
Strengthening Critical Health Literacy for Health Information Appraisal: An Approach from Argumentation Theory

 , , and
, , and 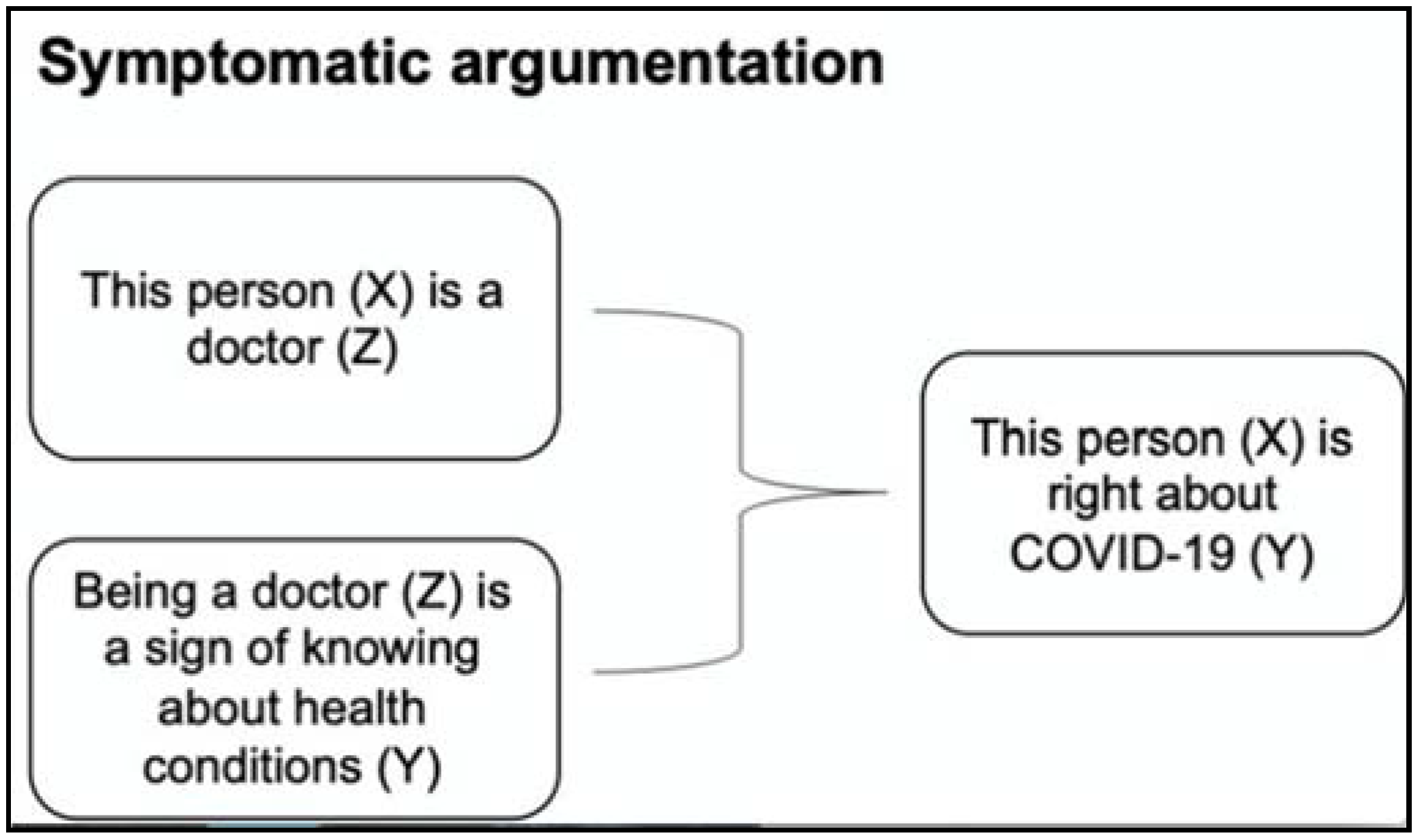{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Analytical Approach
3. Insights from Argumentation Theory
3.1. The Structure and Purpose of an Argument
- Key insight 1: People should be made aware of the concept of argument and that the acceptance of a claim derives from the approval of the supporting reasons that, as such, need to be verified and evaluated.
