
Mercury Exposure in Munduruku Indigenous Communities from Brazilian Amazon: Methodological Background and an Overview of the Principal Results

 , , , ,
, , , ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research’s Background
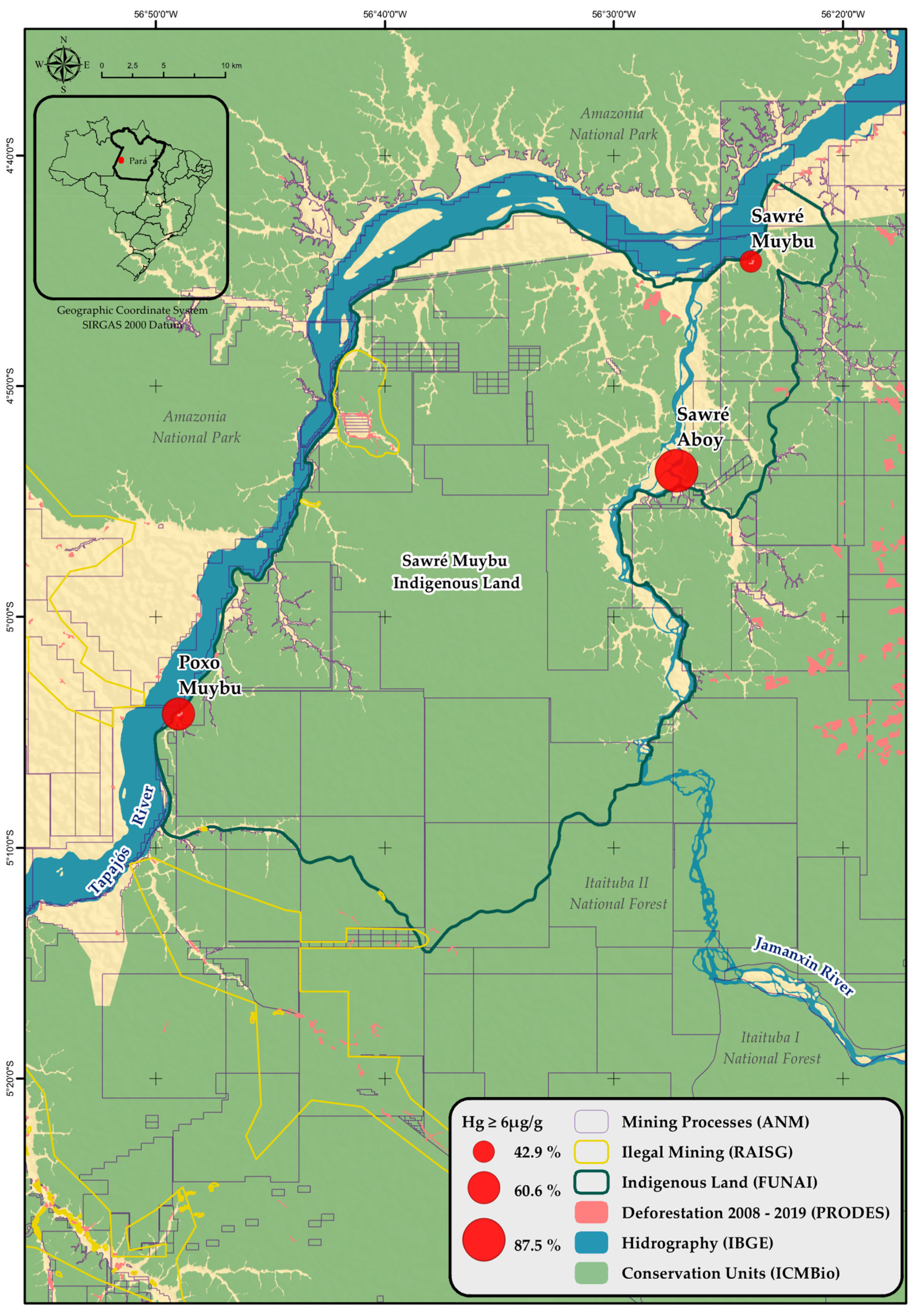
2.2. Population and Study Area
2.3. Study Design
2.4. Fieldwork Steps
2.5. Sociodemographic Characterization
- (a)
- The first section (head of household’s data) characterizes the physical and demographic structure of the homes visited, including the length of residence, materials used for building the house, sources of drinking water and presence of bathroom, occupational activities, income, social benefits, number of years in education for the head of household, and the dietary pattern of inhabitants, with an emphasis on fish consumption.
- (b)
- The second section (family members’ data) characterizes the health of the family and the community, including a history of previous hospitalizations; previous Malaria treatment, and history of contact with mercury from garimpos.
- (c)
- The third section (women’s health data) questionnaire addressed reproductive history, the number of children, pregnant, and breastfeeding status.
- (d)
- The fourth section (children’s data) explores the birth conditions, access to pediatric health care, previous hospitalizations, recent history of diarrhea and acute respiratory infection, and vaccination history.
2.6. Health Assessment
- (1)
- Anthropometric Measurements
- (b)
- Hemoglobin Dosage
- (c)
- Glucose Dosage
- (d)
- Blood Pressure Measurement
- (e)
- Prevalence of Sexually Transmitted Diseases
- (f)
- Neurological Evaluation
- (g)
- Pediatric Evaluation
2.7. Genetic Polymorphism Analysis
2.8. Determination of Mercury Levels
- (a)
- Hair Samples
- (b)
- Fish Samples
2.9. Health Risk Assessment
2.10. Statistical Analysis
3. Results
3.1. Principal Research Results
3.1.1. Sociodemographic Characterization
3.1.2. Health Assessment
3.1.3. Anthropometric Measurements
3.1.4. Hemoglobin Levels
3.1.5. Glucose Levels
3.1.6. Blood Pressure Levels
3.1.7. Sexually Transmitted Diseases
3.1.8. Neurological Evaluation
3.1.9. Pediatric Evaluation
3.1.10. Genetic Polymorphism Analysis
3.2. Determination of Mercury Levels
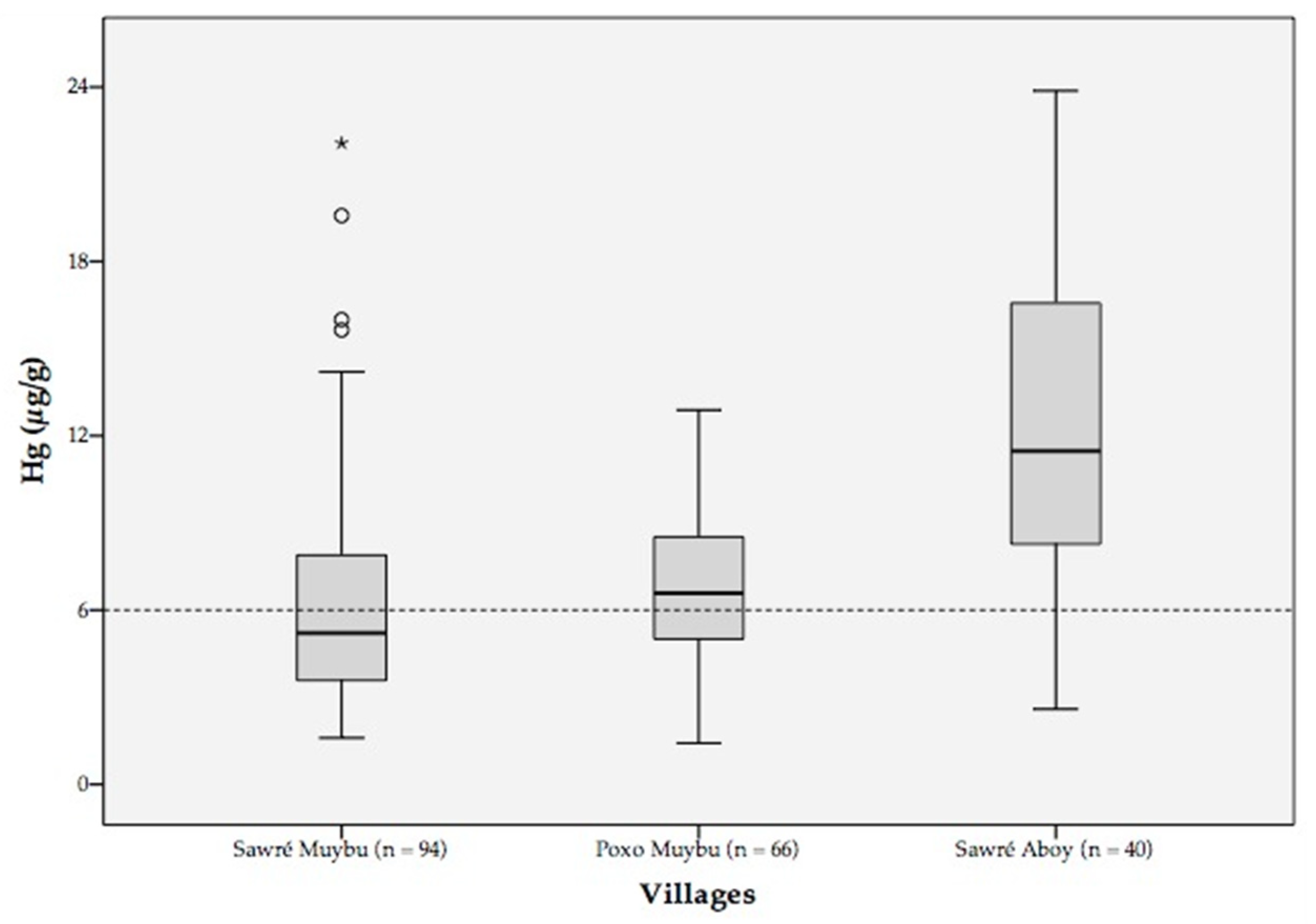
3.2.1. Hair Samples
3.2.2. Fish Samples
3.3. Health Risk Assessment
4. Discussion
5. Conclusions
- (a)
- The immediate interruption of illegal mining activities and cessation of invasion of traditional and protected lands of the Amazon.
