
Residence in a Hispanic Enclave Is Associated with Inferior Overall Survival among Children with Acute Lymphoblastic Leukemia

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
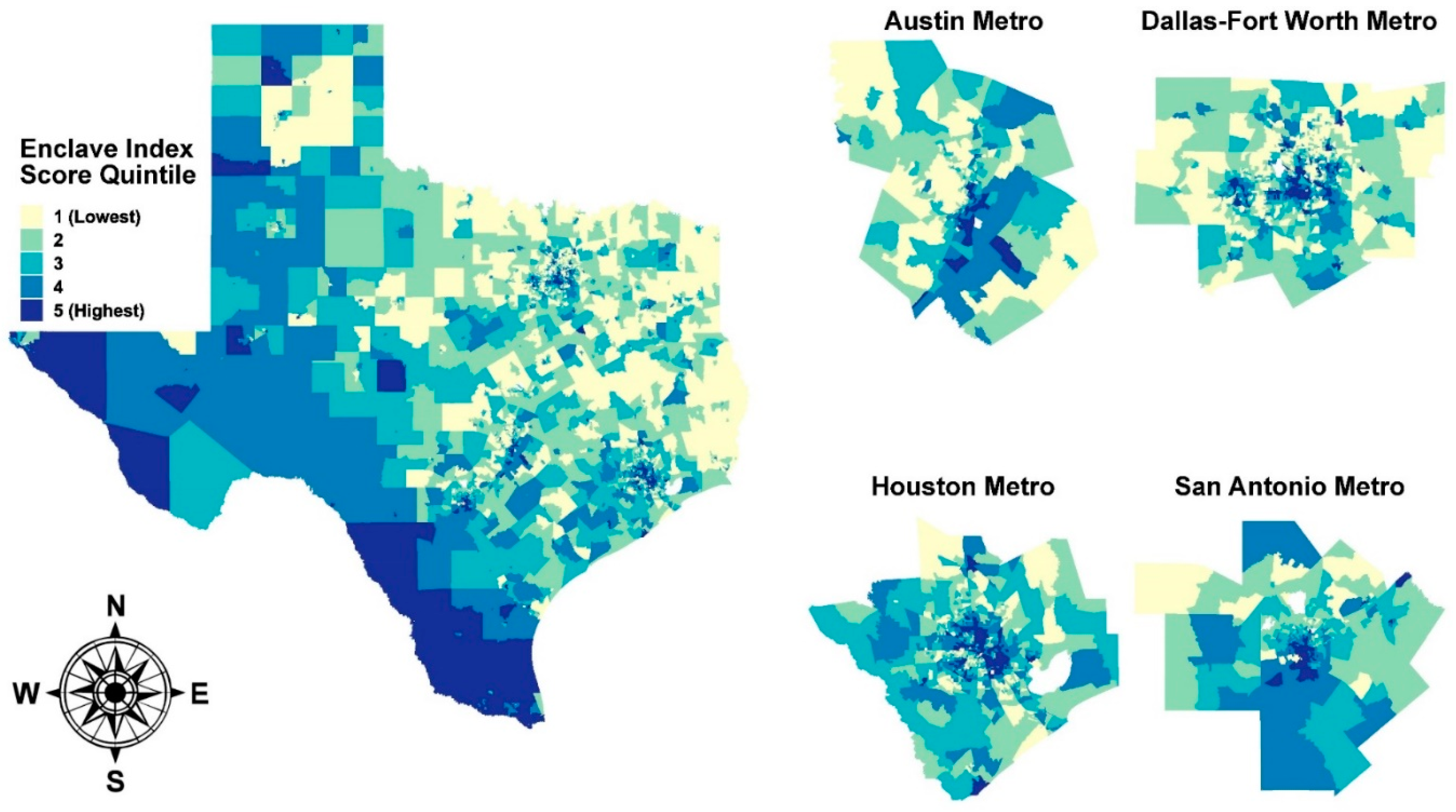
2.2. Hispanic Enclave Index and Area Deprivation Index Scores
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hunger, S.P.; Mullighan, C.G. Acute Lymphoblastic Leukemia in Children. N. Engl. J. Med. 2015, 373, 1541–1552. [Google Scholar] [CrossRef] [Green Version]
- Lupo, P.J.; Spector, L.G. Cancer Progress and Priorities: Childhood Cancer. Cancer Epidemiol. Biomark. Prev. 2020, 29, 1081–1094. [Google Scholar] [CrossRef] [PubMed]
- Society, A.C. Cancer Facts and Figures 2021; American Cancer Society: Atlanta, GA, USA, 2021; Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2021/cancer-facts-and-figures-2021.pdf (accessed on 16 June 2021).
