
Home-Based Parent–Child Interaction Therapy to Prevent Child Maltreatment: A Randomized Controlled Trial


Abstract
:1. Introduction
2. Materials and Methods
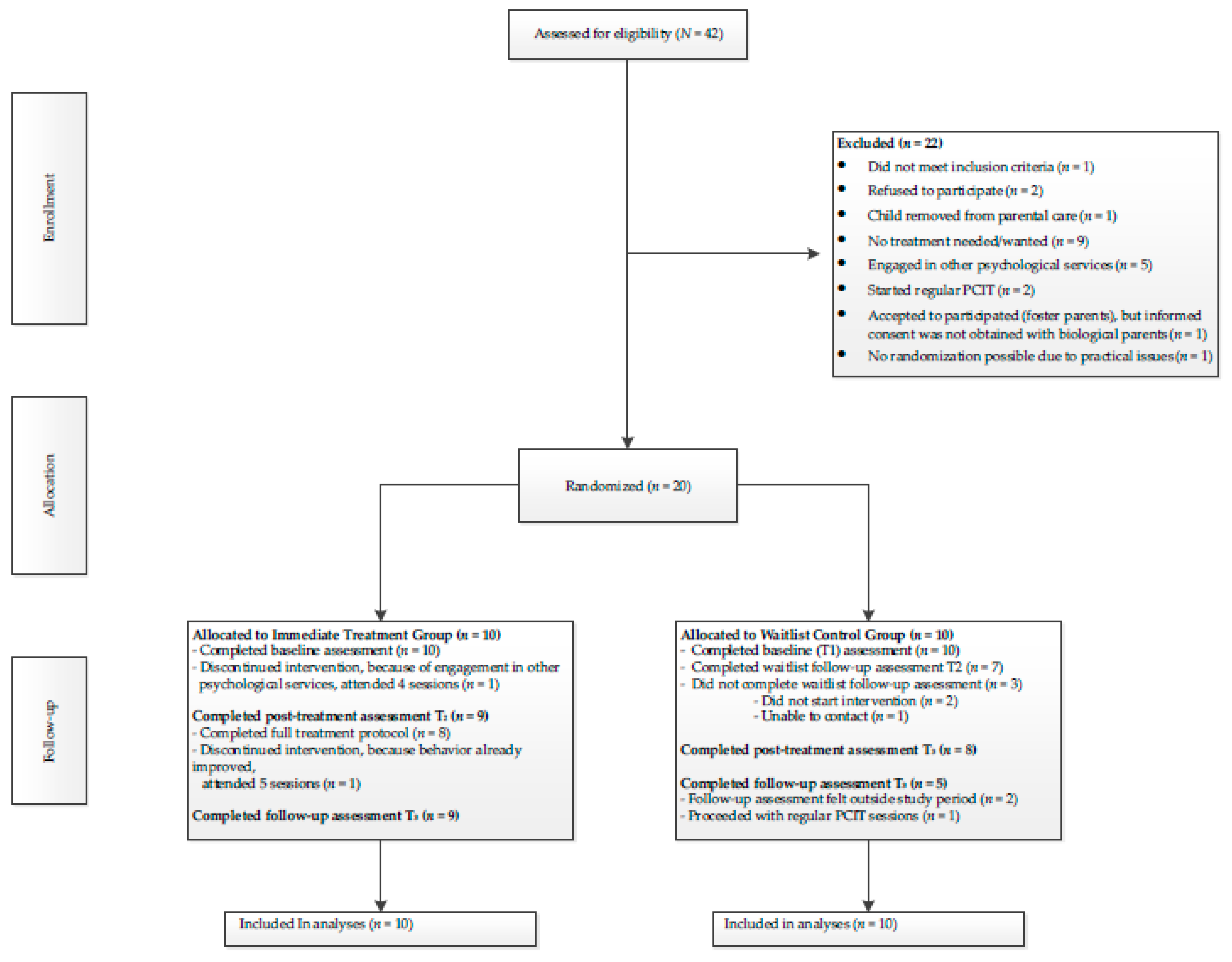
2.1. Participants and Procedure
2.2. Parent–Child Interaction Therapy (PCIT)
2.3. Training and Fidelity
3. Measures
3.1. Brief Child Abuse Potential Inventory
3.2. Eyberg Child Behavior Inventory
3.3. Parenting Stress Questionnaire
3.4. Dyadic Parent–Child Interaction Coding System
3.5. Therapy Attitude Inventory
3.6. Statistical Analyses
4. Results
4.1. Sample Characteristics
4.2. Immediate Treatment Compared to Waitlist
4.3. Overall Treatment Effectiveness
4.4. Treatment Satisfaction
5. Discussion
5.1. Clinical Implications
5.2. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hillis, S.; Mercy, J.; Amobi, A.; Kress, H. Global prevalence of past-year violence against children: A systematic review and minimum estimates. Pediatrics 2016, 137, e20154079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norman, R.E.; Byambaa, M.; De, R.; Butchart, A.; Scott, J.; Vos, T. The long-term health consequences of child physical abuse, emotional abuse, and neglect: A systematic review and meta-analysis. PLoS Med. 2012, 9, e20154079. [Google Scholar] [CrossRef] [Green Version]
- Alink, L.; van IJzendoorn, M.H.; Bakermans-Kranenburg, M.J.; Pannebakker, F.; Vogels, T.; Euser, S. Kindermishandeling in Nederland Anno 2010. In De Tweede Nationale Prevalentiestudie Mishandeling van Kinderen en Jeugdigen (NPM-2010) [Child Maltreatment in the Netherlands]; Casimir Publishers: Leiden, The Netherlands, 2011. [Google Scholar]
- Thomas, R.; Zimmer-Gembeck, M.J. Accumulating evidence for Parent-Child Interaction Therapy in the prevention of child maltreatment. Child Dev. 2011, 82, 177–192. [Google Scholar] [CrossRef] [PubMed]
- De Haan, A.M.; Boon, A.E.; Vermeiren, R.R.J.M.; De Jong, J.T.V.M. Ethnic differences in utilization of youth mental health care. Ethn. Health 2012, 17, 105–110. [Google Scholar] [CrossRef]
- Zwaanswijk, M.; Verhaak, P.F.M.; Bensing, J.M.; Van der Ende, J.; Verhulst, F.C. Help seeking for emotional and behavioural problems in children and adolescents. Eur. Child Adolesc. Psychiatry 2003, 12, 153–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, D.; Julion, W.; Fogg, L. What motivates participation and dropout among low-income urban families of color in a prevention intervention? Fam. Relat. 2001, 50, 246–254. [Google Scholar] [CrossRef]
- Ingoldsby, E.M. Review of interventions to improve family engagement and retention in parent and child mental health programs. J. Child. Fam. Stud. 2010, 19, 629–645. [Google Scholar] [CrossRef] [Green Version]
- Niec, L.N. Handbook of Parent-Child Interaction Therapy: Innovations and Applications for Research and Practice; Springer: Berlin, Germany, 2018. [Google Scholar]