3.2. Argument Schemes
- Key insight 2: People should be able to recognize the most essential argument schemes to evaluate the arguments themselves.
“This person is right about COVID-19 because he is a doctor.”
- The general argument scheme for this type of argument is:Y is true of X,because: Z is true of Xand: Z is symptomatic of Y.
- In the context of the example:This person (X) is right about COVID-19 (Y).because: This person (X) is a doctor (Z).and: Being a doctor is a sign of knowing about health conditions, resulting in true health-related statements.
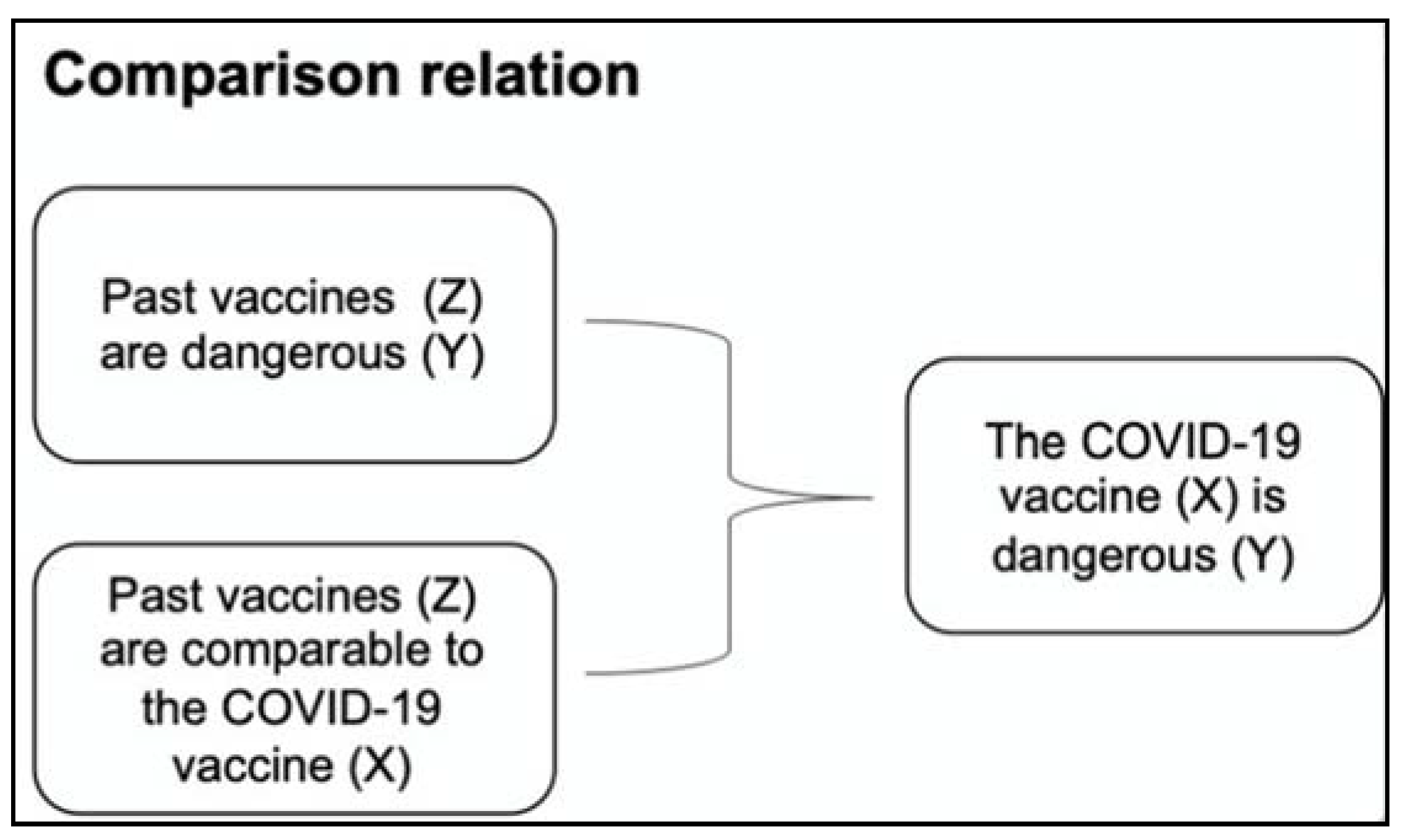
“The COVID-19 vaccine is dangerous because past vaccines have also been found to be dangerous.”