- Shoag, J.M.; Barredo, J.C.; Lossos, I.S.; Pinheiro, P.S. Acute lymphoblastic leukemia mortality in Hispanic Americans. Leuk. Lymphoma 2020, 61, 2674–2681. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, S. Influence of race and socioeconomic status on outcome of children treated for childhood acute lymphoblastic leukemia. Curr. Opin. Pediatr. 2004, 16, 9–14. [Google Scholar] [CrossRef]
- Bhatia, S.; Sather, H.N.; Heerema, N.A.; Trigg, M.E.; Gaynon, P.S.; Robison, L.L. Racial and ethnic differences in survival of children with acute lymphoblastic leukemia. Blood 2002, 100, 1957–1964. [Google Scholar] [CrossRef]
- Dores, G.M.; Devesa, S.S.; Curtis, R.E.; Linet, M.S.; Morton, L.M. Acute leukemia incidence and patient survival among children and adults in the United States, 2001–2007. Blood 2012, 119, 34–43. [Google Scholar] [CrossRef]
- Goggins, W.B.; Lo, F.F. Racial and ethnic disparities in survival of US children with acute lymphoblastic leukemia: Evidence from the SEER database 1988–2008. Cancer Causes Control 2012, 23, 737–743. [Google Scholar] [CrossRef] [PubMed]
- Harvey, R.C.; Mullighan, C.G.; Chen, I.M.; Wharton, W.; Mikhail, F.M.; Carroll, A.J.; Kang, H.; Liu, W.; Dobbin, K.K.; Smith, M.A.; et al. Rearrangement of CRLF2 is associated with mutation of JAK kinases, alteration of IKZF1, Hispanic/Latino ethnicity, and a poor outcome in pediatric B-progenitor acute lymphoblastic leukemia. Blood 2010, 115, 5312–5321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez-Andreu, V.; Roberts, K.G.; Harvey, R.C.; Yang, W.; Cheng, C.; Pei, D.; Xu, H.; Gastier-Foster, J.; Shuyu, E.; Lim, J.Y.; et al. Inherited GATA3 variants are associated with Ph-like childhood acute lymphoblastic leukemia and risk of relapse. Nat. Genet. 2013, 45, 1494–1498. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.; Arthur, D.; Camitta, B.; Carroll, A.J.; Crist, W.; Gaynon, P.; Gelber, R.; Heerema, N.; Korn, E.L.; Link, M.; et al. Uniform approach to risk classification and treatment assignment for children with acute lymphoblastic leukemia. J. Clin. Oncol. 1996, 14, 18–24. [Google Scholar] [CrossRef]
- Skinner, A.C.; Ravanbakht, S.N.; Skelton, J.A.; Perrin, E.M.; Armstrong, S.C. Prevalence of Obesity and Severe Obesity in US Children, 1999–2016. Pediatrics 2018, 141, e20173459. [Google Scholar] [CrossRef] [Green Version]
- Ogden, C.L.; Fryar, C.D.; Hales, C.M.; Carroll, M.D.; Aoki, Y.; Freedman, D.S. Differences in Obesity Prevalence by Demographics and Urbanization in US Children and Adolescents, 2013–2016. JAMA 2018, 319, 2410–2418. [Google Scholar] [CrossRef]
- Pelletier, W.; Bona, K. Assessment of Financial Burden as a Standard of Care in Pediatric Oncology. Pediatr. Blood Cancer 2015, 62 (Suppl. 5), S619–S631. [Google Scholar] [CrossRef] [Green Version]
- Warner, E.L.; Kirchhoff, A.C.; Nam, G.E.; Fluchel, M. Financial Burden of Pediatric Cancer for Patients and Their Families. J. Oncol. Pract. 2015, 11, 12–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatia, S.; Landier, W.; Hageman, L.; Kim, H.; Chen, Y.; Crews, K.R.; Evans, W.E.; Bostrom, B.; Casillas, J.; Dickens, D.S.; et al. 6MP adherence in a multiracial cohort of children with acute lymphoblastic leukemia: A Children’s Oncology Group study. Blood 2014, 124, 2345–2353. [Google Scholar] [CrossRef]
