
A Novel Radiographic Measurement Method for the Evaluation of Metatarsophalangeal Joint Dislocation of the Lesser Toe in Patients with Rheumatoid Arthritis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
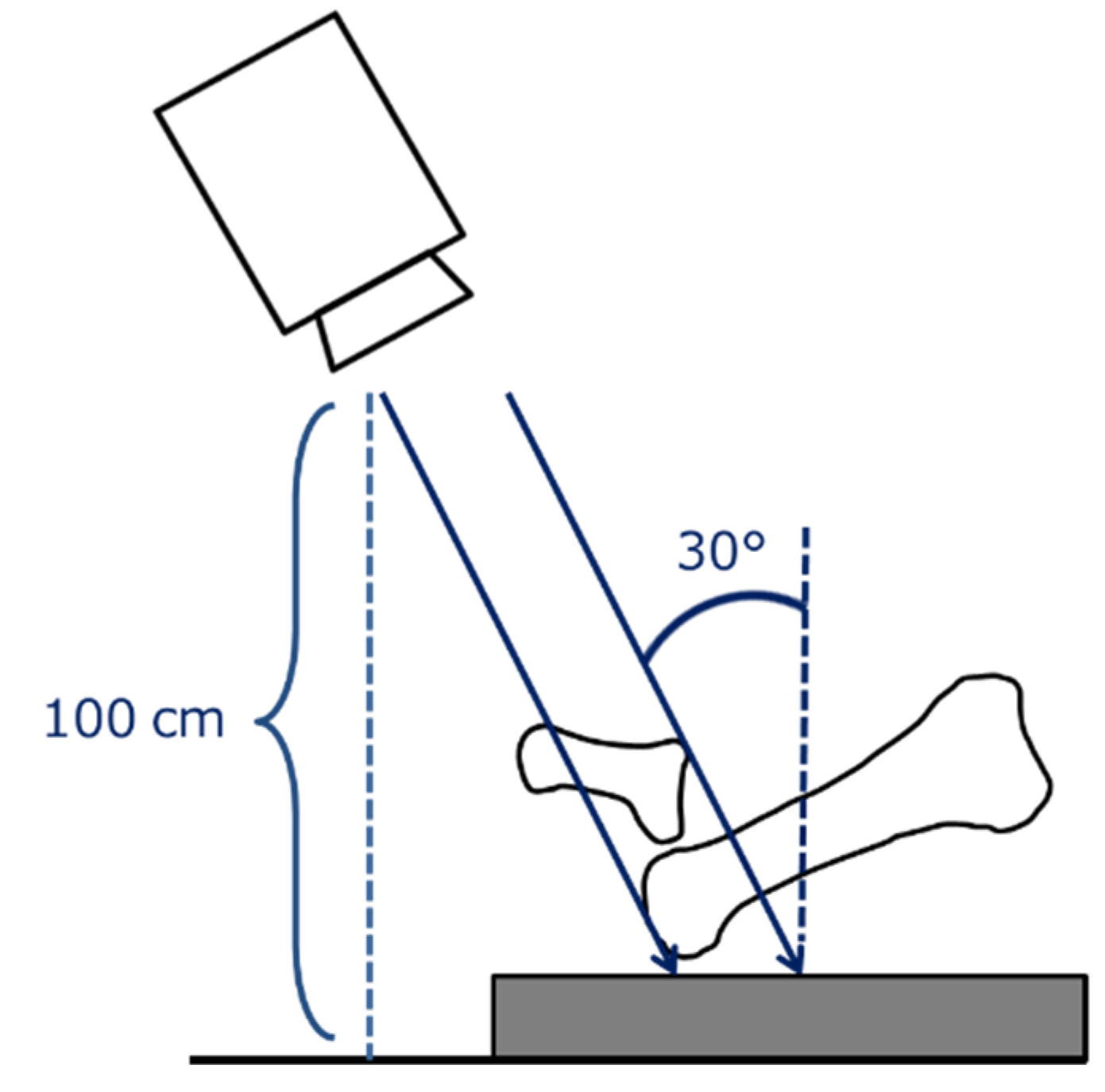
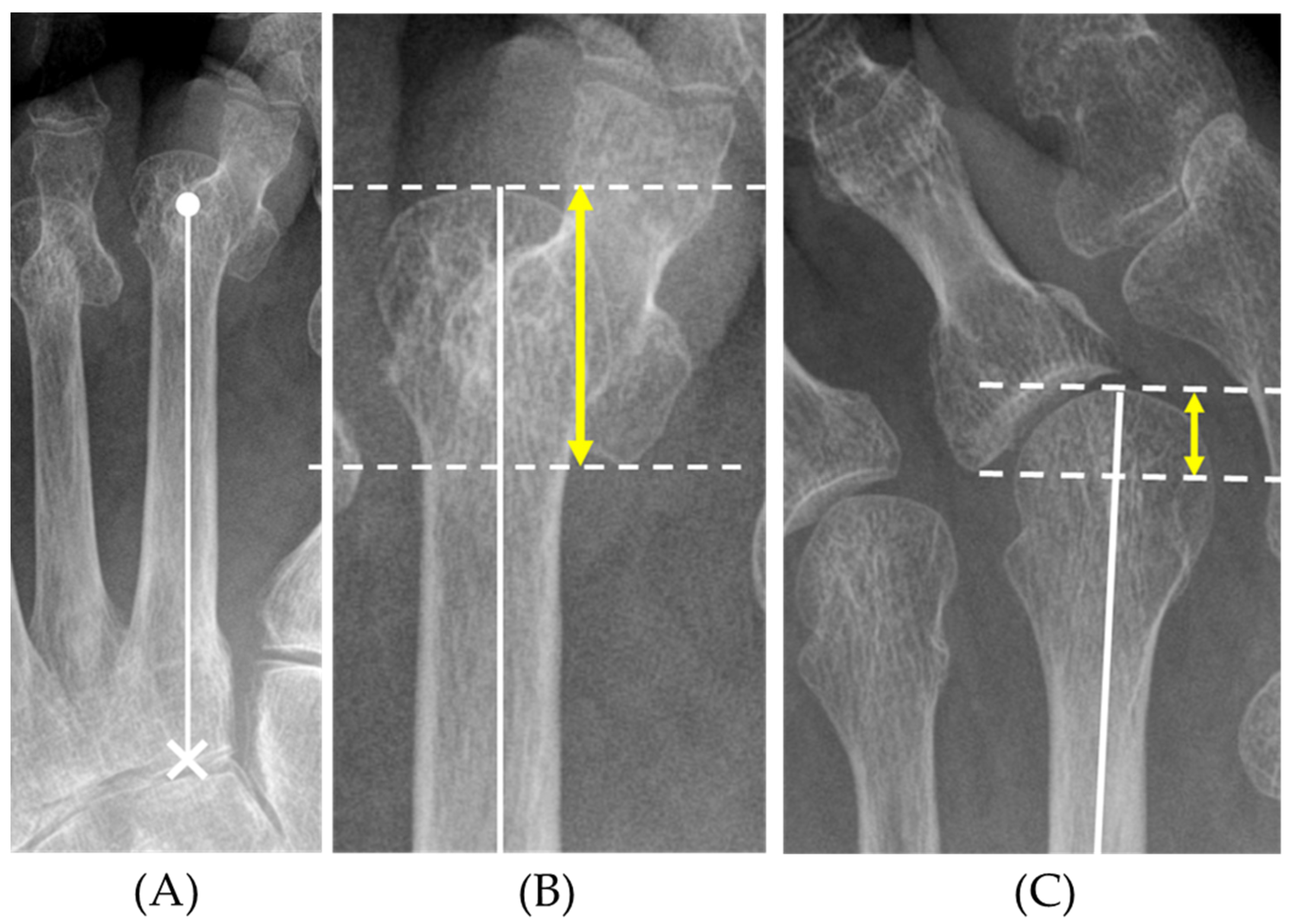
2.2. Radiographic Measurement of Toe Deformities by the Mtp Overlap Distance (MOD)
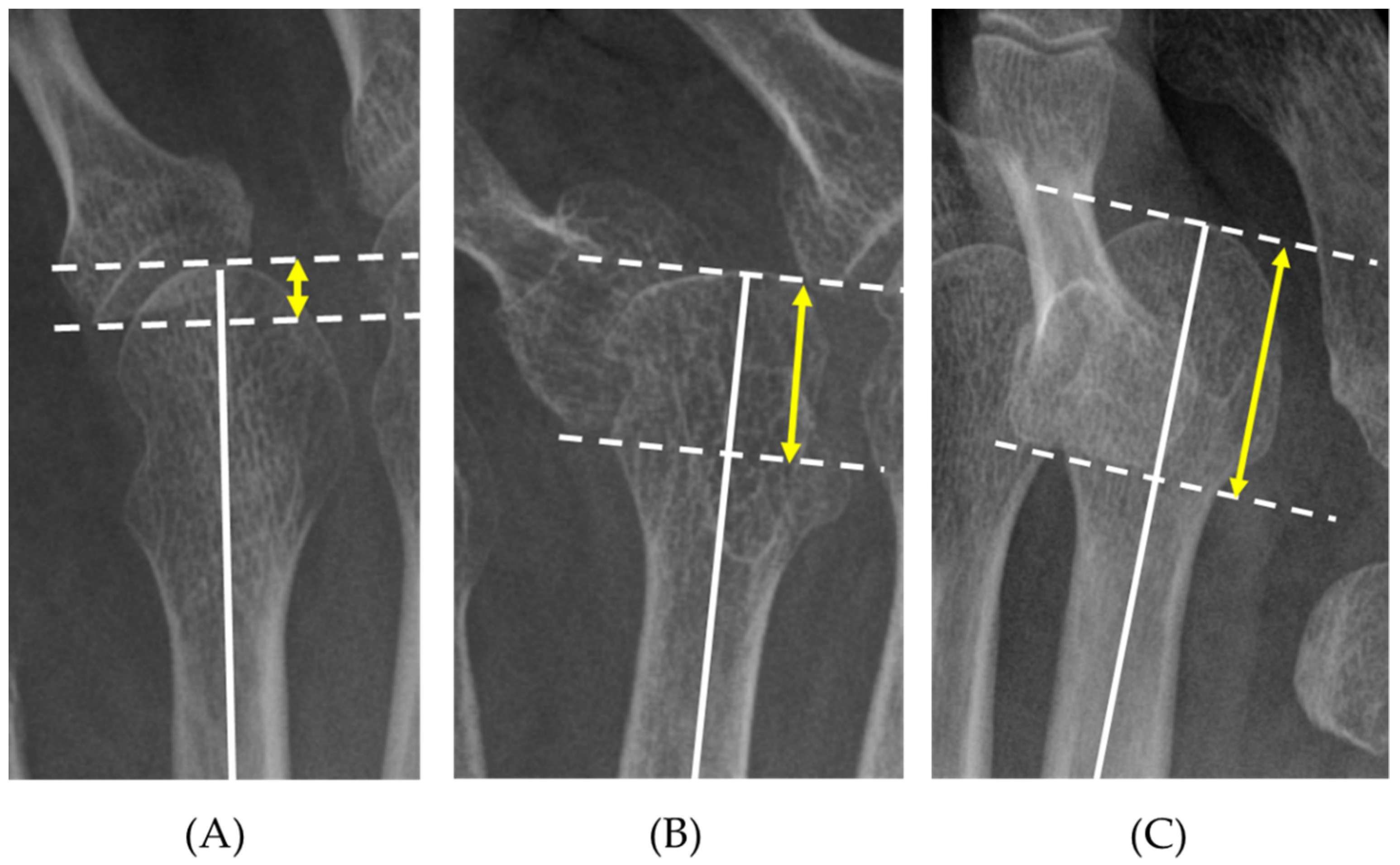
2.3. Grading of Forefoot Deformities Based on the MOD
2.4. Investigation of Reproducibility
2.5. Perioperative Assessment
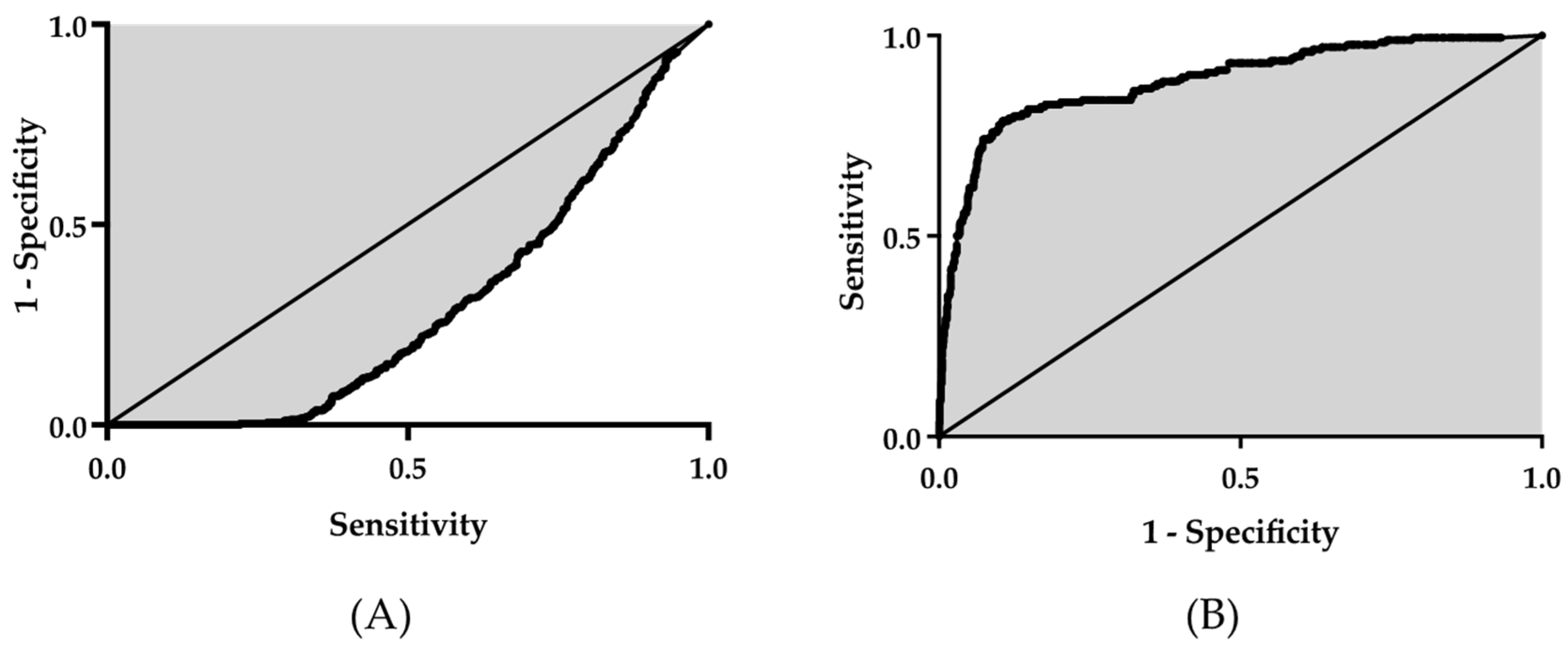
2.6. Statistical Analysis
3. Results
3.1. Measurement of MOD
3.2. Grading of the MOD
3.3. Investigation of Reproducibility
3.4. Perioperative Assessment
3.4.1. Clinical Assessment
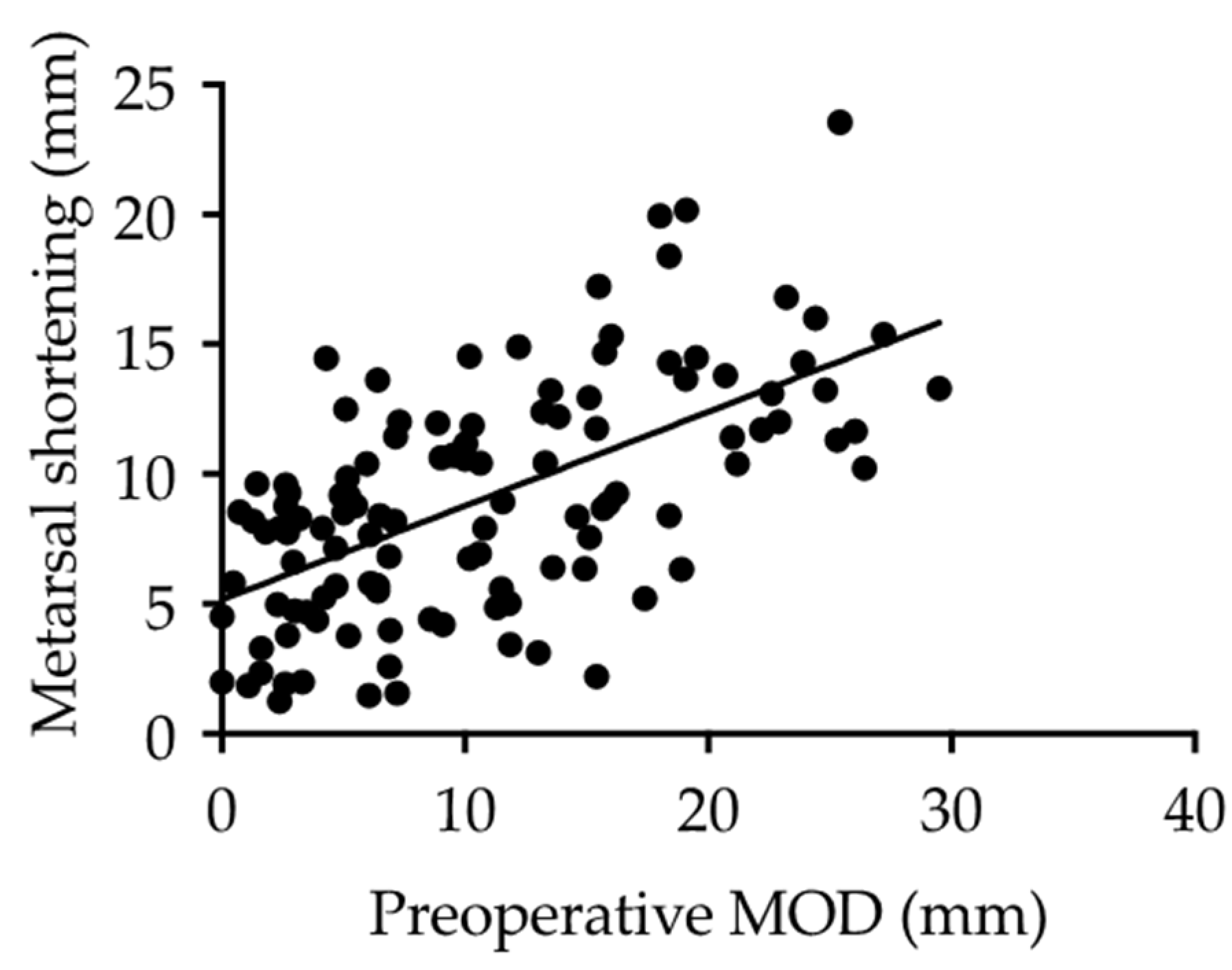
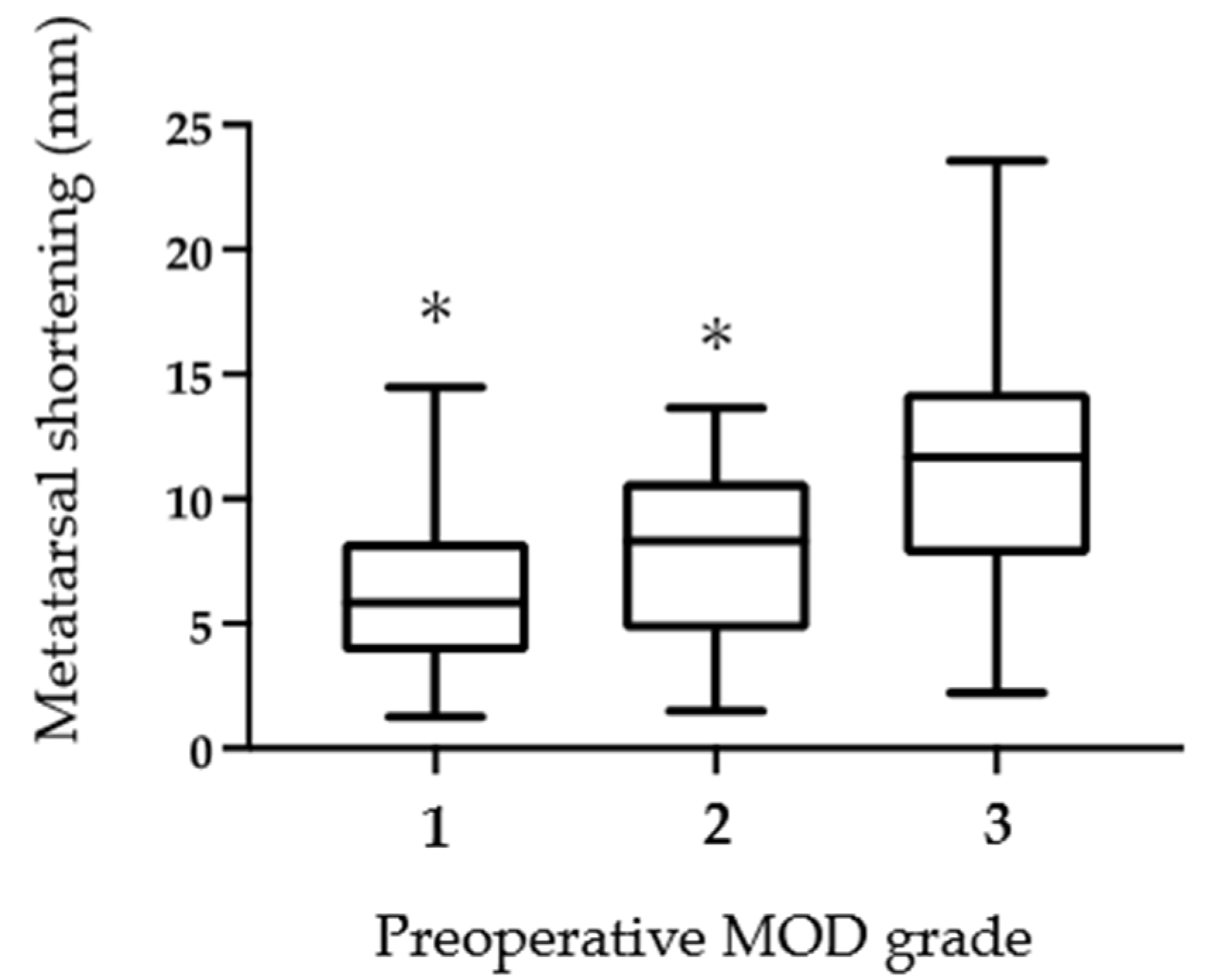
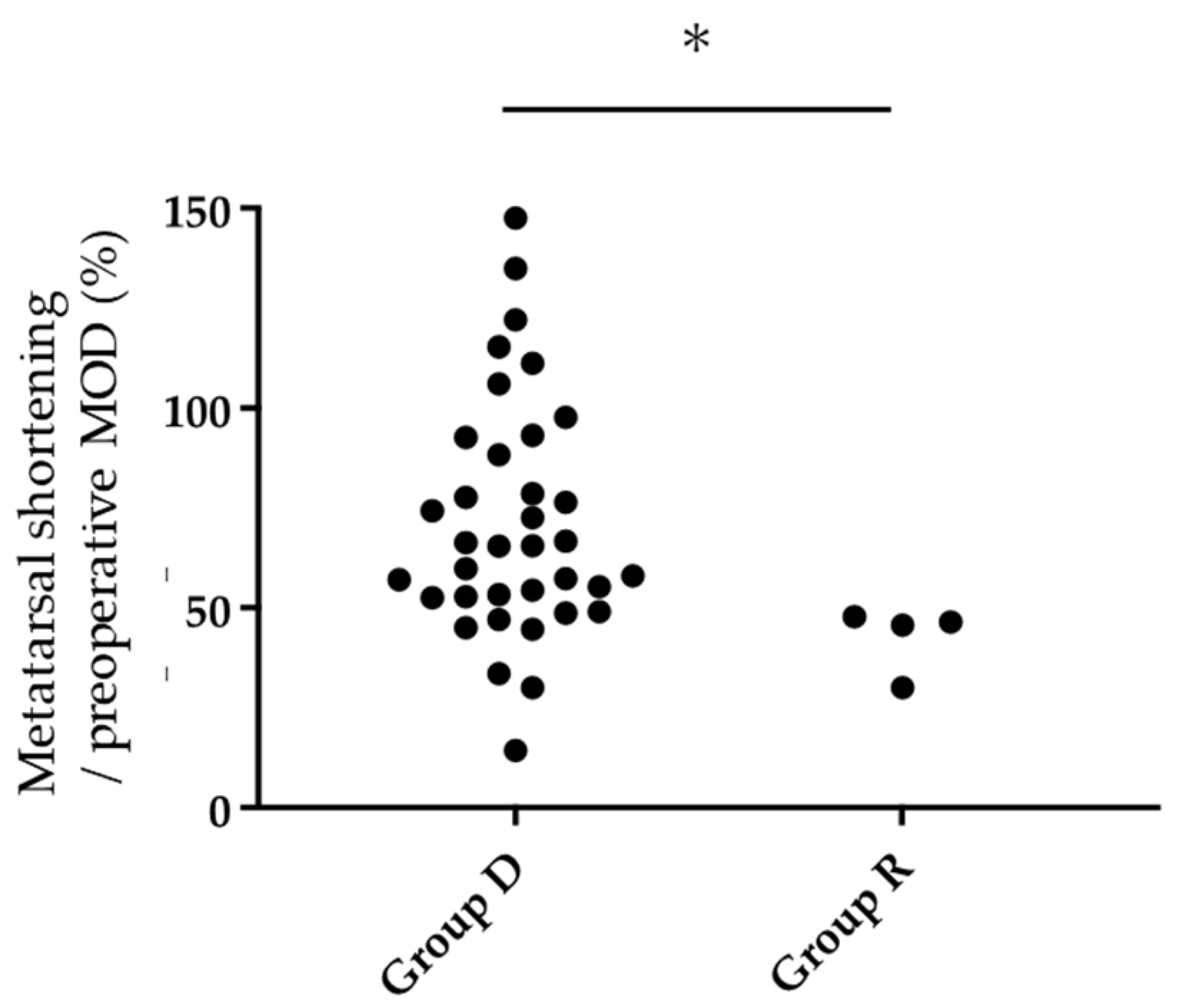
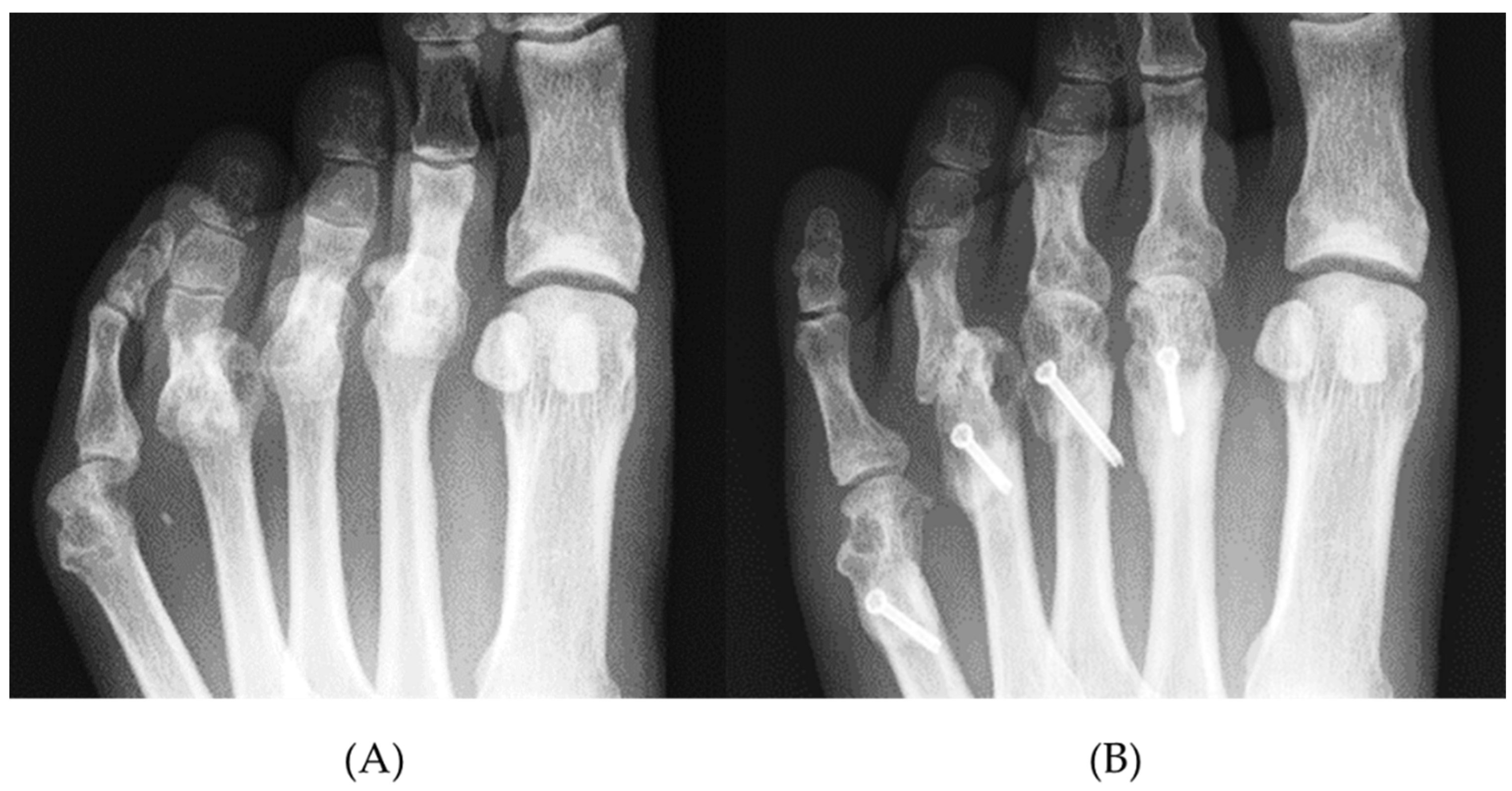
3.4.2. Radiographic Assessment
4. Discussion
4.1. Joint Preservation Surgeries for Rheumatoid Forefoot Deformities
4.2. Classification of Lesser Toe Deformities
4.3. Shortening Oblique Osteotomies for Lesser Toes
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Young, B.L.; Watson, S.L.; Perez, J.L.; McGwin, G.; Singh, J.A.; Ponce, B.A. Trends in Joint Replacement Surgery in Patients with Rheumatoid Arthritis. J. Rheumatol. 2018, 45, 158–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cordtz, R.; Hawley, S.; Prieto-Alhambra, D.; Højgaard, P.; Zobbe, K.; Kristensen, L.E.; Overgaard, S.; Odgaard, A.; Soussi, B.G.; Dreyer, L. Reduction in Upper Limb Joint Surgery Among Rheumatoid Arthritis Patients: An Interrupted Time-Series Analysis Using Danish Health Care Registers. Arthritis Care Res. 2020, 72, 274–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagy, G.; Roodenrijs, N.M.; Welsing, P.M.; Kedves, M.; Hamar, A.; Van Der Goes, M.C.; Kent, A.; Bakkers, M.; Blaas, E.; Senolt, L.; et al. EULAR definition of difficult-to-treat rheumatoid arthritis. Ann. Rheum. Dis. 2021, 80, 31–35. [Google Scholar] [CrossRef] [PubMed]