- (b)
- In parallel, to develop a national plan to discontinue mercury use in artisanal mining to achieve the goals of the Minamata Convention on Mercury.
- (c)
- To develop a risk management plan (RMP) for populations chronically exposed to mercury. The plan should contain a set of integrated guidelines and actions, such as:
- (i)
- to expand the monitoring of mercury levels in fish consumed not only in traditional territories but also in urban areas of the Amazon.
- (ii)
- to develop educational material for the population of the affected areas, containing clear information on safe fish consumption, respecting cultural aspects related to different ethnic groups.
- (iii)
- to include testing of mercury levels in hair samples in the routine of the prenatal care program and in the program for monitoring child growth and development, in the Brazilian Unified Health System (SUS).
- (iv)
- to develop a Basic Care Protocol for Contaminated People to be equally incorporated into the SUS.
- (v)
- to promote a research and scientific development program to carry out more in-depth studies to enhance the knowledge about the health impacts of Amazon populations chronically exposed to mercury.
- (vi)
- to formulate public policies to create sustainable economic alternatives for indigenous communities affected by illegal mining in order to guarantee food security, sovereignty, and respect for ancestral traditions.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morel, F.M.; Kraepiel, A.M.; Amyot, M. The chemical cycle and bioaccumulation of mercury. Annu. Rev. Ecol. Syst. 1998, 29, 543–566. [Google Scholar] [CrossRef] [Green Version]
- Malm, O. Gold mining as a source of mercury exposure in the Brazilian Amazon. Environ. Res. 1998, 77, 73–78. [Google Scholar] [CrossRef]
- Mason, R.P.; Fitzgerald, W.F.; Morel, F.M. The biogeochemical cycling of elemental mercury: Anthropogenic influences. Geochim. Cosmochim. Acta 1994, 58, 3191–3198. [Google Scholar] [CrossRef]
- Clifton II, J.C. Mercury exposure and public health. Pediatr. Clin. N. Am. 2007, 54, 237.e1–237.e45. [Google Scholar] [CrossRef] [PubMed]
- Passos, C.J.; Mergler, D. Human mercury exposure and adverse health effects in the Amazon: A review. Cad. Saúde Pública 2008, 24, s503–s520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bose-O’Reilly, S.; McCarty, K.M.; Steckling, N.; Lettmeier, B. Mercury exposure and children’s health. Curr. Probl. Pediatr. Adolesc. Health Care 2010, 40, 186–215. [Google Scholar] [CrossRef] [Green Version]
- Pfeiffer, W.C.; de Lacerda, L.D. Mercury inputs into the Amazon region, Brazil. Environ. Technol. 1988, 9, 325–330. [Google Scholar] [CrossRef]
- Martinelli, L.A.; Ferreira, J.R.; Forsberg, B.R.; Victoria, R.L. Mercury contamination in the Amazon: A gold rush consequence. Ambio 1988, 17, 252–254. [Google Scholar]
- Cleary, D. An Anatomy of a Gold Rush: Garimpagem in the Brazilian Amazon. Ph.D. Thesis, University of Oxford, Oxford, UK, 1989. [Google Scholar]
- Lacerda, L.D.; Pfeiffer, W.C. Mercury from gold mining in the Amazon environment: An overview. Química Nova 1992, 15, 155–160. [Google Scholar]
- Pfeiffer, W.C.; Lacerda, L.D.; Salomons, W.; Malm, O. Environmental fate of mercury from gold mining in the Brazilian Amazon. Environ. Rev. 1993, 1, 26–37. [Google Scholar] [CrossRef]
- Akagi, H.; Naganuma, A. Human exposure to mercury and the accumulation of methylmercury that is associated with gold mining in the Amazon Basin, Brazil. J. Health Sci. 2000, 46, 323–328. [Google Scholar] [CrossRef] [Green Version]
- Roulet, M.; Lucotte, M.; Canuel, R.; Farella, N.; Courcelles, M.; Guimaraes, J.R.; Mergler, D.; Amorim, M. Increase in mercury contamination recorded in lacustrine sediments following deforestation in the central Amazon. Chem. Geol. 2000, 165, 243–266. [Google Scholar] [CrossRef]
- Lino, A.S.; Kasper, D.; Guida, Y.S.; Thomaz, J.R.; Malm, O. Total and methyl mercury distribution in water, sediment, plankton and fish along the Tapajós River basin in the Brazilian Amazon. Chemosphere 2019, 235, 690–700. [Google Scholar] [CrossRef]
- Teixeira, R.A.; da Silveira Pereira, W.V.; de Souza, E.S.; Ramos, S.J.; Dias, Y.N.; de Lima, M.W.; de Souza Neto, H.F.; de Oliveira, E.S.; Fernandes, A.R. Artisanal gold mining in the eastern Amazon: Environmental and human health risks of mercury from different mining methods. Chemosphere 2021, 284, 131220. [Google Scholar] [CrossRef]
- Khoury, E.D.; Souza, G.D.; da Costa, C.A.; de Araújo, A.A.; de Oliveira, C.S.; Silveira, L.C.; Pinheiro, M.D. Somatosensory psychophysical losses in inhabitants of riverside communities of the Tapajós River Basin, Amazon, Brazil: Exposure to methylmercury is possibly involved. PLoS ONE 2015, 10, e0144625. [Google Scholar] [CrossRef]
- dos Santos Freitas, J.; Lacerda, E.M.; da Silva Martins, I.C.; Rodrigues, D., Jr.; Bonci, D.M.; Cortes, M.I.; Corvelo, T.C.; Ventura, D.F.; de Lima Silveira, L.C.; Pinheiro, M.D.; et al. Cross-sectional study to assess the association of color vision with mercury hair concentration in children from Brazilian Amazonian riverine communities. Neurotoxicology 2018, 65, 60–67. [Google Scholar] [CrossRef]
- Domingues, M.M.; Cury, E.D.; de Araújo, A.A.; Junior, J.M.; Pinheiro, M.D. Somatosensory psychophysic losses in inhabitants of riverside communities of the Tapajós river basin, Amazonas, Brazil: The possible involvement of exposure to methylmercury. J. Neurol. Sci. 2019, 405, 255–256. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, M.D.; Oikawa, T.; Vieira, J.L.; Gomes, M.S.; Guimarães, G.D.; Crespo-López, M.E.; Müller, R.C.; Amoras, W.W.; Ribeiro, D.R.; Rodrigues, A.R.; et al. Comparative study of human exposure to mercury in riverside communities in the Amazon region. Braz. J. Med. Biol. Res. 2006, 39, 411–414. [Google Scholar] [CrossRef] [Green Version]
- Marinho, J.S.; Lima, M.O.; Santos, E.C.; de Jesus, I.M.; Pinheiro, M.D.; Alves, C.N.; Muller, R.C. Mercury speciation in hair of children in three communities of the Amazon, Brazil. BioMed. Res. Int. 2014, 2014, 945963. [Google Scholar] [CrossRef]
- Mapa inédito Indica Epidemia de Garimpo Ilegal na Panamazônia—RAISG. Available online: https://www.amazoniasocioambiental.org/pt-br/radar/mapa-inedito-indica-epidemia-de-garimpo-ilegal-na-panamazonia/ (accessed on 14 June 2021).
- Cerdeira, R.G.P.; Ruffino, M.L.; Isaac, V.J. Consumo de Pescado e Outros Alimentos Pela População Ribeirinha do Lago Grande de Monte Alegre, PA-Brasil. Acta Amaz. 1997, 27, 213–227. [Google Scholar] [CrossRef] [Green Version]
- Santos, G.M.D.; Santos, A.C.M.D. Sustentabilidade da pesca na Amazônia. Estud. Avançados 2005, 19, 165–182. [Google Scholar] [CrossRef] [Green Version]
- Arruda, M.C.F.D. Avaliação dos Indicadores da Política de pesca do Programa Zona Franca Verde: Perspectivas Econômicas e Ambientais. Dissertação de Mestrado, Programa de Pós-Graduação em Engenharia de Produção, Universidade Federal do Amazonas (UFAM), Manaus, Brasil, 2017. Available online: https://tede.ufam.edu.br/handle/tede/6068 (accessed on 19 June 2021).
- Joint FAO/WHO Expert Committee on Food Additives, Meeting, & World Health Organization. Evaluation of Certain Food Additives and Contaminants: Sixty First Report of the Joint FAO/WHO Expert Committee on Food Additives), Rome 10, 19 June 2003. 2003. Available online: ftp://ftp.org/es/esn/jecfa/jecfa61sc.pdf (accessed on 17 June 2021).
- U.S. EPA. Reference Dose for Methylmercury (External Review Draft, 2000); NCEA-S-0930; U.S. Environmental Protection Agency: Washington, DC, USA. Available online: https://www.regulations.gov/document/EPA-HQ-OAR-2018-0794-0006 (accessed on 18 June 2021).
