
The COVID-19 Pandemic Situation in Malaysia: Lessons Learned from the Perspective of Population Density

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. COVID-19 Status in Malaysia
3. COVID-19 and Population Density
4. Methods
4.1. Data Collection
4.2. COVID-19 Cases
4.3. Population Density
4.4. Data Analysis
5. Results and Findings
5.1. Spatio-Temporal Spread of COVID-19
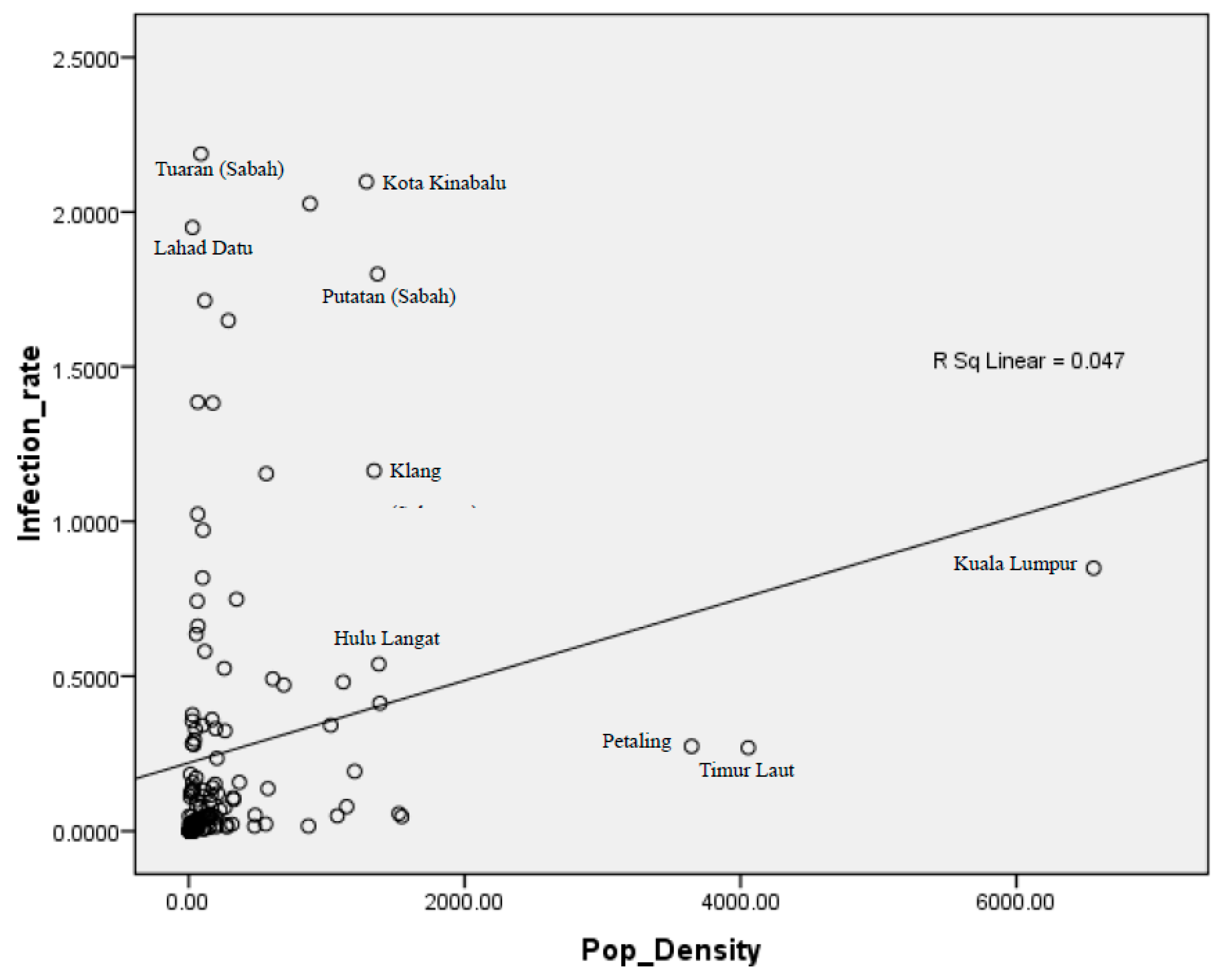
5.2. Population Density and COVID-19 Cases in Malaysia
6. Discussion: Lessons Learned and Recommendations
6.1. Self-Contained Urban Planning
6.2. Managing Crowding Risk in Dense Areas
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers for Disease Control and Prevention About the Variants. Available online: https://www.cdc.gov/coronavirus/2019-ncov/transmission/variant.html (accessed on 27 March 2021).
