
Association of Organizational Behavior with Work Engagement and Work-Home Conflicts of Physician in China

Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Measures
2.2.1. Exposure Factor
2.2.2. Outcome Variables
2.2.3. Control Variables
2.2.4. Statistical Analysis
2.2.5. Sensitivity Analysis
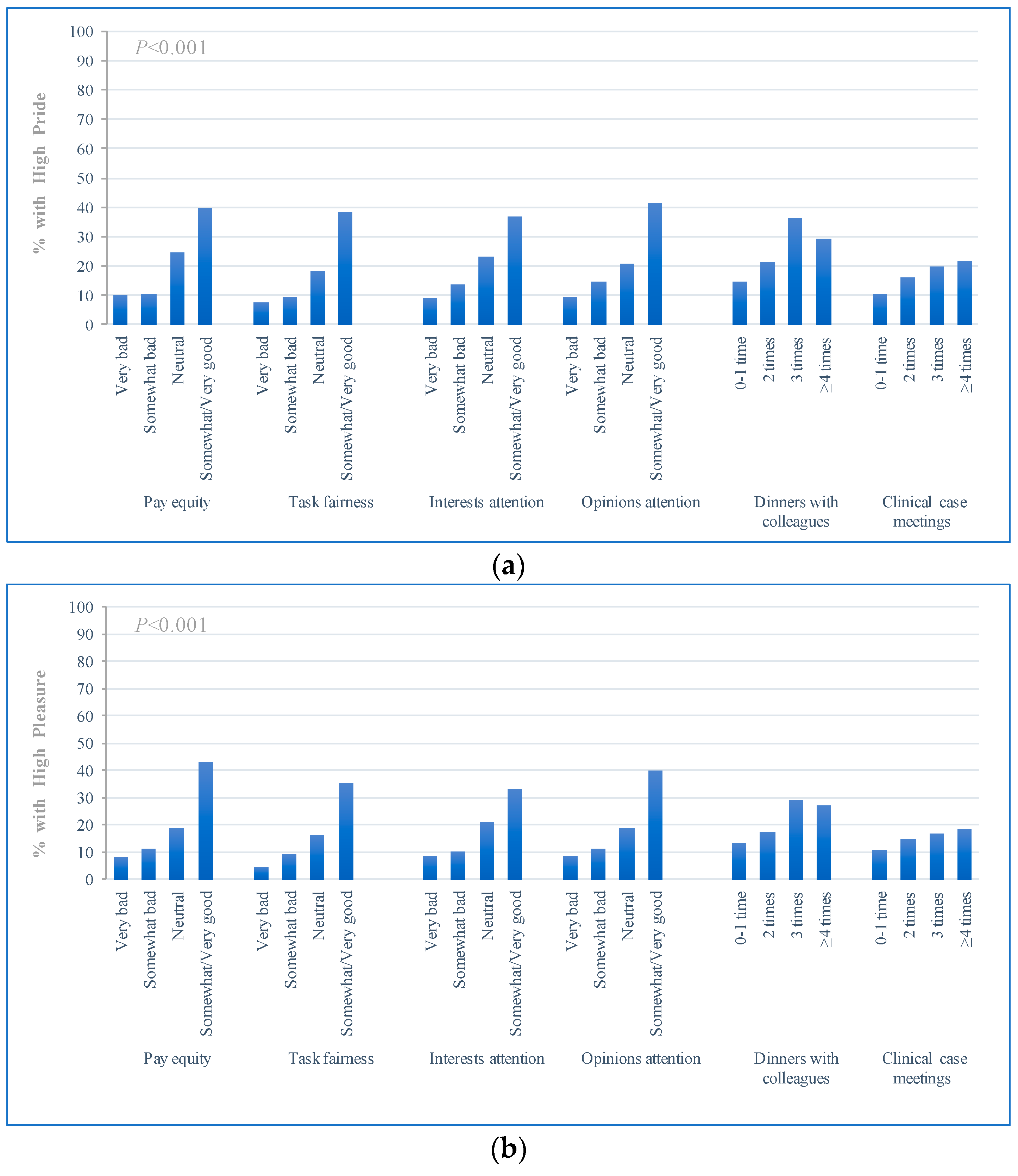
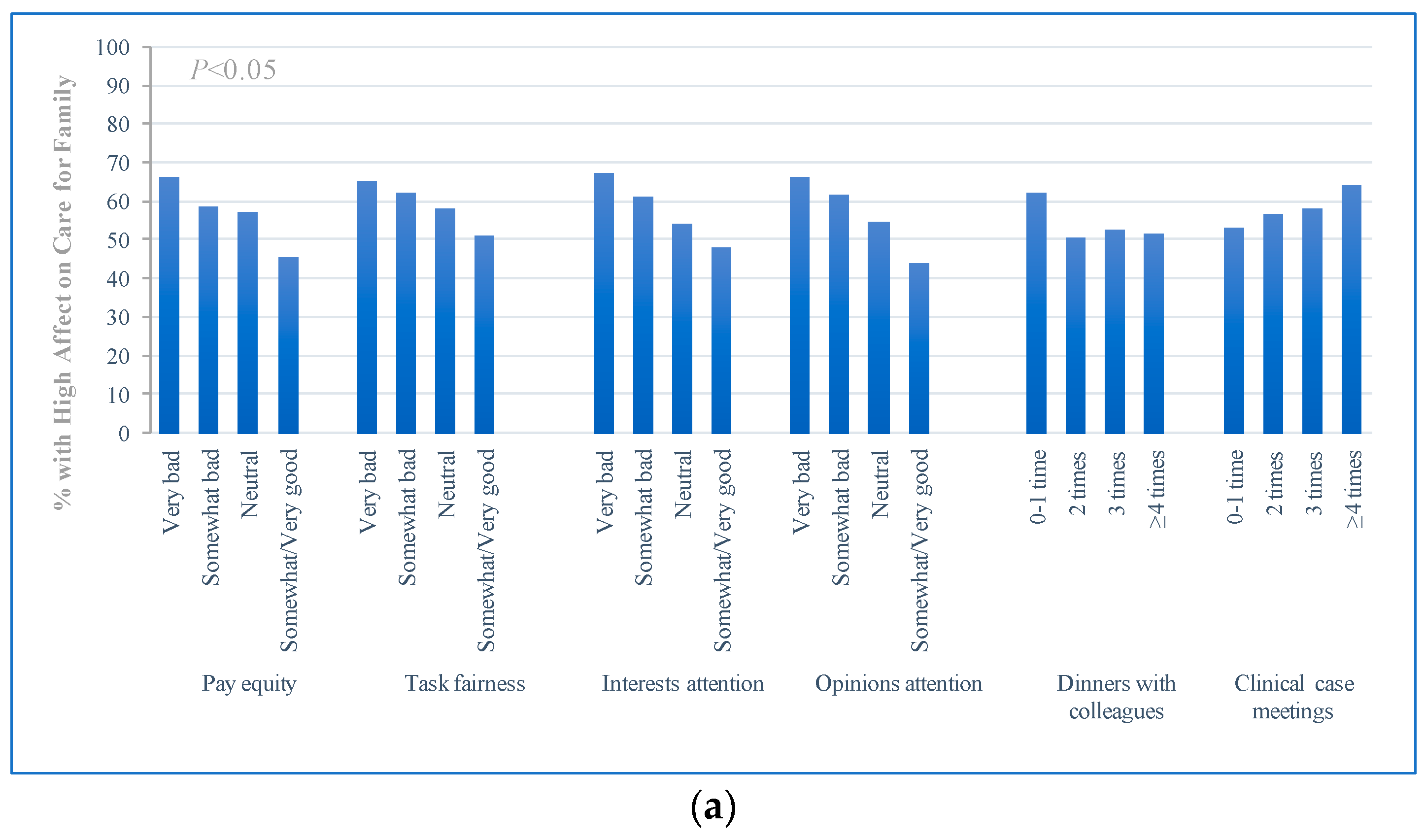
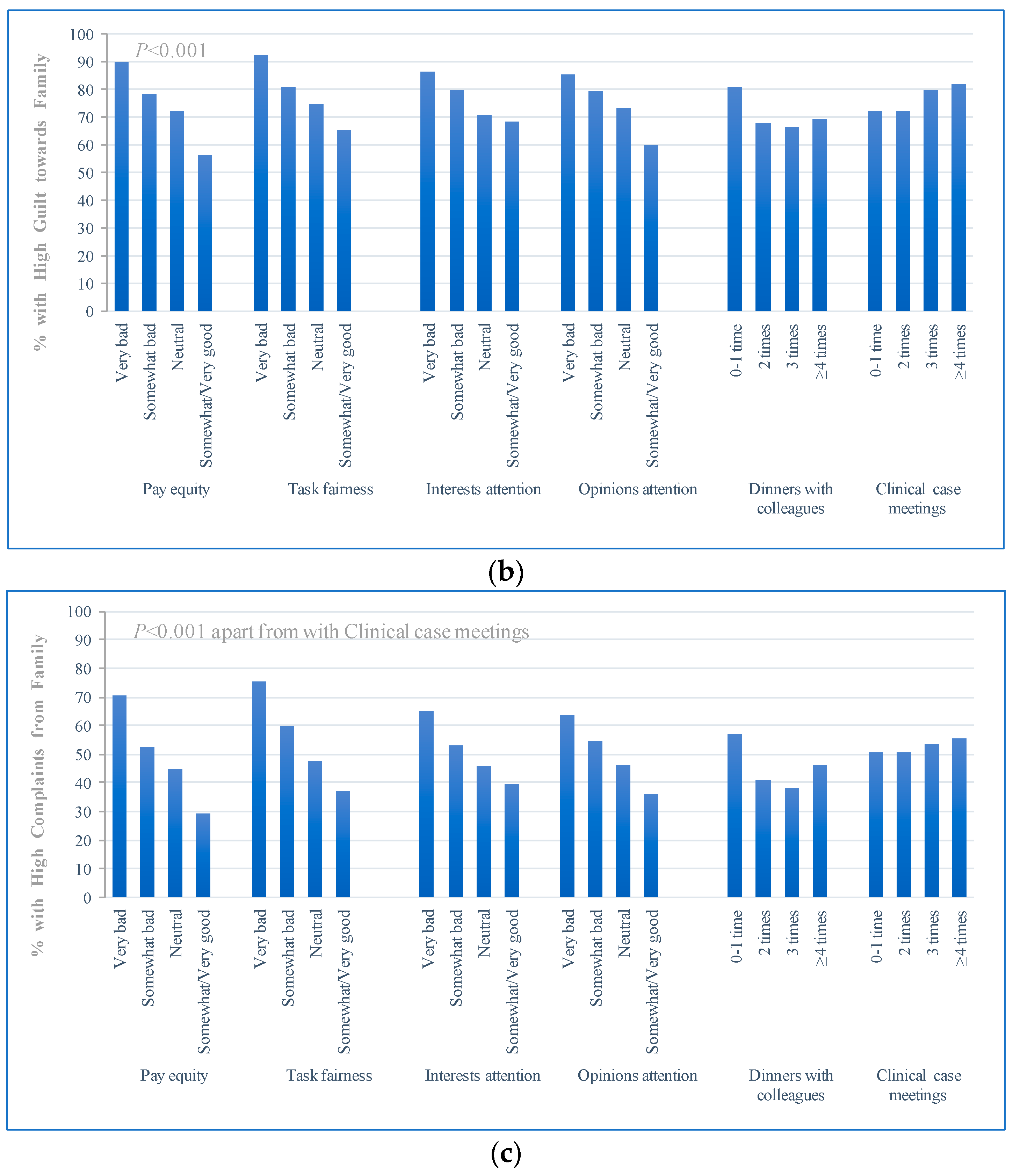
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nahrgang, J.D.; Morgeson, F.P.; Hofmann, D.A. Safety at work: A meta-analytic investigation of the link between job demands, job resources, burnout, engagement, and safety outcomes. J. Appl. Psychol. 2011, 96, 71–94. [Google Scholar] [CrossRef] [PubMed]
- Lassi, Z.S.; Cometto, G.; Huicho, L.; Bhutta, Z.A. Quality of care provided by mid-level health workers: Sys-tematic review and meta-analysis. Bull. World Health Organ. 2013, 91, 824–833. [Google Scholar] [CrossRef]
- Upadyaya, K.; Vartiainen, M.; Salmela-Aro, K. From job demands and resources to work engagement, burnout, life satisfaction, depressive symptoms, and occupational health. J. Burn. 2016, 3, 101–108. [Google Scholar] [CrossRef]
- Shimazu, A.; Schaufeli, W.B.; Kamiyama, K.; Kawakami, N. Workaholism vs. Work Engagement: The Two Different Predictors of Future Well-being and Performance. Int. J. Behav. Med. 2015, 22, 18–23. [Google Scholar] [CrossRef]
- West, C.P.; Shanafelt, T.D.; Kolars, J.C. Quality of life, burnout, educational debt, and medical knowledge among internal medicine residents. JAMA 2011, 306, 952–960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanafelt, T.D.; Boone, S.; Tan, L.; Dyrbye, L.N.; Sotile, W.; Satele, D.; West, C.P.; Sloan, J.; Oreskovich, M.R. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch. Intern. Med. 2012, 18, 1377–1385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanafelt, T.D.; Balch, C.M.; Bechamps, G.J.; Russell, T.; Dyrbye, L.; Satele, D.; Collicott, P.; Novotny, P.J.; Sloan, J.; Freischlag, J.A. Burnout and career satisfaction among American surgeons. Ann. Surg. 2009, 250, 463–471. [Google Scholar] [CrossRef]