- Crespo-Lopez, M.E.; Augusto-Oliveira, M.; Lopes-Araújo, A.; Santos-Sacramento, L.; Takeda, P.Y.; Macchi, B.D.M.; Nascimento, J.L.M.D.; Maia, C.S.; Lima, R.R.; Arrifano, G.P. Mercury: What Can We Learn Amazon? Environ. Int. 2021, 146, 106223. [Google Scholar] [CrossRef]
- Bakir, F.; Damluji, S.F.; Amin-Zaki, L.; Murtadha, M.; Khalidi, A.; Al-Rawi, N.Y.; Tikriti, S.; Dhahir, H.I.; Clarkson, T.W.; Smith, J.C.; et al. Methylmercury poisoning in Iraq. Science 1973, 181, 230–241. [Google Scholar] [CrossRef]
- Akagi, H.; Grandjean, P.; Takizawa, Y.; Weihe, P. Methylmercury dose estimation from umbilical cord concentrations in patients with Minamata disease. Environ. Res. 1998, 77, 98–103. [Google Scholar] [CrossRef]
- Ceccatelli, S.; Daré, E.; Moors, M. Methylmercury-induced neurotoxicity and apoptosis. Chem.-Biol. Interact. 2010, 188, 301–308. [Google Scholar] [CrossRef]
- Lechler, P.J.; Miller, J.R.; Lacerda, L.D.; Vinson, D.; Bonzongo, J.C.; Lyons, W.B.; Warwick, J.J. Elevated mercury concentrations in soils, sediments, water, and fish of the Madeira River basin, Brazilian Amazon: A function of natural enrichments? Sci. Total Environ. 2000, 260, 87–96. [Google Scholar] [CrossRef]
- Rodríguez Martín-Doimeadios, R.C.; Berzas Nevado, J.J.; Guzmán Bernardo, F.J.; Jiménez Moreno, M.; Arrifano, G.P.F.; Herculano, A.M.; Nascimento, J.L.M.D.; Crespo-López, M.E. Comparative study of mercury speciation in commercial fishes of the Brazilian Amazon. Environ. Sci. Pollut. Res. 2014, 21, 7466–7479. [Google Scholar] [CrossRef] [PubMed]
- Souza-Araujo, J.; Giarrizzo, T.; Lima, M.O.; Souza, M.B.G. Mercury and methyl mercury in fishes from Bacajá River (Brazilian Amazon): Evidence for bioaccumulation and biomagnification. J. Fish Biol. 2016, 89, 249–263. [Google Scholar] [CrossRef]
- Lino, A.S.; Kasper, D.; Guida, Y.S.; Thomaz, J.R.; Malm, O. Mercury and selenium in fishes from the Tapajós River in the Brazilian Amazon: An evaluation of human exposure. J. Trace Elements Med. Biol. 2018, 48, 196–201. [Google Scholar] [CrossRef]
- Guimaraes, J.R.D.; Roulet, M.; Lucotte, M.; Mergler, D. Mercury methylation along a lake–forest transect in the Tapajós river floodplain, Brazilian Amazon: Seasonal and vertical variations. Sci. Total Environ. 2000, 261, 91–98. [Google Scholar] [CrossRef]
- Albuquerque, F.E.A.; Minervino, A.H.H.; Miranda, M.; Herrero-Latorre, C.; Barrêto Júnior, R.A.; Oliveira, F.L.C.; Sucupira, M.C.A.; Ortolani, E.L.; López-Alonso, M. Toxic and essential trace element concentrations in fish species in the Lower Amazon, Brazil. Sci. Total Environ. 2020, 732, 138983. [Google Scholar] [CrossRef] [PubMed]
- Hacon, S.D.S.; Oliveira-Da-Costa, M.; Gama, C.D.S.; Ferreira, R.; Basta, P.C.; Schramm, A.; Yokota, D. Mercury exposure through fish consumption in traditional communities in the Brazilian Northern Amazon. Int. J. Environ. Res. Public Health 2020, 17, 5269. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, L.S.; Pestana, I.A.; Almeida, M.G.; Ferreira da Costa Nery, A.; Bastos, W.R.; Magalhães Souza, C.M. Mercury biomagnification in an ichthyic food chain of an amazon floodplain lake (Puruzinho Lake): Influence of seasonality and food chain modeling. Ecotoxicol. Environ. Saf. 2021, 207, 111249. [Google Scholar] [CrossRef] [PubMed]
- Akagi, H.; Malm, O.; Branches, F.J.P.; Kinjo, Y.; Kashima, Y.; Guimaraes, J.R.D.; Oliveira, R.B.; Haraguchi, K.; Pfeiffer, W.C.; Takizawa, Y.; et al. Human exposure to mercury due to goldmining in the Tapajos River Basin, Amazon, Brazil: Speciation of mercury in human hair, blood and urine. Water Air Soil Pollut. 1995, 80, 85–94. [Google Scholar] [CrossRef]
- Lebel, J.; Roulet, M.; Mergler, D.; Lucotte, M.; Larribe, F. Fish diet and mercury exposure in a riparian Amazonian population. Water Air Soil Pollut. 1997, 97, 31–44. [Google Scholar] [CrossRef]
- Malm, O.; Branches, F.J.; Akagi, H.; Castro, M.B.; Pfeiffer, W.C.; Harada, M.; Bastos, W.R.; Kato, H. Mercury and methylmercury in fish and human hair from the Tapajos river basin, Brazil. Sci. Total Environ. 1995, 175, 141–150. [Google Scholar] [CrossRef]
- de Souza Lima, A.P.; Müller, R.C.S.; de Souza Sarkis, J.E.; Alves, C.N.; da Silva Bentes, M.H.; Brabo, E.; de Oliveira Santos, E. Mercury contamination in fish from Santarém, Pará, Brazil. Environ. Res. 2000, 83, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Passos, C.J.S.; Da Silva, D.S.; Lemire, M.; Fillion, M.; Guimaraes, J.R.D.; Lucotte, M.; Mergler, D. Daily mercury intake in fish-eating populations in the Brazilian Amazon. J. Expo. Sci. Environ. Epidemiol. 2008, 18, 76–87. [Google Scholar] [CrossRef]
- Gimenes, T.C.; Penteado, J.O.; dos Santos, M.; da Silva Júnior, F.M.R. Methylmercury in Fish from the Amazon Region—A Review Focused on Eating Habits. Water Air Soil Pollut. 2021, 232, 1–9. [Google Scholar] [CrossRef]
- FAO/WHO. Joint FAO/WHO Expert Committee on Food Additives (JECFA), Report of the Tenth Section, Rotterdam, The Netherlands 4 to 8 April 2016. Available online: http://www.fao.org/fao-who-codexalimentarius/sh-proxy/en/?lnk=1&url=https%253A%252F%252Fworkspace.fao.org%252Fsites%252Fcodex%252FMeetings%252FCX-735-10%252FReport%252FREP16_CFe.pdf (accessed on 22 June 2020).