- The general argument scheme for this type of argument is:Y is appropriate for Y,because: Y is appropriate for Zand: Z is comparable to X.
- In the context of the example:The COVID-19 vaccine (X) is dangerous (Y)because: past vaccines (Z) are dangerous (Y)and: past vaccines (Z) are comparable to the COVID-19 vaccine (X).
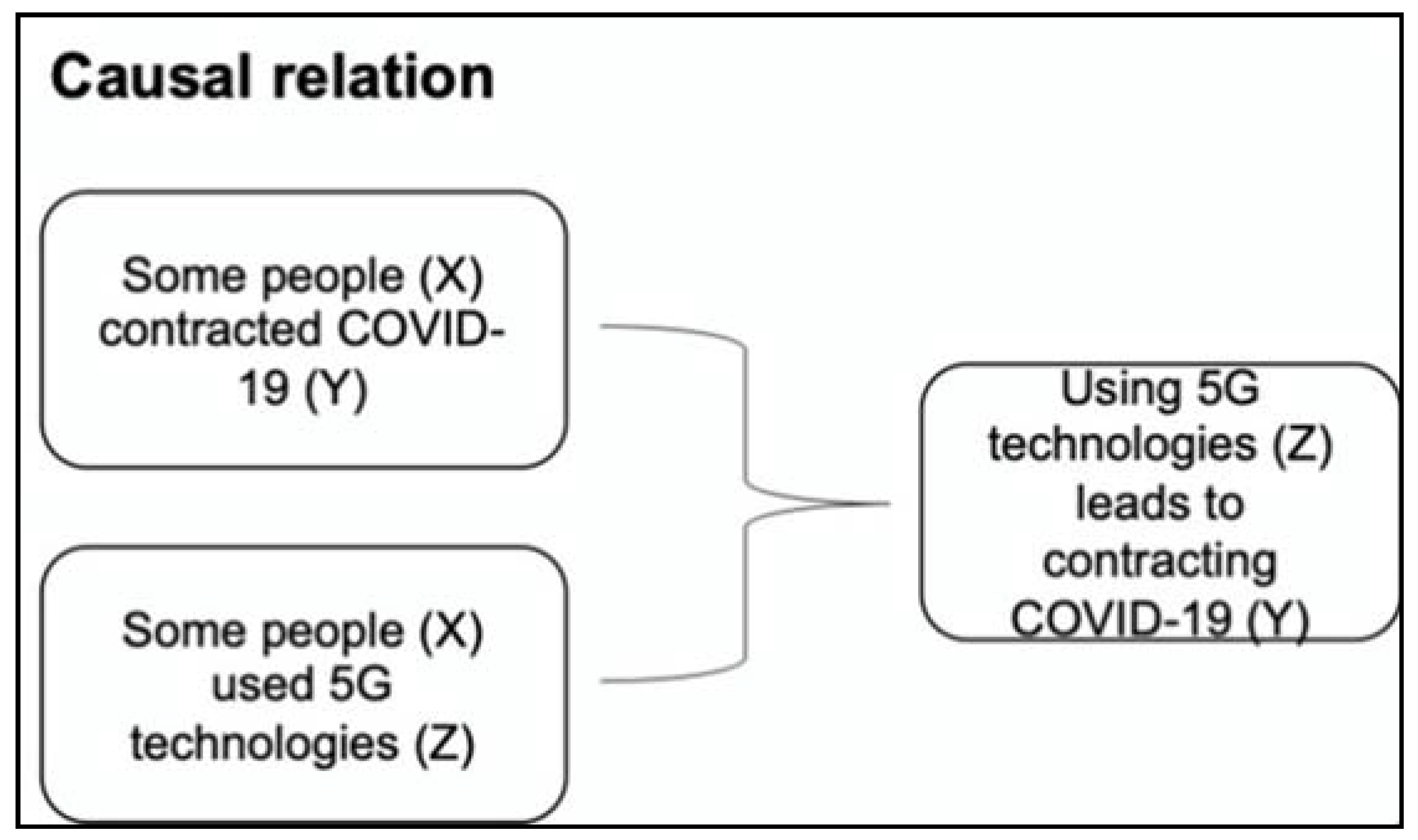
“Some people contracted COVID-19 because they used 5G technologies.”