- Kennedy, S.C.; Kim, J.S.; Tripodi, S.J.; Brown, S.M.; Gowdy, G. Does Parent-Child Interaction Therapy reduce future physical abuse? A meta-analysis. Res. Soc. Work Prac. 2014, 26, 147–156. [Google Scholar] [CrossRef]
- MacMillan, H.L.; Wathen, C.N.; Barlow, J.; Fergusson, D.M.; Leventhal, J.M.; Taussig, H.N. Interventions to prevent child maltreatment and associated impairment. Lancet 2009, 373, 250–266. [Google Scholar] [CrossRef]
- Thomas, R.; Zimmer-Gembeck, M.J. Parent-Child Interaction Therapy: An evidence-based treatment for child maltreatment. Child Maltreat. 2012, 17, 253–266. [Google Scholar] [CrossRef] [Green Version]
- Whipple, E.E.; Webster-Stratton, C. The role of parental stress in physically abusive families. Child Abus. Negl. 1991, 15, 279–291. [Google Scholar] [CrossRef]
- Danko, C.M.; Garbacz, L.L.; Budd, K.S. Outcomes of Parent-Child Interaction Therapy in an urban community clinic: A comparison of treatment completers and dropouts. Child. Youth Serv. Rev. 2016, 60, 42–51. [Google Scholar] [CrossRef]
- Fernandez, M.A.; Butler, A.M.; Eyberg, S.M. Treatment outcome for low socioeconomic status African American families in Parent-Child Interaction Therapy: A pilot study. Child Fam. Behav. Ther. 2011, 33, 32–48. [Google Scholar] [CrossRef]
- McCabe, K.; Yeh, M. Parent-Child Interaction Therapy for Mexican Americans: A randomized clinical trial. J. Clin. Child Adolesc. Psychol. 2009, 38, 753–759. [Google Scholar] [CrossRef]
- Chaffin, M.; Silovsky, J.F.; Funderburk, B.; Valle, L.A.; Brestan, E.V.; Balachova, T.; Jackson, S.; Lensgraf, J.; Bonner, B.L. Parent-Child Interaction Therapy with physically abusive parents: Efficacy for reducing future abuse reports. J. Consult. Clin. Psychol. 2004, 72, 500–510. [Google Scholar] [CrossRef] [Green Version]
- Whitcombe-Dobbs, S.; Tarren-Sweeney, M. What evidence is there that parenting interventions reduce child abuse and neglect among maltreating families? A systematic review. Dev. Child Welf. 2019, 1, 374–393. [Google Scholar] [CrossRef]
- Whitacre, K.B.; Foley, K.; Jackson, C.; Curtis, R.; McNeil, C.B. A Comparison of Child Abuse Potential Inventory and Parenting Stress Index with families in the Parent-Child Interaction Therapy and treatment as usual groups. Child Fam. Behav. Ther. 2020, 42, 169–185. [Google Scholar] [CrossRef]
- Villodas, M.T.; Moses, J.O.; Cromer, K.D.; Mendez, L.; Magariño, L.S.; Villodas, F.M.; Bagner, D.M. Feasibility and promise of community providers implementing home-based Parent-Child Interaction Therapy for families investigated for child abuse: A pilot randomized controlled trial. Child Abus. Negl. 2021, 117, 105063. [Google Scholar] [CrossRef] [PubMed]
- Lanier, P.; Kohl, P.L.; Benz, J.; Swinger, D.; Moussette, P.; Drake, B. Parent-Child Interaction Therapy in a community setting: Examining outcomes, attrition, and treatment setting. Res. Soc. Work Prac. 2011, 21, 689–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrahamse, M.E.; Niec, L.N.; Junger, M.; Boer, F.; Lindauer, R.J.L. Risk factors for attrition from an evidence-based parenting program: Findings from the Netherlands. Child. Youth Serv. Rev. 2016, 64, 42–50. [Google Scholar] [CrossRef]
