
Immigration and Gender as Social Determinants of Mental Health during the COVID-19 Outbreak: The Case of US Latina/os



Abstract
:1. Introduction
1.1. Mental Health Outcomes: The Intangible Implications of Public Health Emergencies
1.2. An Intersectional Approach on Mental Health Outcomes during COVID-19
1.2.1. Gendered Health
1.2.2. Immigration as a Social Determinant of Health
1.2.3. Intersectionality and COVID-19
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
6. Recommendations and Avenues for Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Model Specification
Appendix B. Predicted Probabilities of the Three-Way Interaction

{kind=link}
{kind=link}
{kind=link}
| Mental Health Issues | Characteristics | Margin | SE | CI |
|---|---|---|---|---|
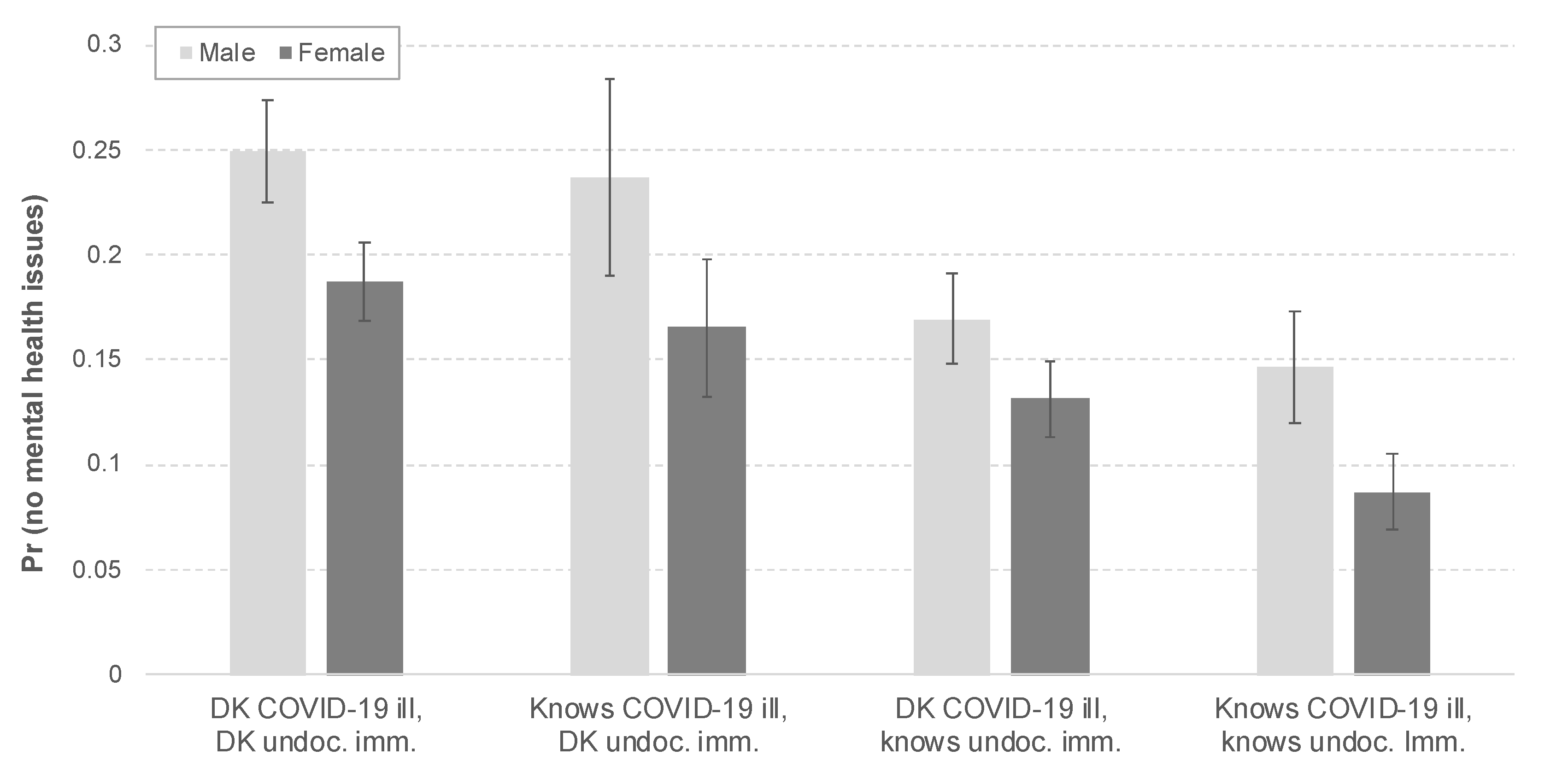
| 0 | Male, DK COVID-19 ill, DK undoc. imm. | 0.250 | 0.024 | 0.202–0.297 |
| Male, DK COVID-19 ill, knows undoc. imm. | 0.170 | 0.022 | 0.127–0.212 | |
| Male, knows COVID-19 ill, DK undoc. imm. | 0.236 | 0.047 | 0.145–0.328 | |
| Male, knows COVID-19 ill, knows undoc. imm. | 0.147 | 0.027 | 0.094–0.199 | |
| Female, DK COVID-19 ill, DK undoc. imm. | 0.187 | 0.019 | 0.150–0.224 | |
| Female, DK COVID-19 ill, knows undoc. imm. | 0.132 | 0.018 | 0.096–0.167 | |
| Female, knows COVID-19 ill, DK undoc. imm. | 0.165 | 0.033 | 0.102–0.229 | |
| Female, knows COVID-19 ill, knows undoc. imm. | 0.087 | 0.018 | 0.052–0.122 | |