- Robertson, S. New SARS-CoV-2 Variant in France Appears Undetectable by PCR. Available online: https://www.news-medical.net/news/20210317/New-SARS-CoV-2-variant-in-France-appears-undetectable-by-PCR.aspx (accessed on 27 March 2021).
- Dyer, O. Covid-19: Moderna and Pfizer Vaccines Prevent Infections as Well as Symptoms, CDC Study Finds. BMJ 2021, n888. [Google Scholar] [CrossRef]
- Zhu, Z.; Lian, X.; Su, X.; Wu, W.; Marraro, G.A.; Zeng, Y. From SARS and MERS to COVID-19: A Brief Summary and Comparison of Severe Acute Respiratory Infections Caused by Three Highly Pathogenic Human Coronaviruses. Respir. Res. 2020, 21, 224. [Google Scholar] [CrossRef]
- Baj, J.; Karakuła-Juchnowicz, H.; Teresiński, G.; Buszewicz, G.; Ciesielka, M.; Sitarz, E.; Forma, A.; Karakuła, K.; Flieger, W.; Portincasa, P.; et al. COVID-19: Specific and Non-Specific Clinical Manifestations and Symptoms: The Current State of Knowledge. J. Clin. Med. 2020, 9, 1753. [Google Scholar] [CrossRef]
- Morawska, L.; Cao, J. Airborne Transmission of SARS-CoV-2: The World Should Face the Reality. Environ. Int. 2020, 139, 105730. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.F.-W.; Yuan, S.; Kok, K.-H.; To, K.K.-W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.-Y.; Poon, R.W.-S.; et al. A Familial Cluster of Pneumonia Associated with the 2019 Novel Coronavirus Indicating Person-to-Person Transmission: A Study of a Family Cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- WebMD How Long Does the Coronavirus Live on Surfaces? Available online: https://www.webmd.com/lung/how-long-covid-19-lives-on-surfaces#:~:text=Still%2C%20it%20is%20possible%20(though,mouth%2C%20nose%2C%20or%20eyes.&text=The%20coronavirus%20can%20live%20for,surfaces%20like%20countertops%20and%20doorknobs (accessed on 27 March 2021).
- Rampal, L.; Liew, B.S. Malaysia’s Third COVID-19 Wave—A Paradigm Shift Required—Third-COVID-19-Wave.Pdf. Med. J. Malays. 2021, 76, 1–4. [Google Scholar]
- The Star. CGS-CIMB Equities Research Daily Economic Losses from MCO around RM750m, Says CGS-CIMB Research. Available online: https://www.thestar.com.my/business/business-news/2021/01/12/daily-economic-losses-from-mco-around-rm750m-cgs-cimb-research-says (accessed on 27 March 2021).
- Hamidi, S.; Sabouri, S.; Ewing, R. Does Density Aggravate the COVID-19 Pandemic? Early Findings and Lessons for Planners. J. Am. Plan. Assoc. 2020, 86, 495–509. [Google Scholar] [CrossRef]
- Dong, E.; Du, H.; Gardner, L. An Interactive Web-Based Dashboard to Track COVID-19 in Real Time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Ministry of Health Malaysia Kemaskini Negeri COVID-19 di Malaysia Sehingga 28 Mac 2021. Available online: http://covid-19.moh.gov.my/terkini-negeri/2021/03/kemaskini-negeri-covid-19-di-malaysia-sehingga-28032021 (accessed on 28 March 2021).