- Boggs, S.R.; Eyberg, S.M.; Edwards, D.L.; Rayfield, A.; Jacobs, J.; Bagner, D.; Hood, K.K. Outcomes of Parent-Child Interaction Therapy: A comparison of treatment completers and study dropouts one to three years later. Child Fam. Behav. Ther. 2005, 26, 1–22. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Fortson, B.L. Predictors of treatment attrition and treatment length in Parent-Child Interaction Therapy in Taiwanese families. Child. Youth Serv. Rev. 2015, 59, 28–37. [Google Scholar] [CrossRef]
- Eyberg, S.M.; Funderburk, B. Parent-Child. Interaction Therapy Protocol; PCIT International: Gainesville, FL, USA, 2011. [Google Scholar]
- Heinrichs, N.; Bertram, H.; Kuschel, A.; Hahlweg, K. Parent recruitment and retention in a universal prevention program for child behavior and emotional problems: Barriers to research and program participation. Prev. Sci. 2005, 6, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Lavigne, J.V.; LeBailly, S.A.; Gouze, K.R.; Binns, H.J.; Keller, J.; Pate, L. Predictors and correlates of completing behavioral parent training for the treatment of Oppositional Defiant Disorder in pediatric primary care. Behav. Ther. 2010, 41, 198–211. [Google Scholar] [CrossRef] [Green Version]
- Masse, J.J.; McNeil, C.B. In-home Parent-Child Interaction Therapy: Clinical considerations. Child Fam. Behav. Ther. 2008, 30, 127–135. [Google Scholar] [CrossRef]
- Fowles, T.R.; Masse, J.J.; McGoron, L.; Beveridge, R.M.; Williamson, A.A.; Smith, M.A.; Parrish, B.P. Home-based vs. clinic-based Parent–Child Interaction Therapy: Comparative effectiveness in the context of dissemination and implementation. J. Child Fam. Stud. 2017, 27, 1115–1129. [Google Scholar] [CrossRef]
- Briss, P.A.; Zaza, S.; Pappaioanou, M.; Fielding, J.; Wright-De Agüero, L.; Truman, B.I.; Hopkins, D.P.; Mullen, P.D.; Thompson, R.S.; Woolf, S.H. Developing an evidence-based guide to community preventive services—methods. Am. J. Prev. Med. 2000, 18, 35–43. [Google Scholar] [CrossRef]
- Bagner, D.M.; Coxe, S.; Hungerford, G.M.; Garcia, D.; Barroso, N.E.; Hernandez, J.; Rosa-Olivares, J. Behavioral parent training in infancy: A window of opportunity for high-risk families. J. Abnorm. Child Psychol. 2016, 44, 901–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagner, D.M.; Rodríguez, G.M.; Blake, C.A.; Rosa-Olivares, J. Home-based preventive parenting intervention for at-risk infants and their families: An open trial. Cogn. Behav. Pract. 2013, 20, 334–348. [Google Scholar] [CrossRef] [Green Version]
- Galanter, R.; Self-Brown, S.; Valente, J.R.; Dorsey, S.; Whitaker, D.J.; Bertuglia-Haley, M.; Prieto, M. Effectiveness of Parent-Child Interaction Therapy delivered to at-risk families in the home setting. Child Fam. Behav. Ther. 2012, 34, 177–196. [Google Scholar] [CrossRef]