- The general argument scheme is:Y is true of X,because: Z is true of Xand: Z leads to Y.
- In the context of the example:Using 5G technologies (Z) leads to contracting COVID-19 (Y).because: Some people (X) contracted COVID-19 (Y)and: Some people (X) used 5G technologies (Z)
3.3. Fallacies and Critical Questions
- Key insight 3: People should learn to identify the structure of an argument and then verify if it is fallacious by asking critical questions.
“This person is right about COVID-19 because they are a doctor.”
“The COVID-19 vaccine is dangerous because past vaccines have also been found to be dangerous.”
“Some people contracted COVID-19 because they were exposed to 5G radiowaves.”
4. Discussion
- (1)
- to recognize when health information is argumentative, that is, when the speaker presents a claim that they want the audience to accept, believe, or act upon;
- (2)
- to identify whether reasons support claims, and if so, which argument scheme they implement (that is, schemes based on symptomatic relations, analogy, or causality);
- (3)
- to ask the main critical questions to look for evidence behind the proposed reasons that can support or deny the claims’ validity (and acceptance).
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19-5 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19-5-march-2020 (accessed on 24 March 2020).
- Eysenbach, G.; Powell, J.; Kuss, O.; Sa, E.R. Empirical studies assessing the quality of health information for consumers on the world wide web: A systematic review. JAMA 2002, 287, 2691–2700. [Google Scholar] [PubMed]
- Cline, R.J.; Haynes, K.M. Consumer health information seeking on the Internet: The state of the art. Health Educ. Res. 2001, 16, 671–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allington, D.; Duffy, B.; Wessely, S.; Dhavan, N.; Rubin, J. Health-protective behaviour, social media usage and conspiracy belief during the COVID-19 public health emergency. Psychol. Med. 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Brennen, J.S.; Simon, F.; Howard, P.N.; Nielsen, R.K. Types, sources, and claims of COVID-19 misinformation. Reuters Inst. 2020, 7, 3-1. [Google Scholar]
- Burel, G.; Farrell, T.; Mensio, M.; Khare, P.; Alani, H. Co-spread of Misinformation and Fact-Checking Content during the Covid-19 Pandemic. In Proceedings of the 12th International Conference on Social Informatics, Pisa, Italy, 6–9 October 2020; pp. 28–42. [Google Scholar]
- Carmi, E.; Yates, S.J.; Lockley, E.; Pawluczuk, A. Data citizenship: Rethinking data literacy in the age of disinformation, misinformation, and malinformation. Internet Policy Rev. 2020, 9, 1–22. [Google Scholar] [CrossRef]
- Call for Action: Managing the Infodemic. Available online: https://www.who.int/news/item/11-12-2020-call-for-action-managing-the-infodemic (accessed on 14 May 2021).
- Rubinelli, S.; Schulz, P.J.; Nakamoto, K. Health literacy beyond knowledge and behaviour: Letting the patient be a patient. Int. J. Public Health 2009, 54, 307–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diviani, N.; Obrenovic, J.; Montoya, C.L.; Karcz, K. Disentangling health information appraisal competence: Results from an interdisciplinary scoping review and online consultation among Swiss stakeholders. PLoS ONE 2020, 15, e0235474. [Google Scholar] [CrossRef] [PubMed]
- Chinn, D. Critical health literacy: A review and critical analysis. Soc. Sci. Med. 2011, 73, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Diviani, N. On the Centrality of Information Appraisal in Health Literacy Research. HLRP Health Lit. Res. Pract. 2019, 3, e21–e24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Eemeren, F.H.; Grootendorst, R.; Kruiger, T. Handbook of Argumentation Theory: A Critical Survey of Classical Backgrounds and Modern Studies; Walter de Gruyter GmbH & Co KG: Berlin, Germany, 2019. [Google Scholar]
- van Eemeren, F.H.; Grootendorst, R.; Jacobs, C.S.; Jackson, S.A. Reconstructing Argumentative Discourse; The University of Alabama Press: Tuscaloosa, AL, USA, 2002. [Google Scholar]