- Wong, D.W.S.; Li, Y. Spreading of COVID-19: Density Matters. PLoS ONE 2020, 15, e0242398. [Google Scholar] [CrossRef]
- Almagro, M.; Orane-Hutchinson, A. The Determinants of the Differential Exposure to COVID-19 in New York City and Their Evolution over Time; Social Science Research Network: Rochester, NY, USA, 2020; Volume 17, pp. 1–16. [Google Scholar] [CrossRef]
- Wheaton, W.C.; Kinsella Thompson, A. The Geography of COVID-19 Growth in the US: Counties and Metropolitan Areas. SSRN J. 2020. [Google Scholar] [CrossRef]
- Bhadra, A.; Mukherjee, A.; Sarkar, K. Impact of Population Density on Covid-19 Infected and Mortality Rate in India. Model. Earth Syst. Environ. 2021, 7, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Fang, W.; Wahba, S. Urban Density Is Not an Enemy in the Coronavirus Fight: Evidence from China. Available online: https://blogs.worldbank.org/sustainablecities/urban-density-not-enemy-coronavirus-fight-evidence-china (accessed on 20 March 2021).
- Carozzi, F.; Provenzano, S.; Roth, S. Urban Density and COVID-19; IZA Discussion Paper No. 13440; Institute of Labor Economics (IZA): Bonn, Germany, 2020; pp. 1–27. [Google Scholar]
- Department of Statistics Malaysia Population Distribution and Basic Demographic Characteristic Report. 2010. Available online: https://www.dosm.gov.my/v1/index.php?r=column/ctheme&menu_id=L0pheU43NWJwRWVSZklWdzQ4TlhUUT09&bul_id=MDMxdHZjWTk1SjFzTzNkRXYzcVZjdz09 (accessed on 20 March 2021).
- Romanova, E. Increase in Population Density and Aggravation of Social and Psychological Problems in Areas with High-Rise Construction. E3S Web Conf. 2018, 33, 03061. [Google Scholar] [CrossRef]
- Batumalai, K. 82% Of Malaysia’s Active Covid Clusters Above 5% Positivity Rate. Available online: https://codeblue.galencentre.org/2020/12/03/82-of-malaysias-active-covid-clusters-above-5-positivity-rate/ (accessed on 27 March 2021).
- The Star. Workplace Infections Top List. Available online: https://www.thestar.com.my/news/nation/2021/03/28/workplace-infections-top-list (accessed on 28 April 2021).
- Rocklöv, J.; Sjödin, H.; Wilder-Smith, A. COVID-19 Outbreak on the Diamond Princess Cruise Ship: Estimating the Epidemic Potential and Effectiveness of Public Health Countermeasures. J. Travel Med. 2020, 27, taaa030. [Google Scholar] [CrossRef] [Green Version]
- Hamzah, H.; Abdullah, S.A. Dispute Resolution of Statified Residential Properties: The Strata Management Tribunal of Malaysia. In Proceedings of the Pacific Rim Regional Meeting of the International Academic Association on Planning, Law, and Property Rights, Taoyuan City, Taiwan, 16 April 2018. [Google Scholar]
- Subbaraman, N. Why Daily Death Tolls Have Become Unusually Important in Understanding the Coronavirus Pandemic. Nature 2020. [Google Scholar] [CrossRef]
- CRPC MOH Kes COVID-19 di Malaysia. Available online: http://statsgen.cloud/covid-19 (accessed on 4 April 2021).
- Chen, P.Z.; Bobrovitz, N.; Premji, Z.; Koopmans, M.; Fisman, D.N.; Gu, F.X. Heterogeneity in transmissibility and shedding SARS-CoV-2 via droplets and aerosols. Elife 2021, 10, e65774. [Google Scholar] [CrossRef] [PubMed]
- Pollock, A.M.; Lancaster, J. Asymptomatic Transmission of Covid-19. BMJ 2020, m4851. [Google Scholar] [CrossRef]
- Buitrago-Garcia, D.; Egli-Gany, D.; Counotte, M.J.; Hossmann, S.; Imeri, H.; Ipekci, A.M.; Salanti, G.; Low, N. Occurrence and Transmission Potential of Asymptomatic and Presymptomatic SARS-CoV-2 Infections: A Living Systematic Review and Meta-Analysis. PLoS Med. 2020, 17, e1003346. [Google Scholar] [CrossRef] [PubMed]
- The Malaysian Insight. Kuching Woman Returning from Italy Brings Death, Despair. Available online: https://www.themalaysianinsight.com/s/232488 (accessed on 15 April 2021).
