
The Use of GIS Technology to Optimize COVID-19 Vaccine Distribution: A Case Study of the City of Warsaw, Poland


Abstract
:1. Introduction
- Phase 0: employees of the health care sector, employees of Residential Care Homes and Municipal Social Services Centres as well as auxiliary and administrative staff in health care facilities, including sanitary and epidemiological stations.
- Phase I: residents of Residential Care Homes, Nursing Homes and other residential care facilities, people over 60 years of age in order of age, uniformed services, teachers.
- Phase II: people under the age of 60 with chronic diseases that increase the risk of severe COVID-19, or during diagnostic testing and treatment, requiring repeated or continuous contact with health care facilities, people directly ensuring the functioning of the basic state operations and at risk of infection due to frequent social contacts.
- Phase III: entrepreneurs and employees of sectors closed under the regulations on establishing specific restrictions, orders and bans in connection with the outbreak of an epidemic, general vaccination of the rest of the adult population.
2. Materials and Methods
2.1. Materials
- number of people registered in the building,
- number of apartments in which at least one person is registered,
- number of people broken down by gender and five-year age groups, e.g., the number of women aged 50–55 registered in the building, the number of men aged 50–55 registered in the building, the number of women aged 55–60 registered in the building etc.
- name of the site/facility where vaccination is carried out,
- number of the entry in the Register of Entities Performing Medical Activities,
- information on whether primary healthcare services are provided at a given site,
- contact details of the vaccination site,
- geographic coordinates.
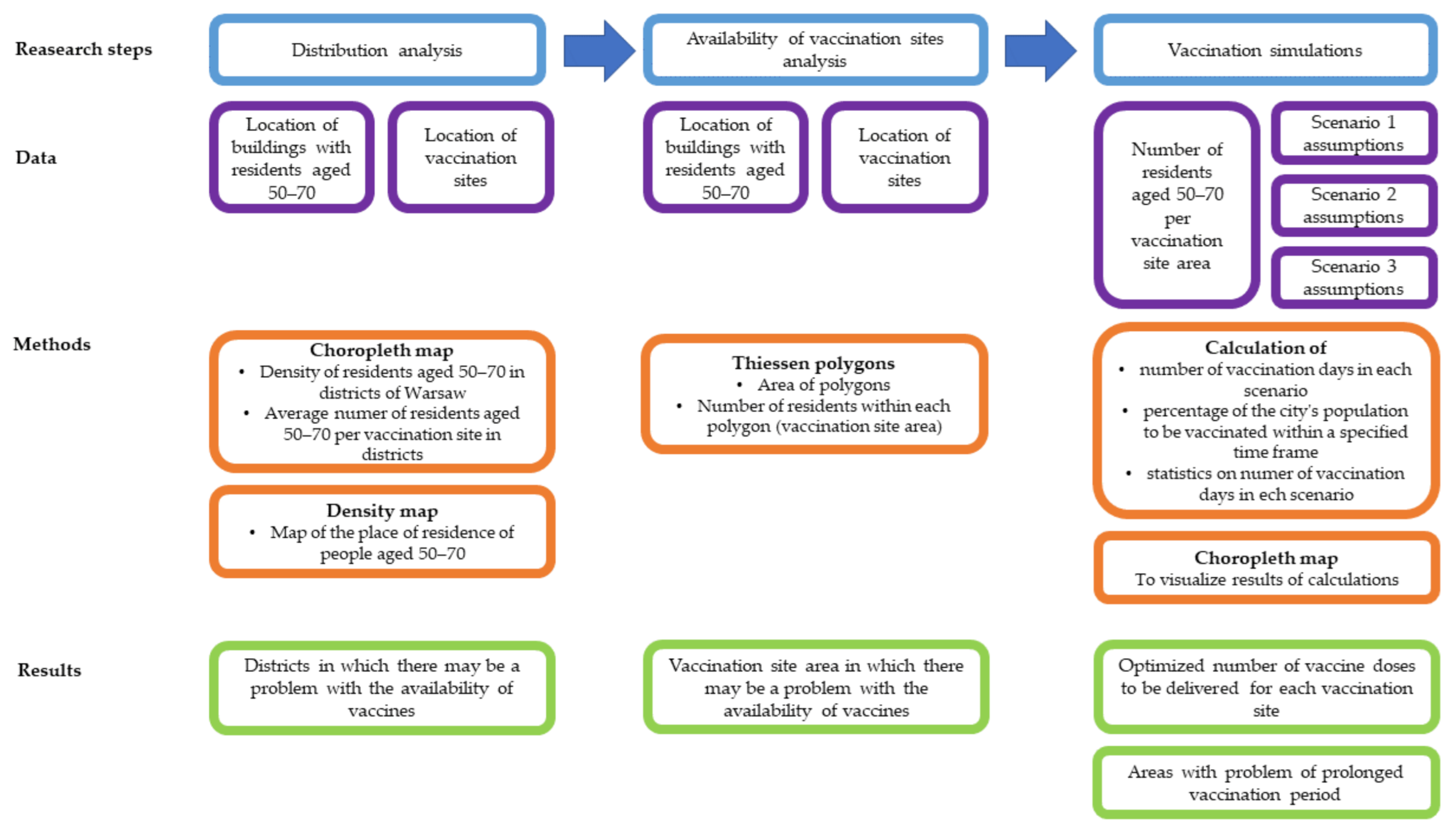
2.2. Methods
- (1)
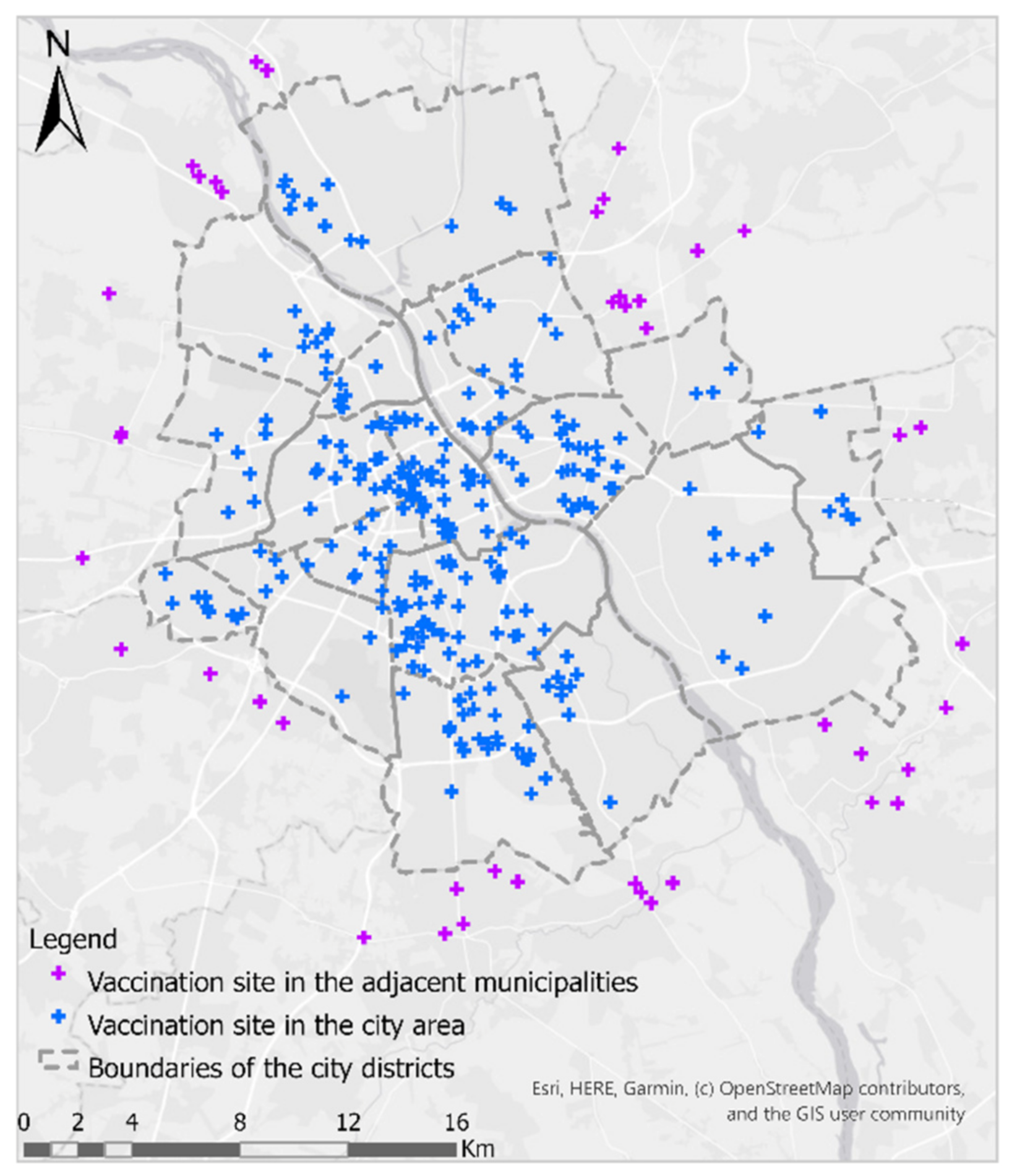
- analysis of the distribution of buildings inhabited by people over the age of 50 and COVID-19 vaccination sites in the area of Warsaw,
- (2)
- analysis of the availability of currently operating vaccination sites (as of 1 April 2021) located in Warsaw,
- (3)
- vaccination simulations according to various scenarios—determining the number of days needed to vaccinate different age groups.
