
Associations between Self-Esteem, Psychological Stress, and the Risk of Exercise Dependence

Abstract
:1. Introduction
1.1. Exercise Dependence
1.2. Self-Esteem and Self-Worth
1.3. Psychological Distress
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Data Analysis and Processing
3. Results
3.1. Demographics
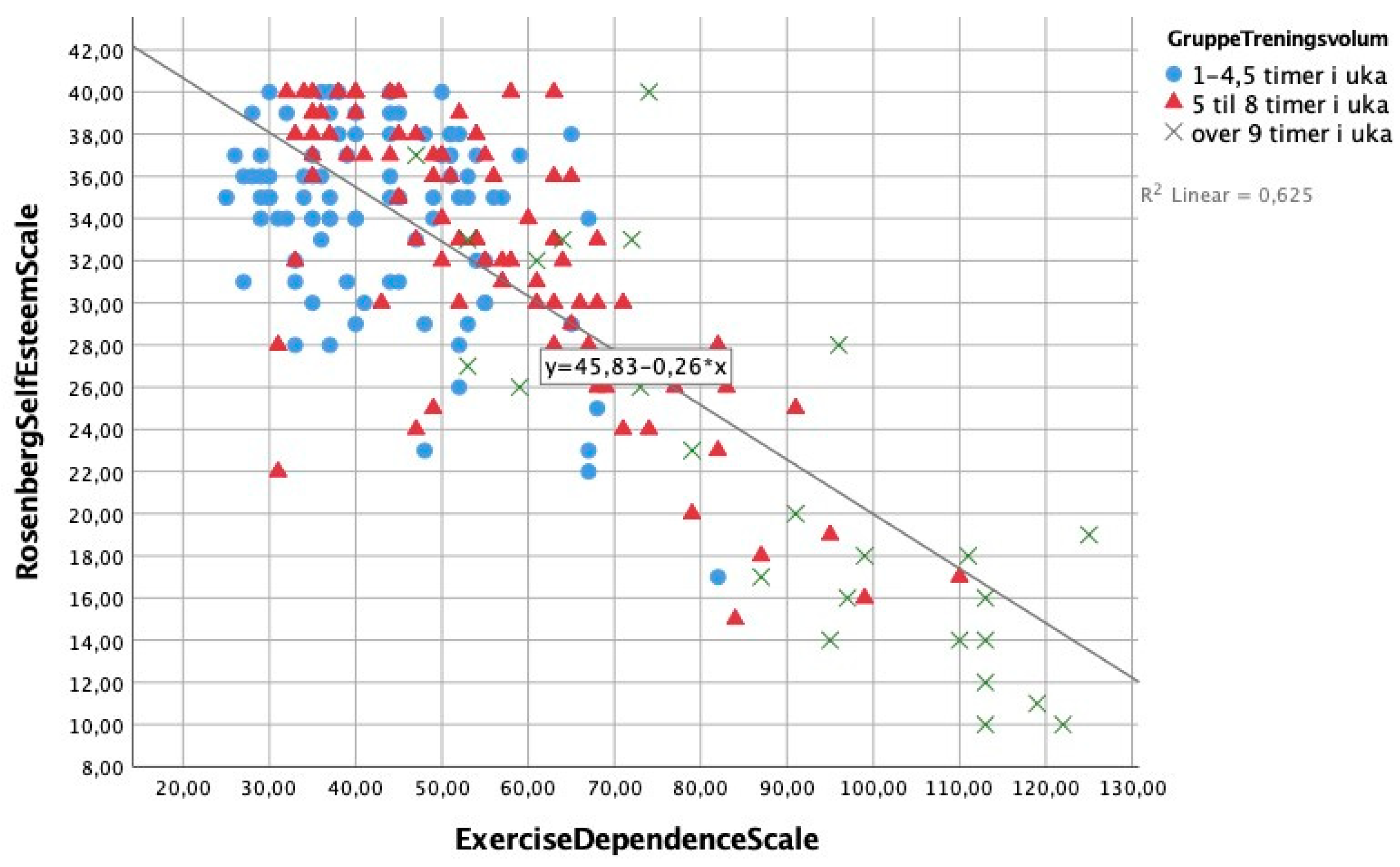
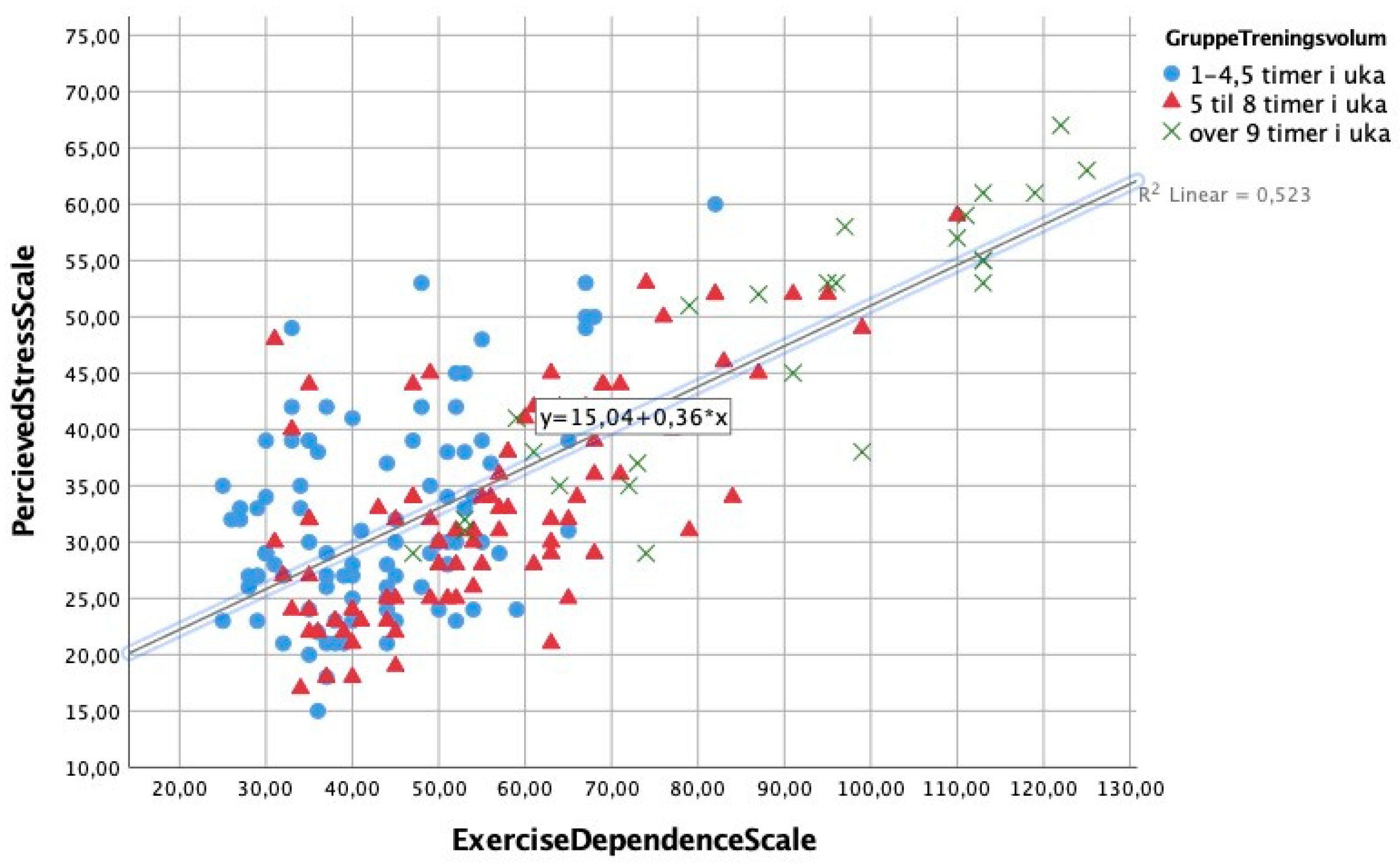
3.2. Relationships between Self-Esteem, Weekly Exercise, Stress, and Exercise Dependence
3.3. Group Differences in Exercise-Dependence Symptoms, Stress, and Self-Esteem
3.4. Age and Gender Differences for Exercise-Dependence Symptoms, Stress, and Self-Esteem
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Egorov, A.Y.; Szabo, A.D. The exercise paradox: An interactional model for a clearer conceptualization of exercise addiction. J. Behav. Addict. 2013, 2, 199–208. [Google Scholar] [CrossRef] [Green Version]
- Silverstone, P.H.; Salsali, M. Low self-esteem and psychiatric patients: Part I—The relationship between low self-esteem and psychiatric diagnosis. Ann. Gen. Psychiatry 2003, 2, 2. [Google Scholar] [CrossRef]
- Lazarus, R.S. Psychological Stress and the Coping Process; McGraw-Hill: New York, NY, USA, 1966. [Google Scholar]
- Freimuth, M.; Moniz, S.; Kim, S.R. Clarifying Exercise Addiction: Differential Diagnosis, Co-occurring Disorders, and Phases of Addiction. Int. J. Environ. Res. Public Health 2011, 8, 4069–4081. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, M.; Schooler, C.; Schoenbach, C.; Rosenberg, F. Global Self-Esteem and Specific Self-Esteem: Different Concepts, Different Outcomes. Am. Sociol. Rev. 1995, 60, 141. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Control; Freeman: New York, NY, USA, 1997. [Google Scholar]
- Taylor, S.E.; Stanton, A.L. Coping Resources, Coping Processes, and Mental Health. Annu. Rev. Clin. Psychol. 2007, 3, 377–401. [Google Scholar] [CrossRef] [Green Version]
- Hagan, A.L.; Hausenblas, H.A. The relationship between exercise dependence symptoms and perfectionism. Am. J. Health Stud. 2003, 18, 133. [Google Scholar]
- Costa, S.; Hausenblas, H.A.; Oliva, P.; Cuzzocrea, F.; Larcan, R. Maladaptive perfectionism as mediator among psychological control, eating disorders, and exercise dependence symptoms in habitual exerciser. J. Behav. Addict. 2016, 5, 77–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bratland-Sanda, S.; Martinsen, E.W.; Rosenvinge, J.H.; Rø, Ø.; Hoffart, A.; Sundgot-Borgen, J. Exercise dependence score in patients with longstanding eating disorders and controls: The importance of affect regulation and physical activity intensity. Eur. Eat. Disord. Rev. 2011, 19, 249–255. [Google Scholar] [CrossRef]