- Berger, D. Corruption ruins the doctor-patient relationship in India. BMJ 2014, 348, g3169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thielscher, C.; Schulte-Sutrum, B. Development the Physician-patient Relationship in Germany during the Last Years from the Perspective of the Heads of Chambers and KVs. Gesundheitswesen 2016, 78, 8–13. [Google Scholar]
- Zhang, P.; Wang, F.; Cheng, Y.; Zhang, L.Y.; Ye, B.Z.; Jiang, H.W.; Sun, Y.; Zhu, X.; Liang, Y. Impact of organizational and individual factors on patient-provider relationships: A national survey of doctors, nurses and patients in China. PLoS ONE 2017, 96, 71–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akkas, M.A. Causes and Consequences of Work-Family Conflict (WFC) among the Female Employees in Bangladesh: An Empirical Study. J. Bus. Econ. 2015, 6, 2063–2071. [Google Scholar] [CrossRef]
- Judge, T.A.; Colquitt, J.A. Organizational Justice and Stress: The Mediating Role of Work-Family Conflict. J. Appl. Psychol. 2004, 89, 395–404. [Google Scholar] [CrossRef] [Green Version]
- Sawatzky, J.A.V.; Enns, C.L. Exploring the key predictors of retention in emergency nurses. J. Nurs. Manag. 2012, 20, 696–707. [Google Scholar] [CrossRef]
- DeChant, P.F.; Acs, A.; Rhee, K.B.; Boulanger, T.S.; Snowdon, J.L.; Tutty, M.A.; Sinsky, C.A.; Craig, K.J.T. Effect of Organization-Directed Workplace Interventions on Physician Burnout: A Systematic Review. Mayo Clin. Proc. Innov. Qual. Outcomes 2019, 3, 384–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanafelt, T.D.; Noseworthy, J.H. Executive leadership and physician well-being: Nine organizational strategies to promote engagement and reduce burnout. Mayo Clin. Proc. 2017, 92, 129–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sillero, A.; Zabalegui, A. Organizational Factors and Burnout of Perioperative Nurses. Clin. Pract. Epidemiol. Ment. Health 2018, 14, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Tawfik, D.S.; Profit, J.; Webber, S.; Shanafelt, T.D. Organizational Factors Affecting Physician Well-Being. Curr. Treat. Options Pediatr. 2019, 5, 11–25. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Salanova, M.; González-Romá, V.; Bakker, A.B. The measurement of engagement and burnout: A two sample confirmatory factor analytic approach. J. Happiness Stud. 2002, 3, 71–92. [Google Scholar] [CrossRef]