- De Hair, M.J.H.; Jacobs, J.W.G.; Schoneveld, J.L.M.; Van Laar, J.M. Difficult-to-treat rheumatoid arthritis: An area of unmet clinical need. Rheumatology 2018, 57, 1135–1144. [Google Scholar] [CrossRef]
- Rahimnia, A.; Alishiri, G.; Bayatpoor, M.E.; Hosseini, M.A.; Najafizadeh-Sari, S.; Yaribeygi, H.; Sahebkar, A. Evaluation of Disease Severity and Health-Related Quality of Life in Patients with Rheumatoid Arthritis Undergoing Total Knee Arthroplasty. Curr. Rheumatol. Rev. 2021, 17, 88–94. [Google Scholar] [CrossRef]
- Siviero, P.; Marseglia, A.; Biz, C.; Rovini, A.; Ruggieri, P.; Nardacchione, R.; Maggi, S. Quality of life outcomes in patients undergoing knee replacement surgery: Longitudinal findings from the QPro-Gin study. BMC Musculoskelet. Disord. 2020, 21, 436. [Google Scholar] [CrossRef]
- Momohara, S.; Inoue, E.; Ikari, K.; Ochi, K.; Ishida, O.; Yano, K.; Sakuma, Y.; Yoshida, S.; Koyama, T.; Koenuma, N.; et al. Recent Trends in Orthopedic Surgery Aiming to Improve Quality of Life for Those with Rheumatoid Arthritis: Data from a Large Observational Cohort. J. Rheumatol. 2014, 41, 862–866. [Google Scholar] [CrossRef]
- Matsumoto, T.; Nishino, J.; Izawa, N.; Naito, M.; Hirose, J.; Tanaka, S.; Yasui, T.; Saisho, K.; Tohma, S. Trends in Treatment, Outcomes, and Incidence of Orthopedic Surgery in Patients with Rheumatoid Arthritis: An Observational Cohort Study Using the Japanese National Database of Rheumatic Diseases. J. Rheumatol. 2017, 44, 1575–1582. [Google Scholar] [CrossRef]