- Wang, B.; Li, R.; Lu, Z.; Huang, Y. Does Comorbidity Increase the Risk of Patients with COVID-19: Evidence from Meta-Analysis. Aging 2020, 12, 6049–6057. [Google Scholar] [CrossRef]
- Oyelade, T.; Alqahtani, J.; Canciani, G. Prognosis of COVID-19 in Patients with Liver and Kidney Diseases: An Early Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2020, 5, 80. [Google Scholar] [CrossRef]
- Ling, G.H.T.; Ho, M.C. Effects of the coronavirus (COVID-19) pandemic on social behaviours: From a social dilemma perspective. Technium Soc. Sci. J 2020, 7, 312. [Google Scholar] [CrossRef]
- Ling, G.H.T.; Md Suhud, N.A.b.; Leng, P.C.; Yeo, L.B.; Cheng, C.T.; Ahmad, M.H.H.; Ak Matusin, A.M.R. Factors Influencing Asia-Pacific Countries’ Success Level in Curbing COVID-19: A Review Using a Social–Ecological System (SES) Framework. Int. J. Environ. Res. Public Health 2021, 18, 1704. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| 14-Days Period | Districts in Penang | ||||
|---|---|---|---|---|---|
| Seberang Perai Tengah | Seberang Perai Utara | Seberang Perai Selatan | Timur Laut | Barat Daya | |
| Year 2010 Population Density (Person per sq km): 1524 | Year 2010 Population Density (Person per sq km): 1077 | Year 2010 Population Density (Person per sq km): 689 | Year 2010 Population Density (Person per sq km): 4056 | Year 2010 Population Density (person per sq Km): 1120 | |
| 18 December–31 December 2020 | 42 | 19 | 65 | 245 | 252 |
| 4 December–17 December 2020 | 39 | 31 | 50 | 238 | 280 |
| 20 November–3 December 2020 | 31 | 26 | 43 | 160 | 245 |
| 6 November–19 November 2020 | 37 | 28 | 268 | 144 | 101 |
| 23 October–5 November 2020 | 14 | 3 | 234 | 137 | 51 |
| 9 October–22 October 2020 | 1 | 8 | 115 | 402 | 1 |
| 25 September–8 October 2020 | 0 | 2 | 0 | 8 | 0 |
| 11 September–24 September 2020 | 0 | 0 | 0 | 3 | 1 |
| 28 August–10 September 2020 | 0 | 0 | 0 | 2 | 0 |
| 14 August–27 August 2020 | 0 | 1 | 0 | 6 | 4 |
| 31 July–13 August 2020 | 2 | 0 | 0 | 0 | 0 |
| 17 July–30 July 2020 | 0 | 0 | 0 | 0 | 0 |
| 3 July–16 July 2020 | 0 | 0 | 0 | 0 | 0 |
| 19 June–2 July 2020 | 0 | 0 | 0 | 0 | 0 |
| 5 June–18 June 2020 | 0 | 0 | 0 | 0 | 0 |
| 22 May–4 June 2020 | 0 | 0 | 0 | 0 | 0 |
| 8 May–21 May 2020 | 0 | 0 | 0 | 0 | 0 |
| 25 January–7 May 2020 * | 40 | 25 | 11 | 32 | 13 |
| Total | 206 | 143 | 786 | 1377 | 948 |
| 14-Days Period | Districts in Perak | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Batang Padang | Manjung | Kinta | Kerian | Kuala Kangsar | Larut dan Matang | Hilir Perak | Ulu Perak | Perak Tengah | Kampar | |
| Year 2010 Population Density (Person per sq km): 64 | Year 2010 Population Density (Person per sq km): 204 | Year 2010 Population Density (Person per sq km): 574 | Year 2010 Population Density (Person per sq km): 192 | Year 2010 Population Density (Person per sq km): 61 | Year 2010 Population Density (Person per sq km): 155 | Year 2010 Population Density (Person per sq km): 116 | Year 2010 Population Density (Person per sq km): 14 | Year 2010 Population Density (Person per sq km): 78 | Year 2010 Population Density (person per sq km): 144 | |
| 18 December–31 December 2020 | 18 | 2 | 129 | 13 | 1 | 59 | 189 | 0 | 16 | 0 |
| 4 December–17 December 2020 | 17 | 2 | 122 | 2 | 5 | 6 | 656 | 0 | 2 | 1 |
| 20 November–3 December 2020 | 3 | 1 | 534 | 3 | 15 | 9 | 235 | 4 | 1 | 39 |
| 6 November–19 November 2020 | 1 | 2 | 113 | 4 | 129 | 121 | 27 | 0 | 0 | 1 |
| 23 October–5 November 2020 | 10 | 2 | 20 | 13 | 2 | 17 | 0 | 2 | 0 | 0 |
| 9 October–22 October 2020 | 7 | 16 | 9 | 24 | 0 | 76 | 4 | 4 | 2 | 0 |
| 25 September–8 October 2020 | 0 | 0 | 3 | 0 | 0 | 9 | 0 | 0 | 1 | 0 |
| 11 September–24 September 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 28 August–10 September 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 14 August–27 August 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 31 July–13 August 2020 | 0 | 0 | 2 | 3 | 0 | 0 | 0 | 0 | 0 | 0 |