- Landier, W.; Chen, Y.; Hageman, L.; Kim, H.; Bostrom, B.C.; Casillas, J.N.; Dickens, D.S.; Evans, W.E.; Maloney, K.W.; Mascarenhas, L.; et al. Comparison of self-report and electronic monitoring of 6MP intake in childhood ALL: A Children’s Oncology Group study. Blood 2017, 129, 1919–1926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aristizabal, P.; Winestone, L.E.; Umaretiya, P.; Bona, K. Disparities in Pediatric Oncology: The 21st Century Opportunity to Improve Outcomes for Children and Adolescents with Cancer. Am. Soc. Clin. Oncol. Educ. Book 2021, 41, e315–e326. [Google Scholar] [CrossRef]
- Colton, M.D.; Hawkins, M.; Goulding, D.; Cockburn, M.; Green, A.L. Socioeconomics, race, and ethnicity in childhood cancer survival: Accessing and addressing root causes of disparities. Cancer 2018, 124, 3975–3978. [Google Scholar] [CrossRef] [PubMed]
- Schraw, J.M.; Peckham-Gregory, E.C.; Rabin, K.R.; Scheurer, M.E.; Lupo, P.J.; Oluyomi, A. Area deprivation is associated with poorer overall survival in children with acute lymphoblastic leukemia. Pediatr. Blood Cancer 2020, 67, e28525. [Google Scholar] [CrossRef]
- Kent, E.E.; Sender, L.S.; Largent, J.A.; Anton-Culver, H. Leukemia survival in children, adolescents, and young adults: Influence of socioeconomic status and other demographic factors. Cancer Causes Control 2009, 20, 1409–1420. [Google Scholar] [CrossRef] [Green Version]
- Abrahao, R.; Lichtensztajn, D.Y.; Ribeiro, R.C.; Marina, N.M.; Keogh, R.H.; Marcos-Gragera, R.; Glaser, S.L.; Keegan, T.H. Racial/ethnic and socioeconomic disparities in survival among children with acute lymphoblastic leukemia in California, 1988-2011: A population-based observational study. Pediatr. Blood Cancer 2015, 62, 1819–1825. [Google Scholar] [CrossRef] [PubMed]
- Acharya, S.; Hsieh, S.; Shinohara, E.T.; DeWees, T.; Frangoul, H.; Perkins, S.M. Effects of Race/Ethnicity and Socioeconomic Status on Outcome in Childhood Acute Lymphoblastic Leukemia. J. Pediatr. Hematol. Oncol. 2016, 38, 350–354. [Google Scholar] [CrossRef]
- Krieger, N.; Williams, D.R.; Moss, N.E. Measuring social class in US public health research: Concepts, methodologies, and guidelines. Annu. Rev. Public Health 1997, 18, 341–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, G.K. Area deprivation and widening inequalities in US mortality, 1969-1998. Am. J. Public Health 2003, 93, 1137–1143. [Google Scholar] [CrossRef]
- Shariff-Marco, S.; Gomez, S.L.; Canchola, A.J.; Fullington, H.; Hughes, A.E.; Zhu, H.; Pruitt, S.L. Nativity, ethnic enclave residence, and breast cancer survival among Latinas: Variations between California and Texas. Cancer 2020, 126, 2849–2858. [Google Scholar] [CrossRef]
- Pruitt, S.L.; Tiro, J.A.; Xuan, L.; Lee, S.J. Hispanic and Immigrant Paradoxes in U.S. Breast Cancer Mortality: Impact of Neighborhood Poverty and Hispanic Density. Int. J. Environ. Res. Public Health 2016, 13, 1238. [Google Scholar] [CrossRef]
- Keegan, T.H.; Quach, T.; Shema, S.; Glaser, S.L.; Gomez, S.L. The influence of nativity and neighborhoods on breast cancer stage at diagnosis and survival among California Hispanic women. BMC Cancer 2010, 10, 603. [Google Scholar] [CrossRef] [Green Version]