- Bratland-Sanda, S.; Sundgot-Borgen, J.; Rø, Ø.; Rosenvinge, J.H.; Hoffart, A.; Martinsen, E.W. “I’m not physically active—I only go for walks”: Physical activity in patients with longstanding eating disorders. Int. J. Eat. Disord. 2009, 43, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Fullana, M.A.; Hidalgo-Mazzei, D.; Vieta, E.; Radua, J. Coping behaviors associated with decreased anxiety and depressive symptoms during the COVID-19 pandemic and lockdown. J. Affect. Disord. 2020, 275, 80–81. [Google Scholar] [CrossRef] [PubMed]
- Haugland, S.; Wold, B.; Torsheim, T. Relieving the Pressure? The Role of Physical Activity in the Relationship between School-Related Stress and Adolescent Health Complaints. Res. Q. Exerc. Sport 2003, 74, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Moljord, I.E.O.; Eriksen, L.; Moksnes, U.K.; Espnes, G.A. Stress and Happiness among Adolescents with Varying Frequency of Physical Activity. Percept. Mot. Skills 2011, 113, 631–646. [Google Scholar] [CrossRef]
- Gerber, M.; Pühse, U. “Don’t crack under pressure!”—Do leisure time physical activity and self-esteem moderate the relationship between school-based stress and psychosomatic complaints? J. Psychosom. Res. 2008, 65, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Searle, A.; Calnan, M.; Lewis, G.; Campbell, J.; Taylor, A.; Turner, K. Patients’ views of physical activity as treatment for depression: A qualitative study. Br. J. Gen. Pract. 2011, 61, e149–e156. [Google Scholar] [CrossRef] [PubMed]
- Chekroud, S.R.; Gueorguieva, R.; Zheutlin, A.B.; Paulus, M.; Krumholz, H.M.; Krystal, J.H.; Chekroud, A.M. Association between physical exercise and mental health in 1·2 million individuals in the USA between 2011 and 2015: A cross-sectional study. Lancet Psychiatry 2018, 5, 739–746. [Google Scholar] [CrossRef]
- Haugen, T.; Ommundsen, Y.; Seiler, S. The Relationship between Physical Activity and Physical Self-Esteem in Adolescents: The Role of Physical Fitness Indices. Pediatr. Exerc. Sci. 2013, 25, 138–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekeland, E.; Heian, F.; Hagen, K.B.; Abbott, J.M.; Nordheim, L. Exercise to improve self-esteem in children and young people. Cochrane Database Syst. Rev. 2004, 1, CD003683. [Google Scholar] [CrossRef]
- Ekeland, E.; Heian, F.; Hagen, K.B. Can exercise improve self esteem in children and young people? A systematic review of randomised controlled trials * Commentary. Br. J. Sports Med. 2005, 39, 792–798. [Google Scholar] [CrossRef] [Green Version]
- Fox, K.R. Self-esteem, self-perceptions and exercise. Int. J. Sport Psychol. 2000, 31, 228–240. [Google Scholar]
- Gerber, M.; Lindwall, M.; Lindegård, A.; Börjesson, M.; Jonsdottir, I.H. Cardiorespiratory fitness protects against stress-related symptoms of burnout and depression. Patient Educ. Couns. 2013, 93, 146–152. [Google Scholar] [CrossRef]