- Bolland, B.J.; Sauvé, P.S.; Taylor, G.R. Rheumatoid Forefoot Reconstruction: First Metatarsophalangeal Joint Fusion Combined with Weil’s Metatarsal Osteotomies of the Lesser Rays. J. Foot Ankle Surg. 2008, 47, 80–88. [Google Scholar] [CrossRef]
- Helal, B. Metatarsal osteotomy for metatarsalgia. J. Bone Jt. Surg. Br. 1975, 57, 187–192. [Google Scholar] [CrossRef]
- Ebina, K.; Hirao, M.; Hashimoto, J.; Nampei, A.; Shi, K.; Tomita, T.; Futai, K.; Kunugiza, Y.; Noguchi, T.; Yoshikawa, H. Comparison of a self-administered foot evaluation questionnaire (SAFE-Q) between joint-preserving arthroplasty and resection-replacement arthroplasty in forefoot surgery for patients with rheumatoid arthritis. Mod. Rheumatol. 2017, 27, 795–800. [Google Scholar] [CrossRef]
- Ebina, K.; Hirao, M.; Takagi, K.; Ueno, S.; Morimoto, T.; Matsuoka, H.; Kitaguchi, K.; Iwahashi, T.; Hashimoto, J.; Yoshikawa, H. Comparison of the effects of forefoot joint-preserving arthroplasty and resection-replacement arthroplasty on walking plantar pressure distribution and patient-based outcomes in patients with rheumatoid arthritis. PLoS ONE 2017, 12, e0183805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirao, M.; Ebina, K.; Tsuboi, H.; Nampei, A.; Kushioka, J.; Noguchi, T.; Tsuji, S.; Owaki, H.; Hashimoto, J.; Yoshikawa, H. Outcomes of modified metatarsal shortening offset osteotomy for forefoot deformity in patients with rheumatoid arthritis: Short to mid-term follow-up. Mod. Rheumatol. 2017, 27, 981–989. [Google Scholar] [CrossRef] [PubMed]
- Horita, M.; Nishida, K.; Hashizume, K.; Nasu, Y.; Saiga, K.; Nakahara, R.; Machida, T.; Ohashi, H.; Ozaki, T. Outcomes of Resection and Joint-Preserving Arthroplasty for Forefoot Deformities for Rheumatoid Arthritis. Foot Ankle Int. 2018, 39, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Nishida, K.; Machida, T.; Horita, M.; Hashizume, K.; Nakahara, R.; Nasu, Y.; Ohashi, H.; Saiga, K.; Ozaki, T. Shortening Oblique Osteotomy with Screw Fixation for Correction of the Lesser Metatarsophalangeal Joints of Rheumatoid Forefoot. Acta Med. Okayama 2016, 70, 477–483. [Google Scholar]