- Pruitt, S.L.; Lee, S.J.; Tiro, J.A.; Xuan, L.; Ruiz, J.M.; Inrig, S. Residential racial segregation and mortality among black, white, and Hispanic urban breast cancer patients in Texas, 1995 to 2009. Cancer 2015, 121, 1845–1855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escobar, K.M.; Sivaram, M.; Gorey, K.M.; Luginaah, I.N.; Kanjeekal, S.M.; Wright, F.C. Colon cancer care of Hispanic people in California: Paradoxical barrio protections seem greatest among vulnerable populations. J Public Health Res. 2020, 9, 1696. [Google Scholar] [CrossRef] [PubMed]
- Schupp, C.W.; Press, D.J.; Gomez, S.L. Immigration factors and prostate cancer survival among Hispanic men in California: Does neighborhood matter? Cancer 2014, 120, 1401–1408. [Google Scholar] [CrossRef] [Green Version]
- Von Behren, J.; Abrahão, R.; Goldberg, D.; Gomez, S.L.; Setiawan, V.W.; Cheng, I. The influence of neighborhood socioeconomic status and ethnic enclave on endometrial cancer mortality among Hispanics and Asian Americans/Pacific Islanders in California. Cancer Causes Control 2018, 29, 875–881. [Google Scholar] [CrossRef]
- Barrington-Trimis, J.L.; Cockburn, M.; Metayer, C.; Gauderman, W.J.; Wiemels, J.; McKean-Cowdin, R. Rising rates of acute lymphoblastic leukemia in Hispanic children: Trends in incidence from 1992 to 2011. Blood 2015, 125, 3033–3034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steliarova-Foucher, E.; Stiller, C.; Lacour, B.; Kaatsch, P. International Classification of Childhood Cancer, third edition. Cancer 2005, 103, 1457–1467. [Google Scholar] [CrossRef] [PubMed]
- Developing Asian and Hispanic Ethnic Enclave Measures for Five States Using U.S. Census and American Community Survey Data. Available online: https://cancerregistry.ucsf.edu/resources/research-tools (accessed on 17 August 2021).
- Gomez, S.L.; Shariff-Marco, S.; DeRouen, M.; Keegan, T.H.; Yen, I.H.; Mujahid, M.; Satariano, W.A.; Glaser, S.L. The impact of neighborhood social and built environment factors across the cancer continuum: Current research, methodological considerations, and future directions. Cancer 2015, 121, 2314–2330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kind, A.J.; Jencks, S.; Brock, J.; Yu, M.; Bartels, C.; Ehlenbach, W.; Greenberg, C.; Smith, M. Neighborhood socioeconomic disadvantage and 30-day rehospitalization: A retrospective cohort study. Ann. Intern. Med. 2014, 161, 765–774. [Google Scholar] [CrossRef] [Green Version]
- Krieger, N.; Dalton, J.; Wang, C.; Perzynski, A. Sociome: Operationalizing Social Determinants of Health Data for Researchers, 2.0.0; Comprehensive R Archive Network, 2021; Available online: https://CRAN.R-project.org/package=sociome (accessed on 16 July 2021).
- Rural-Urban Commuting Area Codes. Available online: https://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes.aspx (accessed on 26 July 2021).
- Kahle, D.; Wickham, H. ggmap: Spatial Visualization with ggplot2. R J. 2013, 5, 144. Available online: https://cran.r-project.org/web/packages/ggmap/index.html (accessed on 30 August 2021). [CrossRef] [Green Version]
- Therneau, T.M. Survival: A Package for Survival Analysis in R, 3.2.7; Comprehensive R Archive Network, 2020; Available online: https://CRAN.R-project.org/package=survival (accessed on 16 June 2021).