| 1 | Male, DK COVID-19 ill, DK undoc. imm. | 0.127 | 0.012 | 0.103–0.151 |
| Male, DK COVID-19 ill, knows undoc. imm. | 0.101 | 0.012 | 0.078–0.124 | |
| Male, knows COVID-19 ill, DK undoc. imm. | 0.123 | 0.016 | 0.091–0.155 | |
| Male, knows COVID-19 ill, knows undoc. imm. | 0.092 | 0.014 | 0.065–0.119 | |
| Female, DK COVID-19 ill, DK undoc. imm. | 0.108 | 0.011 | 0.086–0.129 | |
| Female, DK COVID-19 ill, knows undoc. imm. | 0.085 | 0.011 | 0.064–0.106 | |
| Female, knows COVID-19 ill, DK undoc. imm. | 0.100 | 0.015 | 0.070–0.129 | |
| Female, knows COVID-19 ill, knows undoc. imm. | 0.062 | 0.011 | 0.040–0.084 | |
| 2 | Male, DK COVID-19 ill, DK undoc. imm. | 0.139 | 0.011 | 0.117–0.161 |
| Male, DK COVID-19 ill, knows undoc. imm. | 0.125 | 0.012 | 0.102–0.147 | |
| Male, knows COVID-19 ill, DK undoc. imm. | 0.138 | 0.012 | 0.114–0.161 | |
| Male, knows COVID-19 ill, knows undoc. imm. | 0.117 | 0.013 | 0.092–0.143 | |
| Female, DK COVID-19 ill, DK undoc. imm. | 0.129 | 0.011 | 0.108–0.151 | |
| Female, DK COVID-19 ill, knows undoc. imm. | 0.111 | 0.011 | 0.089–0.133 | |
| Female, knows COVID-19 ill, DK undoc. imm. | 0.124 | 0.013 | 0.097–0.150 | |
| Female, knows COVID-19 ill, knows undoc. imm. | 0.088 | 0.013 | 0.062–0.113 | |
| 3 | Male, DK COVID-19 ill, DK undoc. imm. | 0.167 | 0.012 | 0.144–0.190 |