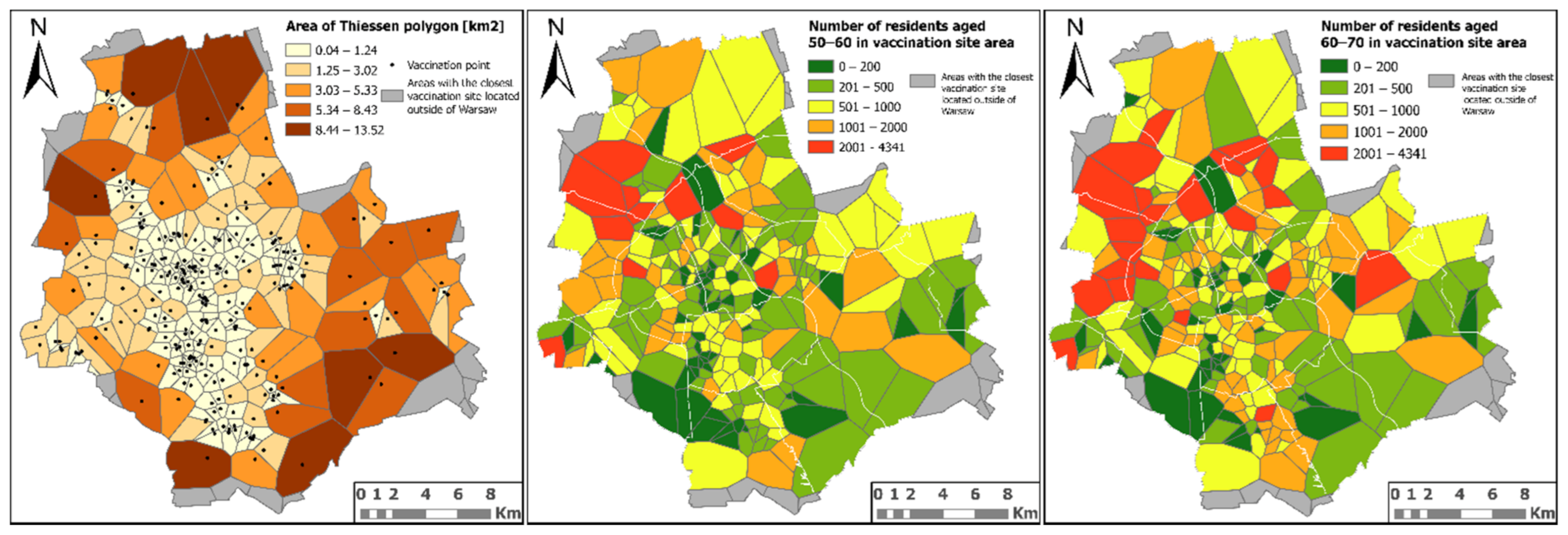
2.2.1. Analysis of the Distribution of Buildings Inhabited by People over the Age of 50 and Vaccination Sites in the Area of Warsaw
2.2.2. Analysis of the Availability of Vaccination Sites Located in Warsaw
- (1)
- triangulation of input points (nodes) and creation of a TIN (triangulated irregular network) that meets the Delaunay criterion,
- (2)
- polygons creation by joining the intersections of bisectors of each side of the triangle belonging to the TIN.
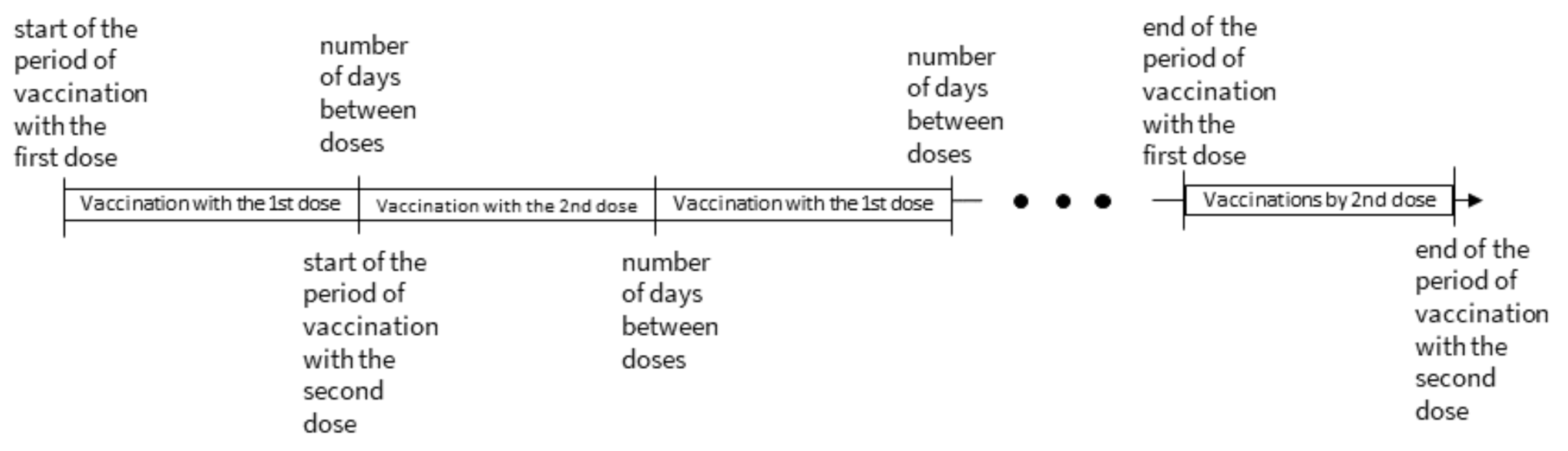
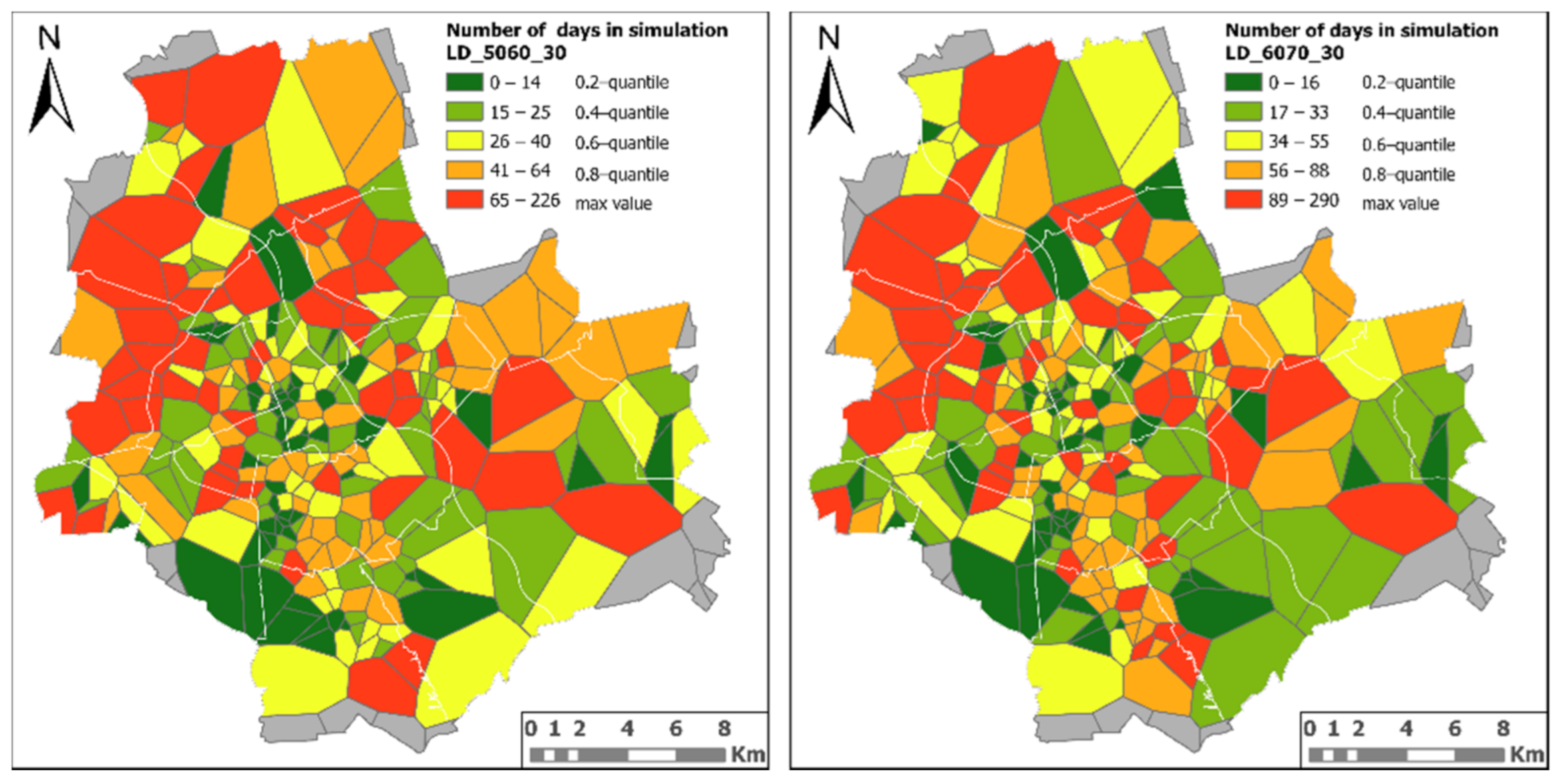