- Therneau, T.M.; Grambsch, P.M. Modeling Survival Data: Extending the Cox Model; Springer: New York, NY, USA, 2000. [Google Scholar]
- Harrington, D.P.; Fleming, T.R. A Class of Rank Test Procedures for Censored Survival Data. Biometrika 1982, 69, 553–566. [Google Scholar] [CrossRef]
- Grambsch, P.M.; Therneau, T.M. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika 1994, 81, 515–526. [Google Scholar]
- Williams, L.A.; Richardson, M.; Marcotte, E.L.; Poynter, J.N.; Spector, L.G. Sex ratio among childhood cancers by single year of age. Pediatr. Blood Cancer 2019, 66, e27620. [Google Scholar] [CrossRef]
- Njoku, K.; Basta, N.; Mann, K.D.; McNally, R.J.; Pearce, M.S. Socioeconomic variation in survival from childhood leukaemia in northern England, 1968–2010. Br. J. Cancer 2013, 108, 2339–2345. [Google Scholar] [CrossRef] [Green Version]
- Lightfoot, T.J.; Johnston, W.T.; Simpson, J.; Smith, A.G.; Ansell, P.; Crouch, S.; Roman, E.; Kinsey, S.E. Survival from childhood acute lymphoblastic leukaemia: The impact of social inequality in the United Kingdom. Eur. J. Cancer 2012, 48, 263–269. [Google Scholar] [PubMed]
- Hunger, S.P.; Lu, X.; Devidas, M.; Camitta, B.M.; Gaynon, P.S.; Winick, N.J.; Reaman, G.H.; Carroll, W.L. Improved survival for children and adolescents with acute lymphoblastic leukemia between 1990 and 2005: A report from the children’s oncology group. J. Clin. Oncol. 2012, 30, 1663–1669. [Google Scholar]
- Vrooman, L.M.; Stevenson, K.E.; Supko, J.G.; O’Brien, J.; Dahlberg, S.E.; Asselin, B.L.; Athale, U.H.; Clavell, L.A.; Kelly, K.M.; Kutok, J.L.; et al. Postinduction dexamethasone and individualized dosing of Escherichia Coli L-asparaginase each improve outcome of children and adolescents with newly diagnosed acute lymphoblastic leukemia: Results from a randomized study--Dana-Farber Cancer Institute ALL Consortium Protocol 00-01. J. Clin. Oncol. 2013, 31, 1202–1210. [Google Scholar] [PubMed] [Green Version]