| Male, DK COVID-19 ill, knows undoc. imm. | 0.173 | 0.012 | 0.150–0.196 | |
| Male, knows COVID-19 ill, DK undoc. imm. | 0.169 | 0.013 | 0.143–0.195 | |
| Male, knows COVID-19 ill, knows undoc. imm. | 0.171 | 0.012 | 0.147–0.195 | |
| Female, DK COVID-19 ill, DK undoc. imm. | 0.173 | 0.012 | 0.150–0.196 | |
| Female, DK COVID-19 ill, knows undoc. imm. | 0.168 | 0.012 | 0.144–0.191 | |
| Female, knows COVID-19 ill, DK undoc. imm. | 0.173 | 0.012 | 0.150–0.196 | |
| Female, knows COVID-19 ill, knows undoc. imm. | 0.148 | 0.015 | 0.119–0.177 | |
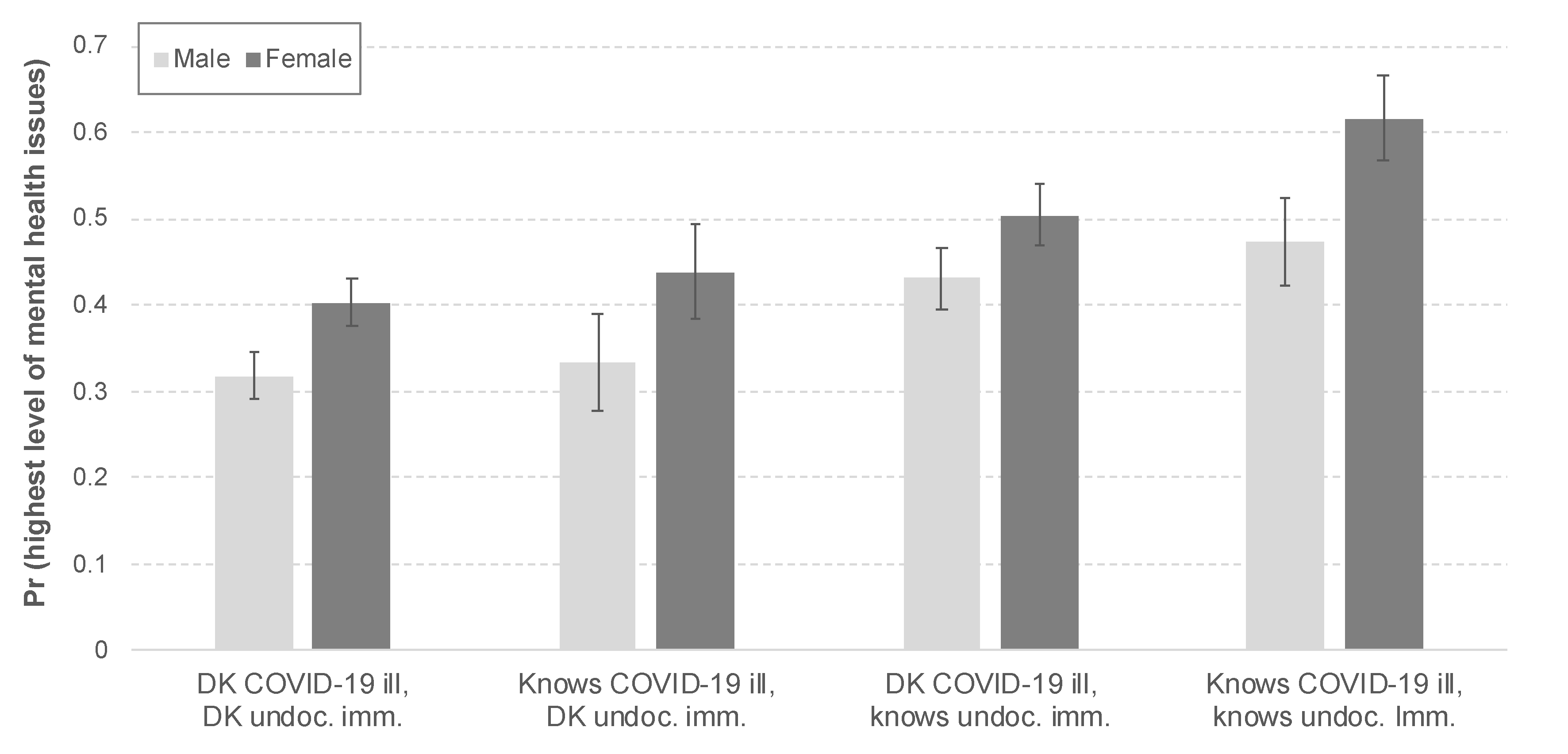
| 4 | Male, DK COVID-19 ill, DK undoc. imm. | 0.318 | 0.027 | 0.265–0.371 |
| Male, DK COVID-19 ill, knows undoc. imm. | 0.431 | 0.036 | 0.362–0.501 | |
| Male, knows COVID-19 ill, DK undoc. imm. | 0.334 | 0.057 | 0.223–0.445 | |
| Male, knows COVID-19 ill, knows undoc. imm. | 0.473 | 0.051 | 0.374–0.573 | |
| Female, DK COVID-19 ill, DK undoc. imm. | 0.403 | 0.028 | 0.348–0.457 | |
| Female, DK COVID-19 ill, knows undoc. imm. | 0.504 | 0.036 | 0.433–0.575 | |
| Female, knows COVID-19 ill, DK undoc. imm. | 0.438 | 0.056 | 0.329–0.547 | |
| Female, knows COVID-19 ill, knows undoc. imm. | 0.616 | 0.050 | 0.519–0.713 |
References
- John Hopkins University (JHU). COVID-19 Dashboard by the Center Systems Science and Engineering (CSSE). Available online: https://0-coronavirus-jhu-edu.brum.beds.ac.uk/map.html (accessed on 25 May 2021).
