkina faso. Remote Sens. 2020, 12, 1717. [Google Scholar] [CrossRef]
- Sorgho, R.; Quiñonez, C.A.M.; Louis, V.R.; Winkler, V.; Dambach, P.; Sauerborn, R.; Horstick, O. Climate Change Policies in 16 West African Countries: A Systematic Review of Adaptation with a Focus on Agriculture, Food Security, and Nutrition. Int. J. Environ. Res. Public Health 2020, 17, 8897. [Google Scholar] [CrossRef] [PubMed]
- Kalame, F.B.; Kudejira, D.; Nkem, J. Assessing the process and options for implementing National Adaptation Programmes of Action (NAPA): A case study from Burkina Faso. Mitig. Adapt. Strateg. Glob. Chang. 2011, 16, 535–553. [Google Scholar] [CrossRef]
- Sherman, M.H.; Ford, J. Stakeholder engagement in adaptation interventions: An evaluation of projects in developing nations. Clim. Policy 2014, 14, 417–441. [Google Scholar] [CrossRef]
- Chin-Yee, S. Defining Climate Policy in Africa: Kenya Climate Change Policy Processes; University of Manchester: Manchester, UK, 2018. [Google Scholar]
- Haas, P.M.; Stevens, C. Organized science, usable knowledge, and multilateral environmental governance. Gov. Air Dyn. Sci. Policy Citiz. Interact. 2011, 125–161. [Google Scholar] [CrossRef]
- Koch, I.C.; Vogel, C.; Patel, Z. Institutional dynamics and climate change adaptation in South Africa. Mitig. Adapt. Strateg. Glob. Chang. 2007, 12, 1323–1339. [Google Scholar] [CrossRef]
- Roberts, D. Thinking globally, acting locally—Institutionalizing climate change at the local government level in Durban, South Africa. Environ. Urban. 2008, 20, 521–537. [Google Scholar] [CrossRef] [Green Version]
- Kondracki, N.L.; Wellman, N.S.; Amundson, D.R. Content analysis: Review of methods and their applications in nutrition education. J. Nutr. Educ. Behav. 2002, 34, 224–230. [Google Scholar] [CrossRef]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- McMahon, S.A.; Winch, P.J. Systematic debriefing after qualitative encounters: An essential analysis step in applied qualitative research. BMJ Glob. Health 2018, 3, e000837. [Google Scholar] [CrossRef]
- Saldaña, J. The Coding Manual for Qualitative Researchers; Sage Publications Ltd.: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Miles, M.B.; Huberman, A.M. Qualitative Data Analysis, 2nd ed.; Sage: Thousand Oaks, CA, USA, 1994. [Google Scholar]
- Polkinghorne, D.E. Validity Issues in Narrative Research. Qual. Inq. 2007, 13, 471–486. [Google Scholar] [CrossRef]
- Booth, A.; Hannes, K.; Harden, A.; Noyes, J.; Harris, J.; Tong, A. COREQ (consolidated criteria for reporting qualitative studies). In Guidelines for Reporting Health Research: A User’s Manual; 2014; pp. 214–226. Available online: http://0-cdn-elsevier-com.brum.beds.ac.uk/promis_misc/ISSM_COREQ_Checklist.pdf (accessed on 1 January 2020).
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Carter, N.; Bryant-Lukosius, D.; DiCenso, A.; Blythe, J.; Neville, A.J. The use of triangulation in qualitative research. Oncol. Nurs. Forum 2014, 41, 545. [Google Scholar] [CrossRef]
- Thurmond, V.A. The point of triangulation. J. Nurs. Scholarsh. 2001, 33, 253–258. [Google Scholar] [CrossRef]
- Shenton, A.K. Strategies for ensuring trustworthiness in qualitative research projects. Educ. Inf. 2004, 22, 63–75. [Google Scholar] [CrossRef] [Green Version]
- Anderson, C. Presenting and Evaluating Qualitative Research. Am. J. Pharm. Educ. 2010, 74, 141. [Google Scholar] [CrossRef] [Green Version]
- Sandelowski, M. Focus on qualitative methods. The use of quotes in qualitative research. Res. Nurs. Health 1994, 17, 479–482. [Google Scholar] [CrossRef]
- USGCRP. The Impacts of Climate Change on Human Health in the United States: A Scientific Assessment. Crimmins; Global Change Research Program: Washington, DC, USA, 2016; p. 312. [Google Scholar]
- FAO. The State of Food Insecurity in the World 2001; Food and Agriculture Organization of the United Nations: Rome, Italy, 2001; pp. 1–8.