- Domenech, C.; Suciu, S.; De Moerloose, B.; Mazingue, F.; Plat, G.; Ferster, A.; Uyttebroeck, A.; Sirvent, N.; Lutz, P.; Yakouben, K.; et al. Dexamethasone (6 mg/m2/day) and prednisolone (60 mg/m2/day) were equally effective as induction therapy for childhood acute lymphoblastic leukemia in the EORTC CLG 58951 randomized trial. Haematologica 2014, 99, 1220–1227. [Google Scholar]
- Tai, E.W.; Ward, K.C.; Bonaventure, A.; Siegel, D.A.; Coleman, M.P. Survival among children diagnosed with acute lymphoblastic leukemia in the United States, by race and age, 2001 to 2009: Findings from the CONCORD-2 study. Cancer 2017, 123 (Suppl. 24), 5178–5189. [Google Scholar] [PubMed] [Green Version]
- Kadan-Lottick, N.S.; Ness, K.K.; Bhatia, S.; Gurney, J.G. Survival variability by race and ethnicity in childhood acute lymphoblastic leukemia. JAMA 2003, 290, 2008–2014. [Google Scholar] [PubMed] [Green Version]
- Ma, H.; Sun, H.; Sun, X. Survival improvement by decade of patients aged 0-14 years with acute lymphoblastic leukemia: A SEER analysis. Sci. Rep. 2014, 4, 4227. [Google Scholar]
- Kahn, J.M.; Keegan, T.H.; Tao, L.; Abrahão, R.; Bleyer, A.; Viny, A.D. Racial disparities in the survival of American children, adolescents, and young adults with acute lymphoblastic leukemia, acute myelogenous leukemia, and Hodgkin lymphoma. Cancer 2016, 122, 2723–2730. [Google Scholar]