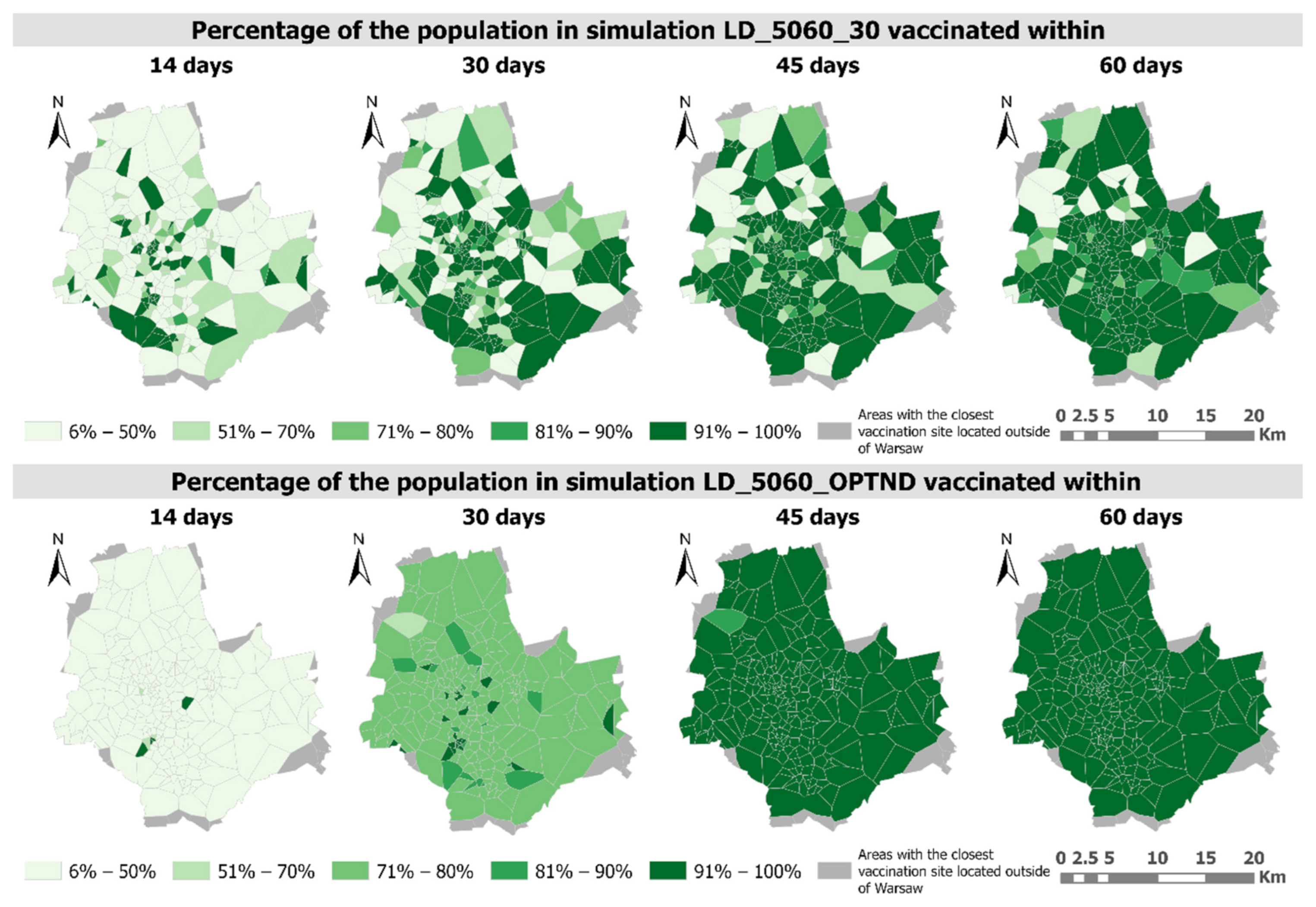
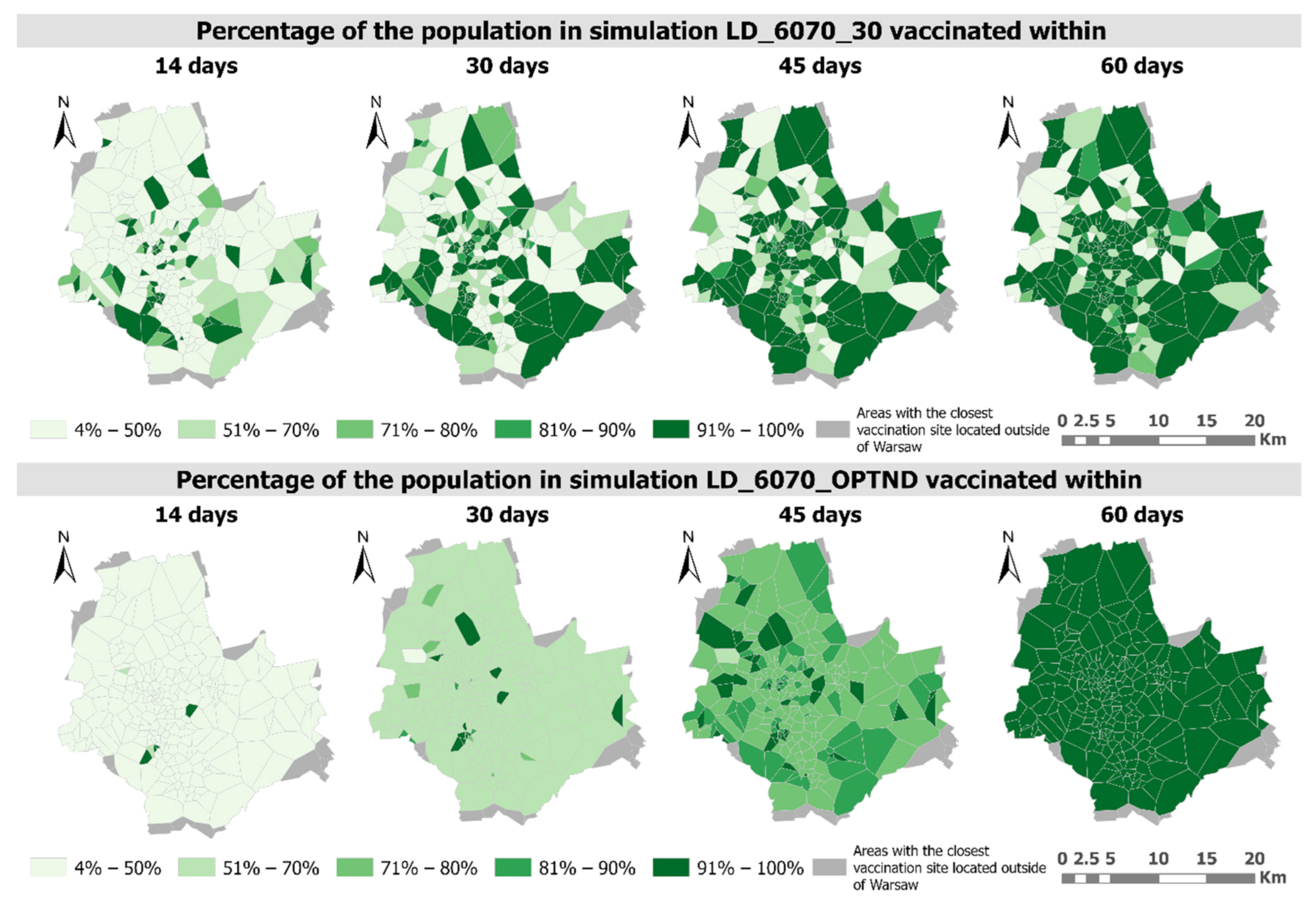
2.2.3. Simulations of the Number of Days Needed to Vaccinate Each Studied Age Group
- (1)
- calculating the median number of days needed to vaccinate the number of people assigned to a given vaccination site, assuming an even distribution of the vaccines (MD),
- (2)
- calculating the number of doses according to the following Equations (3) and (4):where pop—number of people to be vaccinated at a given vaccination site and maxd—the maximum daily number of vaccines that can be distributed at one vaccination site.