- Yano, K.; Ikari, K.; Ishibashi, M.; Momohara, S. Preventing delayed union after distal shortening oblique osteotomy of metatarsals in the rheumatoid forefoot. Mod. Rheumatol. 2016, 26, 546–550. [Google Scholar] [CrossRef]
- Fukushi, J.-I.; Nakashima, Y.; Okazaki, K.; Yamada, H.; Mawatari, T.; Ohishi, M.; Oyamada, A.; Akasaki, Y.; Iwamoto, Y. Outcome of Joint-Preserving Arthroplasty for Rheumatoid Forefoot Deformities. Foot Ankle Int. 2016, 37, 262–268. [Google Scholar] [CrossRef]
- Niki, H.; Hirano, T.; Akiyama, Y.; Mitsui, H.; Fujiya, H. Long-term outcome of joint-preserving surgery by combination metatarsal osteotomies for shortening for forefoot deformity in patients with rheumatoid arthritis. Mod. Rheumatol. 2015, 25, 683–688. [Google Scholar] [CrossRef]
- Ishie, S.; Ito, H.; Azukizawa, M.; Furu, M.; Ishikawa, M.; Ogino, H.; Hamamoto, Y.; Matsuda, S. Delayed wound healing after forefoot surgery in patients with rheumatoid arthritis. Mod. Rheumatol. 2015, 25, 367–372. [Google Scholar] [CrossRef]
- Arnett, F.C.; Edworthy, S.M.; Bloch, D.A.; McShane, D.J.; Fries, J.F.; Cooper, N.S.; Healey, L.A.; Kaplan, S.R.; Liang, M.H.; Luthra, H.S.; et al. The american rheumatism association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988, 31, 315–324. [Google Scholar] [CrossRef]
- Kay, J.; Upchurch, K.S. ACR/EULAR 2010 rheumatoid arthritis classification criteria. Rheumatology 2012, 51 (Suppl. 6), vi5–vi9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shima, H.; Okuda, R.; Yasuda, T.; Jotoku, T.; Kitano, N.; Kinoshita, M. Radiographic Measurements in Patients with Hallux Valgus Before and After Proximal Crescentic Osteotomy. J. Bone Jt. Surg. Am. 2009, 91, 1369–1376. [Google Scholar] [CrossRef]