- Delavar, A.; Barnes, J.M.; Wang, X.; Johnson, K.J. Associations Between Race/Ethnicity and US Childhood and Adolescent Cancer Survival by Treatment Amenability. JAMA Pediatr. 2020, 174, 428–436. [Google Scholar]
- Yang, J.J.; Cheng, C.; Devidas, M.; Cao, X.; Fan, Y.; Campana, D.; Yang, W.; Neale, G.; Cox, N.J.; Scheet, P.; et al. Ancestry and pharmacogenomics of relapse in acute lymphoblastic leukemia. Nat. Genet. 2011, 43, 237–241. [Google Scholar]
- Fang, C.Y.; Tseng, M. Ethnic density and cancer: A review of the evidence. Cancer 2018, 124, 1877–1903. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Quintile 1 | Quintile 2 | Quintile 3 | Quintile 4 | Quintile 5 | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | |
| Cases | 611 | - | 699 | - | 734 | - | 816 | - | 1223 | - |
| Deceased | 84 | 13.7 | 119 | 17.0 | 108 | 14.7 | 144 | 17.6 | 280 | 22.9 |
| Sex | ||||||||||
| Male | 350 | 57.3 | 414 | 59.2 | 391 | 53.3 | 447 | 54.8 | 699 | 57.2 |
| Female | 261 | 42.7 | 285 | 40.8 | 343 | 46.7 | 369 | 45.2 | 524 | 42.8 |
| Race/ethnicity | ||||||||||
| Non-Hispanic White | 448 | 73.3 | 448 | 64.1 | 338 | 46.0 | 194 | 23.8 | 90 | 7.4 |
| Non-Hispanic Black | 43 | 7.0 | 44 | 6.3 | 75 | 10.2 | 70 | 8.6 | 26 | 2.1 |
| Hispanic | 79 | 12.9 | 172 | 24.6 | 290 | 39.5 | 523 | 64.1 | 1095 | 89.5 |
| Non-Hispanic Other | 41 | 6.7 | 35 | 5.0 | 31 | 4.2 | 29 | 3.6 | 12 | 1.0 |
| Residing in a metro area 1 | 530 | 86.7 | 592 | 84.7 | 602 | 82.0 | 686 | 84.1 | 1129 | 92.3 |
| Characteristic | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| Area deprivation score | 79.9 | 17.5 | 85.3 | 14.1 | 94.4 | 12.6 | 104.7 | 12.0 | 121.9 | 12.8 |
| Age at Diagnosis (yrs) | 6.3 | 5.0 | 6.6 | 5.3 | 6.8 | 5.1 | 6.9 | 5.3 | 6.9 | 5.2 |