- Berzas Nevado, J.J.; Rodríguez Martín-Doimeadios, R.C.; Guzmán Bernardo, F.J.; Jiménez Moreno, M.; Herculano, A.M.; do Nascimento, J.L.M.; Crespo-López, M.E. Mercury in the Tapajós River basin, Brazilian Amazon: A review. Environ. Int. 2010, 36, 593–608. [Google Scholar] [CrossRef]
- Santos Serrão de Castro, N.; de Oliveira Lima, M. Hair as a biomarker of long term mercury exposure in Brazilian Amazon: A systematic review. Int. J. Environ. Res. Public Health 2018, 15, 500. [Google Scholar] [CrossRef] [Green Version]
- Arrifano, G.P.; Martín-Doimeadios, R.C.; Jiménez-Moreno, M.; Ramírez-Mateos, V.; da Silva, N.F.; Souza-Monteiro, J.R.; Augusto-Oliveira, M.; Paraense, R.S.; Macchi, B.M.; do Nascimento, J.L.; et al. Large-scale projects in the amazon and human exposure to mercury: The case-study of the Tucuruí Dam. Ecotoxicol. Environ. Saf. 2018, 147, 299–305. [Google Scholar] [CrossRef]
- Kelly, C.A.; Rudd, J.W.M.; Bodaly, R.A.; Roulet, N.P.; StLouis, V.L.; Heyes, A.; Moore, T.R.; Schiff, S.; Aravena, R.; Scott, K.J.; et al. Increases in fluxes of greenhouse gases and methyl mercury following flooding of an experimental reservoir. Environ. Sci. Technol. 1997, 31, 1334–1344. [Google Scholar] [CrossRef]
- Gomes, V.M.; dos Santos, A.; Zara, L.F.; Ramos, D.D.; Forti, J.C.; Ramos, D.D.; Santos, F.A. Study on mercury methylation in the Amazonian rivers in flooded areas for hydroelectric use. Water Air Soil Pollut. 2019, 230, 211. [Google Scholar] [CrossRef]
- Palermo, E.F.A.; Kasper, D.; Reis, T.S.; Nogueira, S.; Branco, C.W.C.; Malm, O. Mercury level increase in fish tissues downstream the Tucuruí reservoir, Brazil. RMZ-M&G 2004, 51, 1292–1294. [Google Scholar]
- Forsberg, B.R.; Melack, J.M.; Dunne, T.; Barthem, R.B.; Goulding, M.; Paiva, R.C.D.; Sorribas, M.V.; Silva, U.L., Jr.; Weisser, S. The potential impact of new Andean dams on Amazon fluvial ecosystems. PLoS ONE 2017, 12, e0182254. [Google Scholar] [CrossRef] [PubMed]
- Pestana, I.A.; Azevedo, L.S.; Bastos, W.R.; de Souza, C.M.M. The impact of hydroelectric dams on mercury dynamics in South America: A review. Chemosphere 2019, 219, 546–556. [Google Scholar] [CrossRef]
- Vasconcellos, A.C.; Barrocas, P.R.; Ruiz, C.M.; Mourão, D.D.; Hacon, S.D. Burden of mild mental retardation attributed to prenatal methylmercury exposure in amazon: Local and regional estimates. Cienc E Saude Coletiva 2018, 23, 3535–3545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poulin, J.; Gibb, H.; Prüss-Üstün, A.; World Health Organization. Mercury: Assessing the Environmental Burden of Disease at National and Local Levels; World Health Organization: Geneva, Switzerland, 2008; 60p. [Google Scholar]
- Reuben, A.; Frischtak, H.; Berky, A.; Ortiz, E.J.; Morales, A.M.; Hsu-Kim, H.; Pendergast, L.L.; Pan, W.K. Elevated Hair Mercury Levels Are Associated With Neurodevelopmental Deficits in Children Living Near Artisanal and Small-Scale Gold Mining in Peru. GeoHealth 2020, 4, e2019GH000222. [Google Scholar] [CrossRef]
- Marques, R.C.; Bernardi, J.V.E.; Abreu, L.; Dórea, J.G. Neurodevelopment Outcomes in Children Exposed to Organic Mercury from Multiple Sources in a Tin-Ore Mine Environment in Brazil. Arch Environ. Contam. Toxicol. 2015, 68, 432–441. [Google Scholar] [CrossRef]
- Marques, R.C.; Bernardi, J.V.E.; Cunha, M.P.L.; Dórea, J.G. Impact of organic mercury exposure and home delivery on neurodevelopment of Amazonian children. Int. J. Hyg. Environ. Health 2016, 219, 498–502. [Google Scholar] [CrossRef] [PubMed]
- Junior, J.M.F.C.; Da Silva Lima, A.A.; Junior, D.R.; Khoury, E.D.T.; Da Silva Souza, G.; De Lima Silveira, L.C.; Pinheiro, M.D.C.N. Manifestações emocionais e motoras de ribeirinhos expostos ao mercúrio na Amazônia. Rev. Bras. Epidemiol. 2017, 20, 212–224. [Google Scholar] [CrossRef] [Green Version]
- Lacerda, E.M.D.C.B.; Souza, G.D.S.; Cortes, M.I.T.; Rodrigues, A.R.; Pinheiro, M.C.N.; Silveira, L.C.D.L.; Ventura, D.F. Comparison of Visual Functions of Two Amazonian Populations: Possible Consequences of Different Mercury Exposure. Front. Neurosci. 2020, 13, 1428. [Google Scholar] [CrossRef] [Green Version]
- Aaseth, J.; Wallace, D.R.; Vejrup, K.; Alexander, J. Methylmercury and developmental neurotoxicity: A global concern. Curr. Opin. Toxicol. 2020, 19, 80–87. [Google Scholar] [CrossRef]
- Kishi, R. Impacts of Developmental Exposure to Environmental Chemicals on Human Health with Global Perspectives. In Health Impacts of Developmental Exposure to Environmental Chemicals; Springer: Singapore, 2020; pp. 3–22. [Google Scholar] [CrossRef]
- Da Silva Brabo, E.; De Oliveira Santos, E.; Maura De Jesus, I.; Fernando Silva Mascarenhas, A.; De Freitas Faial, K. Mercury contamination of fish and exposures of an indigenous community in Para state, Brazil. In Environmental Research; Academic Press Inc.: Cambridge, MA, USA, 2000; pp. 197–203. [Google Scholar]
- Dórea, J.G.; Barbosa, A.C.; Ferrari, Í.; de Souza, J.R. Fish consumption (hair mercury) and nutritional status of Amazonian Amer-Indian children. Am. J. Hum. Biol. 2005, 17, 507–514. [Google Scholar] [CrossRef]
- Telmer, K.; Costa, M.; Angélica, R.S.; Araujo, E.S.; Maurice, Y. The source and fate of sediment and mercury in the Tapajós River, Pará, Brazilian Amazon: Ground- and space-based evidence. J. Environ. Manag. 2006, 81, 101–113. [Google Scholar] [CrossRef]
- Brabo, E.D.; Santos, E.D.; Jesus, I.M.; Mascarenhas, A.F.; Faial, K.F. Mercury levels in fish consumed by the Sai Cinza indigenous community, Munduruku Reservation, Jacareacanga County, State of Pará, Brazil. Cad Saúde Pública/Ministério Da Saúde Fundação Oswaldo Cruz Esc Nac Saúde Pública 1999, 15, 325–331. [Google Scholar] [CrossRef] [Green Version]
- de Oliveira Santos, E.C.; de Jesus, I.M.; Camara, V.D.; Brabo, E.; Loureiro, E.C.; Mascarenhas, A.; Weirich, J.; Luiz, R.R.; Cleary, D. Mercury exposure in Munduruku Indians from the community of Sai Cinza, State of Pará, Brazil. Environ. Res. 2002, 90, 98–103. [Google Scholar] [CrossRef] [Green Version]
- Dórea, J.G.; De Souza, J.R.; Rodrigues, P.; Ferrari, Í.; Barbosa, A.C. Hair mercury (signature of fish consumption) and cardiovascular risk in Munduruku and Kayabi Indians of Amazonia. Environ. Res. 2005, 97, 209–219. [Google Scholar] [CrossRef]
- WHO. Toxicological Evaluation of Certain Food Additives and Contaminants; WHO Food Additives Series, No. 24; Cambridge University Press: Cambridge, UK, 1989. [Google Scholar]
- Siqueira-Gay, J.; Soares-Filho, B.; Sanchez, L.E.; Oviedo, A.; Sonter, L.J. Proposed Legislation to Mine Brazil’s Indigenous Lands Will Threaten Amazon Forests and Their Valuable Ecosystem Services. One Earth 2020, 3, 356–362. [Google Scholar] [CrossRef]
- The Guardian. Brazilian Wildcat Miners Attack Police and Burn Indigenous Homes in Amazon [Internet]. 2021. Available online: https://www.theguardian.com/world/2021/may/28/brazil-wildcat-miners-police-indigenous-amazon (accessed on 31 May 2021).
- Henrique, M.C.; Oliveira RM, D. Os ‘cortadores de cabeças’: A memória como patrimônio dos Munduruku. Boletim do Museu Paraense Emílio Goeldi. Ciências Hum. 2021, 16, e20200049. [Google Scholar] [CrossRef]
- Munduruku—Povos Indígenas no Brasil. Available online: https://pib.socioambiental.org/pt/Povo:Munduruku (accessed on 14 June 2021).
- Hacon, S.; Rochedo, E.R.; Campos, R.R.; Lacerda, L.D. Mercury exposure through fish consumption in the urban area of Alta Floresta in the Amazon Basin. J. Geochem. Explor. 1997, 58, 209–216. [Google Scholar] [CrossRef]
- Hacon, S.; Yokoo, E.; Valente, J.; Campos, R.; Da Silva, V.; De Menezes, A.; De Moraes, L.; Ignotti, E. Exposure to mercury in pregnant women from Alta Floresta—Amazon Basin, Brazil. Environ. Res. 2000, 84, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Vega, C.M.; Orellana, J.D.Y.; Oliveira, M.W.; Hacon, S.S.; Basta, P.C. Human Mercury Exposure in Yanomami Indigenous Villages from the Brazilian Amazon. Int. J. Environ. Res. Public Health 2018, 15, 1051. [Google Scholar] [CrossRef] [Green Version]
- WHO. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development. 2006. Available online: https://www.who.int/publications/i/item/924154693X (accessed on 14 June 2021).
- Rosenfeld, L.G.; Malta, D.C.; Szwarcwald, C.L.; Bacal, N.S.; Cuder, M.A.; Pereira, C.A.; Figueiredo, A.W.; Silva, A.G.; Machado, Í.E.; Silva, W.A.; et al. Reference values for blood count laboratory tests in the Brazilian adult population, national health survey. Rev. Bras. Epidemiol. 2019, 22, E190003-SUPL. [Google Scholar]
- Barroso, W.K.; Rodrigues, C.I.; Bortolotto, L.A.; Mota-Gomes, M.A.; Brandão, A.A.; Feitosa, A.D.; Machado, C.A.; Poli-de-Figueiredo, C.E.; Amodeo, C.; Mion, D.; et al. Diretrizes Brasileiras de Hipertensão Arterial–2020. Arq. Bras. Cardiol. 2021, 116, 516–658. [Google Scholar] [CrossRef]
- Oliveira, R.; Pinto, B.; Resende, B.; Ciampi de Andrade, D.; Basta, P. Neurological impacts of chronic methylmercury exposure in Munduruku indigenous adults: Somatosensory, motor and cognitive abnormalities. Int. J. Environ. Res. Public Health 2021, 18, in press. [Google Scholar]
- Hofer, C.B.; Périssé, A.R.S.; Vasconcellos, A.C.S.; Viana, P.V.; Kempton, J.W.; Lima, M.O.; Jesus, I.M.; Hacon, S.S.; Basta, P.C. Munduruku Indigenous children health’s in the Tapajos River basin: Situational diagnosis and impacts of chronic mercury exposure. Int. J. Environ. Res. Public Health 2021, 18, in press. [Google Scholar]
- Perini, J.A.; Petzl-Erler, M.L.; Tsuneto, L.T.; Suarez-Kurtz, G. VKORC1 polymorphisms in Amerindian populations of Brazil. Pharmacogenomics 2008, 9, 1623–1629. [Google Scholar] [CrossRef] [PubMed]
- Lopes, L.R.; de Miranda, V.A.R.; Guimarães, J.A.M.; Souza, G.G.D.A.; Wainchtock, V.S.; Neto, J.A.G.; Goes, R.D.A.; Perini, J.A. Association of TNF-α-308G > A polymorphism with susceptibility to tendinopathy in athletes: A case–control study. BMC Sports Sci. Med. Rehabil. 2021, 13, 51. [Google Scholar] [CrossRef]
- Akagi, H.; Suzuki, T.; Arimura, K.; Ando, T.; Sakamoto, M.; Satoh, H.; Matsuyama, A. Mercury Analysis Manual, 105th ed.; Ministry of the Environmental: Tokyo, Japan, 2004; Available online: http://nimd.env.go.jp/kenkyu/docs/march_mercury_analysis_manual(e).pdf (accessed on 21 November 2019).