- Niki, H.; Aoki, H.; Inokuchi, S.; Ozeki, S.; Kinoshita, M.; Kura, H.; Tanaka, Y.; Noguchi, M.; Nomura, S.; Hatori, M.; et al. Development reliability of a standard rating system for outcome measurement of foot ankle disorders I: Development of standard rating system. J. Orthop. Sci. 2005, 10, 457–465. [Google Scholar] [CrossRef] [Green Version]
- Niki, H.; Aoki, H.; Inokuchi, S.; Ozeki, S.; Kinoshita, M.; Kura, H.; Tanaka, Y.; Noguchi, M.; Nomura, S.; Hatori, M.; et al. Development and reliability of a standard rating system for outcome measurement of foot and ankle disorders II: Interclinician and intraclinician reliability and validity of the newly established standard rating scales and Japanese Orthopaedic Association rating scale. J. Orthop. Sci. 2005, 10, 466–474. [Google Scholar] [CrossRef] [Green Version]
- Niki, H.; Tatsunami, S.; Haraguchi, N.; Aoki, T.; Okuda, R.; Suda, Y.; Takao, M.; Tanaka, Y. Validity and reliability of a self-administered foot evaluation questionnaire (SAFE-Q). J. Orthop. Sci. 2013, 18, 298–320. [Google Scholar] [CrossRef] [Green Version]
- Biz, C.; Corradin, M.; Kanah, W.T.K.; Dalmau-Pastor, M.; Zornetta, A.; Volpin, A.; Ruggieri, P. Medium-Long-Term Clinical and Radiographic Outcomes of Minimally Invasive Distal Metatarsal Metaphyseal Osteotomy (DMMO) for Central Primary Metatarsalgia: Do Maestro Criteria Have a Predictive Value in the Preoperative Planning for This Percutaneous Technique? BioMed Res. Int. 2018, 2018, 1947024. [Google Scholar] [CrossRef] [Green Version]
- Mann, R.A. Subluxations and dislocations of second metatarsophalangeal joint. In Surgery of the Foot, 5th ed.; Mosby Co.: Maryland Heights, MO, USA, 1986; pp. 148–152. [Google Scholar]