- Norris, R.; Carroll, U.; Cochrane, R. The effects of aerobic and anaerobic training on fitness, blood pressure, and psychological stress and well-being. J. Psychosom. Res. 1990, 34, 367–375. [Google Scholar] [CrossRef]
- Norris, R.; Carroll, D.; Cochrane, R. The effects of physical activity and exercise training on psychological stress and well-being in an adolescent population. J. Psychosom. Res. 1992, 36, 55–65. [Google Scholar] [CrossRef]
- Rimmele, U.; Zellweger, B.C.; Marti, B.; Seiler, R.; Mohiyeddini, C.; Ehlert, U.; Heinrichs, M. Trained men show lower cortisol, heart rate and psychological responses to psychosocial stress compared with untrained men. Psychoneuroendocrinology 2007, 32, 627–635. [Google Scholar] [CrossRef]
- Steptoe, A.; Edwards, S.; Moses, J.; Mathews, A. The effects of exercise training on mood and perceived coping ability in anxious adults from the general population. J. Psychosom. Res. 1989, 33, 537–547. [Google Scholar] [CrossRef]
- Steptoe, A.; Butler, N. Sports participation and emotional wellbeing in adolescents. Lancet 1996, 347, 1789–1792. [Google Scholar] [CrossRef]
- Pate, R.R.; Pratt, M.; Blair, S.N.; Haskell, W.L.; Macera, C.A.; Bouchard, C.; Buchner, D.; Ettinger, W.; Heath, G.W.; King, A.C.; et al. Physical Activity and Public Health: A recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine. JAMA 1995, 273, 402–407. [Google Scholar] [CrossRef] [PubMed]
- Hamer, M.; Stamatakis, E.; Steptoe, A. Dose-response relationship between physical activity and mental health: The Scottish Health Survey. Br. J. Sports Med. 2009, 43, 1111–1114. [Google Scholar] [CrossRef] [PubMed]
- Cox, R.; Orford, J. A qualitative study of the meaning of exercise for people who could be labelled as ‘addicted’ to exercise –Can ‘addiction’ be applied to high frequency exercising? Addict. Res. Theory 2004, 12, 167–188. [Google Scholar] [CrossRef]
- Menczel, Z.; Griffiths, M.D.; Vingender, I.; Eisinger, A.; Farkas, J.; Magi, A.K.; Mervo, B.F.; Kökönyei, G.; Demetrovics, Z. Exercise Dependence in Amateur Competitors and Non-Competitor Recreational Exercisers. Int. J. Ment. Health Addict. 2017, 15, 580–587. [Google Scholar] [CrossRef]
- Hausenblas, H.A.; Downs, D.S. How much is Too Much? The Development and Validation of the Exercise Dependence Scale. Psychol. Health 2002, 17, 387–404. [Google Scholar] [CrossRef]
- Smith, D.K.; Hale, B.D.; Collins, D. Measurement of exercise dependence in bodybuilders. J. Sports Med. Phys. Fit. 1998, 38, 66–74. [Google Scholar]