- FAO. The Future of Food and Agriculture: Alternative Pathways to 2050; Food and Agriculture Organization of the United Nations: Rome, Italy, 2018; pp. 1–228.
- FAO. Combining Agricultural Biodiversity, Resilient Ecosystems, Traditional Farming Practices and Cultural Identity; Food and Agriculture Organization of the United Nations: Rome, Italy, 2018; pp. 1–48.
- INSD. Annuaire Statistique 2018; Institut National de la Statistique et de la déMographie: Ouagadougou, Burkina Faso, 2019. [Google Scholar]
- Compaoré, N. Burkina Faso: Recruiting women for legislative elections. In Women in Parliament: Beyond Numbers; IDEA: Stockholm, Sweden, 2005; pp. 132–140. [Google Scholar]
- Mitsubishi UFJ Research and Consulting. Country Gender Profile: Burkina Faso; Japan International Cooperation Agency: Tokyo, Japan, 2013; p. 56.
- Florida, U.O. Gender Quotas and Representations: Burkina Faso; University of Florida: Gainesville, FL, USA, 2016. [Google Scholar]
- Dwyer, S.C.; Buckle, J.L. The Space Between: On Being an Insider-Outsider in Qualitative Research. Int. J. Qual. Methods 2009, 8, 54–63. [Google Scholar] [CrossRef]
- van Nes, F.; Abma, T.; Jonsson, H.; Deeg, D. Language differences in qualitative research: Is meaning lost in translation? Eur. J. Ageing 2010, 7, 313–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osaka, S.; Bellamy, R. Natural variability or climate change? Stakeholder and citizen perceptions of extreme event attribution. Glob. Environ. Chang. 2020, 62, 102070. [Google Scholar] [CrossRef]
- Hosking, J.; Campbell-Lendrum, D. How well does climate change and human health research match the demands of policymakers? A scoping review. Environ. Health Perspect. 2012, 120, 1076–1082. [Google Scholar] [CrossRef] [PubMed]
- Fischer, H.; van den Broek, K.L.; Ramisch, K.; Okan, Y. When IPCC graphs can foster or bias understanding: Evidence among decision-makers from governmental and non-governmental institutions. Environ. Res. Lett. 2020, 15, 114041. [Google Scholar] [CrossRef]
- Alam, G.M.M.; Alam, K.; Mushtaq, S. Climate change perceptions and local adaptation strategies of hazard-prone rural households in Bangladesh. Clim. Risk Manag. 2017, 17, 52–63. [Google Scholar] [CrossRef]
- Roy, M.; Cawood, S.; Hordijk, M.; Hulme, D. Urban Poverty and Climate Change: Life in the Slums of Asia, Africa and Latin America; Routledge: London, UK, 2016. [Google Scholar]
- Admassie, A.; Adenew, B.; Tadege, A. Perceptions of Stakeholders on Climate Change and Adaptation Strategies in Ethiopia; International Food Policy Research Institute (IFPRI), Research briefs: Washington, DC, USA, 2008. [Google Scholar]
- Tetteh, E.; Opareh, N.; Ampadu, R.; Antwi, K.B. Impact of climate change: Views and perceptions of policy makers on smallholder agriculture in Ghana. Int. J. Sci. Basic Appl. Res. 2014, 1, 79–89. [Google Scholar]
- Walt, G. Health Policy: An Introduction to Process and Power; Bloomsbury Academics: London, UK, 1994. [Google Scholar]
- Béland, D.; Howlett, M. The Role and Impact of the Multiple-Streams Approach in Comparative Policy Analysis. J. Comp. Policy Anal. Res. Pract. 2016, 18, 221–227. [Google Scholar] [CrossRef] [Green Version]
- WHO. Resolution on Climate Change and Health. Provisional Agenda Item 4, 1st ed.; Board, E., Ed.; World Health Organization: Geneva, Switzerland, 2008; Volume WHA61.19.
- WHO. Climate Change and Human Health: Risk and Responses; World Health Organization: Geneva, Switzerland, 2003.