- Rabin, S.I. Lisfranc dislocation and associated metatarsophalangeal joint dislocations. A case report and literature review. Am. J. Orthop. 1996, 25, 305–309. [Google Scholar]
- Doorn, P.F.; Keijsers, N.L.; Van Limbeek, J.; Anderson, P.G.; Laan, R.F.; Bosch, P.V.P.; Malefijt, M.C.D.W.; Louwerens, J.W.K. A clinical classification system for rheumatoid forefoot deformity. Foot Ankle Surg. 2011, 17, 158–165. [Google Scholar] [CrossRef]
- Hirao, M.; Tsuboi, H.; Akita, S.; Koga, T.; Matsushita, M.; Ohshima, S.; Saeki, Y.; Hashimoto, J. Hind-mid-forefoot Deformity in Hallux Valgus Deformity in Rheumatoid Arthritis: Radiographic Evaluation Grouped by Existence of Dorsal Dislocation of Second Metatarsophalangeal Joint. Rheumatol. Curr. Res. 2013, 3. [Google Scholar] [CrossRef] [Green Version]
- Okuda, R.; Kinoshita, M.; Morikawa, J.; Jotoku, T.; Abe, M. Surgical Treatment for Hallux Valgus with Painful Plantar Callosities. Foot Ankle Int. 2001, 22, 203–208. [Google Scholar] [CrossRef]
- Hanyu, T.; Yamazaki, H.; Murasawa, A.; Tohyama, C. Arthroplasty for Rheumatoid Forefoot Deformities by a Shortening Oblique Osteotomy. Clin. Orthop. Relat. Res. 1997, 338, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Niki, H.; Hirano, T.; Okada, H.; Beppu, M. Combination joint-preserving surgery for forefoot deformity in patients with rheumatoid arthritis. J. Bone Jt. Surg. Br. 2010, 92, 380–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brage, M.E.; Holmes, J.R.; Sangeorzan, B.J. The Influence of X-Ray Orientation on the First Metatarsocuneiform Joint Angle. Foot Ankle Int. 1994, 15, 495–497. [Google Scholar] [CrossRef]
- Miller, J.W. Distal first metatarsal displacement osteotomy. Its place in the schema of bunion surgery. J. Bone Jt. Surg. Am. 1974, 56, 923–931. [Google Scholar] [CrossRef]