- (3)
- scaling the number of doses determined in step 2 with a factor (c):where i = 1,…, n—number of vaccination sites, du—the daily number of doses, assuming an even distribution of vaccines between vaccination sites and d—optimized daily number of vaccine doses to be assigned and delivered to a given vaccination site.
3. Results
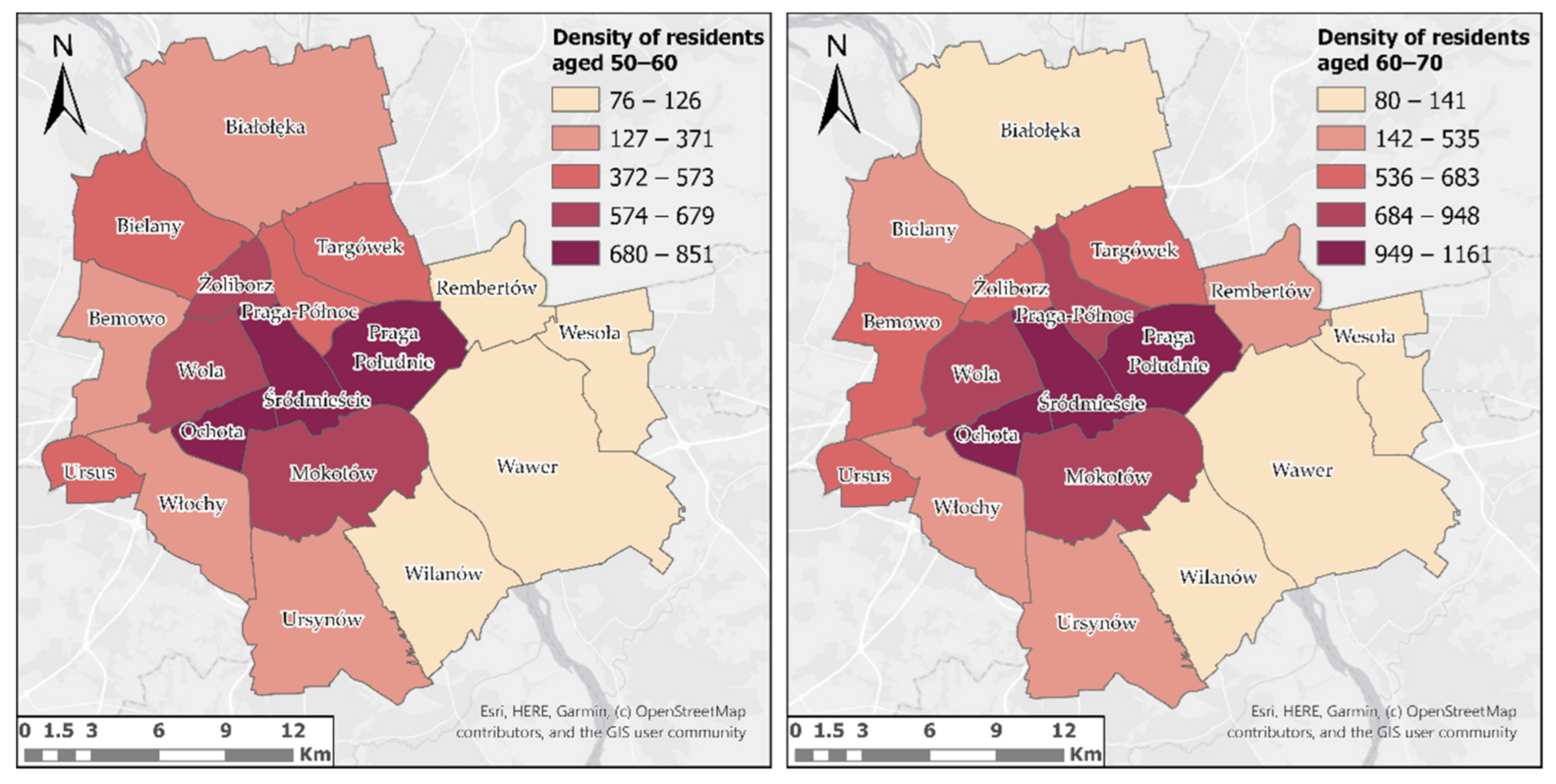
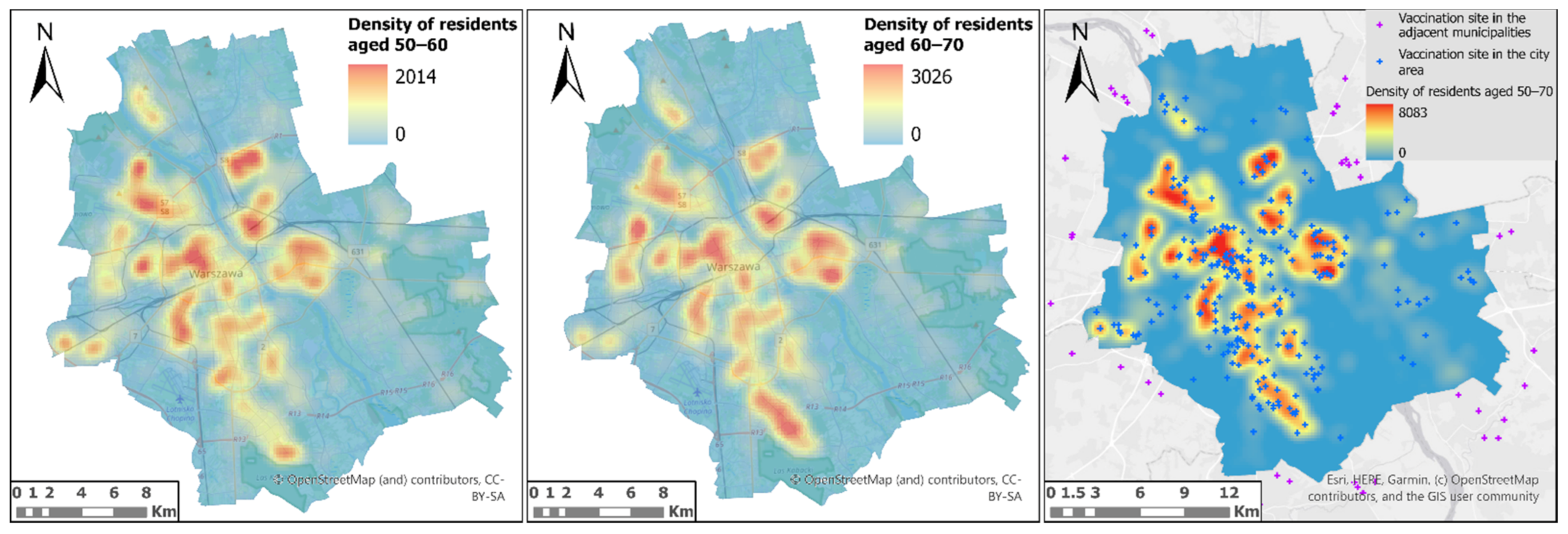
3.1. Analysis of the Distribution of Buildings Inhabited by People over the Age of 50 and Vaccination Sites in the Area of Warsaw
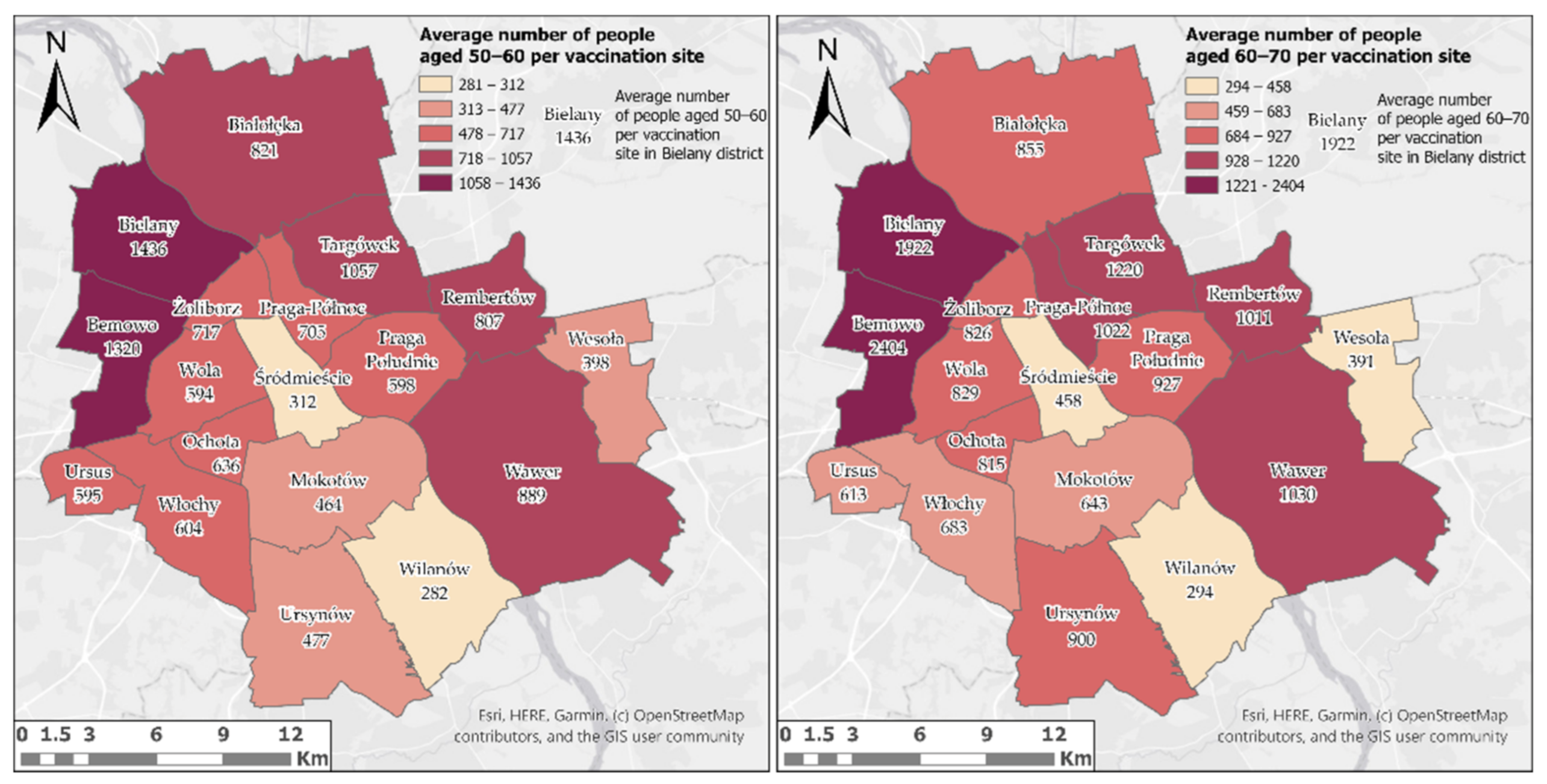
3.2. Analysis of the Availability of Vaccination Sites Located in Warsaw
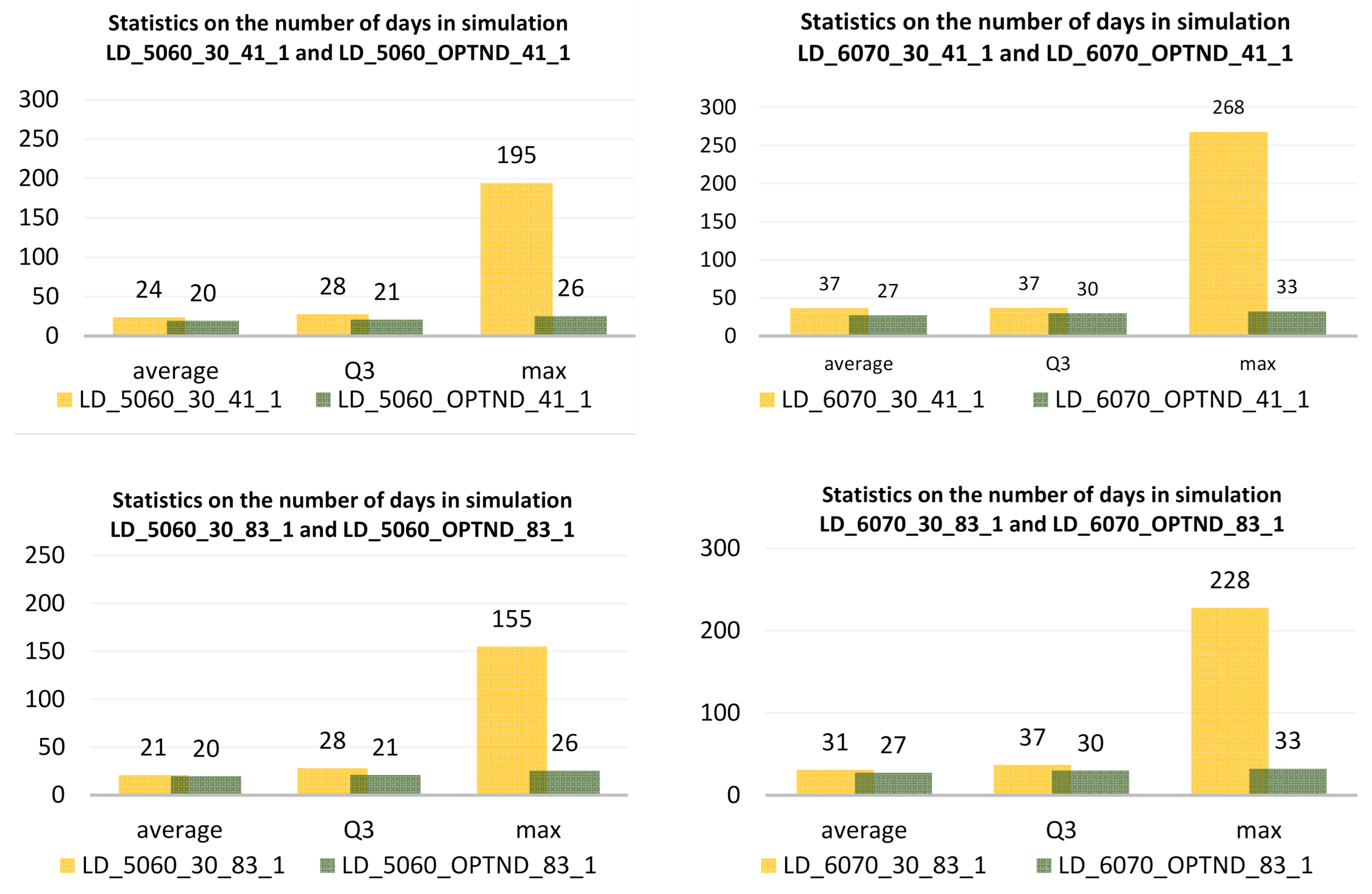
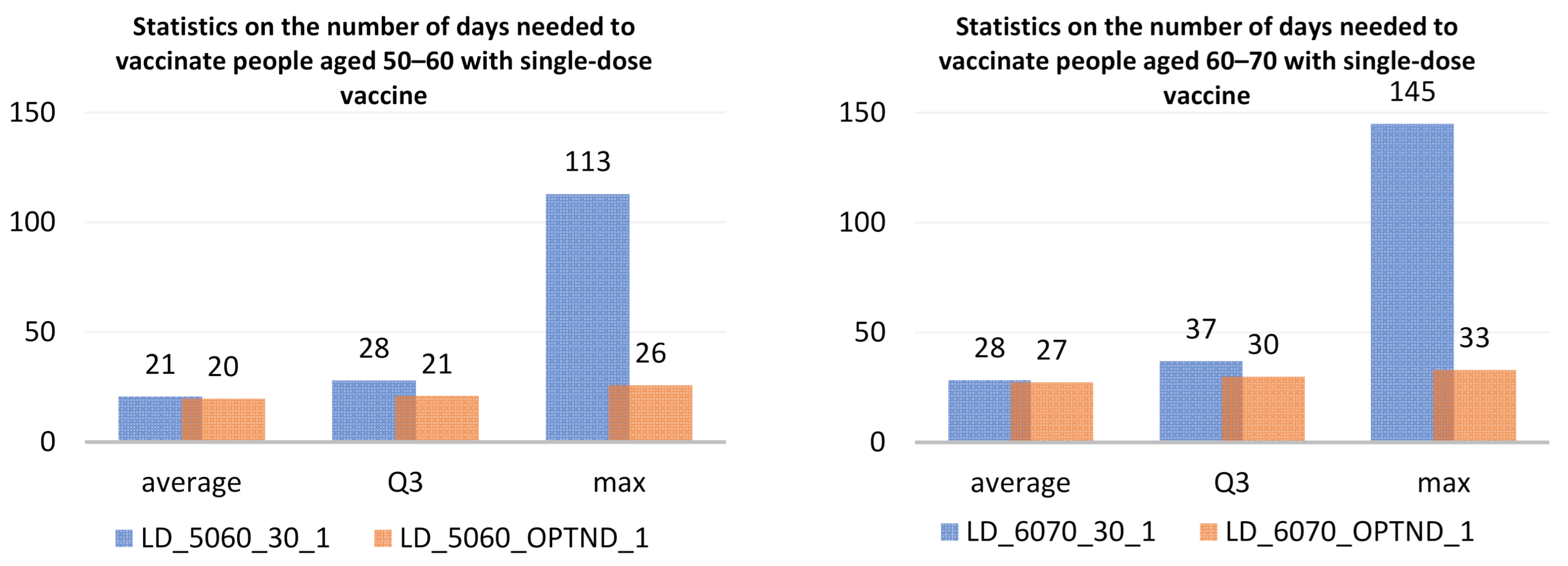