- Bakker, A.B. An evidence-based model of work engagement. Curr. Dir. Psychol. 2011, 20, 265–269. [Google Scholar] [CrossRef]
- Wu, W.-L.; Lee, Y.-C. How Spiritual Leadership Boosts Nurses’ Work Engagement: The Mediating Roles of Calling and Psychological Capital. Int. J. Environ. Res. Public Health 2020, 17, 6364. [Google Scholar] [CrossRef]
- Chena, I.S.; Fellenz, M.R. Personal resources and personal demands for work engagement: Evidence from employees in the service industry. Int. J. Hosp. Manag. 2020, 90, 102600. [Google Scholar] [CrossRef]
- Gemeda, H.K.; Lee, J. Leadership styles, work engagement and outcomes among information and communications technology professionals: A cross-national study. Heliyon 2020, 6, e03699. [Google Scholar] [CrossRef] [PubMed]
- He, G.; An, R.; Zhang, F. Cultural Intelligence and Work-Family Conflict: A Moderated Mediation Model Based on Conservation of Resources Theory. Int. J. Environ. Res. Public Health 2019, 16, 2406. [Google Scholar] [CrossRef] [Green Version]
- Zhou, M.; Zhang, J.; Li, F.; Chen, C. Work-Family Conflict and Depressive Symptoms Among Chinese Employees: Cross-Level Interaction of Organizational Justice Climate and Family Flexibility. Int. J. Environ. Res. Public Health 2020, 17, 6954. [Google Scholar] [CrossRef]
- The Central People’s Government of the People’s Republic of China. China’s Sixth National Census (2010) Main Data Bulletin No 2. Available online: http://www.gov.cn/gzdt/2011-04/29/content_1854891.htm (accessed on 1 May 2020).
- West, C.P.; Dyrbye, L.N.; Sloan, J.A.; Shanafelt, T.D. Single item measures of emotional exhaustion and depersonalization are useful for assessing burnout in medical professionals. J. Gen. Intern. Med. 2009, 24, 1318–1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colquitt, J.A. On the dimensionality of organizational justice: A construct validation of a measure. J. Appl. Psychol. 