- Bastos, W.R.; Gomes, J.P.O.; Oliveira, R.C.; Almeida, R.; Nascimento, E.L.; Bernardi, J.V.E.; de Lacerda, L.D.; da Silveira, E.G.; Pfeiffer, W.C. Mercury in the environment and riverside population in the Madeira River Basin, Amazon, Brazil. Sci Total Environ. 2006, 368, 344–351. [Google Scholar] [CrossRef]
- Ferreira da Silva, S.; de Oliveira Lima, M. Mercury in fish marketed in the Amazon Triple Frontier and Health Risk Assessment. Chemosphere 2020, 248, 125989. [Google Scholar] [CrossRef] [PubMed]
- Vasconcellos, A.C.S.; Hallwass, G.; Bezerra, J.G.; Aciole, A.N.S.; Meneses, H.N.M.; Lima, M.O.; Jesus, I.M.; Hacon, S.S.; Basta, P.C. Health Risk Assessment of Mercury Exposure from Fish Consumption in Munduruku Indigenous Communities in the Brazilian Amazon. Int. J. Environ. Res. Public Health 2021, 18, 7940. [Google Scholar] [CrossRef]
- WHO. Guidance for Identifying Populations at Risk from Mercury Exposure; WHO: Geneva, Switerzeland, 2008; Available online: https://wedocs.unep.org/.../IdentifyingPopnatRiskExposuretoMercury2008Web.pdf (accessed on 20 March 2021).
- Bastos, L.S.; Oliveira, R.D.V.C.D.; Velasque, L.D.S. Obtendo razões de chance prevalentes de modelos de regressão logística em estudos transversais. Cad Saude Publica 2015, 31, 487–495. [Google Scholar] [CrossRef] [Green Version]
- Ospina, R.; Amorim, L. prLogisticDelta: Estimation of Prevalence Ratios using Logistic Models. 2013. Available online: https://rdrr.io/cran/prLogistic/man/prLogisticDelta.html (accessed on 14 June 2021).
- Kempton, J.W.; Hofer, C.B.; Périssé, A.R.S.; Vasconcellos, A.C.S.; Viana, P.V.S.; Lima, M.O.; Jesus, I.M.; Hacon, S.S.; Basta, P.C. An assessment of health outcomes and methylmercury exposure in Munduruku indigenous women of childbearing age and their children under 2 years old. Int. J. Environ. Res. Public Health 2021, 18. in press. [Google Scholar]
- Perini, J.A.; Silva, M.C.; Vasconcellos, A.C.S.; Viana, P.V.S.; Lima, M.O.; Jesus, I.M.; Kempton, J.W.; Oliveira, R.A.A.; Hacon, S.S.; Basta, P.C. Genetic polymorphism of Delta Aminolevulinic Acid Dehydratase (ALAD) Gene and Symptoms of Chronic Mercury Exposure in Munduruku Indigenous Children from within the Brazilian Amazon. Int. J. Environ. Res. Public Health 2021, 18, 8746. [Google Scholar] [CrossRef]
- Afrifa, J.; Opoku, Y.K.; Gyamerah, E.O.; Ashiagbor, G.; Sorkpor, R.D. The clinical importance of the mercury problem in artisanal small-scale gold mining. Front. Public Health 2019, 7, 1–9. [Google Scholar] [CrossRef]
- Kjellstrom, T.; Kennedy, P.; Wallis, S.; Mantell, C. Physical and Mental Development of Children with Prenatal Exposure to Mercury from Fish. Stage 1: Preliminary Tests at Age 4; Report 3080; National Swedish Environmental Board: Solna, Sweden, 1986. [Google Scholar]
- Kjellstrom, T.; Kennedy, P.; Wallis, S.; Mantell, C. Physical and Mental Development of Children with Prenatal Exposure to Mercury from Fish. Stage 2. Interviews and Psychological Tests at Age 6; Report 3642; National Swedish Environmental Board: Solna, Sweden, 1989. [Google Scholar]
- Crump, K.S.; Kjellström, T.; Shipp, A.M.; Silvers, A.; Stewart, A. Influence of prenatal mercury exposure upon scholastic and psychological test performance: Benchmark analysis of a New Zealand cohort. Risk Anal. 1998, 18, 701–713. [Google Scholar] [CrossRef]
- Joint FAO/WHO Expert Committee on Food Additives. Evaluation of Mercury, Lead, Cadmium and the Food Additives Amaranth, Diethylpyrocarbonate and Octyl Gallate. FAO Nutrition Meetings Report Series, No. 51A; WHO Food Additives Series No. 4. 1972. Available online: https://apps.who.int/iris/handle/10665/40985 (accessed on 15 May 2021).
- Joint FAO/WHO Expert Committee on Food Additives. Evaluation of Certain Food Additives and Contaminants; Technical Report Series No. 776; World Health Organization: Geneva, Switzerland, 1989. [Google Scholar]
- Joint FAO/WHO Expert Committee on Food Additives. Safety Evaluation of Certain Food Additives and Contaminants; WHO Food Additives Series 44; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Houston, M.C. The role of mercury in cardiovascular disease. J. Cardiovasc. Dis. Diagn 2014, 2, 1–8. [Google Scholar] [CrossRef]
- Virtanen, J.K.; Rissanen, T.H.; Voutilainen, S.; Tuomainen, T.P. Mercury as a risk factor for cardiovascular diseases. J. Nutr. Biochem. 2007, 18, 75–85. [Google Scholar] [CrossRef]
- Hu, X.F.; Lowe, M.; Chan, H.M. Mercury exposure, cardiovascular disease, and mortality: A systematic review and dose-response meta-analysis. Environ. Res. 2021, 193, 110538. [Google Scholar] [CrossRef]
- Kim, D.S.; Yu, S.D.; Cha, J.H.; Ahn, S.C.; Lee, E.H. Heavy metal as risk factor of cardiovascular disease-an analysis of blood lead and urinary mercury. J. Prev. Med. Public Health 2005, 38, 401–407. [Google Scholar] [PubMed]
- Virtanen, J.K.; Voutilainen, S.; Rissanen, T.H.; Mursu, J.; Tuomainen, T.-P.; Korhonen, M.; Valkonen, V.-P.; Seppänen, K.; Laukkanen, J.; Salonen, J.T. Mercury, fish oils, and risk of acute coronary events and cardiovascular disease, coronary heart disease, and all-cause mortality in men in eastern Finland. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 228–233. [Google Scholar] [CrossRef]
- Salonen, J.T.; Seppänen, K.; Nyyssönen, K.; Korpela, H.; Kauhanen, J.; Kantola, M.; Tuomilehto, J.; Esterbauer, H.; Tatzber, F.; Salonen, R. Intake of mercury from fish, lipid peroxidation, and the risk of myocardial infarction and coronary, cardiovascular, and any death in eastern Finnish men. Circulation 1995, 91, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Fillion, M.; Mergler, D.; Passos CJ, S.; Larribe, F.; Lemire, M.; Guimarães JR, D. A preliminary study of mercury exposure and blood pressure in the Brazilian Amazon. Environ. Health 2006, 5, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Barcelos, G.R.M.; de Souza, M.F.; de Oliveira, A.; Ávila, S.; Lengert, A.V.H.; de Oliveira, M.T.; Camargo, R.B.D.O.G.; Grotto, D.; Valentini, J.; Garcia, S.; et al. Effects of genetic polymorphisms on antioxidant status and concentrations of the metals in the blood of riverside Amazonian communities co-exposed to Hg and Pb. Environ. Res. 2015, 138, 224–232. [Google Scholar] [CrossRef]
- Faial, K.; Deus, R.; Deus, S.; Neves, R.; Jesus, I.; Santos, E.; Alves, C.N.; Brasil, D. Mercury levels assessment in hair of riverside inhabitants of the Tapajós River, Pará State, Amazon, Brazil: Fish consumption as a possible route of exposure. J. Trace Elem. Med. Biol. 2015, 30, 66–76. [Google Scholar] [CrossRef]
- Freitas, J.S.; Lacerda, E.M.D.C.B.; Júnior, D.R.; Corvelo, T.C.O.; Silveira, L.C.L.; Pinheiro, M.D.C.N.; Souza, G.S. Mercury exposure of children living in amazonian villages: Influence of geographicalocation where they lived during prenatal and postnatal development. Acad. Bras. Cienc. 2019, 91, e20180097. [Google Scholar] [CrossRef]
- Hacon, S.; Barrocas, P.R.; Vasconcellos, A.C.S.D.; Barcellos, C.; Wasserman, J.C.; Campos, R.C.; Ribeiro, C.; Azevedo-Carloni, F.B. An overview of mercury contamination research in the Amazon basin with an emphasis on Brazil Uma revisão das pesquisas sobre contaminação por mercúrio na Amazônia com ênfase no território brasileiro. Cad Saude Publica. 2008, 24, 1479–1492. [Google Scholar] [CrossRef] [Green Version]
- Galvis, S.R. The Amazon Biome in the face of Mercury Contamination. WWF Gaia Amaz 2020, 168. Available online: https://d2ouvy59p0dg6k.cloudfront.net/downloads/reporte_eng.pdf (accessed on 19 March 2021).