- Timmer, S.G.; Zebell, N.M.; Culver, M.A.; Urquiza, A.J. Efficacy of adjunct in-home coaching to improve outcomes in Parent-Child Interaction Therapy. Res. Social Work Prac. 2010, 20, 36–45. [Google Scholar] [CrossRef]
- Bakermans-Kranenburg, M.J.; Van IJzendoorn, M.H.; Juffer, F. Less is more: Meta-analyses of sensitivity and attachment interventions in early childhood. Psychol. Bull. 2003, 129, 195–215. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Abell, B.; Webb, H.J.; Avdagic, E.; Zimmer-Gembeck, M.J. Parent-Child Interaction Therapy: A meta-analysis. Pediatrics 2017, 140, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Abrahamse, M.E.; Junger, M.; Van Wouwe, M.A.M.; Boer, F.; Lindauer, R.J.L. Treating child disruptive behavior in high-risk families: A comparative effectiveness trial from a community-based implementation. J. Child Fam. Stud. 2016, 25, 1605–1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masse, J.J.; Quetsch, L.B.; McNeil, C.B. Taking PRIDE in your home: Implementing home-based Parent–Child Interaction Therapy (PCIT) with fidelity. In Handbook of Parent-Child Interaction Therapy; Niec, L.N., Ed.; Springer: Berlin, Germany, 2018; pp. 161–181. [Google Scholar]
- Ondersma, S.J.; Chaffin, M.J.; Mullins, S.M.; LeBreton, J.M. A brief form of the Child Abuse Potential Inventory: Development and validation. J. Clin. Child Adolesc. Psychol. 2005, 34, 301–311. [Google Scholar] [CrossRef] [PubMed]
- Milner, J.S. The Child Abuse Potential Inventory: Manual; Psytec Inc.: DeKalb, IL, USA, 1986. [Google Scholar]
- Grietens, H.; De Haene, L.; Uyttebroek, K. Cross-cultural validation of the Child Abuse Potential Inventory in Belgium (Flanders): Relations with demographic characteristics and parenting problems. J. Fam. Violence 2007, 22, 223–229. [Google Scholar] [CrossRef]
- Eyberg, S.M.; Pincus, D.B. Eyberg Child Behavior Inventory and Sutter-Eyberg Behavior Inventory-Revised: Professional Manual; Psychological Assessment Resources: Odessa, FL, USA, 1999. [Google Scholar]
- Abrahamse, M.E.; Junger, M.; Leijten, P.H.; Lindeboom, R.; Boer, F.; Lindauer, R.J.L. Psychometric properties of the Dutch Eyberg Child Behavior Inventory (ECBI) in a community sample and a multi-ethnic clinical sample. J. Psychopathol. Behav. Assess. 2015, 37, 679–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weeland, J.; van Aar, J.; Overbeek, G. Dutch Norms for the Eyberg Child Behavior Inventory: Comparisons with other Western Countries. J. Psychopathol. Behav. Assess. 2018, 40, 224–234. [Google Scholar] [CrossRef] [Green Version]
- Vermulst, A.; Kroes, G.; De Meyer, R.; Nguyen, L.; Veerman, J.W. Handleiding OBVL [Manual Parenting Stress Questionnaire]; Praktikon: Nijmegen, The Netherlands, 2015. [Google Scholar]
- Eyberg, S.M.; Nelson, M.M.; Ginn, N.C.; Bhuiyan, N.N.; Boggs, S.R. Manual for the Dyadic Parent–Child. Interaction Coding System; PCIT International: Gainesville, FL, USA, 2013. [Google Scholar]