2001, 86, 386–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moliner, C.; Martínez-Tur, V.; Peiró, J.M.; Ramos, J.; Cropanzano, R. Perceived Reciprocity and Well-Being at Work in Non-Professional Employees: Fairness or Self-Interest? Stress Health 2012, 29, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Kahn, W.A. To Be Fully There: Psychological Presence at Work. Hum. Relat. 1992, 45, 321–349. [Google Scholar] [CrossRef]
- Nyberg, A.; Peristera, P.; Bernhard-Oettel, C.; Leineweber, C. Does work-personal life interference predict turnover among male and female managers, and do depressive symptoms mediate the association? A longitudinal study based on a Swedish cohort. BMC Public Health 2018, 18, 828. [Google Scholar] [CrossRef]
- Miyasaki, J.M.; Rheaume, C.; Gulya, L.; Ellenstein, A.; Schwarz, H.B.; Vidic, T.R.; Shanafelt, T.D.; Cascino, T.L.; Keran, C.M.; Busis, N.A. Qualitative study of burnout, career satisfaction, and well-being among US neurologists. Neurology 2017, 89, 1730–1738. [Google Scholar] [CrossRef]
- Gupta, V.; Agarwal, U.A.; Khatri, N. The relationships between perceived organizational support, affective commitment, psy-chological contract breach, organizational citizenship behaviour and work engagement. J. Adv. Nurs. 2016, 72, 2806–2817. [Google Scholar] [CrossRef]
- Hakanen, J.J.; Ropponen, A.; Schaufeli, W.B.; De Witte, H. Who is engaged at work? A large-scale study in 30 European countries. J. Occup. Environ. Med. 2019, 61, 373–381. [Google Scholar] [CrossRef]
- Francis, V. The Importance of Workplace Support and Work Flexibility for Civil Engineers; The University of Melbourne: Melbourne, Australia, 2004. [Google Scholar]
- Mache, S.; Vitzthum, K.; Wanke, E.; David, A.; Klapp, B.F.; Danzer, G. Exploring the impact of resilience, self-efficacy, optimism and organizational resources on work engagement. Work 2014, 47, 491–500. [Google Scholar] [PubMed]
- Zheng, J.; Wu, G. Work-family conflict, Perceived organizational support and professional commitment: A mediation mecha-nism for Chinese project professionals. Int. J. Environ. Res. Public Health 2018, 15, 344. [Google Scholar] [CrossRef] [Green Version]