- Costa, S.; Hausenblas, H.A.; Oliva, P.; Cuzzocrea, F.; Larcan, R. The role of age, gender, mood states and exercise frequency on exercise dependence. J. Behav. Addict. 2013, 2, 216–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edmunds, J.; Ntoumanis, N.; Duda, J.L. Examining Exercise Dependence Symptomatology from a Self-determination Perspective. J. Health Psychol. 2006, 11, 887–903. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, M.B.; Christiansen, E.; Elklit, A.; Bilenberg, N.; Støving, R.K. Exercise addiction: A study of eating disorder symptoms, quality of life, personality traits and attachment styles. Psychiatry Res. 2014, 215, 410–416. [Google Scholar] [CrossRef]
- Cook, B.; Hausenblas, H.A.; Rossi, J. The moderating effect of gender on ideal-weight goals and exercise dependence symptoms. J. Behav. Addict. 2013, 2, 50–55. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, M.B.; Jensen, T.T. Exercise addiction in CrossFit: Prevalence and psychometric properties of the Exercise Addiction Inventory. Addict. Behav. Rep. 2016, 3, 33–37. [Google Scholar] [CrossRef] [Green Version]
- Lichtenstein, M.B.; Emborg, B.; Hemmingsen, S.D.; Hansen, N.B. Is exercise addiction in fitness centers a socially accepted behavior? Addict. Behav. Rep. 2017, 6, 102–105. [Google Scholar] [CrossRef] [PubMed]
- Mayolas-Pi, C.; Simón-Grima, J.; Peñarrubia-Lozano, C.; Munguía-Izquierdo, D.; Moliner-Urdiales, D.; Legaz-Arrese, A. Exercise addiction risk and health in male and female amateur endurance cyclists. J. Behav. Addict. 2017, 6, 74–83. [Google Scholar] [CrossRef] [Green Version]
- Kleppang, A.L.; Hartz, I.; Thurston, M.; Hagquist, C. The association between physical activity and symptoms of depression in different contexts—A cross-sectional study of Norwegian adolescents. BMC Public Health 2018, 18, 1368. [Google Scholar] [CrossRef]
- Doré, I.; O’Loughlin, J.L.; Beauchamp, G.; Martineau, M.; Fournier, L. Volume and social context of physical activity in association with mental health, anxiety and depression among youth. Prev. Med. 2016, 91, 344–350. [Google Scholar] [CrossRef]
- Meulemans, S.; Pribis, P.; Grajales, T.; Krivak, G. Gender Differences in Exercise Dependence and Eating Disorders in Young Adults: A Path Analysis of a Conceptual Model. Nutrients 2014, 6, 4895–4905. [Google Scholar] [CrossRef]
- Mónok, K.; Berczik, K.; Urbán, R.; Szabo, A.; Griffiths, M.D.; Farkas, J.; Magi, A.; Eisinger, A.; Kurimay, T.; Kökönyei, G.; et al. Psychometric properties and concurrent validity of two exercise addiction measures: A population wide study. Psychol. Sport Exerc. 2012, 13, 739–746. [Google Scholar] [CrossRef]
- Birche, J.; Griffiths, M.D.; Kasos, K.; Demetrovics, Z.; Szabo, A. Exercise addiction and personality: A two-decade systematic review of the empirical literature (1995–2016). Balt. J. Sport Health Sci. 2017, 3, 19–33. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual for Mental Disorders, 4th ed.; American Psychiatric Publishing: Washington, DC, USA, 2000. [Google Scholar]