- Structural Inequalities and Not Behavior Explain Covid-19 Racial Disparities. Latino Rebels, 2020. Available online: https://www.latinorebels.com/2020/05/01/structuralinequalitiescovid/ (accessed on 11 May 2021).
- Compliant but Unprotected: Communities of Color. Take Greater Action to Prevent the Spread of COVID-19 but Remain at Risk. Interdisciplinary Association for Population Health Science, 2020. Available online: http://compliant-but-unprotected-communities-of-color-take-greater-action-to-prevent-the-spread-of-covid-19-but-remain-at-risk/ (accessed on 28 May 2021).
- Powell, C. The Color and Gender of COVID: Essential Workers, Not Disposable People. Think Global Health, 2020. Available online: https://www.thinkglobalhealth.org/article/color-and-gender-covid-essential-workers-not-disposable-people (accessed on 11 May 2021).
- Where the Women Aren’t: On Coronavirus Task Forces. NPR, 24 June 2020. Available online: https://www.npr.org/sections/goatsandsoda/2020/06/24/882109538/where-the-women-arent-on-coronavirus-task-forces (accessed on 25 May 2021).
- Algasseer, N.; Dresden, E.; Keeney, G.; Warren, N. Status of women and infants in complex humanitarian emergencies. J. Midwif. Women’s Health 2004, 49, 7–13. [Google Scholar] [CrossRef]
- Latino Decisions. SOMOS—COVID-19 Crisis National Latino Survey. April 2020. Available online: https://latinodecisions.com/polls-and-research/somos-covid-19-crisis-national-latino-survey-april-2020/ (accessed on 25 May 2021).
- Reger, M.A.; Stanley, I.H.; Joiner, T.E. Suicide Mortality and Coronavirus Disease 2019—A Perfect Storm? JAMA Psychiatry 2020, 77, 1093–1094. [Google Scholar] [CrossRef] [Green Version]
- Sher, L. The impact of the COVID-19 pandemic on suicide rates. QJM Int. J. Med. 2020, 113, 707–712. [Google Scholar] [CrossRef]
- Greenberg, N.; Docherty, M.; Gnanapragasam, S.; Wessely, S. Managing mental health challenges faced by healthcare workers during covid-19 pandemic. BMJ 2020, 368, m1211. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.-H.; Lin, H.-H.; Wang, C.-C.; Jhang, S. How to Defend COVID-19 in Taiwan? Talk about People’s Disease Awareness, Attitudes, Behaviors and the Impact of Physical and Mental Health. Int. J. Environ. Res. Public Health 2020, 17, 4694. [Google Scholar] [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jalloh, M.F.; Li, W.; Bunnell, R.E.; Ethier, K.A.; O’Leary, A.; Hageman, K.M.; Sengeh, P.; Jalloh, M.B.; Morgan, O.; Hersey, S.; et al. Impact of Ebola experiences and risk perceptions on mental health in Sierra Leone, July 2015. BMJ Glob. Health 2018, 3, e000471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.M.; Kang, W.S.; Cho, A.-R.; Kim, T.; Park, J.K. Psychological impact of the 2015 MERS outbreak on hospital workers and quarantined hemodialysis patients. Compr. Psychiatry 2018, 87, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Mak, I.W.C.; Chu, C.M.; Pan, P.C.; Yiu, M.G.C.; Chan, V.L. Long-term psychiatric morbidities among SARS survivors. Gen. Hosp. Psychiatry 2009, 31, 318–326. [Google Scholar] [CrossRef]
- Case, A.; Angus, D. Deaths of Despair and the Future of Capitalism; Princeton University Press: Princeton, NJ, USA, 2020. [Google Scholar]
- Sanchez, G.R.; Vargas, E.D.; Juarez, M.D.; Gomez-Aguinaga, B.; Pedraza, F.I. Nativity and citizenship status affect Latinos’ health insurance coverage under the ACA. J. Ethn. Migr. Stud. 2017, 43, 2037–2054. [Google Scholar] [CrossRef]