- Tyler, T.R.; De Cremer, D. Process-based leadership: Fair procedures and reactions to organizational change. Leadersh. Q. 2005, 16, 529–545. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.; Xie, Y.H.; Wang, L. Organizational Justice and Employees’ Work Behaviors: Mediating Role of Psychological Safety. J. Peking Univ. 2015, 51, 180–186. [Google Scholar]
- Zhang, X.; Yao, Z. Impact of relational leadership on employees’ unethical pro-organizational behavior: A survey based on tourism companies in four countries. PLoS ONE. 2019, 12, e0225706. [Google Scholar] [CrossRef] [PubMed]
- Ko, W.H.; Kang, H. Effect of leadership style and organizational climate on employees’ food safety and hygiene behaviors in the institutional food service of schools. Food. Sci. Nutr. 2019, 6, 2131–2143. [Google Scholar] [CrossRef] [Green Version]
- Dyrbye, L.N.; Freischlag, J.; Kaups, K.L.; Oreskovich, M.R.; Satele, D.V.; Hanks, J.B.; Sloan, J.A.; Balch, C.M.; Shanafelt, T.D. Work-home conflicts have a substantial impact on career decisions that affect the adequacy of the surgical workforce. Arch. Surg. 2012, 147, 933–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | N(%; 95% CI) |
|---|---|
| Socio–Demographic Characteristics | |
| Sex | |
| Men | 1842(56.58; 54.88–58.28) |
| Women | 1413(43.42; 41.72–45.12) |
| Age, y | |
| ≤34 | 945(29.02; 27.46–30.58) |
| 35–44 | 1127(34.63; 33.00–36.26) |
| ≥45 | 1183(36.35; 34.70–38.00) |
| Marital status | |
| Single/other | 515(16.48; 15.21–17.75) |
| Married | 2609(83.52; 82.25–84.79) |
| Education level | |
| Undergraduate and below | 1679(52.93; 51.22–54.62) |
| Masters | 1130(35.61; 33.96–37.26) |
| PhD | 364(11.47; 10.38–12.56) |
| Economic status | |
| Very bad | 421(12.96; 11.81–14.11) |
| Somewhat bad | 653(20.12; 18.74–21.50) |
| Neutral | 1903(58.63; 56.94–60.32) |
| Good | 269(8.28; 7.33–9.23) |
| Title | |
| Primary/other | 695(24.22; 22.75–25.69) |
| Middle | 907(31.63; 30.03–33.23) |
| High | 1267(44.15; 42.44–45.86) |
| Hospital and Departmental characteristics | |
| Hospital level | |
| Secondary | 490(15.06; 13.83–16.29) |
| Tertiary | 2765(84.94; 83.71–86.17) |
| Hospital type | |
| Traditional Chinese medicine | 904(27.78; 26.24–29.32) |