- Veale, D.C. Exercise Dependence. Br. J. Addict. 1987, 82, 735–740. [Google Scholar] [CrossRef] [Green Version]
- Veale, D.C. Does primary exercise dependence really exist? In Exercise Addiction: Motivation for Participation in Sport and Exercise; British Psychological Society: London, UK, 1995; pp. 71–75. [Google Scholar]
- Allegre, B.; Souville, M.; Therme, P.; Griffiths, M. Definitions and measures of exercise dependence. Addict. Res. Theory 2006, 14, 631–646. [Google Scholar] [CrossRef]
- Bamber, D.; Cockerill, I.M.; Carroll, D. The pathological status of exercise dependence. Br. J. Sports Med. 2000, 34, 125–132. [Google Scholar] [CrossRef] [Green Version]
- Silberstein, L.R.; Striegel-Moore, R.H.; Timko, C.; Rodin, J. Behavioral and psychological implications of body dissatisfaction: Do men and women differ? Sex Roles 1988, 19, 219–232. [Google Scholar] [CrossRef]
- Lichtenstein, M.B.; Hinze, C.J.; Emborg, B.; Thomsen, F.; Hemmingsen, S.D. Compulsive exercise: Links, risks and challenges faced. Psychol. Res. Behav. Manag. 2017, 10, 85–95. [Google Scholar] [CrossRef] [Green Version]
- Brewer, B.W.; Van Raalte, J.L.; Linder, D.E. Athletic identity: Hercules’ muscles or Achilles heel? Int. J. Sport Psychol. 1993, 24, 237–254. [Google Scholar]
- Murray, A.L.; McKenzie, K.; Newman, E.; Brown, E. Exercise identity as a risk factor for exercise dependence. Br. J. Health Psychol. 2012, 18, 369–382. [Google Scholar] [CrossRef]
- Groves, M.; Biscomb, K.; Nevill, A.; Matheson, H. Exercise dependence, self-esteem and identity reinforcement: A comparison of three universities in the United Kingdom. Sport Soc. 2008, 11, 59–73. [Google Scholar] [CrossRef]
- Avison, W.R.; Rosenberg, M. Conceiving the Self. Can. J. Sociol. 1981, 6, 212–214. [Google Scholar] [CrossRef]
- Shavelson, R.J.; Hubner, J.J.; Stanton, G.C. Self-Concept: Validation of Construct Interpretations. Rev. Educ. Res. 1976, 46, 407–441. [Google Scholar] [CrossRef]
- Covington, M.V. Making the Grade: A Self-Worth Perspective on Motivation and School Reform; Cambridge University Press: Cambridge, UK, 1992. [Google Scholar]
- Szabo, A. The impact of exercise deprivation on well-being of habitual exercises. Aust. J. Sci. Med. Sport 1995, 27, 68–77. [Google Scholar]
- Moksnes, U.K.; Moljord, I.E.; Espnes, G.A.; Byrne, D.G. The association between stress and emotional states in adolescents: The role of gender and self-esteem. Personal. Individ. Differ. 2010, 49, 430–435. [Google Scholar] [CrossRef]
- Moksnes, U.K.; Moljord, I.E.; Espnes, G.A.; Byrne, D.G. Leisure time physical activity does not moderate the relationship between stress and psychological functioning in Norwegian adolescents. Ment. Health Phys. Act. 2010, 3, 17–22. [Google Scholar] [CrossRef]