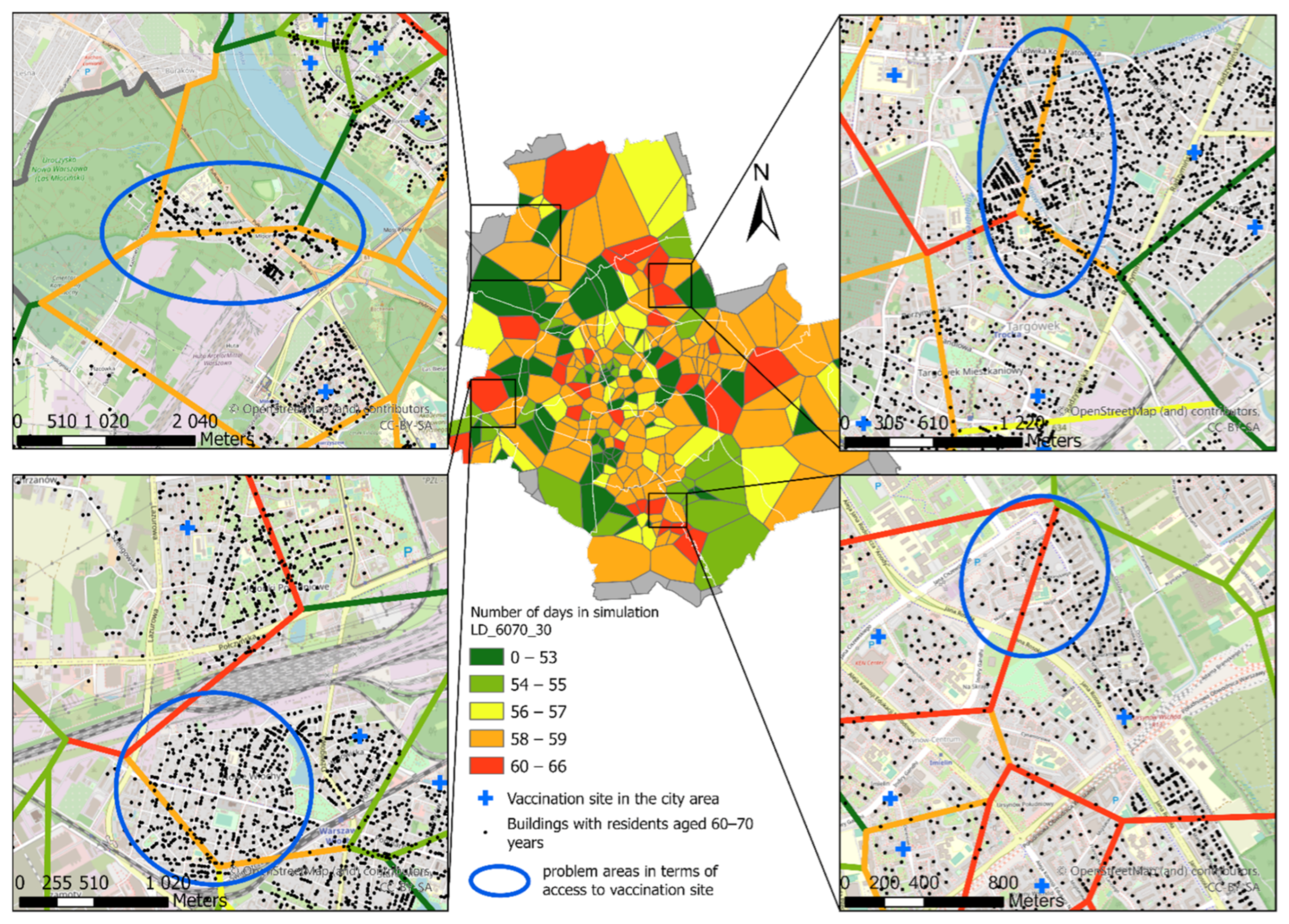
3.3. Simulations of the Number of Days Needed to Vaccinate Each Studied Age Group
4. Discussion
5. Conclusions
A nationalistic rather than a global approach to COVID-19 vaccine availability, distribution, and delivery will make a pessimistic outcome much more likely. Additionally, unless countries work together to scale up prevention efforts, the risk of other pandemics, or other transboundary disasters with similar consequences, including those fuelled by climate change, will remain a constant threat [57].
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Bank. The COVID-19 Pandemic: Shocks to Education and Policy Responses; World Bank: Washington, DC, USA, 2021; Available online: https://openknowledge.worldbank.handle/10986/33696 (accessed on 19 March 2021).
