
Impact of the COVID-19 Pandemic on Patients Affected by Non-Communicable Diseases in Europe and in the USA

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
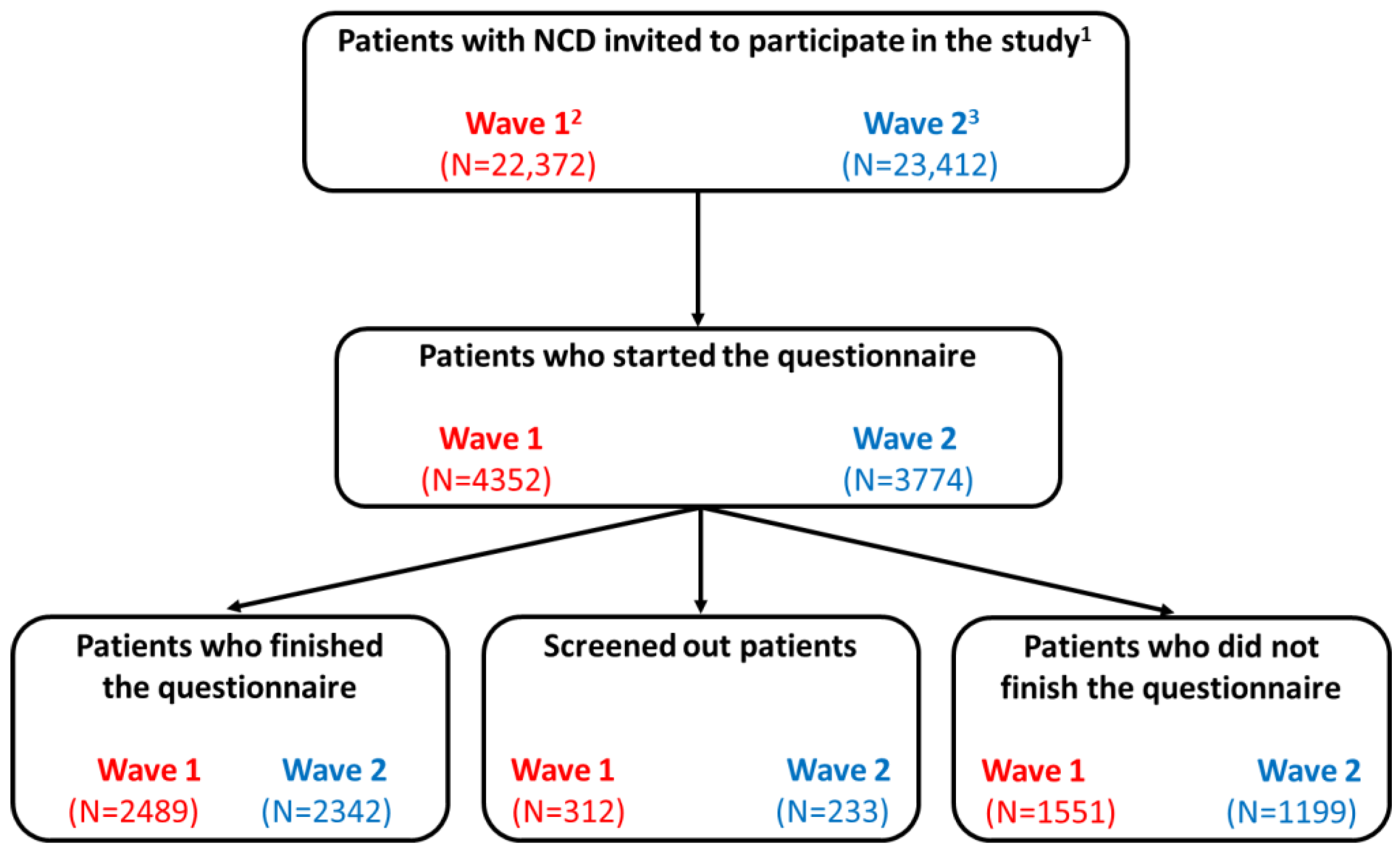
2.1. Study Design
2.2. Study Population
2.3. Ethical Considerations
2.4. Data Collection
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.1.1. Sociodemographic Profile
3.1.2. Clinical Characteristics
3.2. Impact of COVID-19 Pandemic on the Medical Condition of Patients with NCDs
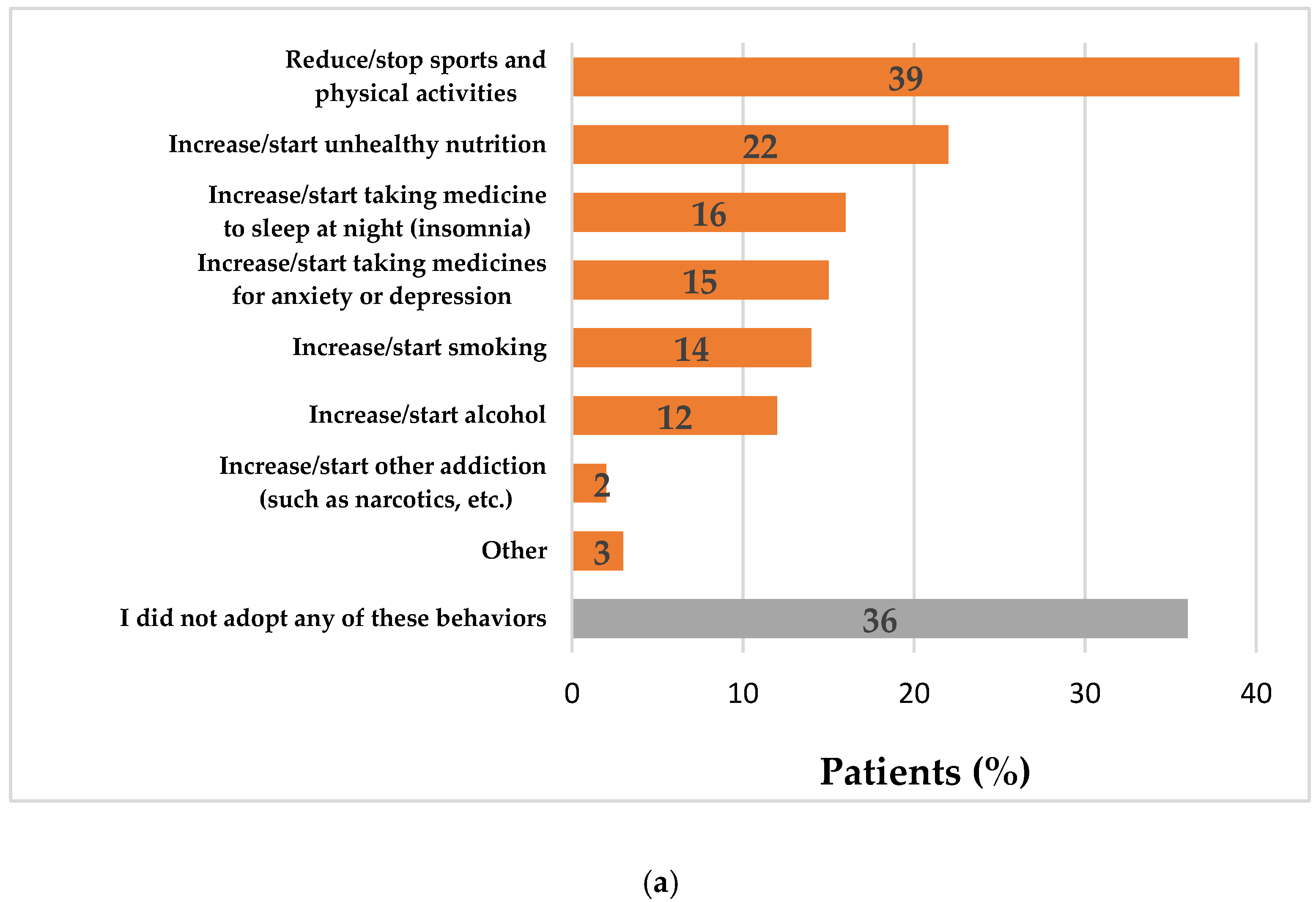
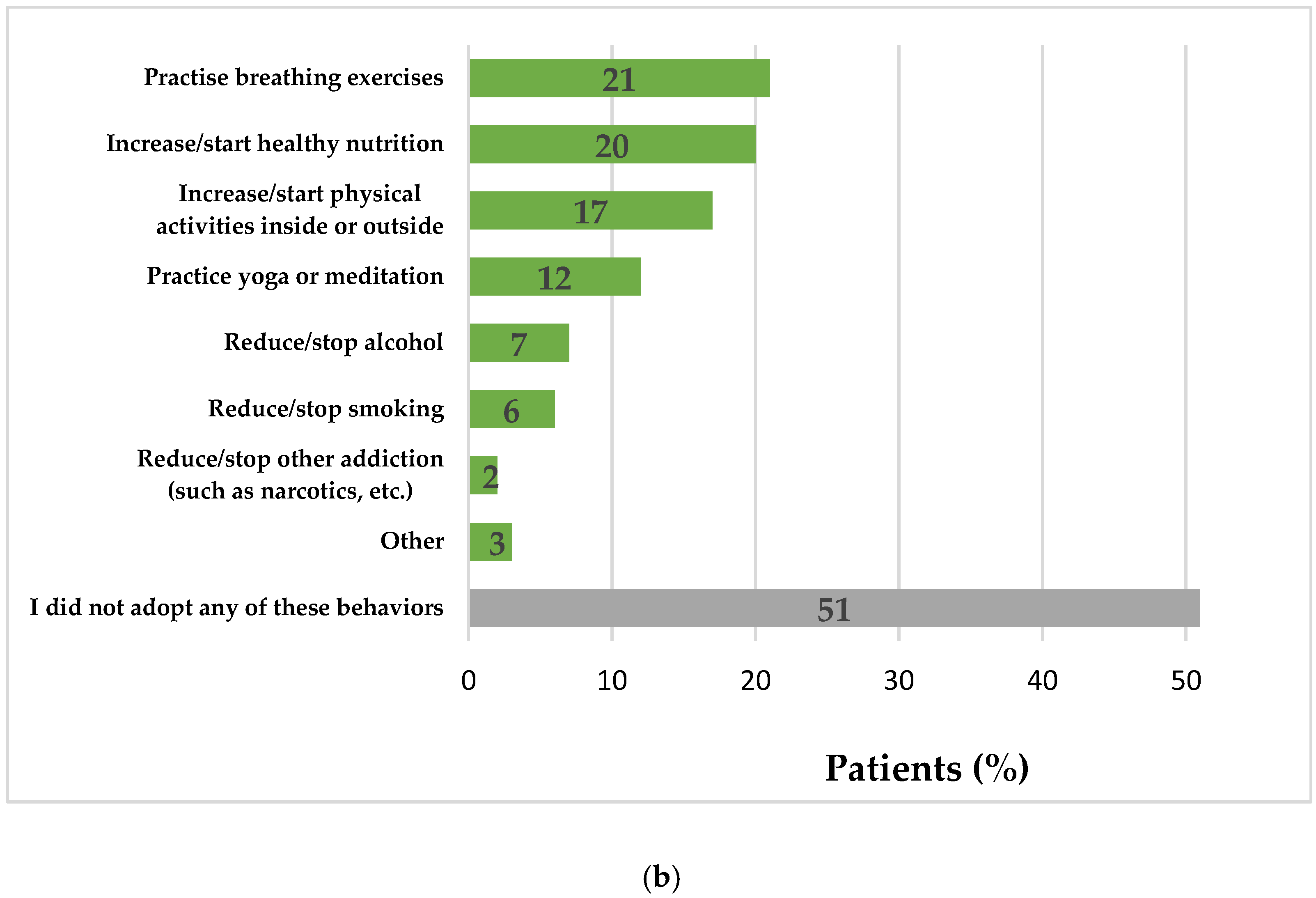
3.3. Impact of COVID-19 Pandemic on the Behaviors of Patients with NCDs
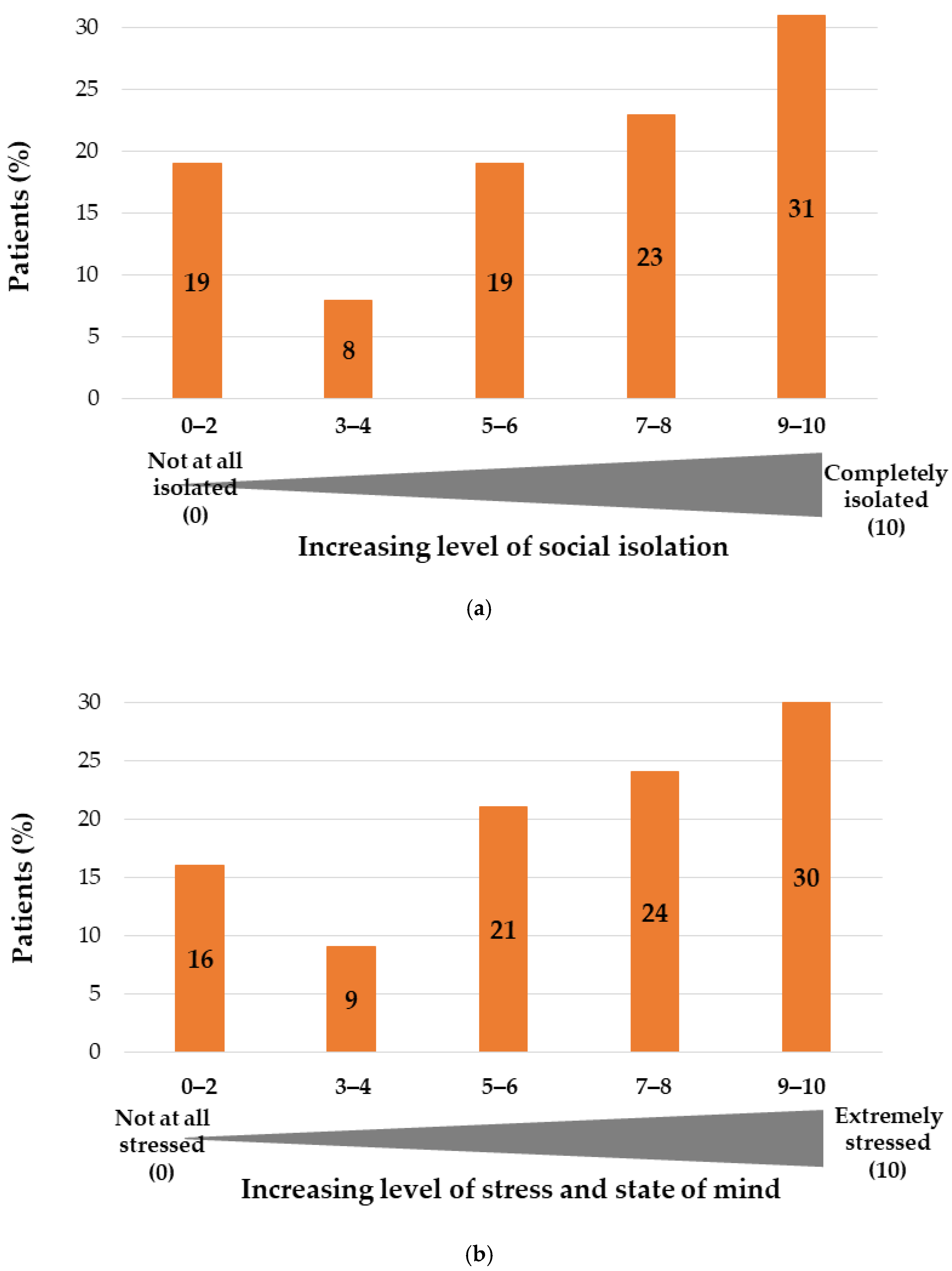