| 17 July–30 July 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 3 July–16 July 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 19 June–2 July 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 5 June–18 June 2020 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 22 May–4 June 2020 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 8 May–21 May 2020 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 25 January–7 May 2020 * | 9 | 23 | 95 | 19 | 4 | 19 | 65 | 6 | 11 | 2 |
| Total | 65 | 50 | 1029 | 81 | 156 | 316 | 1176 | 16 | 33 | 43 |
| 14-Days Period | Districts in Sarawak | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Kuching | Bau | Lundu | Samarahan | Serian | Simunjan | Sri Aman | Lubok Antu | Betong | Saratok | |
| Year 2010 Population Density (Person per sq km): 321 | Year 2010 Population Density (Person per sq km): 60 | Year 2010 Population Density (Person per sq km): 18 | Year 2010 Population Density (Person per sq km): 210 | Year 2010 Population Density (Person per sq km): 44 | Year 2010 Population Density (Person per sq km): 17 | Year 2010 Population Density (Person per sq km): 28 | Year 2010 Population Density (Person per sq km): 9 | Year 2010 Population Density (Person per sq km): 24 | Year 2010 Population Density (Person per sq km): 27 | |
| 18 December–31 December 2020 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 4 December–17 December 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 20 November–3 December 2020 | 3 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| 6 November–19 November 2020 | 97 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 23 October–5 November 2020 | 124 | 0 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 9 October–22 October 2020 | 12 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 |
| 25 September–8 October 2020 | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 11 September–24 September 2020 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 28 August–10 September 2020 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 14 August–27 August 2020 | 4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 31 July–13 August 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 17 July–30 July 2020 | 51 | 0 | 1 | 4 | 0 | 0 | 0 | 0 | 0 | 0 |
| 3 July–16 July 2020 | 8 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 19 June–2 July 2020 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 5 June–18 June 2020 | 6 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| 22 May–4 June 2020 | 4 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 |
| 8 May–21 May 2020 | 3 | 0 | 0 | 0 | 3 | 0 | 0 | 0 | 0 | 0 |
| 25 January–7 May 2020 * | 325 | 5 | 1 | 98 | 17 | 7 | 3 | 0 | 16 | 0 |
| Total | 645 | 5 | 5 | 104 | 22 | 7 | 3 | 1 | 16 | 0 |
| 14-Days Period | Districts in Sarawak | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sarikei | Maradong | Daro | Julau | Sibu | Dalat | Mukah | Kanowit | Bintulu | Tatau | Kapit | |
| Year 2010 Population Density (Person per sq km): 57 | Year 2010 Population Density (Person per sq km): 40 | Year 2010 Population Density (Person per sq km): 15 | Year 2010 Population Density (Person per sq km): 9 | Year 2010 Population Density (Person per sq km): 108 | Year 2010 Population Density (Person per sq km): 20 | Year 2010 Population Density (Person per sq km): 16 | Year 2010 Population Density (Person per sq km): 13 | Year 2010 Population Density (Person per sq km): 25 | Year 2010 Population Density (Person per sq km): 6 | Year 2010 Population Density (Person per sq km): 4 | |
| 18 December–31 December 2020 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 |
| 4 December–17 December 2020 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| 20 November–3 December 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 6 November–19 November 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 23 October–5 November 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 9 October–22 October 2020 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 4 | 0 | 0 |
| 25 September–8 October 2020 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 1 | 0 | 0 |
| 11 September–24 September 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 28 August–10 September 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 14 August–27 August 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 |