- WWF. Factsheet: Garimpos—Gold Mines in the Amazon. 2006. Available online: https://wwf.panda.org/?72800/Factsheet-Garimpos-Gold-mines-in-the-Amazon (accessed on 22 June 2021).
- Barbieri, F.L.; Gardon, J. Hair mercury levels in Amazonian populations: Spatial distribution and trends. Int. J. Health Geogr. 2009, 8, 71. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, L.V.B. Avaliação dos Níveis de Estresse Oxidativo Induzido por Exposição ao Mercúrio em População Ribeirinha Infantojuvenil do rio Madeira (RO); Fundação Oswaldo Cruz: Rio de Janeiro, Brazil, 2016. [Google Scholar]
- de Bortoli, M.C. Avaliação dos Níveis Sanguíneos do Hormônio Tireoidiano Ativo (T3) e do Estado Nutricional Relativo ao Selênio de Mulheres Residentes em área de Exposição ao Mercúrio. Ph.D. Thesis, Universidade de São Paulo, São Paulo, Brazil, 2010. [Google Scholar] [CrossRef] [Green Version]
- Rocha, A.V.; Cardoso, B.R.; Zavarize, B.; Almondes, K.; Bordon, I.; Hare, D.; Favaro, D.I.T.; Cozzolino, S.M.F. GPX1 Pro198Leu polymorphism and GSTM1 deletion do not affect selenium and mercury status in mildly exposed Amazonian women in an urban population. Sci. Total Environ. 2016, 571, 801–808. [Google Scholar] [CrossRef]
- Farias, L.A.; Fávaro, D.I.T.; Pessoa, A.; Aguiar, J.P.L.; Yuyama, L.K.O. Mercury and methylmercury concentration assessment in children’s hair from Manaus, Amazonas state, Brazil. Acta Amaz. 2012, 42, 279–286. [Google Scholar] [CrossRef] [Green Version]
- Begossi, A.; Salivonchyk, S.V.; Hallwass, G.; Hanazaki, N.; Lopes, P.; Silvano, R.A.M.; Dumaresq, D.; Pittock, J. Fish consumption on the amazon: A review of biodiversity, hydropower and food security issues. Braz. J Biol. 2019, 79, 345–357. [Google Scholar] [CrossRef] [PubMed]
- Dórea, J.G. Mercury and lead during breast-feeding. Br. J. Nutr. 2004, 92, 21–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, M.C.; Garn, J.V.; Sclar, G.D.; Boisson, S.; Medlicott, K.; Alexander, K.T.; Penakalapati, G.; Anderson, D.; Mahtani, A.G.; Grimes, J.E.T.; et al. The impact of sanitation on infectious disease and nutritional status: A systematic review and meta-analysis. Int. J. Hyg. Environ. Health 2017, 220, 928–949. [Google Scholar] [CrossRef] [PubMed]
- Dangour, A.D.; Watson, L.; Cumming, O.; Boisson, S.; Che, Y.; Velleman, Y.; Cavill, S.; Allen, E.; Uauy, R. Interventions to improve water quality and supply, sanitation and hygiene practices, and their effects on the nutritional status of children. Cochrane Database Syst. Rev. 2013, 8, CD009382. [Google Scholar] [CrossRef] [Green Version]
- Horta, B.L.; Santos, R.V.; Welch, J.R.; Cardoso, A.M.; dos Santos, J.V.; Assis, A.M.; Lira, P.C.; Coimbra, C.E., Jr. Nutritional status of indigenous children: Findings from the First National Survey of Indigenous People’s Health and Nutrition in Brazil. Int. J. Equity Health 2013, 12, 23. [Google Scholar] [CrossRef] [Green Version]
- Santos, A.P.; Mazzeti, C.M.D.S.; Franco, M.D.C.P.; Santos, N.L.G.O.; Conde, W.L.; Leite, M.S.; Pimenta, A.M.; Villela, L.C.M.; Castro, T.G. Estado nutricional e condições ambientais e de saúde de crianças Pataxó, Minas Gerais, Brasil [Nutritional status and environmental and health conditions of Pataxó indigenous children, Minas Gerais State, Brazil]. Cad Saude Publica 2018, 34, e00165817. [Google Scholar] [CrossRef] [Green Version]
- Frankenburg, W.K.; Dodds, J.; Archer, P.; Shapiro, H.; Bresnick, B. The Denver II: A Major Revision and Restandardization of the Denver Developmental Screening Test. Pediatrics 1992, 89, 91–97. Available online: https://pediatrics.aappublications.org/content/89/1/91 (accessed on 21 April 2021).
- Santos-Sacramento, L.; Arrifano, G.P.; Lopes-Araújo, A.; Augusto-Oliveira, M.; Albuquerque-Santos, R.; Takeda, P.Y.; Souza-Monteiro, J.R.; Macchi, B.M.; Nascimento, J.L.M.D.; Lima, R.R.; et al. Human neurotoxicity of mercury in the Amazon: A scoping review with insights and critical considerations. Ecotoxicol. Environ. Saf. 2021, 208, 111686. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Overall n = 35 | Village | ||
|---|---|---|---|---|
| Poxo Muybu n = 8 | Sawre Aboy n = 7 | Sawre Muybu n = 20 | ||
| Family Monthly income (USD) Median (Q1, Q3) | 294.1 (201.0–414.5) | 355.7 (274.5–728.4) | 235.3 (203.9–485.3) | 284.3 (166.7–382.0) |
| Regular salary | ||||
| Yes | 24 (68.6%) | 6 (75.0%) | 6 (85.7%) | 14 (75.0%) |
| No | 11 (31.4%) | 2 (25.0%) | 1 (14.3%) | 6 (25.0%) |
| Regular cash transfer | ||||
| Yes | 24 (68.6%) | 6 (75.0%) | 6 (85.7%) | 12 (60.0%) |
| No | 11(31.4%) | 2 (25.0%) | 1 (14.3%) | 8 (40.0%) |
| Roof cover | ||||
| Dry straw | 21 (60.0%) | 8 (100.0%) | 7 (100.0%) | 6 (30.0%) |
| Zinc or asbestos | 13 (37.1%) | 0 (0.0%) | 0 (0.0%) | 13 (65.0%) |
| Clay | 1 (2.9%) | 0 (0.0%) | 0 (0.0%) | 1 (5.0%) |
| Wallcovering | ||||
| Wood or brick | 23 (65.7%) | 3 (37.5%) | 1 (14.3%) | 19 (95.0%) |
| Dry straw or canvas | 12 (34.3%) | 5 (62.5%) | 6 (85.7%) | 1 (5.0%) |
| Floor | ||||
| Dirt floor | 28 (80.0%) | 8 (100.0%) | 7 (100.0%) | 13 (65.0%) |
| Cement or ceramic | 6 (17.1%) | 0 (0.0%) | 0 (0.0%) | 6 (30.0%) |
| Wood | 1 (2.9%) | 0 (0.0%) | 0 (0.0%) | 1 (5.0%) |
| Disposal of human waste | ||||
| Collective cesspool | 25 (71.4%) | 6 (75.0%) | 7 (100.0%) | 12 (60.0%) |
| Forest | 4 (11.4%) | 1 (12.5%) | 0 (0.0%) | 3 (15.0%) |
| Individual cesspool | 2 (5.7%) | 0 (0.0%) | 0 (0.0%) | 2 (10.0%) |
| Bathroom outside | 2 (5.7%) | 0 (0.0%) | 0 (0.0%) | 2 (10.0%) |
| River/stream | 2 (5.7%) | 1 (12.5%) | 0 (0.0%) | 1 (5.0%) |
| Water source | ||||
| River/stream | 32 (91.4%) | 8 (100.0%) | 7 (100.0%) | 17 (85.0%) |
| Artesian well | 3 (8.6%) | 0 (0.0%) | 0 (0.0%) | 3 (15.0%) |
| Water treatment | ||||
| Yes | 11 (31.4%) | 1 (12.5%) | 4 (57.1%) | 6 (30.0%) |
| No | 24 (68.6%) | 7 (87.5%) | 3 (42.9%) | 14 (70.0%) |
| Characteristics | Overall n = 200 | Village | p-Value 1 | ||
|---|---|---|---|---|---|