| Western medicine | 2351(72.22; 70.68–73.76) |
| Academic status | |
| Nonteaching | 2615(80.32; 78.95–81.69) |
| Teaching | 641(19.68; 18.31–21.05) |
| Physician specialty | |
| Internal medicine | 1723(52.94; 51.23–54.65) |
| Surgery | 1532(47.06; 45.35–48.77) |
| The ratio of physicians to beds | |
| <0.20 | 932(28.62; 27.07–30.17) |
| 0.20–0.30 | 1304(40.05; 38.37–41.73) |
| ≥0.30 | 1020(31.34; 29.75–32.93) |
| Family support | |
| Very low/Somewhat low | 115(3.52; 2.89–4.15) |
| Neutral | 574(17.66; 16.35–18.97) |
| Somewhat high/Very high | 2564(78.82; 77.42–80.22) |
| Patient behavior | |
| Patient trust | |
| Very low/Somewhat low | 1375(42.51; 40.81–44.21) |
| Neutral | 1496(46.24; 44.53–47.95) |
| Somewhat high/Very high | 364(11.26; 10.17–12.35) |
| Unreasonable request from the patient | |
| Very low/Somewhat low | 1047(32.22; 30.61–33.83) |
| Neutral | 1102(33.89; 32.26–35.52) |
| Somewhat high/Very high | 1102(33.89; 32.26–35.52) |
| Variable Description | N(%; 95% CI) | Recategorization |
|---|---|---|
| Work engagement | ||
| Pride | ||
| Very low | 594(18.23; 16.90–19.56) | No |
| Somewhat low | 751(23.08; 21.63–24.53) | No |
| Neutral | 1339(41.12; 39.43–42.81) | No |
| Somewhat high | 478(14.69; 13.47–15.91) | Yes |
| Very high | 94(2.88; 2.31–3.45) | Yes |
| Pleasure | ||
| Very low | 712(21.87; 20.45–23.29) | No |
| Somewhat low | 922(28.34; 26.79–29.89) | No |
| Neutral | 1115(34.25; 32.62–35.88) | No |
| Somewhat high | 432(13.27; 12.10–14.44) | Yes |
| Very high | 74(2.27; 1.76–2.78) | Yes |
| Work–home Conflicts | ||
| Affecting care for family | ||
| Very low | 408(12.53; 11.39–13.67) | No |
| Somewhat low | 422(12.96; 11.81–14.11) | No |
| Neutral | 500(15.37; 14.13–16.61) | No |
| Somewhat high | 869(26.69; 25.17–28.21) | Yes |
| Very high | 1056(32.44; 30.83–34.05) | Yes |
| Guilty towards family | ||
| Very low | 49(1.51; 1.09–1.93) | No |
| Somewhat low | 149(4.57; 3.85–5.29) | No |
| Neutral | 532(16.33; 15.06–17.60) | No |
| Somewhat high | 1184(36.37; 34.72–38.02) | Yes |
| Very high | 1342(41.23; 39.54–42.92) | Yes |
| Complaint from family | ||
| Very low | 141(4.32; 3.62–5.02) | No |