- Zizka, A.; Thiombiano, A.; Dressler, S.; Nacoulma, B.M.I.; Ouédraogo, A.; Ouédraogo, I.; Ouédraogo, O.; Zizka, G.; Hahn, K.; Schmidt, M. Traditional plant use in Burkina Faso (West Africa): A national-scale analysis with focus on traditional medicine. J. Ethnobiol. Ethnomed. 2015, 11, 9. [Google Scholar] [CrossRef] [Green Version]
- WHO. Connecting Global Priorities: Biodiversity and Human Health; World Helath Organization, Convention on Biological Diversity, United Nations Environment Programme: Geneva, Switzerland, 2015.
- UCSUSA. The Science Connecting Extreme Weather to Climate Change; Union of Concerned Scientists: Cambridge, MA, USA, 2018. [Google Scholar]
- Asare-Kyei, D.; Renaud, F.G.; Kloos, J.; Walz, Y.; Rhyner, J. Development and validation of risk profiles of West African rural communities facing multiple natural hazards. PLoS ONE 2017, 12, e0171921. [Google Scholar] [CrossRef]
- Challinor, A.J.; Adger, W.N.; Benton, T.G.; Conway, D.; Joshi, M.; Frame, D. Transmission of climate risks across sectors and borders. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2018, 376, 20170301. [Google Scholar] [CrossRef] [Green Version]
- Berry, H.; Bowen, K.; Kjellstrom, T. Climate change and mental health: A causal pathways framework. Int. J. Public Health 2010, 55, 123–132. [Google Scholar] [CrossRef]
- Cianconi, P.; Betrò, S.; Janiri, L. The impact of climate change on mental health: A systematic descriptive review. Front. Psychiatry 2020, 11, 1–15. [Google Scholar] [CrossRef]
- Hayes, K.; Blashki, G.; Wiseman, J.; Burke, S.; Reifels, L. Climate change and mental health: Risks, impacts and priority actions. Int. J. Ment. Health Syst. 2018, 12, 28. [Google Scholar] [CrossRef]
- Acharibasam, J.W.; Anuga, S.W. Psychological distance of climate change and mental health risks assessment of smallholder farmers in Northern Ghana: Is habituation a threat to climate change? Clim. Risk Manag. 2018, 21, 16–25. [Google Scholar] [CrossRef]
- FAO; IFAD; UNICEF; WFP; WHO. The State of Food Security and Nutrition in the World 2018: Building Climate Resilience for Food Security and Nutrition; FAO: Rome, Italy, 2018.
- FAO. Food Security and Agricultural Mitigation in Developing Countries: Options for Capturing Synergies; Food and Agriculture Organization of the United Nations: Rome, Italy, 2013.
- Ayodotun, B.; Bamba, S.; Adio, A. Vulnerability Assessment of West African Countries to Climate Change and Variability. J. Geosci. Environ. Prot. 2019, 7, 13–15. [Google Scholar] [CrossRef] [Green Version]
- GH2. Integrating Climate Change and Disaster Risk Reduction into National Developement Policies and Planning in Ghana; The National Development Plan: Accra, Ghana, 2010; pp. 1–28.
- Beg, N.; Morlot, J.C.; Davidson, O.; Afrane-Okesse, Y.; Tyani, L.; Denton, F.; Sokona, Y.; Thomas, J.P.; La Rovere, E.L.; Parikh, J.K. Linkages between climate change and sustainable development. Clim. Policy 2002, 2, 129–144. [Google Scholar] [CrossRef]
- Denton, F. Financing adaptation in Least Developed Countries in West Africa: Is finance the real deal? Clim. Policy 2010, 10, 655–671. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sorgho, R.; Jungmann, M.; Souares, A.; Danquah, I.; Sauerborn, R. Climate Change, Health Risks, and Vulnerabilities in Burkina Faso: A Qualitative Study on the Perceptions of National Policymakers. Int. J. Environ. Res. Public Health 2021, 18, 4972. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094972
Sorgho R, Jungmann M, Souares A, Danquah I, Sauerborn R. Climate Change, Health Risks, and Vulnerabilities in Burkina Faso: A Qualitative Study on the Perceptions of National Policymakers. International Journal of Environmental Research and Public Health. 2021; 18(9):4972. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094972
Chicago/Turabian StyleSorgho, Raissa, Maximilian Jungmann, Aurélia Souares, Ina Danquah, and Rainer Sauerborn. 2021. "Climate Change, Health Risks, and Vulnerabilities in Burkina Faso: A Qualitative Study on the Perceptions of National Policymakers" International Journal of Environmental Research and Public Health 18, no. 9: 4972. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094972