| Poxo Muybu n = 66 | Sawre Aboy n = 40 | Sawre Muybu n = 94 | |||
| Age mean (in years) Minimum–Maximum | 18 (0–73) | 16 (0–59) | 17 (0–72) | 18 (0–73) | 0.820 |
| Sex | 0.570 | ||||
| Female | 109 (55.0%) | 36 (55.0%) | 19 (48.0%) | 54 (57.0%) | |
| Male | 91 (45.0%) | 30 (45.0%) | 21 (52.0%) | 40 (43.0%) | |
| Age group | 0.100 | ||||
| Under 12 years | 88 (44.0%) | 31 (47.0%) | 16 (40.0%) | 41 (44.0%) | |
| 13–19 years | 38 (19.0%) | 15 (23.0%) | 12 (30.0%) | 11 (12.0%) | |
| 20–29 years | 39 (20.0%) | 8 (12.0%) | 5 (12.0%) | 26 (28.0%) | |
| 30–44 years | 21 (10.0%) | 8 (12.0%) | 5 (12.0%) | 8 (8.5%) | |
| 45 years and over | 14 (7.0%) | 4 (6.1%) | 2 (5.0%) | 8 (8.5%) | |
| Schooling | 0.390 | ||||
| Illiterate | 4 (2.0%) | 1 (1.5%) | 1 (2.5%) | 2 (2.1%) | |
| 1–9 years | 142 (71.0%) | 42 (64.0%) | 31 (78.0%) | 69 (73.0%) | |
| ≥10 years | 26 (13.0%) | 14 (21.0%) | 3 (7.5%) | 9 (9.6%) | |
| Not applicable | 28 (14.0%) | 9 (14.0%) | 5 (12.0%) | 14 (15.0%) | |
| Marital status | 0.049 | ||||
| Single | 30 (15.0%) | 15 (23.0%) | 9 (22.0%) | 6 (6.4%) | |
| Married | 78 (39.0%) | 23 (35.0%) | 16 (40.0%) | 39 (41.0%) | |
| Widow(er) | 6 (3.0%) | 1 (1.5%) | 1 (2.5%) | 4 (4.3%) | |
| Not applicable | 86 (43.0%) | 27 (41.0%) | 14 (35.0%) | 45 (48.0%) | |
| Anemia | 0.054 | ||||
| Yes | 66 (33.0%) | 22 (33.0%) | 19 (48.0%) | 25 (27.0%) | |
| No | 129 (64.0%) | 42 (64.0%) | 19 (48.0%) | 68 (72.0%) | |
| Missing | 5 (2.5%) | 2 (3.0%) | 2 (5.0%) | 1 (1.0%) | |
| Body Mass Index 2 | 0.827 | ||||
| <18.5 | 4 (3.5%) | 2 (5.4%) | 1 (4.2%) | 1 (1.9%) | |
| 18.5–24.9 | 73 (63.5%) | 22 (59.5%) | 17 (70.8%) | 34 (63.0%) | |
| 25.0–29.9 | 34 (29.6%) | 11 (29.7%) | 5 (20.8%) | 18 (33.3%) | |
| ≥30.0 | 4 (3.5%) | 2 (5.4%) | 1 (4.2%) | 1 (1.9%) | |
| Gene/SNP | Village | n * | Genotypic Distribution n (%) | p-Value ** | ||
|---|---|---|---|---|---|---|
| TNF-α (Chromossome 6) | ||||||
| rs1799964 | TT | TC | CC | |||
| Poxo Muybu | 61 | 56 (91.8) | 4 (6.6) | 1 (1.6) | 0.008 | |
| Sawre Aboy | 40 | 25 (62.5) | 13 (32.5) | 2 (5.0) | ||
| Sawre Muybu | 97 | 70 (72.1) | 25 (25.8) | 2 (2.1) | ||
| rs1799724 | CC | CT | TT | |||
| Poxo Muybu | 62 | 31 (50.0) | 27 (43.5) | 4 (6.5) | 0.34 | |
| Sawre Aboy | 40 | 15 (37.5) | 24 (60.0) | 1 (2.5) | ||
| Sawre Muybu | 97 | 50 (51.5) | 40 (41.3) | 7 (7.2) | ||
| rs1800629 | GG | GA | AA | |||
| Poxo Muybu | 56 | 56 (100) | 0 | 0 | 0.050 | |
| Sawre Aboy | 40 | 39 (97.5) | 1 (2.5) | 0 | ||
| Sawre Muybu | 97 | 89 (91.8) | 8 (8.2) | 0 | ||
| IL6 (Chromosome 7) | ||||||
| rs1800795 | GG | GC | CC | |||
| Poxo Muybu | 62 | 62 (100) | 0 | 0 | 0.59 | |
| Sawre Aboy | 40 | 40 (100) | 0 | 0 | ||
| Sawre Muybu | 97 | 96 (99.0) | 1 (1.0) | 0 | ||
| ALAD (Chromosome 9) | ||||||
| rs1800435 | CC | CG | GG | |||
| Poxo Muybu | 56 | 56 (100) | 0 | 0 | 0.36 | |
| Sawre Aboy | 40 | 40 (100) | 0 | 0 | ||
| Sawre Muybu | 96 | 94 (97.9) | 2 (2.1) | 0 | ||
| GSTP1 (Chromosome 11) | ||||||
| rs1695 | AA | AG | GG | |||
| Poxo Muybu | 62 | 37 (59.7) | 24 (38.7) | 1 (1.6) | <0.0001 | |
| Sawre Aboy | 40 | 30 (75.0) | 10 (25.0) | 0 | ||
| Sawre Muybu | 97 | 13 (13.4) | 61 (62.9) | 23 (23.7) | ||
| VDR (Chromosome 12) | ||||||
| rs2228570 | CC | CT | TT | |||
| Poxo Muybu | 62 | 27 (43.5) | 29 (46.8) | 6 (9.7) | 0.01 | |
| Sawre Aboy | 40 | 9 (22.5) | 22 (55) | 9 (22.5) | ||
| Sawre Muybu | 97 | 49 (50.5) | 41 (42.3) | 7 (7.2) | ||
| MMP2 (Chromosome 16) | ||||||
| rs2285053 | CC | CT | TT | |||
| Poxo Muybu | 62 | 58 (93.5) | 4 (6.5) | 0 | <0.0001 | |
| Sawre Aboy | 40 | 34 (85.0) | 6 (15.0) | 0 | ||
| Sawre Muybu | 96 | 58 (60.4) | 37 (38.5) | 1 (1.1) | ||
| Hair Mercury Levels | |||||||
|---|---|---|---|---|---|---|---|
| Villages | n | Mean | Standard Deviation | Median | Minimum | Maximum | ≥6.0 µg/g |
| Sawré Muybu | |||||||
| Children < 12 years | 38 | 5.9 | 4.7 | 4.3 | 1.6 | 22.1 | 28.9 |
| Adults ≥ 12 years | |||||||
| Male | 24 | 7.3 | 3.2 | 6.9 | 2.6 | 16.0 | 66.7 |
| Female | 29 | 6.3 | 3.5 | 4.7 | 2.0 | 14.1 | 41.4 |
| Total | 91 | 6.4 | 4.0 | 5.2 | 1.6 | 22.1 | 42.9 |
| Poxo Muybu | |||||||
| Children < 12 years | 28 | 5.9 | 2.6 | 5.8 | 1.4 | 11.8 | 46.4 |
| Adults ≥ 12 years | |||||||
| Male | 18 | 7.1 | 2.3 | 7.3 | 2.8 | 11.9 | 61.1 |
| Female | 20 | 7.6 | 2.2 | 7.3 | 4.2 | 12.9 | 80.0 |
| Total | 66 | 6.8 | 2.5 | 6.6 | 1.4 | 12.9 | 60.6 |
| Sawré Aboy | |||||||
| Children < 12 years | 15 | 11.0 | 5.7 | 10.1 | 2.6 | 23.9 | 80.0 |
| Adults ≥ 12 years | |||||||
| Male | 14 | 13.6 | 5.4 | 14.2 | 4.8 | 22.8 | 92.9 |
| Female | 11 | 12.1 | 4.1 | 11.9 | 5.0 | 20.2 | 90.9 |
| Total | 40 | 12.2 | 5.3 | 11.5 | 2.6 | 23.9 | 87.5 |
| All Villages | |||||||
| Children < 12 years | 81 | 6.9 | 4.8 | 5.5 | 1.4 | 23.9 | 44.4 |
| Adults ≥ 12 years | |||||||
| Male | 56 | 8.8 | 4.6 | 7.5 | 2.6 | 22.8 | 71.4 |
| Female | 60 | 7.8 | 3.8 | 7.3 | 2.0 | 20.2 | 63.3 |
| Total | 197 | 7.7 | 4.5 | 6.6 | 1.4 | 23.9 | 57.9 |
| Hair Mercury Levels | |||||||
|---|---|---|---|---|---|---|---|
| <6.0 µg/g | ≥6.0 µg/g | Total | p-Value * | ||||
| Sociodemographic Characteristics | |||||||
| Sex | n | % # | n | % # | n | % † | |
| Female | 22 | 36.7 | 38 | 63.3 | 60 | 51.7 | 0.353 |
| Male | 16 | 28.6 | 40 | 71.4 | 56 | 48.3 | |
| Total | 38 | 32.8 | 78 | 67.2 | 116 | ||
| Age range (years) | |||||||
| 12 to 19 | 13 | 29.5 | 31 | 70.5 | 44 | 37.9 | 0.843 |
| 20 to 29 | 13 | 34.2 | 25 | 65.8 | 38 | 32.8 | |
| 30 and + | 12 | 35.3 | 22 | 64.7 | 34 | 29.3 | |
| Total | 38 | 78 | 116 | ||||
| Marital Status | |||||||
| Married | 25 | 33.3 | 50 | 66.7 | 75 | 64.7 | 0.980 |
| Single | 11 | 31.4 | 24 | 68.6 | 35 | 30.2 | |
| Widow(er) | 2 | 33.3 | 4 | 66.7 | 6 | 5.2 | |
| Total | 38 | 78 | 116 | ||||
| Income | |||||||
| Yes | 18 | 45.0 | 22 | 55.0 | 40 | 34.5 | 0.042 |
| No | 20 | 26.3 | 56 | 73.7 | 76 | 65.5 | |
| Total | 38 | 78 | 116 | ||||
| Schooling (years) | |||||||
| ≥10 | 11 | 45.8 | 13 | 54.2 | 24 | 20.7 | 0.170 |