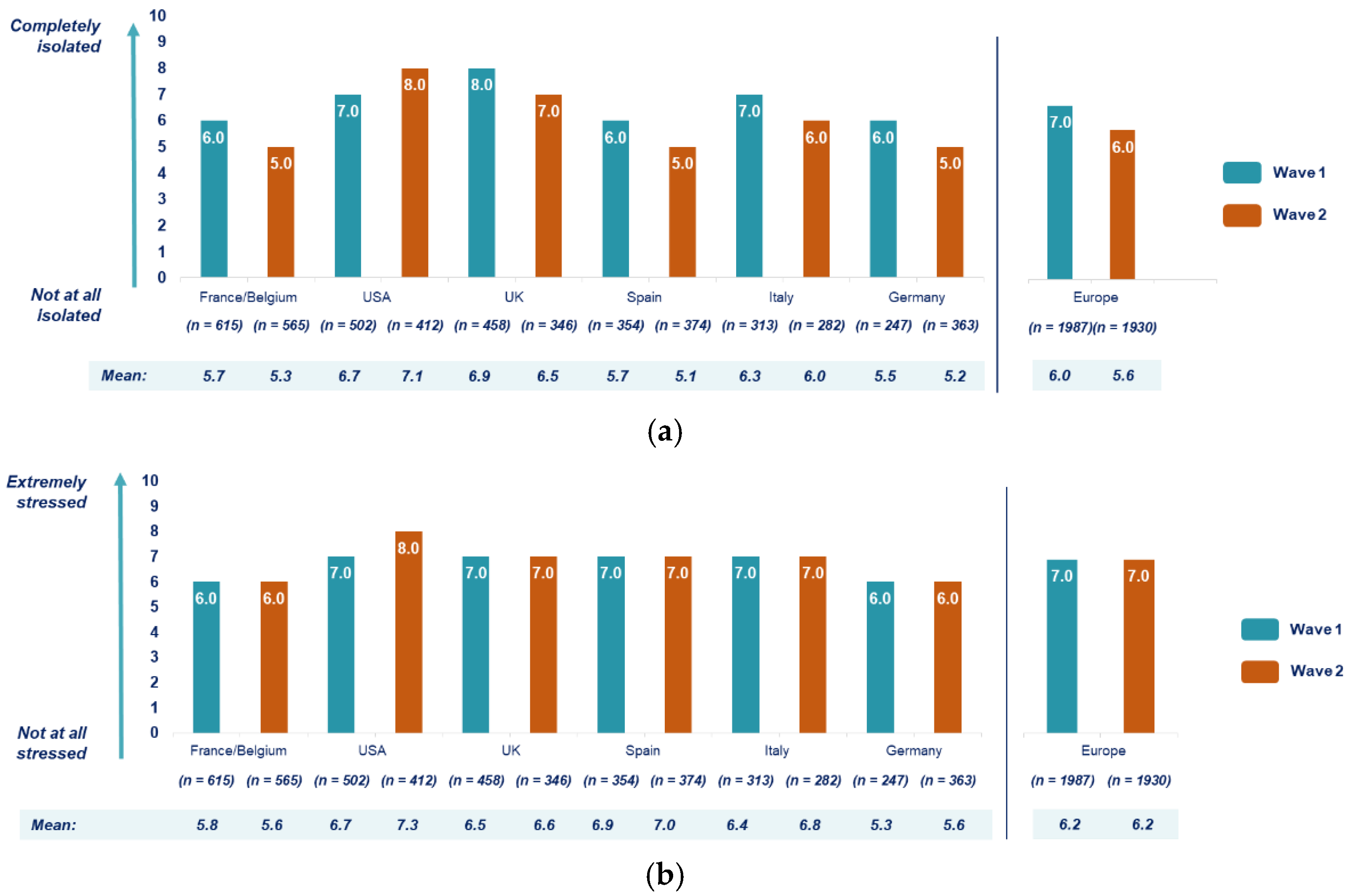
3.4. Impact of COVID-19 Pandemic on Mental Health of Patients with NCDs
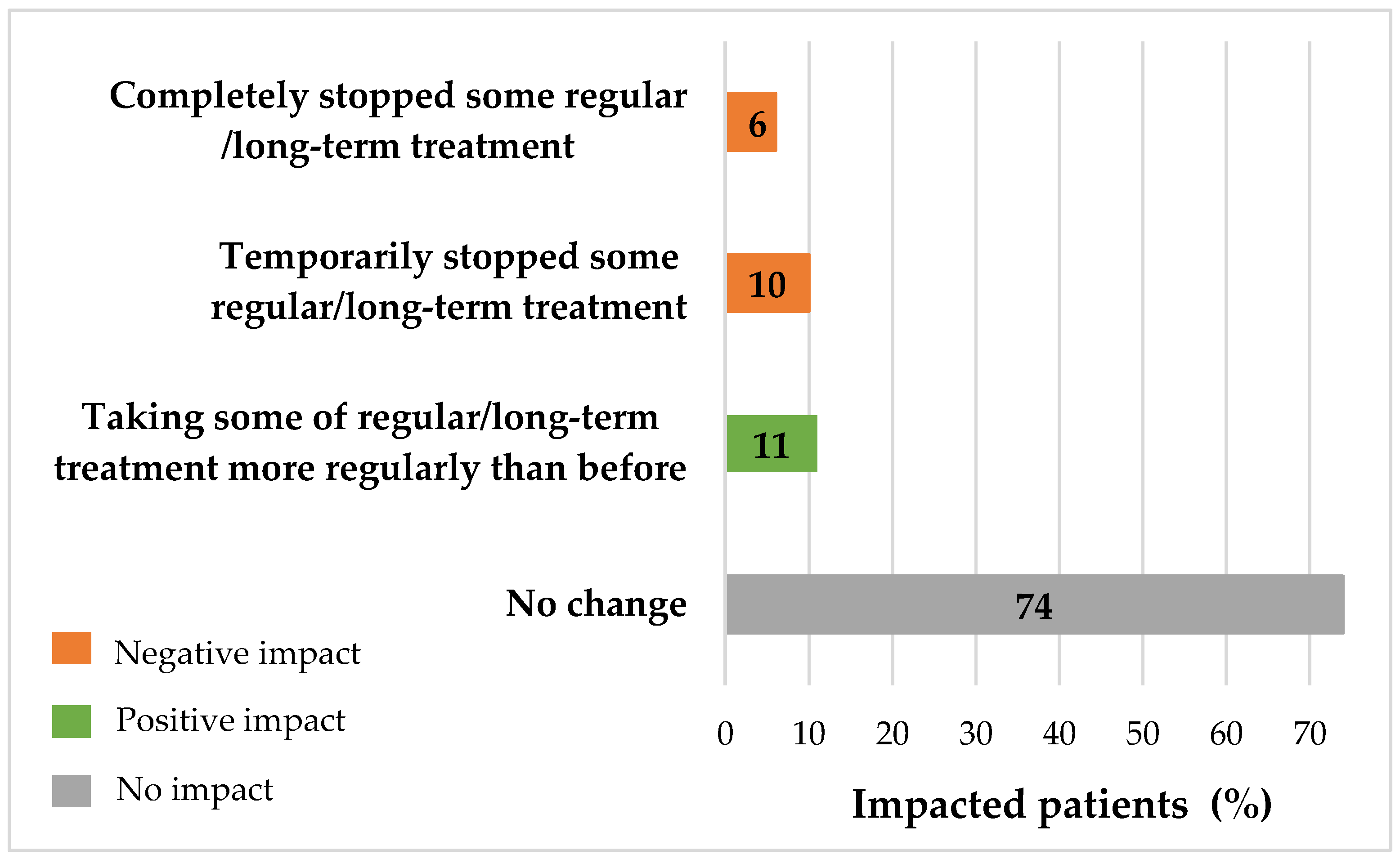
3.5. Impact of COVID-19 Pandemic on the Care Pathway of Patients with NCDs
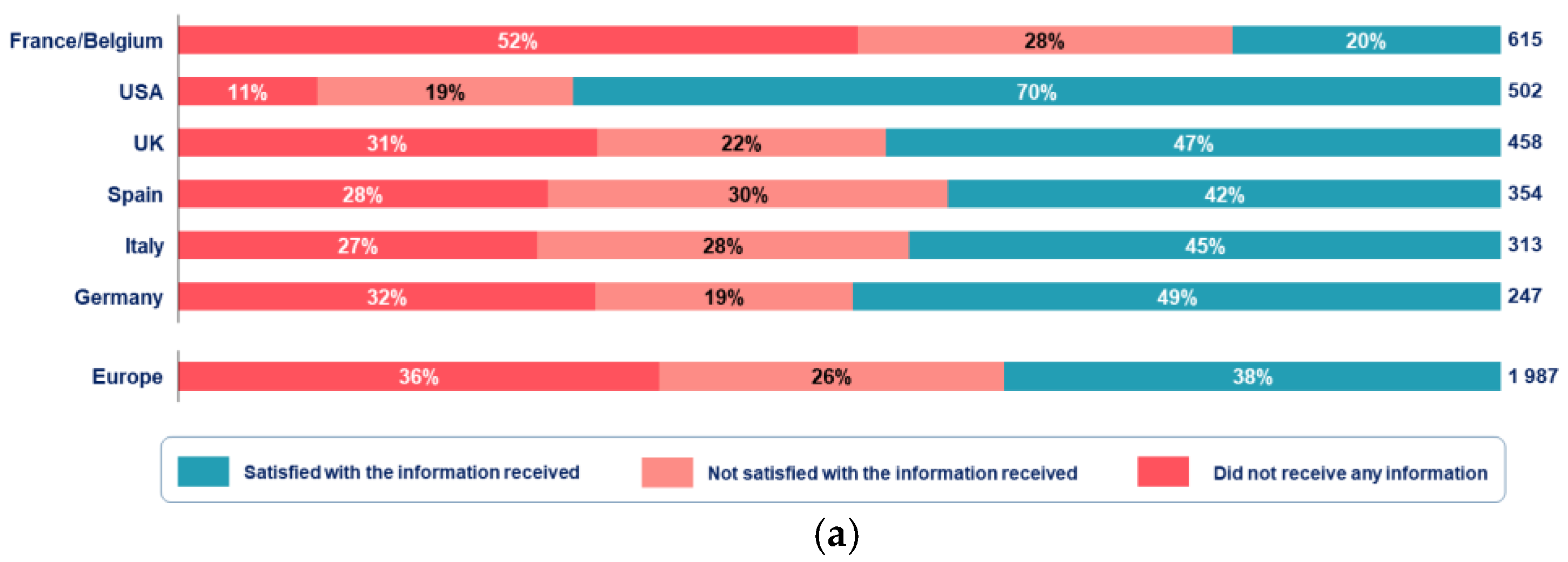
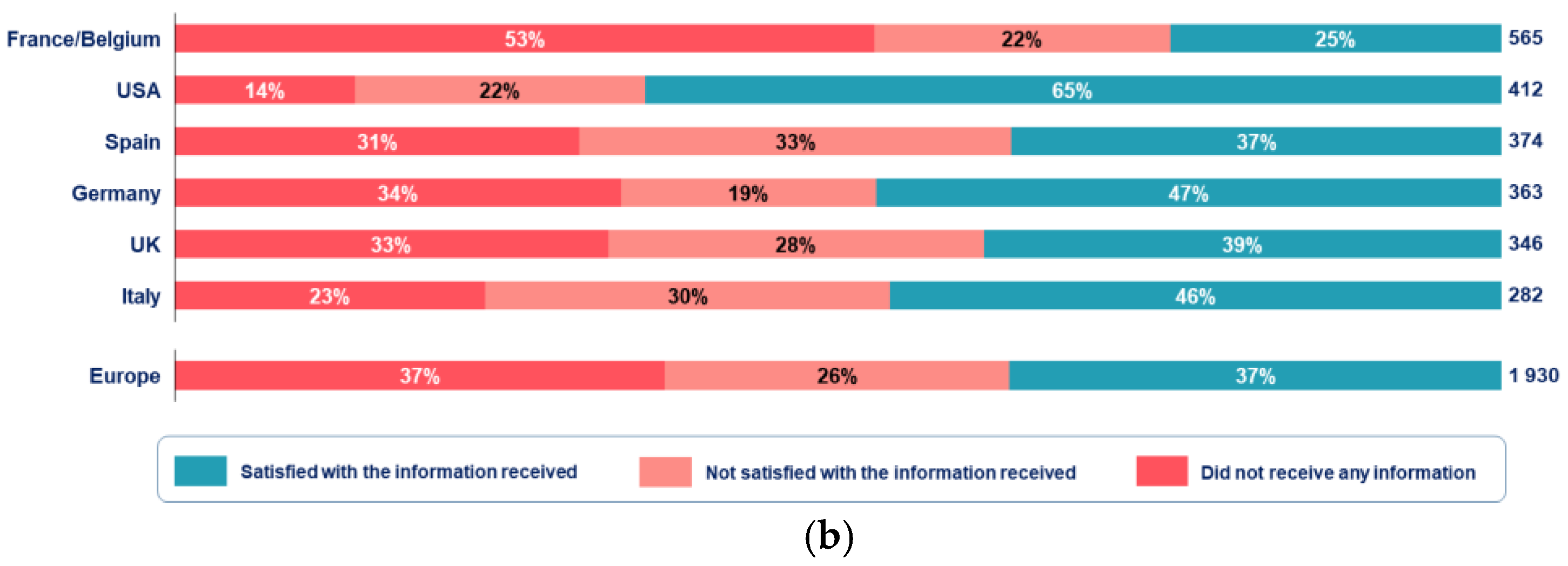
3.6. Access and Need for Disease-Specific Information
3.7. Impact of the Pandemic and Patients’ Need Depending on Patients’ Profile
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Noncommunicable Diseases Country Profiles 2018. Available online: https://www.who.int/nmh/publications/ncd-profiles-2018/en/ (accessed on 21 June 2021).