| Somewhat low | 440(13.52; 12.35–14.69) | No |
| Neutral | 951(29.21; 27.65–30.77) | No |
| Somewhat high | 976(29.99; 28.42–31.56) | Yes |
| Very high | 747(22.96; 21.52–24.40) | Yes |
| Organizational Behavior | %(95% CI) | Work Engagement | Work–Home Conflicts | |||
|---|---|---|---|---|---|---|
| High Pride (OR, 95% CI) | High Pleasure (OR, 95% CI) | High Effect on Care for Family (OR, 95% CI) | High Guilt towards Family (OR, 95% CI) | High Complaints from Family (OR, 95% CI) | ||
| Organizational fairness | ||||||
| Pay equity | ||||||
| Very bad | 27.88(26.34–39.42) | 1[reference] | 1[reference] | 1[reference] | 1[reference] | 1[reference] |
| Somewhat bad | 27.74(26.20–29.28) | 0.55(0.36–0.83) | 0.84(0.56–1.28) | 0.84(0.65–1.08) | 0.66(0.47–0.94) | 0.72(0.56–0.92) |
| Neutral | 36.50(34.85–38.15) | 1.05(0.70–1.57) | 0.93(0.61–1.42) | 0.96(0.73–1.27) | 0.66(0.45–0.95) | 0.68(0.52–0.89) |
| Somewhat good/Very good | 7.89 (6.96–8.82) | 0.75(0.43–1.33) | 1.32(0.75–2.32) | 0.65(0.43–1.00) | 0.38(0.23–0.63) | 0.38(0.24–0.58) |
| Task fairness | ||||||
| Very bad | 15.11(13.88–16.34) | |||||
| Somewhat bad | 21.51(20.10–22.92) | 1.01(0.60–1.69) | 1.68(0.93–3.04) | 1.01(0.75–1.37) | 0.48(0.30–0.77) | 0.63(0.46–0.87) |
| Neutral | 49.93(48.21–51.65) | 1.27(0.78–2.07) | 2.12(1.20–3.74) | 1.03(0.77–1.39) | 0.48(0.30–0.76) | 0.48(0.35–0.66) |
| Somewhat good/Very good | 13.46(12.29–14.63) | 2.37(1.35–4.18) | 2.64(1.39–5.01) | 0.98(0.67–1.44) | 0.45(0.26–0.77) | 0.52(0.35–0.77) |
| Leadership attention | ||||||
| Interests attention | ||||||
| Very bad | 31.35(29.76–32.94) | |||||
| Somewhat bad | 23.76(22.30–25.22) | 1.01(0.64–1.59) | 0.70(0.43–1.14) | 0.76(0.56–1.01) | 1.03(0.70–1.51) | 0.97(0.72–1.30) |
| Neutral | 35.82(34.17–37.47) | 1.22(0.77–1.92) | 1.09(0.68–1.74) | 0.77(0.57–1.05) | 0.86(0.58–1.27) | 0.87(0.64–1.18) |
| Somewhat good/Very good | 9.07 (8.08–10.06) | 1.96(1.12–3.45) | 1.23(0.69–2.21) | 0.68(0.45–1.03) | 1.18(0.70–1.99) | 0.81(0.53–1.24) |
| Opinions attention | ||||||
| Very bad | 33.30(31.68–34.92) | |||||
| Somewhat bad | 24.18(22.71–25.65) | 1.07(0.70–1.63) | 0.97(0.62–1.52) | 1.18(0.89–1.56) | 1.17(0.81–1.69) | 0.97(0.73–1.28) |