- Maestro, M.; Besse, J.-L.; Ragusa, M.; Berthonnaud, E. Forefoot morphotype study and planning method for forefoot osteotomy. Foot Ankle Clin. 2003, 8, 695–710. [Google Scholar] [CrossRef]
- Biz, C.; Maso, G.; Malgarini, E.; Tagliapietra, J.; Ruggieri, P. Hypermobility of the first ray: The cinderella of the measurements conventionally assessed for correction of hallux valgus. Acta Biomed. 2020, 91, 47–59. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| with Callosities | without Callosities | ||||||
|---|---|---|---|---|---|---|---|
| Number of Toes | MOD (mm) | Number of Toes | MOD (mm) | p Value | AUC | Cut-Off Value (mm) | |
| 2nd | 63 | 14.0 ± 8.1 | 213 | 3.2 ± 3.8 | <0.001 | 0.90 | 10 |
| 3rd | 66 | 14.7 ± 7.1 | 210 | 3.4 ± 3.1 | <0.001 | 0.91 | 8.4 |
| 4th | 20 | 16.8 ± 4.7 | 256 | 4.0 ± 4.9 | <0.001 | 0.95 | 9.8 |
| 5th | 25 | 8.5 ± 4.4 | 251 | 4.1 ± 2.7 | <0.001 | 0.80 | 6.6 |
| Total | 174 | 14.0 ± 7.3 | 930 | 3.7 ± 3.8 | <0.001 | 0.89 | 7.8 |
| Preoperative | Postoperative | p Value | ||
|---|---|---|---|---|
| MOD (mm) | 10.7 ± 7.5 | 4.8 ± 2.4 | <0.001 | |
| MOD grade | grade 1 | 31 | 75 | <0.001 |
| (toes) | grade 2 | 28 | 39 | |
| grade 3 | 57 | 2 | ||
| JSSF scale | General pain | 21.0 ± 3.1 | 28.1 ± 4.0 | <0.001 |
| Deformity | 15.1 ± 3.5 | 21.3 ± 2.7 | <0.001 | |
| Motion | 9.4 ± 3.6 | 11.0 ± 2.6 | 0.006 | |
| Walking ability | 12.8 ± 4.5 | 18.9 ± 3.2 | <0.001 | |
| ADL | 4.0 ± 2.2 | 5.6 ± 2.8 | <0.001 | |
| Total | 62.4 ± 7.5 | 85.0 ± 9.4 | <0.001 | |
| SAFE-Q | Pain-related | 59.3 ± 17.1 | 68.0 ± 14.5 | 0.016 |
| Physical Functioning and Daily Living | 65.6 ± 17.2 | 71.0 ± 14.8 | 0.005 | |
| Social Functioning | 70.0 ± 23.1 | 76.6 ± 17.5 | 0.021 | |