- Roser, M.; Ritchie, H. Burden of Disease. 2019. Available online: https://ourworldindata.org/burden-of-disease (accessed on 21 June 2021).
- White Paper: Leading the Conversation on Noncommunicable Diseases Worldwide: An Evidence-Based Review of Key Research and Strategies to Develop Sustainable Solutions; Upjoin: Kalamazoo, MI, USA, 2020; Available online: https://cdn.pfizer.com/pfizercom/Upjohn_NCD_White_Paper-24JAN2020.pdf (accessed on 21 June 2021).
- England, K.; Azzopardi-Muscat, N. Demographic trends and public health in Europe. Eur. J. Public Health 2017, 27 (Suppl. 4), 9–13. [Google Scholar] [CrossRef] [Green Version]
- Mather, M.; Jacobsen, L.A.; Pollard, K.M. Aging in the United States; Population Reference Bureau: Washington, DC, USA, 2015; Available online: https://www.prb.org/wp-content/uploads/2016/01/aging-us-population-bulletin-1.pdf (accessed on 21 June 2021).
- Chen, S.; Kuhn, M.; Prettner, K.; Bloom, D.E. The macroeconomic burden of noncommunicable diseases in the United States: Estimates and projections. PLoS ONE 2018, 13, e0206702. [Google Scholar] [CrossRef]
- Budreviciute, A.; Damiati, S.; Sabir, D.K.; Onder, K.; Schuller-Goetzburg, P.; Plakys, G.; Katileviciute, A.; Khoja, S.; Kodzius, R. Management and Prevention Strategies for Non-communicable Diseases (NCDs) and Their Risk Factors. Front. Public Health 2020, 8, 788. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.M.; Farwell, W.R.; Jha, A.K. Primary care visit duration and quality: Does good care take longer? Arch. Intern. Med. 2009, 169, 1866–1872. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). The Impact of the COVID-19 Pandemic on Noncommunicable Disease Resources and Services: Results of a Rapid Assessment. 2020. Available online: https://www.who.int/teams/noncommunicable-diseases/covid-19 (accessed on 21 June 2021).
- World Health Organization (WHO). Information Note: Covid-19 and NCDs. 2020. Available online: https://www.who.int/docs/default-source/inaugural-who-partners-forum/covid-19-and-ncds---final---corr7.pdf?sfvrsn=9b65e287_1&download=true (accessed on 21 June 2021).