- Global Economic Prospects. International Bank for Reconstruction and Development/The World Bank. Available online: https://openknowledge.worldbank.bitstream/handle/10986/33748/9781464815539.pdf (accessed on 2 April 2021).
- World Bank. The Economy in the Time of Covid-19; LAC Semiannual Report, April 2020; World Bank: Washington, DC, USA, 2021; Available online: https://openknowledge.worldbank.handle/10986/33555 (accessed on 19 March 2021).
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 2 April 2021).
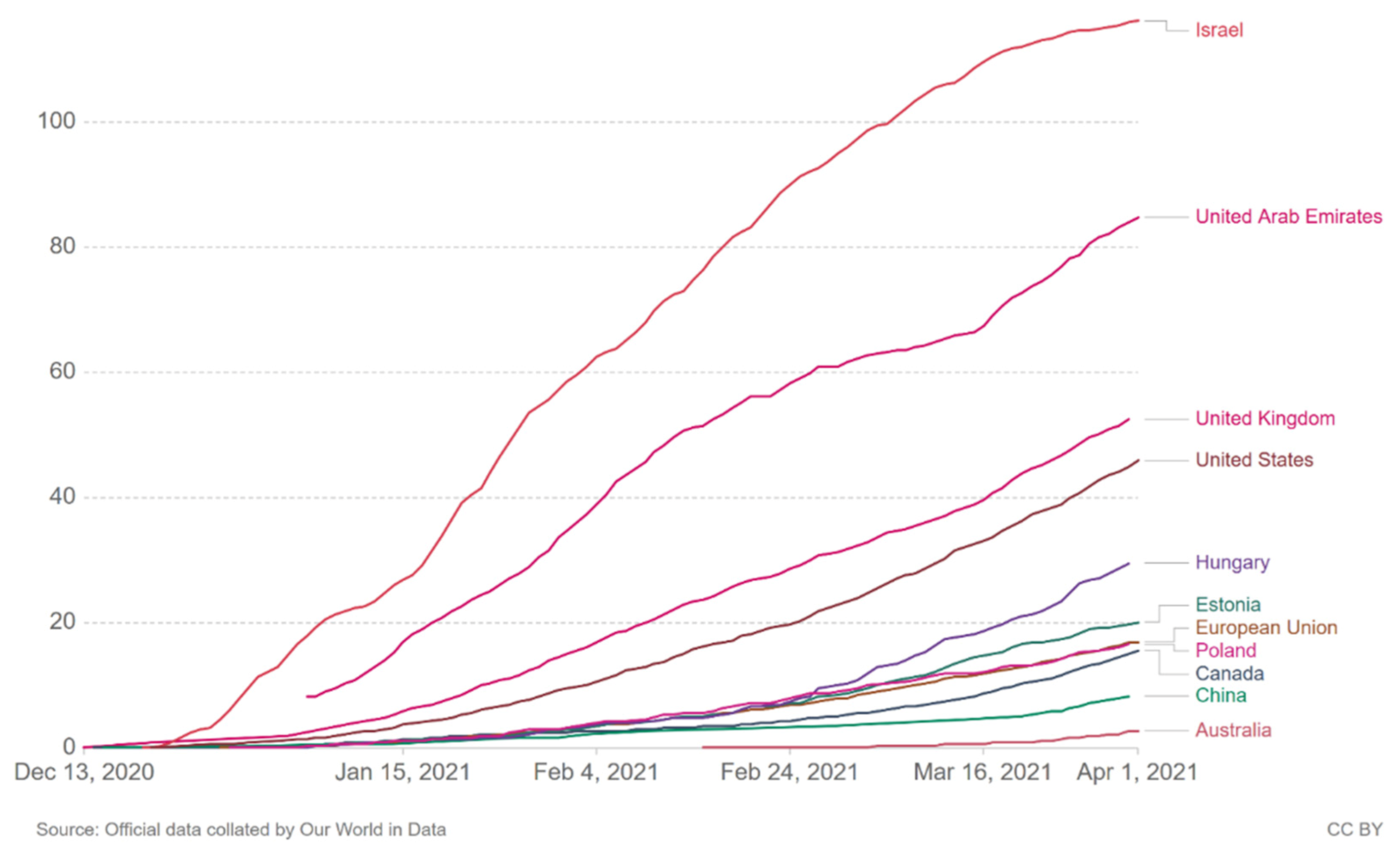
- Our World in Data. 2021. Available online: https://ourworldindata.org (accessed on 1 April 2021).