- Salmon, P. Effects of physical exercise on anxiety, depression, and sensitivity to stress. Clin. Psychol. Rev. 2001, 21, 33–61. [Google Scholar] [CrossRef]
- Østerås, B.; Sigmundsson, H.; Haga, M. Physical Fitness Levels Do Not Affect Stress Levels in a Sample of Norwegian Adolescents. Front. Psychol. 2017, 8, 2176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindwall, M.; Lindgren, E.-C. The effects of a 6-month exercise intervention programme on physical self-perceptions and social physique anxiety in non-physically active adolescent Swedish girls. Psychol. Sport Exerc. 2005, 6, 643–658. [Google Scholar] [CrossRef]
- Guidi, J.; Clementi, C.; Grandi, S. Psychological distress and personality characteristics among individuals with primary exercise dependence. Riv. Psichiatr. 2013, 48, 121–129. [Google Scholar]
- Downs, D.S.; Savage, J.S.; DiNallo, J.M. Self-Determined to Exercise? Leisure-Time Exercise Behavior, Exercise Motivation, and Exercise Dependence in Youth. J. Phys. Act. Health 2013, 10, 176–184. [Google Scholar] [CrossRef]
- Downs, D.S.; Hausenblas, H.A.; Nigg, C.R. Factorial Validity and Psychometric Examination of the Exercise Dependence Scale-Revised. Meas. Phys. Educ. Exerc. Sci. 2004, 8, 183–201. [Google Scholar] [CrossRef]
- Hausenblas, H.A.; Fallon, E.A. Relationship among body image, exercise behavior, and exercise dependence symptoms. Int. J. Eat. Disord. 2002, 32, 179–185. [Google Scholar] [CrossRef]
- Kovacsik, R.; Griffiths, M.D.; Pontes, H.M.; Soós, I.; De La Vega, R.; Ruíz-Barquín, R.; Demetrovics, Z.; Szabó, A. The Role of Passion in Exercise Addiction, Exercise Volume, and Exercise Intensity in Long-term Exercisers. Int. J. Ment. Health Addict. 2018, 17, 1389–1400. [Google Scholar] [CrossRef] [Green Version]
- Terry, A.; Szabo, A.; Griffiths, M. The exercise addiction inventory: A new brief scanning tool. Addict. Res. Theory 2004, 12, 489–499. [Google Scholar] [CrossRef]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Moksnes, U.K.; Espnes, G.A. Self-esteem and life satisfaction in adolescents—Gender and age as potential moderators. Qual. Life Res. 2013, 22, 2921–2928. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, M.G.; Ørnbøl, E.; Vestergaard, M.; Bech, P.; Larsen, F.B.; Lasgaard, M.; Christensen, K.S. The construct validity of the Perceived Stress Scale. J. Psychosom. Res. 2016, 84, 22–30. [Google Scholar] [CrossRef]
- Godin, G. The Godin-Shephard leisure-time physical activity questionnaire. Health Fit. J. Can. 2011, 4, 18–22. [Google Scholar] [CrossRef]
- Kjelsås, E.; Augestad, L.B.; Götestam, K.G. Exercise Dependence in Physically Active Women. Eur. J. Psychiatry 2003, 17, 145–155. [Google Scholar]
- Griffiths, M. Exercise Addiction: A Case Study. Addict. Res. 1997, 5, 161–168. [Google Scholar] [CrossRef]