- Eyberg, S.M. Assessing therapy outcome with preschool children: Progress and problems. J. Clin. Child Psychol. 1992, 21, 306–311. [Google Scholar] [CrossRef]
- Brestan, E.V.; Jacobs, J.R.; Rayfield, A.D.; Eyberg, S.M. A consumer satisfaction measure for parent-child treatments and its relation to measures of child behavior change. Behav. Ther. 1999, 30, 17–30. [Google Scholar] [CrossRef]
- Barnett, D.; Manly, J.T.; Cicchetti, D. Defining child maltreatment: The interface between policy and research. Child Abus. Child Dev. Soc. Policy 1993, 8, 7–73. [Google Scholar]
- Thomas, R.; Zimmer-Gembeck, M.J. Behavioral outcomes of Parent-Child Interaction Therapy and Triple P-Positive Parenting Program: A review and meta-analysis. J. Abnorm. Child Psychol. 2007, 35, 475–495. [Google Scholar] [CrossRef] [PubMed]
- Weisz, J.R.; Doss, A.J.; Hawley, K.M. Youth Psychotherapy Outcome Research: A Review and Critique of the Evidence Base. Annu. Rev. Psychol. 2005, 56, 337–363. [Google Scholar] [CrossRef] [Green Version]
- Van der Put, C.E.; Assink, M.; Boekhout van Solinge, N.F. Predicting child maltreatment: A meta-analysis of the predictive validity of risk assessment instruments. Child Abus. Negl. 2017, 73, 71–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Means (SD) or Percentages | ||||
|---|---|---|---|---|
| Total (N = 20) | IT (n = 10) | WL (n = 10) | p | |
| Child characteristics | ||||
| Age (years) | 5.7 (1.6) | 5.8 (1.9) | 5.6 (1.3) | 0.795 |
| Gender (% male) | 70.0 | 60.0 | 80.0 | 0.628 |
| Ethnicity (% non-Western) | 40.0 | 40.0 | 40.0 | 1.00 |
| Maltreatment history (% reported in client file) | 70.0 | 90.0 | 50.0 | 0.141 |
| Family characteristics | ||||
| Caregivers (% biological parent) | 70.0 | 40.0 | 100.0 | 0.011 * |
| Family status (% single-parent) | 40.0 | 30.0 | 50.0 | 0.650 |
| Family income (% poor or fair financial situation) | 45.0 | 20.0 | 70.0 | 0.070 |
| Therapy characteristics | ||||
| Dropout (% that not completed the 8-session protocol) | 15.0 | 10.0 | 20.0 | 1.00 |
| Baseline (T0) | Post-Test (T1/T01) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Measures | Group | n | M | SD | n | M | SD | F (1,10–14) | p | |
| Child behavior | ||||||||||
| ECBI Intensity | IT | 10 | 121.0 | 30.2 | 9 | 80.8 | 24.9 | 13.12 | 0.003 * | 0.502 |
| WL | 10 | 131.3 | 40.6 | 8 | 136.3 | 46.0 | ||||
| ECBI Problem | IT | 10 | 13.6 | 8.3 | 9 | 5.6 | 4.4 | 5.44 | 0.038 * | 0.312 |
| WL | 9 | 19.4 | 7.5 | 7 | 19.4 | 10.4 | ||||
| Child abuse potential | ||||||||||
| BCAP risk scale | IT | 10 | 2.2 | 1.7 | 9 | 1.0 | 1.3 | 0.78 | 0.392 | 0.057 |
| WL | 10 | 9.1 | 7.2 | 8 | 7.5 | 6.2 | ||||
| Parenting stress | ||||||||||
| OBVL-total (t-score) | IT | 10 | 59.9 | 11.7 | 9 | 48.7 | 8.3 | 2.46 | 0.141 | 0.159 |
| WL | 10 | 69.6 | 6.6 | 8 | 67.6 | 9.3 | ||||
| Parenting skills | ||||||||||
| DPICS % Positive Following | IT | 9 | 9.7 | 7.9 | 8 | 36.0 | 12.1 | 18.30 | <0.001 * | 0.604 |
| WL | 10 | 4.7 | 4.2 | 8 | 6.5 | 5.4 | ||||