- Juárez, M.; Gomez-Aguinaga, B.; Bettez, S.P. Twenty years after IIRIRA: The rise of immigrant detention and its effects on Latinx communities across the nation. J. Migrat. Human Securit. 2018, 6, 74–96. [Google Scholar] [CrossRef]
- Dijkstra-Kersten, S.M.A.; Biesheuvel-Leliefeld, K.E.M.; van der Wouden, J.; Penninx, B.W.J.H.; Van Marwijk, H.W.J. Associations of financial strain and income with depressive and anxiety disorders. J. Epidemiol. Community Health 2015, 69, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Reeves, A.; Stuckler, D.; McKee, M.; Gunnell, D.; Chang, S.-S.; Basu, S. Increase in state suicide rates in the USA during economic recession. Lancet 2012, 380, 1813–1814. [Google Scholar] [CrossRef]
- Karpman, M.; Dulce, G.; Genevieve, M.K. Parents are Struggling to Provide for Their Families during the Pandemic; Urban Institute: Washington, DC, USA, 2020. [Google Scholar]
- Mwarumba, N. Global Social Vulnerability to Pandemics: An Examination of Social Determinants of H1N1 2009 Mortality. Ph.D. Thesis, Oklahoma State University, Stillwater, OK, USA, 2017. [Google Scholar]
- López, N.; Vargas, E.D.; Juarez, M.; Cacari-Stone, L.; Bettez, S. What’s Your Street Race? Leveraging Multidimensional Measures of Race and Intersectionality for Examining Physical and Mental Health Status among Latinxs. Sociol. Race Ethn. 2018, 4, 49–66. [Google Scholar] [CrossRef] [Green Version]
- Sampaio, A. Racing and gendering immigration politics: Analyzing contemporary immigration enforcement using intersectional analysis. Pol. Groups Ident. 2014, 2, 202–221. [Google Scholar] [CrossRef]
- Collins, P.H. Black Feminist Thought: Knowledge, Consciousness, and the Politics of Empowerment; Routledge: Oxfordshire, UK, 2002. [Google Scholar]
- Seng, J.S.; Lopez, W.D.; Sperlich, M.; Hamama, L.; Meldrum, C.D.R. Marginalized identities, discrimination burden, and mental health: Empirical exploration of an interpersonal-level approach to modeling intersectionality. Soc. Sci. Med. 2012, 75, 2437–2445. [Google Scholar] [CrossRef] [Green Version]
- CDC (Centers for Disease Control and Prevention). Racial and Ethnic Disparities Continue in Pregnancy-Related Deaths. CDC Newsroom. Available online: https://www.cdc.gov/media/releases/2019/p0905-racial-ethnic-disparities-pregnancy-deaths.html (accessed on 25 May 2021).
- Mays, V.M.; Cochran, S.D.; Barnes, N.W. Race, Race-Based Discrimination, and Health Outcomes Among African Americans. Annu. Rev. Psychol. 2007, 58, 201–225. [Google Scholar] [CrossRef] [Green Version]
- Eaton, N.R.; Keyes, K.M.; Krueger, R.F.; Balsis, S.; Skodol, A.E.; Markon, K.E.; Grant, B.F.; Hasin, D.S. An invariant dimensional liability model of gender differences in mental disorder prevalence: Evidence from a national sample. J. Abnorm. Psychol. 2012, 121, 282–288. [Google Scholar] [CrossRef] [Green Version]
- Richards, E.M. Mental Health Among African-American Women. John Hopkins Medicine. Available online: https://www.hopkinsmedicine.org/health/wellness-and-prevention/mental-health-among-african-american-women (accessed on 11 May 2021).
- Campbell, L. Why Many Men Have a Harder Time Seeking Treatment for Mental Illness. Health Line, 2019. Available online: https://www.healthline.com/health-news/how-can-we-reduce-mens-mental-health-stigma (accessed on 11 April 2021).