- Webster, J.; Tiggemann, M. The Relationship between Women’s Body Satisfaction and Self-Image across the Life Span: The Role of Cognitive Control. J. Genet. Psychol. 2003, 164, 241–252. [Google Scholar] [CrossRef] [PubMed]
- Tiggemann, M.; Lynch, J.E. Body image across the life span in adult women: The role of self-objectification. Dev. Psychol. 2001, 37, 243–253. [Google Scholar] [CrossRef] [PubMed]
- Tiggemann, M.; Williamson, S. The Effect of Exercise on Body Satisfaction and Self-Esteem as a Function of Gender and Age. Sex Roles 2000, 43, 119–127. [Google Scholar] [CrossRef]
- Striegel-Moore, R.H.; Bulik, C.M. Risk factors for eating disorders. Am. Psychol. 2007, 62, 181–198. [Google Scholar] [CrossRef] [PubMed]
- Furnham, A.; Badmin, N.; Sneade, I. Body Image Dissatisfaction: Gender Differences in Eating Attitudes, Self-Esteem, and Reasons for Exercise. J. Psychol. 2002, 136, 581–596. [Google Scholar] [CrossRef] [PubMed]
- Arem, H.; Moore, S.C.; Patel, A.; Hartge, P.; De Gonzalez, A.B.; Visvanathan, K.; Linet, M.S. Leisure time physical activity and mortality: A detailed pooled analysis of the dose-response relationship. JAMA Intern. Med. 2015, 175, 959–967. [Google Scholar] [CrossRef]
- Kim, Y.S.; Park, Y.S.; Allegrante, J.; Marks, R.; Ok, H.; Cho, K.O.; Garber, C.E. Relationship between physical activity and general mental health. Prev. Med. 2012, 55, 458–463. [Google Scholar] [CrossRef]
- Lindwall, M.; Palmeira, A. Factorial Validity and Invariance Testing of the Exercise Dependence Scale-Revised in Swedish and Portuguese Exercisers. Meas. Phys. Educ. Exerc. Sci. 2009, 13, 166–179. [Google Scholar] [CrossRef]
- Blaydon, M.J.; Lindner, K.J.; Kerr, J.H. Metamotivational characteristics of eating-disordered and exercise-dependent triathletes: An application of reversal theory. Psychol. Sport Exerc. 2002, 3, 223–236. [Google Scholar] [CrossRef]
- Szabo, A.; Griffiths, M.D.; Marcos, R.D.L.V.; Mervó, B.; Demetrovics, Z. Focus: Addiction: Methodological and conceptual limitations in exercise addiction research. Yale J. Biol. Med. 2015, 88, 303. [Google Scholar]
- Cheng, C.-Y. Acculturation and Cultural Value Orientations of Immigrant Chinese Americans: Effects on Body Image, Aesthetics for Appearance, and Involvement in Dress. Ph.D. Thesis, Iowa State University, Ames, IA, USA, 2018. [Google Scholar]
- Dotse, J.E.; Asumeng, M. Relationship between Body Image Satisfaction and Psychological Well-Being: The Impact of Africentric Values. J. Soc. Sci. Stud. 2014, 2, 320. [Google Scholar] [CrossRef] [Green Version]
- Portney, L.G.; Gross, L.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice; EE. UU: Davis Company: Boston, MA, USA, 2015. [Google Scholar]