| Group | N at Risk (5 year OS) | 5 Year OS % (95% CI) | cHR (95% CI) | aHR (95% CI) 1 | aHR (95% CI) 2 |
|---|---|---|---|---|---|
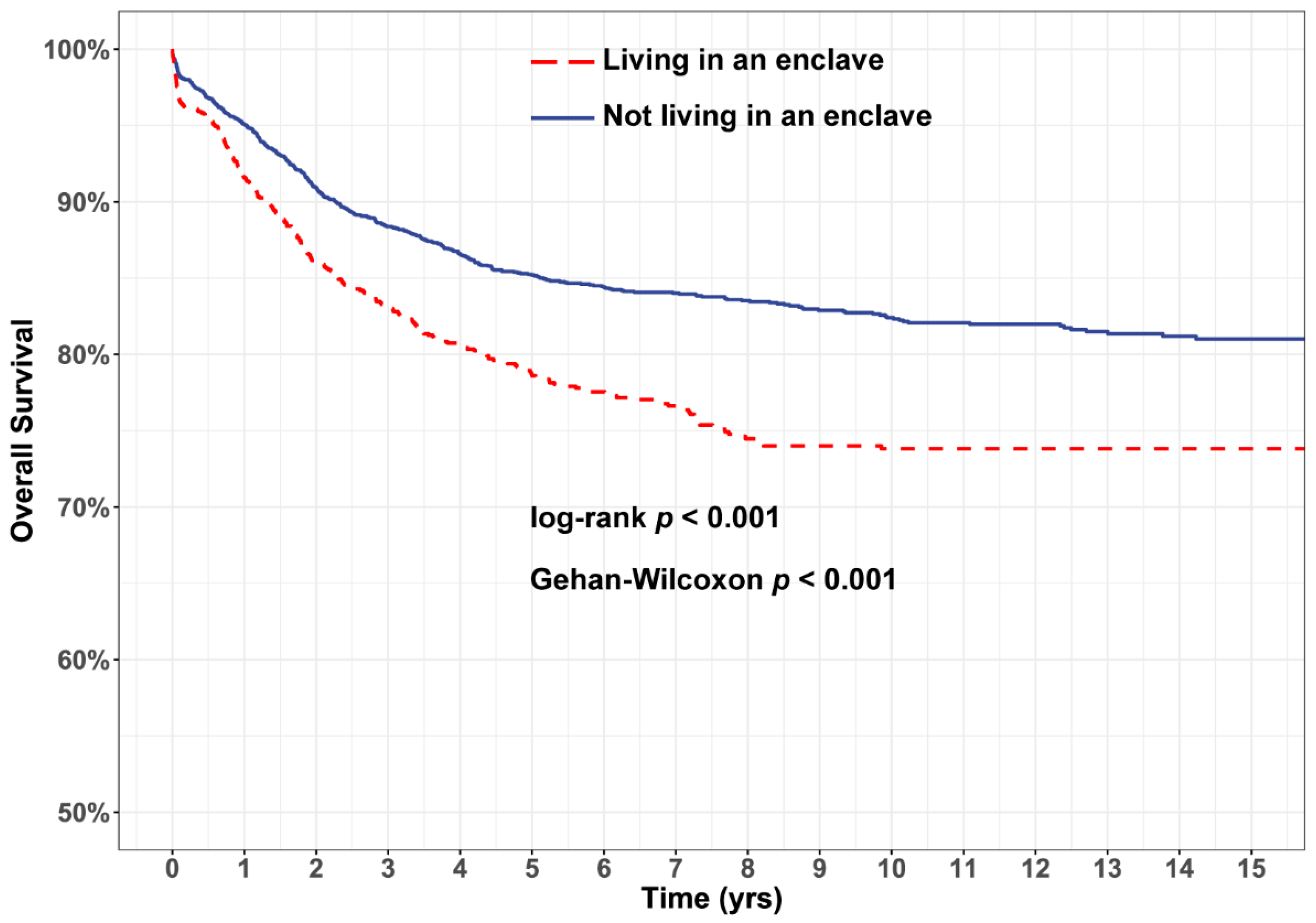
| All children | |||||
| Not living in an enclave | 1790 | 85.8 (84.4–87.3) | 1.00 | 1.00 | 1.00 |
| Living in an enclave | 691 | 78.6 (76.2–81.0) | 1.52 (1.31–1.76) | 1.22 (1.01–1.49) | 1.19 (0.97–1.45) |
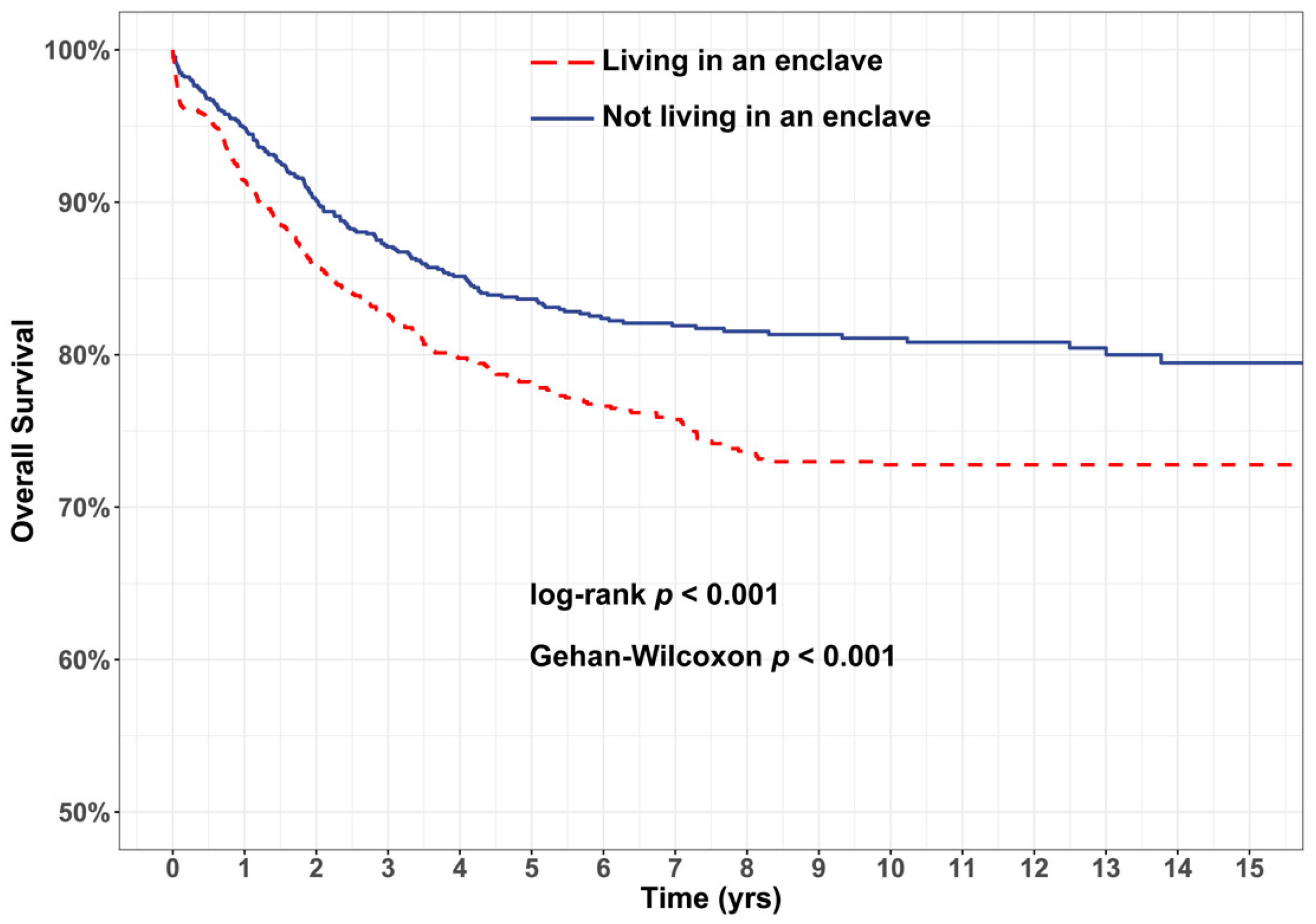
| Hispanic children | |||||
| Not living in an enclave | 626 | 83.7 (81.4–86.0) | 1.00 | 1.00 | - |
| Living in an enclave | 608 | 77.8 (75.3–80.5) | 1.43 (1.19–1.73) | 1.30 (1.03–1.65) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schraw, J.M.; Peckham-Gregory, E.C.; Hughes, A.E.; Scheurer, M.E.; Pruitt, S.L.; Lupo, P.J. Residence in a Hispanic Enclave Is Associated with Inferior Overall Survival among Children with Acute Lymphoblastic Leukemia. Int. J. Environ. Res. Public Health 2021, 18, 9273. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179273
Schraw JM, Peckham-Gregory EC, Hughes AE, Scheurer ME, Pruitt SL, Lupo PJ. Residence in a Hispanic Enclave Is Associated with Inferior Overall Survival among Children with Acute Lymphoblastic Leukemia. International Journal of Environmental Research and Public Health. 2021; 18(17):9273. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179273
Chicago/Turabian StyleSchraw, Jeremy M., Erin C. Peckham-Gregory, Amy E. Hughes, Michael E. Scheurer, Sandi L. Pruitt, and Philip J. Lupo. 2021. "Residence in a Hispanic Enclave Is Associated with Inferior Overall Survival among Children with Acute Lymphoblastic Leukemia" International Journal of Environmental Research and Public Health 18, no. 17: 9273. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179273