| DPICS % Negative Leading | IT | 9 | 38.0 | 12.9 | 8 | 11.4 | 10.3 | 15.55 | <0.002 * | 0.564 |
| WL | 10 | 40.9 | 15.0 | 8 | 39.3 | 10.7 | ||||
| Pre-Test (T0/T01) | Post-Test (T1) | Follow-Up (T2) | Effect Size d | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Measures | Group | n | M | SD | M | SD | p (T0–T1) | n | M | SD | p (T1–T2) | Within-Group T0–T2 |
| Child behavior | ||||||||||||
| ECBI Intensity | IT | 9 | 116.2 | 27.7 | 80.8 | 24.9 | 0.001 * | 9 | 84.1 | 28.0 | 0.206 | 1.15 * |
| WL | 8 | 138.4 | 43.4 | 103.3 | 46.2 | 0.040 * | 5 | 101.2 | 28.6 | 0.698 | 1.01 * | |
| Total | 17 | 126.6 | 36.6 | 91.4 | 37.1 | <0.001 * | 14 | 90.2 | 28.4 | 0.310 | 1.65 * | |
| ECBI Problem | IT | 9 | 11.9 | 6.7 | 5.6 | 4.4 | 0.030 * | 9 | 3.9 | 3.1 | 0.236 | 1.53 * |
| WL | 8 | 18.6 | 9.9 | 10.8 | 6.6 | 0.029 * | 5 | 12.8 | 5.1 | 0.675 | 0.74 * | |
| Total | 17 | 15.1 | 8.8 | 8.0 | 6.0 | 0.001 * | 14 | 7.1 | 5.8 | 0.396 | 1.07 * | |
| Child abuse potential | ||||||||||||
| BCAP risk scale | IT | 9 | 2.1 | 1.8 | 1.0 | 1.3 | 0.030 * | 8 | 1.3 | 1.8 | 0.763 | −0.44 * |
| WL | 8 | 7.3 | 6.3 | 7.1 | 6.1 | 0.912 | 5 | 7.6 | 6.8 | 0.178 | −0.05 | |
| Total | 17 | 4.5 | 5.1 | 3.9 | 5.2 | 0.261 | 13 | 3.7 | 5.3 | 0.387 | 0.15 * | |
| Parenting stress | ||||||||||||
| OBVL-total | IT | 9 | 58.3 | 11.2 | 48.7 | 8.3 | 0.006 * | 8 | 49.1 | 12.3 | 0.964 | 0.78 * |
| WL | 8 | 67.1 | 9.3 | 65.1 | 12.0 | 0.629 | 5 | 65.8 | 13.3 | 0.553 | 0.11 | |
| Total | 17 | 62.5 | 11.1 | 56.4 | 13.0 | 0.025 * | 13 | 55.5 | 14.8 | 0.926 | 0.54 * | |
| Parenting skills | ||||||||||||
| DPICS % Positive Following | IT | 8 | 8.3 | 7.3 | 36.0 | 12.1 | <0.001 * | 8 | 31.3 | 15.6 | 0.269 | −1.89 * |
| WL | 7 | 5.5 | 4.0 | 25.0 | 22.4 | 0.052 * | 4 | 26.5 | 27.0 | 0.340 | −1.09 | |
| Total | 15 | 7.0 | 5.9 | 30.9 | 17.9 | <0.001 * | 12 | 29.7 | 18.9 | 0.690 | −1.62 * | |
| DPICS % Negative Leading | IT | 8 | 38.5 | 13.6 | 11.4 | 10.3 | <0.001 * | 8 | 17.0 | 11.8 | 0.035* | 1.69 * |
| WL | 7 | 39.3 | 10.7 | 23.2 | 16.7 | 0.132 | 4 | 15.1 | 11.0 | 0.419 | 2.23 * | |
| Total | 15 | 37.7 | 12.0 | 16.9 | 14.5 | <0.001 * | 12 | 16.3 | 11.1 | 0.987 | 1.85 * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abrahamse, M.E.; Tsang, V.M.W.; Lindauer, R.J.L. Home-Based Parent–Child Interaction Therapy to Prevent Child Maltreatment: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 8244. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168244
Abrahamse ME, Tsang VMW, Lindauer RJL. Home-Based Parent–Child Interaction Therapy to Prevent Child Maltreatment: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(16):8244. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168244
Chicago/Turabian StyleAbrahamse, Mariëlle E., Vionna M. W. Tsang, and Ramón J. L. Lindauer. 2021. "Home-Based Parent–Child Interaction Therapy to Prevent Child Maltreatment: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 16: 8244. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168244