| 5 to 9 | 23 | 31.5 | 50 | 68.5 | 73 | 62.9 | |
| 1 to 4 | 2 | 13.3 | 13 | 86.7 | 15 | 12.9 | |
| Iliterate | 2 | 50.0 | 2 | 50.0 | 4 | 3.4 | |
| Total | 38 | 78 | 116 | ||||
| Villages | |||||||
| Sawré Muybu | 25 | 47.2 | 28 | 52.8 | 53 | 45.7 | 0.002 |
| Poxo Muybu | 11 | 28.9 | 27 | 71.1 | 38 | 32.8 | |
| Sawré Aboy | 2 | 8.0 | 23 | 92.0 | 25 | 21.6 | |
| Total | 38 | 78 | 116 | ||||
| Clinical characteristics | |||||||
| BMI (kg/m2) | n | % | n | % | n | % | |
| 18.5–24.9 | 24 | 33.3 | 48 | 66.7 | 72 | 63.7 | 0.972 |
| <18.5 | 1 | 25.0 | 3 | 75.0 | 4 | 3.5 | |
| 25.0–29.9 | 11 | 33.3 | 22 | 66.7 | 33 | 29.2 | |
| ≥30.0 | 1 | 25.0 | 3 | 25.0 | 4 | 3.5 | |
| Total | 37 | 76 | 113 | ||||
| Blood Pressure | |||||||
| Normal | 37 | 36.3 | 65 | 63.7 | 102 | 88.7 | 0.039 |
| Hypertension | 1 | 7.7 | 12 | 92.3 | 13 | 11.3 | |
| Total | 38 | 77 | 115 | ||||
| Anemia | |||||||
| No | 32 | 34.8 | 60 | 65.2 | 92 | 80.0 | 0.428 |
| Yes | 6 | 26.1 | 17 | 73.9 | 23 | 20.0 | |
| Total | 38 | 77 | 115 | ||||
| Glucose | |||||||
| <100.0 mg/dL | 2 | 50.0 | 2 | 50.0 | 4 | 11.1 | 0.293 |
| ≥100.0 mg/dL | 8 | 25.0 | 24 | 75.0 | 32 | 88.9 | |
| Total | 10 | 26 | 36 | ||||
| Previous Hospitalization | |||||||
| No | 22 | 32.4 | 46 | 67.6 | 68 | 58.6 | 0.912 |
| Yes | 16 | 33.3 | 32 | 66.7 | 48 | 41.4 | |
| Total | 38 | 78 | 116 | ||||
| Hair Mercury Levels | |||||||
|---|---|---|---|---|---|---|---|
| Women Features | <6.0 µg/g | ≥6.0 µg/g | Total | p-Value * | |||
| Number of children | n | % # | n | % # | n | % † | |
| 1 to 2 | 4 | 28.6 | 10 | 71.4 | 14 | 26.4 | 0.531 |
| 3 to 6 | 8 | 50.0 | 8 | 50.0 | 16 | 30.2 | |
| 7 or + | 1 | 20.0 | 4 | 80.0 | 5 | 9.4 | |
| No children | 7 | 38.9 | 11 | 61.1 | 18 | 34.0 | |
| Total | 20 | 37.7 | 33 | 62.3 | 53 | ||
| Pregnant | |||||||
| No | 20 | 41.7 | 28 | 58.3 | 48 | 90.6 | 0.067 |
| Yes | 0 | 0.0 | 5 | 100.0 | 5 | 9.4 | |
| Total | 20 | 33 | 53 | ||||
| Breastfeeding | |||||||
| No | 13 | 36.1 | 23 | 63.9 | 36 | 67.9 | 0.723 |
| Yes | 7 | 41.2 | 10 | 58.8 | 17 | 32.1 | |
| Total | 20 | 33 | 53 | ||||
| Clinical Characteristics | Hg Detected | Participants | Mean | SD # | SE † | F-Test | p-Value |
|---|---|---|---|---|---|---|---|
| Height (cm) | <6.0 µg/g | 37 | 150.6 | 6.7916 | 1.1165 | 0.065 | 0.799 |
| ≥6.0 µg/g | 76 | 151.2 | 7.2156 | 0.8277 | |||
| Weight (kg) | <6.0 µg/g | 37 | 53.7 | 9.5022 | 1.5621 | 1.189 | 0.278 |
| ≥6.0 µg/g | 77 | 52.8 | 9.7792 | 1.1144 | |||
| BMI (kg/m2) | <6.0 µg/g | 37 | 23.6 | 3.38 | 0.5557 | 1.936 | 0.167 |
| ≥6.0 µg/g | 76 | 23.1 | 3.6339 | 0.4168 | |||
| SBP * (mmHg) | <6.0 µg/g | 38 | 110.5 | 9.42 | 1.528 | 4.157 | 0.044 |
| ≥6.0 µg/g | 77 | 113.2 | 15.557 | 1.773 | |||
| DBP ** (mmHg) | <6.0 µg/g | 38 | 67.8 | 7.577 | 1.229 | 4.363 | 0.039 |
| ≥6.0 µg/g | 77 | 69.3 | 11.225 | 1.279 | |||
| Glucose level (mg/dL) | <6.0 µg/g | 10 | 115.2 | 16.858 | 5.331 | 0.075 | 0.786 |
| ≥6.0 µg/g | 26 | 115.4 | 19.438 | 3.812 | |||
| Hemoglobin level (g/dL) | <6.0 µg/g | 38 | 13.8 | 1.2437 | 0.2018 | 0.175 | 0.677 |
| ≥6.0 µg/g | 77 | 13.8 | 1.3299 | 0.1516 |
| Indigenous ≥ 12 Years-Old Both Sex | ||||||
| Characteristics | Crude PR | 95%CI | p-Value | Adjusted PR | 95%CI | p-Value |
| Villages | ||||||
| Sawré Muybu | 1 | 1 | ||||
| Poxo Muybu | 1.3 | (0.9–1.9) | 0.074 | 1.3 | (0.9–1.8) | 0.098 |
| Sawré Aboy | 1.7 | (1.3–2.3) | 0.001 | 1.8 | (1.3–2.3) | 0.001 |
| Income | ||||||
| Yes | 1 | 1 | ||||
| No | 1.3 | (0.9–1.8) | 0.065 | 1.3 | (1.0–1.8) | 0.031 |
| Schooling (years) | ||||||
| ≥10 | 1 | |||||
| 5 to 9 | 1.3 | (0.9–1.9) | 0.250 | -- | ||
| 1 to 4 | 1.6 | (1.0–2.4) | 0.028 | -- | ||
| Illiterate | 0.9 | (0.3–2.6) | 0.881 | -- | ||
| Blood Pressure | ||||||
| Normal | 1 | |||||
| Hypertension | 1.4 | (1.2–1.8) | 0.001 | 1.6 | (1.3–2.1) | 0.001 |
| Women of Childbearing Age | ||||||
| Characteristics | Crude PR | 95%CI | p-Value | Adjusted PR | 95%CI | p-Value |
| Villages | ||||||
| Sawré Muybu | 1 | 1 | ||||
| Poxo Muybu | 2.1 | (1.2–3.7) | 0.010 | 1.9 | (1.0–3.4) | 0.044 |
| Sawré Aboy | 2.4 | (1.4–4.2) | 0.002 | 2.5 | (1.4–4.4) | 0.001 |
| Income | ||||||
| Yes | 1 | -- | ||||
| No | 1.3 | (0.8–2.3) | 0.273 | -- | ||
| Blood Pressure | ||||||
| Normal | 1 | 1 | ||||
| Hypertension | 1.7 | (1.3–2.1) | 0.001 | 1.9 | (1.2–3.3) | 0.012 |
| Pregnant status | ||||||
| No | 1 | 1 | ||||
| Yes | 1.7 | (1.4–2.2) | 0.001 | 1.5 | (1.0–2.1) | 0.029 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basta, P.C.; Viana, P.V.d.S.; Vasconcellos, A.C.S.d.; Périssé, A.R.S.; Hofer, C.B.; Paiva, N.S.; Kempton, J.W.; Ciampi de Andrade, D.; Oliveira, R.A.A.d.; Achatz, R.W.; et al. Mercury Exposure in Munduruku Indigenous Communities from Brazilian Amazon: Methodological Background and an Overview of the Principal Results. Int. J. Environ. Res. Public Health 2021, 18, 9222. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179222
Basta PC, Viana PVdS, Vasconcellos ACSd, Périssé ARS, Hofer CB, Paiva NS, Kempton JW, Ciampi de Andrade D, Oliveira RAAd, Achatz RW, et al. Mercury Exposure in Munduruku Indigenous Communities from Brazilian Amazon: Methodological Background and an Overview of the Principal Results. International Journal of Environmental Research and Public Health. 2021; 18(17):9222. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179222
Chicago/Turabian StyleBasta, Paulo Cesar, Paulo Victor de Sousa Viana, Ana Claudia Santiago de Vasconcellos, André Reynaldo Santos Périssé, Cristina Barroso Hofer, Natalia Santana Paiva, Joseph William Kempton, Daniel Ciampi de Andrade, Rogério Adas Ayres de Oliveira, Rafaela Waddington Achatz, and et al. 2021. "Mercury Exposure in Munduruku Indigenous Communities from Brazilian Amazon: Methodological Background and an Overview of the Principal Results" International Journal of Environmental Research and Public Health 18, no. 17: 9222. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179222