- Chinazzi, M.; Davis, J.T.; Ajelli, M.; Gioannini, C.; Litvinova, M.; Merler, S.; Pastore y Piontti, A.; Mu, K.; Rossi, L.; Sun, K.; et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science 2020, 368, 395–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarrataca, L.; Dias, C.M.; Haddad, D.B.; De Arruda, E.F. Flattening the curves: On-off lock-down strategies for COVID-19 with an application to Brazil. J. Math. Ind. 2021, 11, 2. [Google Scholar] [CrossRef] [PubMed]
- Schlosser, F.; Maier, B.F.; Jack, O.; Hinrichs, D.; Zachariae, A.; Brockmann, D. COVID-19 lockdown induces disease-mitigatingstructural changes in mobility networks. Proc. Natl. Acad. Sci. USA 2020, 117, 32883–32890. [Google Scholar] [CrossRef] [PubMed]
- EUROSTAT, GDP and Main Components (Output, Expenditure and Income). 2021. Available online: https://ec.europa.eu/eurostat/databrowser/view/NAMQ_10_GDP__custom_77309/bookmark/table?lang=en&bookmarkId=b74febcd-e664-4f22-9c93-2ef510fe371f (accessed on 21 March 2021).
- Overview of the Implementation of COVID-19 Vaccination Strategies and Vaccine Deployment Plans in the EU/EEA. 2021. Available online: https://www.ecdc.europa.eu/en/publications-data/overview-implementation-covid-19-vaccination-strategies-and-vaccine-deployment (accessed on 1 April 2021).
- WHO COVAX. Available online: https://www.who.int/initiatives/act-accelerator/covax (accessed on 21 March 2021).
- Omer, S.B.; Yildirim, I.; Forman, H.P. Herd Immunity and Implications for SARS-CoV-2 Control. JAMA 2020, 324, 2095–2096. [Google Scholar] [CrossRef]
- Aschwanden, C. The false promise of herd immunity for COVID-19. Nature 2020, 587, 26–28. [Google Scholar] [CrossRef]
- Aschwenden, C. Five reasons why COVID herd immunity is probably impossible. Nature 2021, 591, 520–522. [Google Scholar] [CrossRef]
- Rader, B.; Scarpino, S.; Nande, A.; Hill, A.; Dalziel, B.; Reiner, R.; Pigott, D.; Gutierrez, B.; Shrestha, M.; Brownstein, J.; et al. Crowding and the epidemic intensity of COVID-19 transmission. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Guo, X.; Pan, H.; Zhong, S. What determines city’s resilience against epidemic outbreak: Evidence from China’s COVID-19 experience. Sustain. Cities Soc. 2021, 70, 102892. [Google Scholar] [CrossRef]
- Kraemer, M.U.G.; Yang, C.-H.; Gutierrez, B.; Wu, C.-H.; Klein, B.; Pigott, D.M.; Scarpino, S.V. The effect of human mobility and control measures on the COVID-19 epidemic in China. Science 2020, 368, 493–497. [Google Scholar] [CrossRef] [Green Version]
- MacIntyre, C.R.; Costantino, V.; Trent, M. Modelling of COVID-19 vaccination strategies and herd immunity, in scenarios of limited and full vaccine supply in NSW, Australia. Vaccine 2021. In Press. [Google Scholar] [CrossRef]
- Kwok, K.O.; Lai, F.; Wei, W.I.; Wong, S.Y.S.; Tang, J.W.T. Herd immunity—Estimating the level required to halt the COVID-19 epidemics in affected countries. J. Infect. 2020, 80, e32–e33. [Google Scholar] [CrossRef]
- Gomes, D.S.; Andrade, L.A.; Ribeiro, C.J.N.; Peixoto, M.V.S.; Lima, S.; Duque, A.M.; Cirilo, T.M.; Góes, M.A.O.; Lima, A.; Santos, M.B.; et al. Risk clusters of COVID-19 transmission in northeastern Brazil: Prospective space-time modelling. Epidemiol. Infect. 2020, 148, e188. [Google Scholar] [CrossRef]
- Gomes, M.G.M.; Corder, R.M.; King, J.G.; Langwig, K.E.; Souto-Maior, C.; Carneiro, J.; Penha-Gonçalves, G.G.C.; Ferreira, M.U.; Aguas, R. Individual variation in susceptibility or exposure to SARS-CoV-2 lowers the herd immunity threshold. medRxiv 2020. [Google Scholar] [CrossRef]
- Rossman, H.; Shilo, S.; Meir, T.; Gorfine, M.; Shalit, U.; Segal, E. COVID-19 dynamics after a national immunization program in Israel. Nat. Med. 2021, 1–17. [Google Scholar] [CrossRef]
- European Commission. Communication from the Commission to the European Parliament and the Council. In A United Front to Beat COVID-19; European Commission: Brussels, Belgium, 2021; Available online: https://ec.europa.eu/info/sites/info/files/communication-united-front-beat-covid-19_en.pdf (accessed on 21 March 2021).
- European Centre for Disease Prevention and Control (ECDC), COVID-19 Vaccine Tracker. Available online: https://vaccinetracker.ecdc.europa.eu/public/extensions/COVID-19/vaccine-tracker.html (accessed on 2 April 2021).
- Ministry of Health (Poland). 2021. Available online: https://www.gov.pl/web/szczepimysie/raport-szczepien-przeciwko-covid-19 (accessed on 2 April 2021).
- Statistics Poland, Socio-Economic Situation of the Country in 2020. Available online: https://stat.gov.pl/download/gfx/portalinformacyjny/pl/defaultaktualnosci/5498/1/104/1/sytuacja_spoleczno-gospodarcza.pdf (accessed on 23 March 2021).
- Goujard, A.; Guérin, P. Boosting SMEs’ Internationalisation in Poland, OECD Economics Department Working Papers, No. 1654; OECD Publishing: Paris, France, 2021. [Google Scholar]
- National COVID-19 Immunization Program. 2020. Available online: https://www.gov.pl/attachment/d4663c78-4c3c-4cf1-87f0-608ba273e947 (accessed on 21 March 2021).
- Politykazdrowotna.com. Available online: https://www.politykazdrowotna.com/69725,szef-kprm-mamy-juz-zaszczepionych-ponad-94-proc-wszystkich-lekarzy (accessed on 2 April 2021).
- Thornton, L.E.; Pearce, J.R.; Kavanagh, A.M. Using Geographic Information Systems (GIS) to assess the role of the built environment in influencing obesity: A glossary. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 71. [Google Scholar] [CrossRef] [Green Version]
- Pearce, J.; Witten, K.; Bartie, P. Neighbourhoods and health: A GIS approach to measuring community resource accessibility. J. Epidemiol. Commun. Health 2006, 60, 389–395. [Google Scholar] [CrossRef] [Green Version]
- Manonmani, R.; Prabaharan, S.; Vidhya, R.; Ramalingam, M. Application of GIS in urban utility mapping using image processing techniques. GeoSpat. Inf. Sci. 2012, 15, 271–275. [Google Scholar] [CrossRef]
- Kyushik, O.; Seunghyun, J. Assessing the spatial distribution of urban parks using GIS. Landsc. Urban Plan. 2007, 82, 1–2. [Google Scholar] [CrossRef]
- Kim, Y.; Byon, Y.-J.; Yeo, H. Enhancing healthcare accessibility measurements using GIS: A case study in Seoul, Korea. PLoS ONE 2018, 13, e0193013. [Google Scholar] [CrossRef] [Green Version]
- Cetin, M. Using GIS analysis to assess urban green space in terms of accessibility: Case study in Kutahya. Int. J. Sustain. Dev. World Ecol. 2015, 22, 420–424. [Google Scholar] [CrossRef]
- Franch-Pardo, A.; Napoletano, B.M.; Rosete-Verges, F.; Billa, L. Spatial analysis and GIS in the study of COVID-19. A review. Sci. Total Environ. 2020, 739, 140033. [Google Scholar] [CrossRef] [PubMed]
- Fatima, M.; O’Keefe, K.J.; Wei, W.; Arshad, S.; Gruebner, O. Geospatial Analysis of COVID-19: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 2336. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Liao, H.; Marley, G.; Wang, Z.; Cheng, W.; Wu, D.; Yu, R. The Changing Patterns of Coronavirus Disease 2019 (COVID-19) in China: A Tempogeographic Analysis of the Severe Acute Respiratory Syndrome Coronavirus 2 Epidemic. Clin. Infect. Dis. 2020, 71, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Deng, M.; Li, C.; Huang, J. Spatio-Temporal Patterns of the 2019-nCoV Epidemic at the County Level in Hubei Province, China. Int. J. Environ. Res. Public Health 2020, 17, 2563. [Google Scholar] [CrossRef] [Green Version]
- Ren, H.; Zhao, L.; Zhang, A.; Song, L.; Liao, Y.; Lu, W.; Cui, C. Early forecasting of the potential risk zones of COVID-19 in China’s megacities. Sci. Total Environ. 2020, 729, 138995. [Google Scholar] [CrossRef]
- Azevedo, L.; Pereira, M.J.; Ribeiro, M.C.; Soares, A. Geostatistical COVID-19 infection risk maps for Portugal. Int. J. Health Geogr. 2020, 19, 1–8. [Google Scholar] [CrossRef]
- Cavalcante, J.R.; Abreu, A.J.L. COVID-19 in the city of Rio de Janeiro: Spatial analysis of first confirmed cases and deaths. Epidemiol. Serv. Saude 2020, 29, 9. [Google Scholar]