- Smith-Jackson, T.; Reel, J.J.; Thackeray, R. Coping with “Bad Body Image Days”: Strategies from first-year young adult college women. Body Image 2011, 8, 335–342. [Google Scholar] [CrossRef]
- Sibley, B.A.; Hancock, L.; Bergman, S.M. University Students’ Exercise Behavioral Regulation, Motives, and Physical Fitness. Percept. Mot. Skills 2013, 116, 322–339. [Google Scholar] [CrossRef] [PubMed]
- De La Vega, R.; Parastatidou, I.S.; Ruíz-Barquín, R.; Szabo, A.D. Exercise Addiction in Athletes and Leisure Exercisers: The Moderating Role of Passion. J. Behav. Addict. 2016, 5, 325–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hausenblas, H.A.; Downs, D.S. Exercise Dependence Scale-21 Manual. 2002. Available online: http://www.personal.psu.edu/dsd11/EDS/EDS21Manual.pdf (accessed on 20 April 2021).



{kind=link}
{kind=link}
| Variable | Total (n = 203) | Men | Women | Range | Z |
|---|---|---|---|---|---|
| Exercise (Hours/Week) | 5.47 (SD = 3.0) | 5.9 (SD = 2.9) | 5.1 (SD = 3.0) | 1–21 | −2.59 ** |
| Self-Esteem (RSES) | 31.8 (SD = 7.1) | 32.7 (SD = 7.25) | 31.1 (SD = 6.9) | 10–40 | −1.53 |
| Stress (PSS) | 34.5 (SD = 10.8) | 32.1 (SD = 9.8) | 36.5 (SD = 11.2) | 14–70 | −2.85 ** |
| Exercise Dependence (EDS) | 54.4 (SD = 21.8) | 54.5 (SD = 20.9) | 54.0 (SD = 22.4) | 21–126 | −0.33 |
| Self-Esteem (RSES) | Exercise Dependence (EDS) | Weekly Training Hours | Stress (PSS) | |
|---|---|---|---|---|
| (RSES) | 1 | |||
| (EDS) | −0.597 ** | 1 | ||
| Weekly Training Hours | −0.338 ** | 0.566 ** | 1 | |
| (PSS) | −0.781 ** | 0.567 ** | 0.298 ** | 1 |
| 1–4.5 h/Week (n = 93) | 5–8.5 h/Week (n = 85) | >9 h/Week (n = 25) | |
|---|---|---|---|
| RSES (Mean Score, SD) | 34.2 (SD = 4.4) | 32.2 (SD = 6.4) | 21.9 (SD = 9.0) |
| EDS (Mean Score, SD) | 42.9 (SD = 11.7) | 56.4 (SD = 17.2) | 89.6 (SD = 24.4) |
| PSS (Mean Score, SD) | 31.9 (SD = 8.9) | 33.6 (SD = 9.7) | 47.5 (SD = 11.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wågan, F.A.; Darvik, M.D.; Pedersen, A.V. Associations between Self-Esteem, Psychological Stress, and the Risk of Exercise Dependence. Int. J. Environ. Res. Public Health 2021, 18, 5577. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115577
Wågan FA, Darvik MD, Pedersen AV. Associations between Self-Esteem, Psychological Stress, and the Risk of Exercise Dependence. International Journal of Environmental Research and Public Health. 2021; 18(11):5577. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115577
Chicago/Turabian StyleWågan, Frida Austmo, Monica Dahle Darvik, and Arve Vorland Pedersen. 2021. "Associations between Self-Esteem, Psychological Stress, and the Risk of Exercise Dependence" International Journal of Environmental Research and Public Health 18, no. 11: 5577. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115577