- Negrini, S.; Grabljevec, K.; Boldrini, P.; Kiekens, C.; Moslavac, S.; Zampolini, M.; Christodoulou, N. Up to 2.2 million people experiencing disability suffer collateral damage each day of COVID-19 lockdown in Europe. Eur. J. Phys. Rehabil. Med. 2020, 56, 361–365. [Google Scholar] [CrossRef]
- Caminiti, C.; Maglietta, G.; Meschi, T.; Ticinesi, A.; Silva, M.; Sverzellati, N. Effects of the COVID-19 Epidemic on Hospital Admissions for Non-Communicable Diseases in a Large Italian University-Hospital: A Descriptive Case-Series Study. J. Clin. Med. 2021, 10, 880. [Google Scholar] [CrossRef]
- Jones, D.; Neal, R.D.; Duffy, S.R.G.; Scott, S.E.; Whitaker, K.L.; Brain, K. Impact of the COVID-19 pandemic on the symptomatic diagnosis of cancer: The view from primary care. Lancet Oncol. 2020, 21, 748–750. [Google Scholar] [CrossRef]
- Mafham, M.M.; Spata, E.; Goldacre, R.; Gair, D.; Curnow, P.; Bray, M.; Hollings, S.; Roebuck, C.; Gale, C.P.; Mamas, M.A.; et al. COVID-19 pandemic and admission rates for and management of acute coronary syndromes in England. Lancet 2020, 396, 381–389. [Google Scholar] [CrossRef]
- Elective surgery cancellations due to the COVID-19 pandemic: Global predictive modelling to inform surgical recovery plans. Br. J. Surg. 2020, 107, 1440–1449.
- Mouawad, N.J.; Woo, K.; Malgor, R.D.; Wohlauer, M.V.; Johnson, A.P.; Cuff, R.F.; Coleman, D.M.; Coogan, S.M.; Sheahan, M.G., 3rd; Shalhub, S. The impact of the COVID-19 pandemic on vascular surgery practice in the United States. J. Vasc. Surg. 2021, 73, 772–779.e4. [Google Scholar] [CrossRef] [PubMed]
- Davis, K.L.; Davis, D.D. Disability Determination and Impairment Rating. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2021. [Google Scholar]
- Zavaleta, D.; Samuel, K.; Mills, C. Measures of Social Isolation. Soc. Indic. Res. 2017, 131, 367–391. [Google Scholar] [CrossRef] [Green Version]
- What Is Depression? 2020. Available online: https://www.psychiatry.org/patients-families/depression/what-is-depression (accessed on 21 June 2021).
- Pérez-Rodrigo, C.; Gianzo Citores, M.; Hervás Bárbara, G.; Ruiz-Litago, F.; Casis Sáenz, L.; Arija, V.; López-Sobaler, A.M.; de Victoria, E.M.; Ortega, R.M.; Partearroyo, T.; et al. Patterns of Change in Dietary Habits and Physical Activity during Lockdown in Spain Due to the COVID-19 Pandemic. Nutrients 2021, 13, 300. [Google Scholar] [CrossRef]
- Drieskens, S.; Berger, N.; Vandevijvere, S.; Gisle, L.; Braekman, E.; Charafeddine, R.; De Ridder, K.; Demarest, S. Short-term impact of the COVID-19 confinement measures on health behaviours and weight gain among adults in Belgium. Arch. Public Health 2021, 79, 1–10. [Google Scholar] [CrossRef]
- Sidor, A.; Rzymski, P. Dietary Choices and Habits during COVID-19 Lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef]
- Ferrante, G.; Camussi, E.; Piccinelli, C.; Senore, C.; Armaroli, P.; Ortale, A.; Garena, F.; Giordano, L. Did social isolation during the SARS-CoV-2 epidemic have an impact on the lifestyles of citizens? Epidemiol. Prev. 2020, 44, 353–362. [Google Scholar]
- Lehtisalo, J.; Palmer, K.; Mangialasche, F.; Solomon, A.; Kivipelto, M.; Ngandu, T. Changes in Lifestyle, Behaviors, and Risk Factors for Cognitive Impairment in Older Persons During the First Wave of the Coronavirus Disease 2019 Pandemic in Finland: Results from the FINGER Study. Front. Psychiatry 2021, 12, 21. [Google Scholar] [CrossRef]
- Campaign to End Loneliness, What Works Centre for Wellbeing. Available online: https://www.campaigntoendloneliness.org/ (accessed on 21 June 2021).
- Wang, B.; Li, R.; Lu, Z.; Huang, Y. Does comorbidity increase the risk of patients with COVID-19: Evidence from meta-analysis. Aging 2020, 12, 6049–6057. [Google Scholar] [CrossRef]
- Palmer, K.; Monaco, A.; Kivipelto, M.; Onder, G.; Maggi, S.; Michel, J.P.; Prieto, R.; Sykara, G.; Donde, S. The potential long-term impact of the COVID-19 outbreak on patients with non-communicable diseases in Europe: Consequences for healthy ageing. Aging Clin. Exp. Res. 2020, 32, 1189–1194. [Google Scholar] [CrossRef]
- Lakhan, R.; Agrawal, A.; Sharma, M. Prevalence of Depression, Anxiety, and Stress during COVID-19 Pandemic. J. Neurosci. Rural Pract. 2020, 11, 519–525. [Google Scholar]
- Werneck, A.O.; Silva, D.R.; Malta, D.C.; Gomes, C.S.; Souza-Júnior, P.R.; Azevedo, L.O.; Barros, M.B.; Szwarcwald, C.L. Associations of sedentary behaviours and incidence of unhealthy diet during the COVID-19 quarantine in Brazil. Public Health Nutr. 2021, 24, 422–426. [Google Scholar] [CrossRef]
- Zhang, H.Q.; Lin, J.Y.; Guo, Y.; Pang, S.; Jiang, R.; Cheng, Q.J. Medication adherence among patients with chronic obstructive pulmonary disease treated in a primary general hospital during the COVID-19 pandemic. Ann. Transl. Med. 2020, 8, 1179. [Google Scholar] [CrossRef]
- Cutler, R.L.; Fernandez-Llimos, F.; Frommer, M.; Benrimoj, C.; Garcia-Cardenas, V. Economic impact of medication non-adherence by disease groups: A systematic review. BMJ Open 2018, 8, e016982. [Google Scholar] [CrossRef] [Green Version]
- Sampa, M.B.; Hoque, M.R.; Islam, R.; Nishikitani, M.; Nakashima, N.; Yokota, F.; Kikuchi, K.; Rahman, M.M.; Shah, F.; Ahmed, A. Redesigning Portable Health Clinic Platform as a Remote Healthcare System to Tackle COVID-19 Pandemic Situation in Unreached Communities. Int. J. Environ. Res. Public Health 2020, 17, 4709. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Algorithm for COVID-19 Triage and Referral: Patient Triage and Referral for Resource Limited Settings during Community Transmission. 2020. Available online: https://apps.who.int/iris/handle/10665/331915 (accessed on 21 June 2021).