- van Eemeren, F.H.; Grootendorst, R.; Eemeren, F.H. A Systematic Theory of Argumentation: The Pragma-Dialectical Approach; Cambridge University Press: Cambridge, UK, 2004. [Google Scholar]
- Rubinelli, S. Rational versus unreasonable persuasion in doctor-patient communication: A normative account. Patient Educ. Couns. 2013, 92, 296–301. [Google Scholar] [CrossRef]
- Rubinelli, S.; Henkemans, A.F.S. Argumentation and Health; John Benjamins Publishing Company: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Walton, D. Fundamentals of Critical Argumentation; Cambridge University Press: Cambridge, UK, 2005. [Google Scholar]
- Walton, D. Argument Evaluation and Evidence; Springer: Cham, Switzerland, 2015. [Google Scholar]
- Jiménez-Aleixandre, M.P.; Puig, B. Argumentation, evidence evaluation and critical thinking. In Second International Handbook of Science Education; Springer: Dordrecht, The Netherlands, 2012; pp. 1001–1015. [Google Scholar]
- Van Eemeren, F.H.; Grootendorst, R.; Meuffels, B. The skill of identifying argumentation. J. Am. Forensic Assoc. 1989, 25, 239–245. [Google Scholar] [CrossRef] [Green Version]
- Cacioppo, J.T.; Petty, R.E. The elaboration likelihood model of persuasion. In Communication and Persuasion; Springer: New York, NY, USA, 1986. [Google Scholar]
- Walton, D.; Reed, C.; Macagno, F. Argumentation Schemes, 1st ed.; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2008. [Google Scholar]
- van Eemeren, F.H.; Garssen, B.; Labrie, N. Argumentation between Doctors and Patients: Understanding Clinical Argumentative Discourse; John Benjamins Publishing Company: Amsterdam, The Netherlands, 2021. [Google Scholar]
- van Eemeren, F.H.; Grootendorst, R. Argumentation, Communication, and Fallacies: A Pragma-Dialectical Perspective; Routledge: Abingdon, UK, 2016. [Google Scholar]
- van Eemeren, F.H.; Henkemans, A.F.S. Argumentation: Analysis and Evaluation; Routledge: Abingdon, UK, 2016. [Google Scholar]
- Siegel, H. Critical thinking as an educational ideal. In The Educational Forum; Taylor & Francis: Abingdon, UK, 1980; pp. 7–23. [Google Scholar]
- Andrews, R. Critical thinking and/or argumentation in higher education. In The Palgrave Handbook of Critical Thinking in Higher Education; Springer: Cham, Switzerland, 2015; pp. 49–62. [Google Scholar]
- Hitchcock, D. On Reasoning and Argument; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Hyytinen, H.; Toom, A.; Shavelson, R.J. Enhancing Scientific Thinking Through the Development of Critical Thinking in Higher Education. In Redefining Scientific Thinking for Higher Education; Springer: Cham, Switzerland, 2019; pp. 59–78. [Google Scholar]
- Tversky, A.; Kahneman, D. Judgment under uncertainty: Heuristics and biases. Science 1974, 185, 1124–1131. [Google Scholar] [CrossRef] [PubMed]
- Rubinelli, S.; Diviani, N.; Fiordelli, M. The Cognitive and Behavioral Sciences. In Communicating about Risks and Safe Use of Medicines: Real Life and Applied Research; Bahri, P., Ed.; Springer: Heidelberg, Germany, 2020. [Google Scholar]
- Bacon, F. Essays; WL Allison: New York, NY, USA, 1888. [Google Scholar]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rubinelli, S.; Ort, A.; Zanini, C.; Fiordelli, M.; Diviani, N. Strengthening Critical Health Literacy for Health Information Appraisal: An Approach from Argumentation Theory. Int. J. Environ. Res. Public Health 2021, 18, 6764. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136764
Rubinelli S, Ort A, Zanini C, Fiordelli M, Diviani N. Strengthening Critical Health Literacy for Health Information Appraisal: An Approach from Argumentation Theory. International Journal of Environmental Research and Public Health. 2021; 18(13):6764. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136764
Chicago/Turabian StyleRubinelli, Sara, Alexander Ort, Claudia Zanini, Maddalena Fiordelli, and Nicola Diviani. 2021. "Strengthening Critical Health Literacy for Health Information Appraisal: An Approach from Argumentation Theory" International Journal of Environmental Research and Public Health 18, no. 13: 6764. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136764