| Shoe-related | 44.3 ± 21.3 | 51.9 ± 27.0 | 0.062 | |
| General Health and Well-being | 65.7 ± 24.5 | 75.2 ± 23.2 | 0.002 | |
| r Value | p Value | ||
|---|---|---|---|
| Δ JSSF scale | General pain | 0.24 | 0.22 |
| Deformity | 0.46 | 0.02 | |
| Motion | 0.08 | 0.68 | |
| Walking ability | −0.24 | 0.23 | |
| ADL | 0.25 | 0.22 | |
| Total | 0.29 | 0.15 | |
| Δ SAFE-Q | Pain-related | −0.11 | 0.59 |
| Physical Functioning and Daily Living | −0.14 | 0.51 | |
| Social Functioning | −0.33 | 0.10 | |
| Shoe-related | 0.08 | 0.69 | |
| General Health and Well-being | −0.20 | 0.33 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohashi, H.; Nishida, K.; Nasu, Y.; Saiga, K.; Nakahara, R.; Horita, M.; Okita, S.; Ozaki, T. A Novel Radiographic Measurement Method for the Evaluation of Metatarsophalangeal Joint Dislocation of the Lesser Toe in Patients with Rheumatoid Arthritis. Int. J. Environ. Res. Public Health 2021, 18, 7520. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147520
Ohashi H, Nishida K, Nasu Y, Saiga K, Nakahara R, Horita M, Okita S, Ozaki T. A Novel Radiographic Measurement Method for the Evaluation of Metatarsophalangeal Joint Dislocation of the Lesser Toe in Patients with Rheumatoid Arthritis. International Journal of Environmental Research and Public Health. 2021; 18(14):7520. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147520
Chicago/Turabian StyleOhashi, Hideki, Keiichiro Nishida, Yoshihisa Nasu, Kenta Saiga, Ryuichi Nakahara, Masahiro Horita, Shunji Okita, and Toshifumi Ozaki. 2021. "A Novel Radiographic Measurement Method for the Evaluation of Metatarsophalangeal Joint Dislocation of the Lesser Toe in Patients with Rheumatoid Arthritis" International Journal of Environmental Research and Public Health 18, no. 14: 7520. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147520