- Lawrance, B. Ebola’s Would-be Refugees: Performing Fear and Navigating Asylum During a Public Health Emergency. Med. Anthr. 2018, 37, 514–532. [Google Scholar] [CrossRef] [Green Version]
- Petchesky, R.P. Biopolitics at the crossroads of sexuality and disaster: The case of Haiti. In The Ashgate Research Companion to the Globalization of Health; Routledge: Oxfordshire, UK, 2016; pp. 191–212. [Google Scholar]
- Vedam, S.; Council, G.-U.S.; Stoll, K.; Taiwo, T.K.; Rubashkin, N.; Cheyney, M.; Strauss, N.; McLemore, M.; Cadena, M.; Nethery, E.; et al. The Giving Voice to Mothers study: Inequity and mistreatment during pregnancy and childbirth in the United States. Reprod. Health 2019, 16, 77. [Google Scholar] [CrossRef] [Green Version]
- Kent, J.A.; Patel, V.; Varela, N.A. Gender Disparities in Health Care. Mt. Sinai J. Med. A J. Transl. Pers. Med. 2012, 79, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Holdcroft, A. Gender bias in research: How does it affect evidence based medicine? J. R. Soc. Med. 2007, 100, 2–3. [Google Scholar] [CrossRef] [PubMed]
- Thresia, C.U.; Katia, S.M. Gender bias in health research: Implications for women’s health in Kerala (India) and Sri Lanka. Crit. Public Health 2011, 21, 327–337. [Google Scholar] [CrossRef]
- Latinas Emerge as a Powerful Force in the U.S. Job Market. Los Angeles Times. 2019. Available online: https://www.latimes.com/business/story/2019-12-31/latinas-emerge-as-a-powerful-force-in-the-u-s-job-market. (accessed on 11 May 2021).
- Hallock, J.; Ariel, G.R.S.; Michael, F. In Search of Safety, Growing Numbers of Women Flee Central America; Migration Policy Institute: Washington, DC, USA, 2018. [Google Scholar]
- Desai, S.; Samari, G. COVID-19 and Immigrants’ Access to Sexual and Reproductive Health Services in the United States. Perspect. Sex. Reprod. Health 2020, 52, 69–73. [Google Scholar] [CrossRef]
- Watson, L.B.; Deblaere, C.; Langrehr, K.J.; Zelaya, D.G.; Flores, M.J. The influence of multiple oppressions on women of color’s experiences with insidious trauma. J. Couns. Psychol. 2016, 63, 656–667. [Google Scholar] [CrossRef]
- Berchick, E. Most Uninsured Were Working-Age Adults; U.S. Census Bureau: Suitland-Silver, MD, USA, 2018.
- Office of Disease Prevention and Health Promotion (ODPHP). Disparities. Available online: https://www.healthypeople.gov/2020/about/foundation-health-measures/Disparities (accessed on 2 June 2021).
- Guadamuz, J.S.; Kapoor, K.; Lazo, M.; Eleazar, A.; Yahya, T.; Kanaya, A.M.; Cainzos-Achirica, M.; Bilal, U. Understanding Immigration as a Social Determinant of Health: Cardiovascular Disease in Hispanics/Latinos and South Asians in the United States. Curr. Atheroscler. Rep. 2021, 23, 25. [Google Scholar] [CrossRef]
- Williams, D.R.; Selina, A.M. Racism and health I: Pathways and scientific evidence. Am. Behav. Sci. 2013, 57, 1152–1173. [Google Scholar] [CrossRef]
- In U.S., 14% With Likely COVID-19 to Avoid Care Due to Cost. Gallup. Available online: https://news.gallup.com/poll/309224/avoid-care-likely-covid-due-cost.aspx (accessed on 28 April 2020).