- Wosik, J.; Fudim, M.; Cameron, B.; Gellad, Z.F.; Cho, A.; Phinney, D.; Curtis, S.; Roman, M.; Poon, E.G.; Ferranti, J.; et al. Telehealth transformation: COVID-19 and the rise of virtual care. J. Am. Med. Inform. Assoc. 2020, 27, 957–962. [Google Scholar] [CrossRef]
- Martorella, G.; Fredericks, S.; Sanders, J.; Wynne, R. Breaking pandemic chain reactions: Telehealth psychosocial support in cardiovascular disease during COVID-19. Eur. J. Cardiovasc. Nurs. 2021, 20, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Neubeck, L.; Hansen, T.; Jaarsma, T.; Klompstra, L.; Gallagher, R. Delivering healthcare remotely to cardiovascular patients during COVID-19: A rapid review of the evidence. Eur. J. Cardiovasc. Nurs. 2020, 19, 486–494. [Google Scholar] [CrossRef]
- Frayn, M.; Fojtu, C.; Juarascio, A. COVID-19 and binge eating: Patient perceptions of eating disorder symptoms, tele-therapy, and treatment implications. Curr. Psychol. 2021, 40, 1–10. [Google Scholar]
- Thelliez, B. Téléconsultation à L’officine: Avez-Vous Sauté le pas? Le Pharmacien de France. 2021. Available online: http://www.lepharmaciendefrance.fr/actualite-web/teleconsultation-a-lofficine-avez-vous-saute-le-pas (accessed on 21 June 2021).
- Smith, A.C.; Thomas, E.; Snoswell, C.L.; Haydon, H.; Mehrotra, A.; Clemensen, J.; Caffery, L.J. Telehealth for global emergencies: Implications for coronavirus disease 2019 (COVID-19). J. Telemed. Telecare 2020, 26, 309–313. [Google Scholar] [CrossRef] [Green Version]
- Eurocarers. Why Addressing the Needs of Informal Carers Is a Crucial Issue for Europe; Eurocarers: Etterbeek, Belgium, 2017; Available online: https://eurocarers.org/publications/why-addressing-the-needs-of-informal-carers-is-a-crucial-issue-for-europe/ (accessed on 21 June 2021).
- Eurocarers. How Informal Caregivers’ Life and Care Situations Changed during the Corona-Pandemic in Germany. 2021. Available online: https://eurocarers.org/how-informal-caregivers-life-and-care-situations-changed-during-the-corona-pandemic-in-germany/ (accessed on 21 June 2021).
- European Centre for Social Welfare Policy and Research. Socioeconomic Condition of Informal Carers during the COVID-19 Pandemic. Available online: https://www.euro.centre.org/webitem/3855 (accessed on 21 June 2021).
- Carers, U.K. Caring Behind Closed Doors. Available online: https://www.carersuk.org/news-and-campaigns/campaigns/caring-behind-closed-doors (accessed on 21 June 2021).
- Eurocarers. Eurocarers’ Policy Paper on Non-Communicable Diseases and Informal Care; Eurocarers: Etterbeek, Belgium, 2017; Available online: https://eurocarers.org/publications/non-communicable-diseases-mental-health-and-informal-care/ (accessed on 21 June 2021).
- Je T’aide, Tout un Collectif Pour Les Aidant.e.s. Les Aidant.e.s à L’épreuve du Confinement. 2020. Available online: http://associationjetaide.org (accessed on 21 June 2021).
- Monaco, A.; Palmer, K.; Marengoni, A.; Maggi, S.; Hassan, T.A.; Donde, S. Integrated care for the management of ageing-related non-communicable diseases: Current gaps and future directions. Aging Clin. Exp. Res. 2020, 32, 1353–1358. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). WHO Package of Essential Noncommunicable (PEN) Disease Interventions for Primary Health Care; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/who-package-of-essential-noncommunicable-(pen)-disease-interventions-for-primary-health-care (accessed on 21 June 2021).
- Bousquet, J.; Anto, J.M.; Sterk, P.J.; Adcock, I.M.; Chung, K.F.; Roca, J.; Agusti, A.; Brightling, C.; Cambon-Thomsen, A.; Cesario, A.; et al. Systems medicine and integrated care to combat chronic noncommunicable diseases. Genome Med. 2011, 3, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Mobula, L.M.; Heller, D.J.; Commodore-Mensah, Y.; Walker Harris, V.; Cooper, L.A. Protecting the vulnerable during COVID-19: Treating and preventing chronic disease disparities. Gates Open Res. 2020, 4, 125. [Google Scholar] [CrossRef] [PubMed]
- Kluge, H.H.P.; Wickramasinghe, K.; Rippin, H.L.; Mendes, R.; Peters, D.H.; Kontsevaya, A.; Breda, J. Prevention and control of non-communicable diseases in the COVID-19 response. Lancet 2020, 395, 1678–1680. [Google Scholar] [CrossRef]
- Bekey. Healthcare Systems in the USA and Europe: Differences, Challenges, Trends. 2019. Available online: https://bekey.io/blog/healthcare-systems-in-the-usa-and-europe-differences-challenges-trends (accessed on 21 June 2021).
- Statista. Percentage of Global Population Accessing the Internet from 2005 to 2019, by Market Maturity. 2020. Available online: https://0-www-statista-com.brum.beds.ac.uk/statistics/209096/share-of-internet-users-in-the-total-world-population-since-2006/ (accessed on 21 June 2021).
- Raïs, S.; Radoszycki, L.; Dourgnon, P.; Rochaix, L.; Chekroun, M. Accurate Representation of Patients’ Opinions for Decisionmaking: Are Online Health Communities Good Candidates? 2017. Available online: https://www.carenity.co.uk/static/doc/corporate/poster-ISPOR2017-Accurate-Representation-of-patients-opinions-for-decision-making.pdf (accessed on 21 June 2021).
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development. 2015. Available online: https://sdgs.un.org/2030agenda (accessed on 21 June 2021).