| 31 July–13 August 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 17 July–30 July 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 3 July–16 July 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 19 June–2 July 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 3 | 0 | 0 |
| 5 June–18 June 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 5 | 0 | 0 |
| 22 May–4 June 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 8 May–21 May 2020 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| 25 January–7 May 2020 * | 6 | 0 | 0 | 0 | 6 | 0 | 1 | 0 | 12 | 0 | 0 |
| Total | 6 | 0 | 0 | 0 | 12 | 0 | 1 | 0 | 28 | 0 | 0 |
| 14-Days Period | Districts in Sarawak | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Song | Belaga | Miri | Marudi | Limbang | Lawas | Matu | Asajaya | Pakan | Selangau | |
| Year 2010 Population Density (Person per sq km): 5 | Year 2010 Population Density (Person per sq km): 2 | Year 2010 Population Density (Person per sq km): 62 | Year 2010 Population Density (Person per sq km): 3 | Year 2010 Population Density (Person per sq km): 12 | Year 2010 Population Density (Person per sq km): 10 | Year 2010 Population Density (Person per sq km): 11 | Year 2010 Population Density (Person per sq km): 103 | Year 2010 Population Density (Person per sq km): 16 | Year 2010 Population Density (Person per sq km): 6 | |
| 18 December–31 December 2020 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| 4 December–17 December 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 20 November–3 December 2020 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 6 November–19 November 2020 | 0 | 0 | 5 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| 23 October–5 November 2020 | 0 | 0 | 11 | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| 9 October–22 October 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 25 September–8 October 2020 | 0 | 0 | 0 | 0 | 0 | 3 | 0 | 0 | 0 | 0 |
| 11 September–24 September 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 28 August–10 September 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 14 August–27 August 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 31 July–13 August 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 17 July–30 July 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 3 July–16 July 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 19 June–2 July 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 5 June–18 June 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 22 May–4 June 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 8 May–21 May 2020 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 25 January–7 May 2020 * | 0 | 0 | 23 | 0 | 9 | 1 | 1 | 3 | 0 | 0 |
| Total | 0 | 0 | 40 | 0 | 10 | 6 | 1 | 3 | 0 | 0 |
| Correlations | |||
|---|---|---|---|
| Population Density | Cumulative Cases | Infection Rates | |
| Population Density | 1 | 0.644 ** (0.415) | 0.216 ** (0.047) |
| 0.000 | 0.005 | ||
| 143 | 143 | 143 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aw, S.B.; Teh, B.T.; Ling, G.H.T.; Leng, P.C.; Chan, W.H.; Ahmad, M.H. The COVID-19 Pandemic Situation in Malaysia: Lessons Learned from the Perspective of Population Density. Int. J. Environ. Res. Public Health 2021, 18, 6566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126566
Aw SB, Teh BT, Ling GHT, Leng PC, Chan WH, Ahmad MH. The COVID-19 Pandemic Situation in Malaysia: Lessons Learned from the Perspective of Population Density. International Journal of Environmental Research and Public Health. 2021; 18(12):6566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126566
Chicago/Turabian StyleAw, Siew Bee, Bor Tsong Teh, Gabriel Hoh Teck Ling, Pau Chung Leng, Weng Howe Chan, and Mohd Hamdan Ahmad. 2021. "The COVID-19 Pandemic Situation in Malaysia: Lessons Learned from the Perspective of Population Density" International Journal of Environmental Research and Public Health 18, no. 12: 6566. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126566