- Vargas, E.D.; Juárez, M.; Sanchez, G.R.; Livaudais, M. Latinos’ connections to immigrants: How knowing a deportee impacts Latino health. J. Ethn. Migr. Stud. 2019, 45, 2971–2988. [Google Scholar] [CrossRef]
- Gramlich, J. How Border Apprehensions, ICE Arrests and Deportations have Changed under Trump; Pew Research Center: Washington, DC, USA, 2020. [Google Scholar]
- Gómez-Aguiñaga, B. Stepping into the Vacuum: State and Cities Act. on Immigration, but Do Restrictions Work? Migration Information Source: Washington, DC, USA, 2016. [Google Scholar]
- Pedraza, F.I.; Nichols, V.C.; Lebrón, A.M.W. Cautious Citizenship: The Deterring Effect of Immigration Issue Salience on Health Care Use and Bureaucratic Interactions among Latino US Citizens. J. Health Pol. Policy Law 2017, 42, 925–960. [Google Scholar] [CrossRef] [Green Version]
- Vargas, E.D.; Benitez, V.L. Latino parents’ links to deportees are associated with developmental disorders in their children. J. Community Psychol. 2019, 47, 1151–1168. [Google Scholar] [CrossRef]
- Ross, E.J.; Merton, R.K. Social Theory and Social Structure. Am. Cathol. Sociol. Rev. 1958, 19, 159. [Google Scholar] [CrossRef]
- Pearlin, L.I.; Schieman, S.; Fazio, E.M.; Meersman, S.C. Stress, Health, and the Life Course: Some Conceptual Perspectives. J. Health Soc. Behav. 2005, 46, 205–219. [Google Scholar] [CrossRef] [PubMed]
- Fothergill, A.; Maestas, E.G.M.; Darlington, J.D. Race, Ethnicity and Disasters in the United States: A Review of the Literature. Disasters 1999, 23, 156–173. [Google Scholar] [CrossRef]
- Noh, S.; Kaspar, V.; Wickrama, K.A.S. Overt and Subtle Racial Discrimination and Mental Health: Preliminary Findings for Korean Immigrants. Am. J. Public Health 2007, 97, 1269–1274. [Google Scholar] [CrossRef]
- Bailey, Z.D.; Krieger, N.; Agénor, M.; Graves, J.; Linos, N.; Bassett, M.T. Structural racism and health inequities in the USA: Evidence and interventions. Lancet 2017, 389, 1453–1463. [Google Scholar] [CrossRef]
- Williams Institute. LGBT Latino/a Individuals and Latino/a Same-Sex Couples. UCLA School of Law Williams Institute, October 2013. Available online: https://williamsinstitute.law.ucla.edu/publications/lgbt-latinx-indv-and-ss-couples/ (accessed on 11 May 2021).
- CDC (Centers for Disease Control and Prevention). COVID Data Tracker 2021. Available online: https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm (accessed on 5 May 2021).
- Joshi, A.; Kale, S.; Chandel, S.; Pal, D.K. Likert Scale: Explored and Explained. Br. J. Appl. Sci. Technol. 2015, 7, 396–403. [Google Scholar] [CrossRef]
- López, N.; Gadsden, V.L.; University of Pennsylvania; University of New Mexico. Health Inequities, Social Determinants, and Intersectionality. NAM Perspect. 2016, 6. [Google Scholar] [CrossRef]
- López, N. Chapter Contextualizing Lived Race-Gender and the Racialized-Gendered Social Determinants of Health. In Mapping Race; Rutgers University Press: New Brunswick, NJ, USA, 2019; pp. 179–212. [Google Scholar]
- Perreira, K.M.; Pedroza, J.M. Policies of Exclusion: Implications for the Health of Immigrants and Their Children. Annu. Rev. Public Health 2019, 40, 147–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinedo, M. The impact of deportation policies on the substance using behaviors of US-citizen Latinos. Int. J. Drug Policy 2020, 75, 102605. [Google Scholar] [CrossRef] [PubMed]
- Frey, W.H. Diversity Explosion: How New Racial Demographics Are Remaking America; Brookings Institution Press: Washington, DC, USA, 2018. [Google Scholar]
- Crenshaw, K. Mapping the Margins: Intersectionality, Identity Politics, and Violence against Women of Color. Stanf. Law Rev. 1991, 43, 1241. [Google Scholar] [CrossRef]