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | First Wave (n = 2489) | Second Wave (n = 2342) |
|---|---|---|
| Gender, n (%) | ||
| Female | 1602 (64) | 1396 (60) |
| Male | 887 (36) | 946 (40) |
| Mean age, years (range) | 53 (18–91) | 52 (18–90) |
| Age groups, years | ||
| ≤40 | 528 (21) | 560 (24) |
| 41–50 | 423 (17) | 393 (17) |
| 51–60 | 698 (28) | 652 (28) |
| 61–70 | 612 (25) | 531 (23) |
| >70 | 228 (9) | 206 (9) |
| Country of residence, n (%) | ||
| Belgium | 4 (<1) | 14 (<1) |
| France | 611 (25) | 551 (24) |
| Germany | 247 (10) | 363 (15) |
| Italy | 313 (13) | 282 (12) |
| Spain | 354 (14) | 374 (16) |
| United Kingdom | 458 (18) | 346 (15) |
| United States of America | 502 (20) | 412 (18) |
| City size, n (%) | ||
| Metropolitan city a | 542 (22) | 533 (23) |
| Large city b | 333 (13) | 285 (12) |
| Mid-sized city c | 568 (23) | 580 (25) |
| Small city d | 637 (26) | 568 (24) |
| Rural town e | 357 (14) | 339 (14) |
| Other | 52 (2) | 37 (2) |
| Housing type, n (%) | ||
| House with a yard | 1418 (56) | 1260 (54) |
| Apartment | 814 (33) | 831 (35) |
| House without a yard | 125 (5) | 111 (5) |
| Studio apartment | 63 (3) | 90 (4) |
| Other | 69 (3) | 50 (2) |
| Number of people per household f, | ||
| Mean number (range) | 2.7 (1–10) | 2.6 (1–9) |
| n (%) | ||
| 1 | 469 (19) | 451 (19) |
| 2 | 944 (38) | 849 (36) |
| 3 | 478 (19) | 466 (20) |
| >3 | 598 (24) | 576 (25) |
| Number of children per household | ||
| Mean number (range) | 0.5 (0–4) | 0.5 (0–5) |
| n (%) | ||
| 0 | 1754 (71) | 1599 (68) |
| 1 | 373 (15) | 378 (16) |
| 2 | 251 (10) | 257 (11) |
| ≥3 | 79 (3) | 79 (3) |
| Variables a, n (%) | First Wave (n = 2489) | Second Wave (n = 2342) |
|---|---|---|
| Chronic diseases | ||
| Metabolic diseases | 1042 (42) | 989 (42) |
| Respiratory diseases | 930 (37) | 772 (33) |
| Cardiovascular diseases | 603 (24) | 691 (30) |
| Mental disorders | 577 (23) | 597 (25) |
| Cancer | 155 (6) | 170 (7) |
| Most frequent chronic conditions | ||
| Type 2 diabetes | 832 (33) | 693 (30) |
| Arterial hypertension | 575 (23) | 419 (18) |
| Asthma | 562 (23) | 543 (23) |
| COPD b | 459 (18) | 312 (13) |
| Depression | 412 (17) | 301 (13) |
| Disability level of disease c, mean (range) | 5.5 (0–10) | 5.5 (0–10) |
| 0–1 | 366 (15) | 336 (14) |
| 2–3 | 370 (15) | 360 (15) |
| 4–5 | 621 (25) | 560 (24) |
| 6–7 | 620 (25) | 603 (26) |
| 8–10 | 512 (20) | 483 (21) |
| Intake of regular/long-term treatments | ||
| Yes | 2242 (90) | 2114 (90) |
| No | 247 (10) | 228 (10) |
| Depressive symptoms before lockdown | ||
| Yes | 1033 (41) | 1072 (46) |
| No | 1456 (59) | 1270 (54) |
| Anxiety before lockdown | ||
| Yes | 1138 (46) | 1105 (47) |
| No | 1351 (54) | 1237 (53) |
| COVID-19 testing | ||
| Yes | 612 (25) | 825 (35) |
| No | 1877 (75) | 1517 (65) |
| COVID-19 testing results | ||
| Positive | 100 (16) | 166 (20) |
| Negative | 503 (82) | 649 (79) |
| Positive and negative d | 9 (2) | 10 (1) |
| Variables | Cluster 1 (n = 802) | Cluster 2 (n = 887) | Cluster 3 (n = 800) |
|---|---|---|---|
| Type of Patients | Younger highly Impacted Patients | Middle-aged Moderately Impacted Patients | Less impacted Older Patients |
| Age (mean) | ≤45 years old (40.5) | 46 to 60 years old (57.5) | >60 years old (60.1) |
| Gender | 59% of women | 79% of women | 54% of women |
| Number of chronic diseases | less than 3 | more than 3 | less than 3 |
| Primary chronic diseases | mental diseases | respiratory diseases and cancers | metabolic and cardiovascular diseases |
| Living in… | Italy, Spain and the USA | the UK and France/Belgium | France/Belgium and Germany |
| Depressive and anxiety Symptoms before lockdown | yes | yes | no |
| More likely to live in big or small cities | big | small | small |
| Disabling medical condition | moderately disabling | very disabling | not very disabling |
| Adoption of bad habits during lockdown | yes | yes | no |
| Level of isolation and stress | isolated and stressed | isolated and stressed | not isolated and not stressed |
| Worsening of the medical condition | yes | yes | no |
| Have seen their physician… | more thanusual | more than usual | As usual |
| Difficulty in finding an available HCP | yes | no | no |
| Affected by cancellation of consultations or surgeries | very affected | very affected | less affected |
| Development of a new illness | yes | yes | no |
| Development of a new mental illness | yes | yes | no |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pécout, C.; Pain, E.; Chekroun, M.; Champeix, C.; Kulak, C.; Prieto, R.; van Vugt, J.; Gilchrist, K.; Lainé-Pellet, A.-F. Impact of the COVID-19 Pandemic on Patients Affected by Non-Communicable Diseases in Europe and in the USA. Int. J. Environ. Res. Public Health 2021, 18, 6697. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136697
Pécout C, Pain E, Chekroun M, Champeix C, Kulak C, Prieto R, van Vugt J, Gilchrist K, Lainé-Pellet A-F. Impact of the COVID-19 Pandemic on Patients Affected by Non-Communicable Diseases in Europe and in the USA. International Journal of Environmental Research and Public Health. 2021; 18(13):6697. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136697
Chicago/Turabian StylePécout, Catherine, Emilie Pain, Michael Chekroun, Claire Champeix, Claudie Kulak, Rita Prieto, Joris van Vugt, Kim Gilchrist, and Anne-Félice Lainé-Pellet. 2021. "Impact of the COVID-19 Pandemic on Patients Affected by Non-Communicable Diseases in Europe and in the USA" International Journal of Environmental Research and Public Health 18, no. 13: 6697. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136697