- Andrade, L.A.; Gomes, D.S.; Góes, M.A.; Souza, M.S.; Teixeira, D.C.; Ribeiro, C.J.; Alves, J.A.; Araújo, K.C.; Santos, A.D. Surveillance of the first cases of COVID-19 in Sergipe using a prospective spatiotemporal analysis: The spatial dispersion and its public health implications. Rev. Soc. Bras. Med. Trop. 2020, 53. [Google Scholar] [CrossRef]
- Oteri, J.; Hussaini, M.I.; Bawa, S.; Ibizugbe, S.; Lambo, K.; Mogekwu, F.; Wiwa, O.; Seaman, V.; Kolbe-Booysen, O.; Braka, F.; et al. Application of the Geographic Information System (GIS) in immunisation service delivery; its use in the 2017/2018 measles vaccination campaign in Nigeria. Vaccine 2021. [Google Scholar] [CrossRef]
- Ali, D.; Levin, A.; Abdulkarim, M.; Tijjani, U.; Ahmed, B.; Namalam, F.; Oyewole, F.; Dougherty, L. A cost-effectiveness analysis of traditional and geographic information system-supported microplanning approaches for routine immunization program management in northern Nigeria. Vaccine 2020, 38, 1408–1415. [Google Scholar] [CrossRef]
- Barau, I.; Zubairu, M.; Mwanza, M.N.; Seaman, V.Y. Improving Polio Vaccination Coverage in Nigeria Through the Use of Geographic Information System Technology. J. Infect. Dis. 2014, 210 (Suppl. S1), S102–S110. [Google Scholar] [CrossRef] [Green Version]
- Kazi, A.M.; Ali, M.; Ayub, K.; Kalimuddin, H.; Zubair, K.; Kazi, A.N.; Artani, A.; Ali, S.A. Geo-spatial reporting for monitoring of household immunization coverage through mobile phones: Findings from a feasibility study. Int. J. Med. Inform. 2017, 107, 48–55. [Google Scholar] [CrossRef]
- Utazi, C.E.; Thorley, J.; Alegana, V.A.; Ferrari, M.J.; Takahashi, S.; Metcalf, C.J.E.; Lessler, J.; Cutts, F.T.; Tatem, A.J. Mapping vaccination coverage to explore the effects of delivery mechanisms and inform vaccination strategies. Nat. Commun. 2019, 10, 1633. [Google Scholar] [CrossRef]
- Statistics Poland, Area and Population in the Territorial Profile in 2020. Table 21. Area, Population and Ranking Positions by Gminas. Available online: https://stat.gov.pl/obszary-tematyczne/ludnosc/ludnosc/powierzchnia-i-ludnosc-w-przekroju-terytorialnym-w-2020-roku,7,17.html (accessed on 12 March 2021).
- Statistics Poland, Local Data Bank. Available online: https://bdl.stat.gov.pl/BDL/metadane/metryka/2137?back=True (accessed on 22 March 2021).
- Chancellery of the Prime Minister, Rejestr PESEL. Available online: https://www.gov.pl/web/cyfryzacja/rejestr-pesel1 (accessed on 12 March 2021).
- Kałuża-Kopias, D. Specyfika przemieszczeń wewnętrznych osób starszych w Polsce. Studia Demograficzne 2014, 2, 97–120. [Google Scholar] [CrossRef]
- Ratajski, L. Metodyka Kartografii Społeczno-Gospodarczej; PPWK: Warsaw, Poland, 1989. [Google Scholar]
- Silverman, B.W. Density Estimation for Statistics and Data Analysis; Chapman and Hall: New York, NY, USA, 1986. [Google Scholar]
- Communication of the Ministry of Health on the Use of Vaccination Schedules Against COVID-19 with AstraZeneca, Pfizer/BioNTech and Moderna. Available online: https://szczepienia.pzh.gov.pl/komunikat-mz-dotyczacy-stosowania-schematow-szczepein-pzreciw-covid-19-preparatami-astrazeneca-pfizer-biontech-oraz-moderna/ (accessed on 23 March 2021).
- Centrum e-Zdrowia. Internetowe Konto Pacjenta Pomocne w Pandemii. Available online: https://cez.gov.pl/aktualnosci/szczegoly/internetowe-konto-pacjenta-pomocne-w-pandemii/ (accessed on 23 March 2021).
- Skegg, D.; Gluckman, P.; Boulton, G.; Hackmann, H.; Karim, S.S.A.; Piot, P.; Woopen, C. Future scenarios for the COVID-19 pandemic. Lancet 2021, 397, 777–778. [Google Scholar] [CrossRef]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scenario | Simulation Abbreviation | Description of the Simulation |
|---|---|---|
| 1 | LD_5060_30 | Number of days needed to vaccinate people aged 50–60 years, based on 30 doses per day (same number of doses at each vaccination site) and any interval between doses |
| 1 | LD_6070_30 | Number of days needed to vaccinate people aged 60–70 years, based on 30 doses per day (same number of doses at each vaccination site) and any interval between doses |
| 1 | LD_5060_30_41_1 | Number of days needed to vaccinate people aged 50–60 years with the first dose based on 30 doses per day (same number of doses at each vaccination site) and an interval between doses of 41 days |
| 1 | LD_6070_30_41_1 | Number of days needed to vaccinate people aged 60–70 years with the first dose based on 30 doses per day (same number of doses at each vaccination site) and an interval between doses of 41 days |
| 1 | LD_5060_30_83_1 | Number of days needed to vaccinate people aged 50–60 years with the first dose based on 30 doses per day (same number of doses at each vaccination site) and an interval between doses of 83 days |
| 1 | LD_6070_30_83_1 | Number of days needed to vaccinate people aged 60–70 years with the first dose based on 30 doses per day (same number of doses at each vaccination site) and an interval between doses of 83 days |
| 3a | LD_5060_30_1 | Number of days needed to vaccinate people aged 50–60 years with the single dose vaccine based on 30 doses per day (the same number of doses at each vaccination site) |
| 3a | LD_6070_30_1 | Number of days needed to vaccinate people aged 60–70 years with the single dose vaccine based on 30 doses per day (the same number of doses at each vaccination site) |
| 2 | LD_5060_OPTND | Number of days needed to vaccinate people aged 50–60 years, assuming an optimized number of doses per day and any interval between doses |
| 2 | LD_6070_OPTND | Number of days needed to vaccinate people aged 60–70 years, assuming an optimized number of doses per day and any interval between doses |
| 2 | LD_5060_OPTND_41_1 | Number of days needed to vaccinate people aged 50–60 years with the first dose based on the optimized number of doses per day and an interval between doses of 41 days |
| 2 | LD_6070_OPTND_41_1 | Number of days needed to vaccinate people aged 60–70 years with the first dose based on the optimized number of doses per day and an interval between doses of 41 days |
| 2 | LD_5060_OPTND_83_1 | Number of days needed to vaccinate people aged 50–60 years with the first dose based on the optimized number of doses per day and an interval between doses of 83 days |
| 2 | LD_6070_OPTND_83_1 | Number of days needed to vaccinate people aged 60–70 years with the first dose based on the optimized number of doses per day and an interval between doses of 83 days |
| 3b | LD_5060_OPTND_1 | Number of days needed to vaccinate people aged 50–60 years with the single dose vaccine assuming an optimized number of doses per day |
| 3b | LD_6070_OPTND_1 | Number of days needed to vaccinate people aged 60–70 years with the single dose vaccine assuming an optimized number of doses per day |
| Simulation | 0.2-Quantile | 0.4-Quantile | 0.6-Quantile | 0.8-Quantile | Max Value |
|---|---|---|---|---|---|
| LD_5060_OPTND | 39 | 40 | 41 | 42 | 52 |
| LD_6070_OPTND | 53 | 57 | 58 | 59 | 66 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krzysztofowicz, S.; Osińska-Skotak, K. The Use of GIS Technology to Optimize COVID-19 Vaccine Distribution: A Case Study of the City of Warsaw, Poland. Int. J. Environ. Res. Public Health 2021, 18, 5636. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115636
Krzysztofowicz S, Osińska-Skotak K. The Use of GIS Technology to Optimize COVID-19 Vaccine Distribution: A Case Study of the City of Warsaw, Poland. International Journal of Environmental Research and Public Health. 2021; 18(11):5636. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115636
Chicago/Turabian StyleKrzysztofowicz, Sylwia, and Katarzyna Osińska-Skotak. 2021. "The Use of GIS Technology to Optimize COVID-19 Vaccine Distribution: A Case Study of the City of Warsaw, Poland" International Journal of Environmental Research and Public Health 18, no. 11: 5636. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18115636