- Evans, C.R.; Williams, D.R.; Onnela, J.-P.; Subramanian, S. A multilevel approach to modeling health inequalities at the intersection of multiple social identities. Soc. Sci. Med. 2018, 203, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Perez-Truglia, R. Applied Econometrics Using Stata; Manual Department of Economics, Harvard University: Cambridge, MA, USA, 2009. [Google Scholar]
- Long, J.S.; Freese, J. Regression Models for Categorical Dependent Variables using Stata; Stata Press: Lakeway Drive College Station, TX, USA, 2006; Volume 7. [Google Scholar]



| Variable | Observations | Mean | Std. Dev. | Min–Max |
|---|---|---|---|---|
| Mental health | 1202 | 2.433 | 1.581 | 0–4 |
| Female | 1200 | 0.520 | 0.500 | 0–1 |
| Knows COVID-19 ill | 1200 | 0.253 | 0.435 | 0–1 |
| Knows undocumented immigrant | 1200 | 0.462 | 0.499 | 0–1 |
| US-born | 1200 | 0.600 | 0.490 | 0–1 |
| Education | 1200 | 3.003 | 1.539 | 1–6 |
| Age | 1083 | 2.222 | 1.012 | 1–4 |
| Married | 1200 | 0.428 | 0.495 | 0–1 |
| Income | 1196 | 2.834 | 1.803 | 1–7 |
| Uninsured | 1200 | 0.716 | 0.451 | 0–1 |
| Mexican ancestry | 1202 | 0.408 | 0.492 | 0–1 |
| Spanish survey | 1200 | 0.414 | 0.493 | 0–1 |
| β | Odds | |
|---|---|---|
| Variables | (Standard Errors) | Ratio |
| Female | 0.396 ** | 1.486 ** |
| (0.114) | ||
| Knows COVID-19 ill | 0.224 * | 1.250 * |
| (0.135) | ||
| Knows undocumented immigrant | 0.518 ** | 1.679 ** |
| (0.118) | ||
| US-born | 0.229 | 1.257 |
| (0.142) | ||
| Education | 0.099 ** | 1.104 ** |
| (0.038) | ||
| Age category | −0.197 ** | 0.821 ** |
| (0.061) | ||
| Married | 0.037 | 1.038 |
| (0.124) | ||
| Income | −0.095 ** | 0.910 ** |
| (0.034) | ||
| Uninsured | -0.151 | 0.860 |
| (0.129) | ||
| Mexican ancestry | −0.059 | 0.943 |
| (0.119) | ||
| Spanish survey | −0.251 * | 0.778 * |
| (0.143) | ||
| Observations | 1079 | 1079 |
| β | Odds | |
|---|---|---|
| Variables | (Standard Errors) | Ratio |
| Female | 0.381 ** | 1.464 ** |
| (0.168) | ||
| Knows COVID-19 ill | 0.074 | 1.077 |
| (0.287) | ||
| Knows undocumented immigrant | 0.503 *** | 1.653 *** |
| (0.193) | ||
| Female x Knows COVID-19 ill x | 0.219 | 1.244 |
| Knows undocumented immigrant | (0.531) | |
| Female x Knows COVID-19 ill | 0.077 | 1.081 |
| (0.386) | ||
| Female x Knows undocumented | −0.077 | 0.926 |
| immigrant | (0.265) | |
| Knows COVID-19 ill x Knows | 0.103 | 1.108 |
| undocumented immigrant | (0.383) | |
| US-born | 0.234 * | 1.264 * |
| (0.142) | ||
| Education | 0.100 *** | 1.105 *** |
| (0.038) | ||
| Age category | −0.200 *** | 0.819 *** |
| (0.062) | ||
| Married | 0.041 | 1.042 |
| (0.124) | ||
| Income | −0.097 *** | 0.908 *** |
| (0.034) | ||
| Uninsured | −0.154 | 0.857 |
| (0.129) | ||
| Mexican ancestry | −0.054 | 0.947 |
| (0.119) | ||
| Spanish survey | −0.246 * | 0.782 * |
| (0.143) | ||
| Observations | 1079 | 1079 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gomez-Aguinaga, B.; Dominguez, M.S.; Manzano, S. Immigration and Gender as Social Determinants of Mental Health during the COVID-19 Outbreak: The Case of US Latina/os. Int. J. Environ. Res. Public Health 2021, 18, 6065. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116065
Gomez-Aguinaga B, Dominguez MS, Manzano S. Immigration and Gender as Social Determinants of Mental Health during the COVID-19 Outbreak: The Case of US Latina/os. International Journal of Environmental Research and Public Health. 2021; 18(11):6065. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116065
Chicago/Turabian StyleGomez-Aguinaga, Barbara, Melanie Sayuri Dominguez, and Sylvia Manzano. 2021. "Immigration and Gender as Social Determinants of Mental Health during the COVID-19 Outbreak: The Case of US Latina/os" International Journal of Environmental Research and Public Health 18, no. 11: 6065. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116065