| Neutral | 32.88(31.27–34.49) | 1.11(0.71–1.74) | 1.27(0.80–2.02) | 0.87(0.65–1.18) | 1.03(0.70–1.53) | 1.05(0.78–1.43) |
| Somewhat good/Very good | 9.63(8.62–10.64) | 1.40(0.81–2.43) | 1.86(1.07–3.26) | 0.64(0.42–0.96) | 0.73(0.45–1.20) | 1.09(0.72–1.67) |
| Team interaction | ||||||
| Number of dinners with colleagues | ||||||
| 0–1 time | 74.04(72.53–75.55) | |||||
| 2 times | 13.70(12.52–14.88) | 1.03(0.73–1.44) | 0.80(0.56–1.14) | 0.71(0.56–0.90) | 0.62(0.47–0.82) | 0.65(0.50–0.82) |
| 3 times | 5.16(4.40–5.92) | 1.48(0.93–2.37) | 1.27(0.80–2.02) | 0.68(0.47–0.98) | 0.50(0.33–0.74) | 0.47(0.32–0.69) |
| ≥4 times | 7.10(6.22–7.98) | 1.96(1.30–2.96) | 2.11(1.39–3.19) | 0.71(0.52–0.97) | 0.48(0.33–0.70) | 0.72(0.52–0.99) |
| Number of clinical case meetings | ||||||
| 0–1 time | 23.57(22.11–25.03) | |||||
| 2 times | 19.58(18.22–20.94) | 1.47(1.00–2.18) | 1.30(0.88–1.90) | 1.21(0.95–1.55) | 1.12(0.84–1.50) | 1.15(0.89–1.48) |
| 3 times | 15.82(14.57–17.07) | 1.73(1.16–2.59) | 1.36(0.91–2.04) | 1.35(1.04–1.76) | 1.80(1.30–2.50) | 1.16(0.88–1.52) |
| ≥4 times | 41.03(39.34–42.72) | 1.91(1.36–2.69) | 1.42(1.02–1.99) | 1.74(1.40–2.16) | 1.98(1.51–2.59) | 1.27(1.02–1.58) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, N.; Zhu, Y.; Wang, X.; Jiang, H.; Liang, Y. Association of Organizational Behavior with Work Engagement and Work-Home Conflicts of Physician in China. Int. J. Environ. Res. Public Health 2021, 18, 5405. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105405
Liu N, Zhu Y, Wang X, Jiang H, Liang Y. Association of Organizational Behavior with Work Engagement and Work-Home Conflicts of Physician in China. International Journal of Environmental Research and Public Health. 2021; 18(10):5405. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105405
Chicago/Turabian StyleLiu, Nannan, Yimei Zhu, Xiaoyu Wang, Hongwei Jiang, and Yuan Liang. 2021. "Association of Organizational Behavior with Work Engagement and Work-Home Conflicts of Physician in China" International Journal of Environmental Research and Public Health 18, no. 10: 5405. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105405