
The Seamless Communication on a Rural Island in Japan: A Qualitative Study from the Perspective of Healthcare Professionals



Abstract
:1. Introduction
2. Materials and Methods
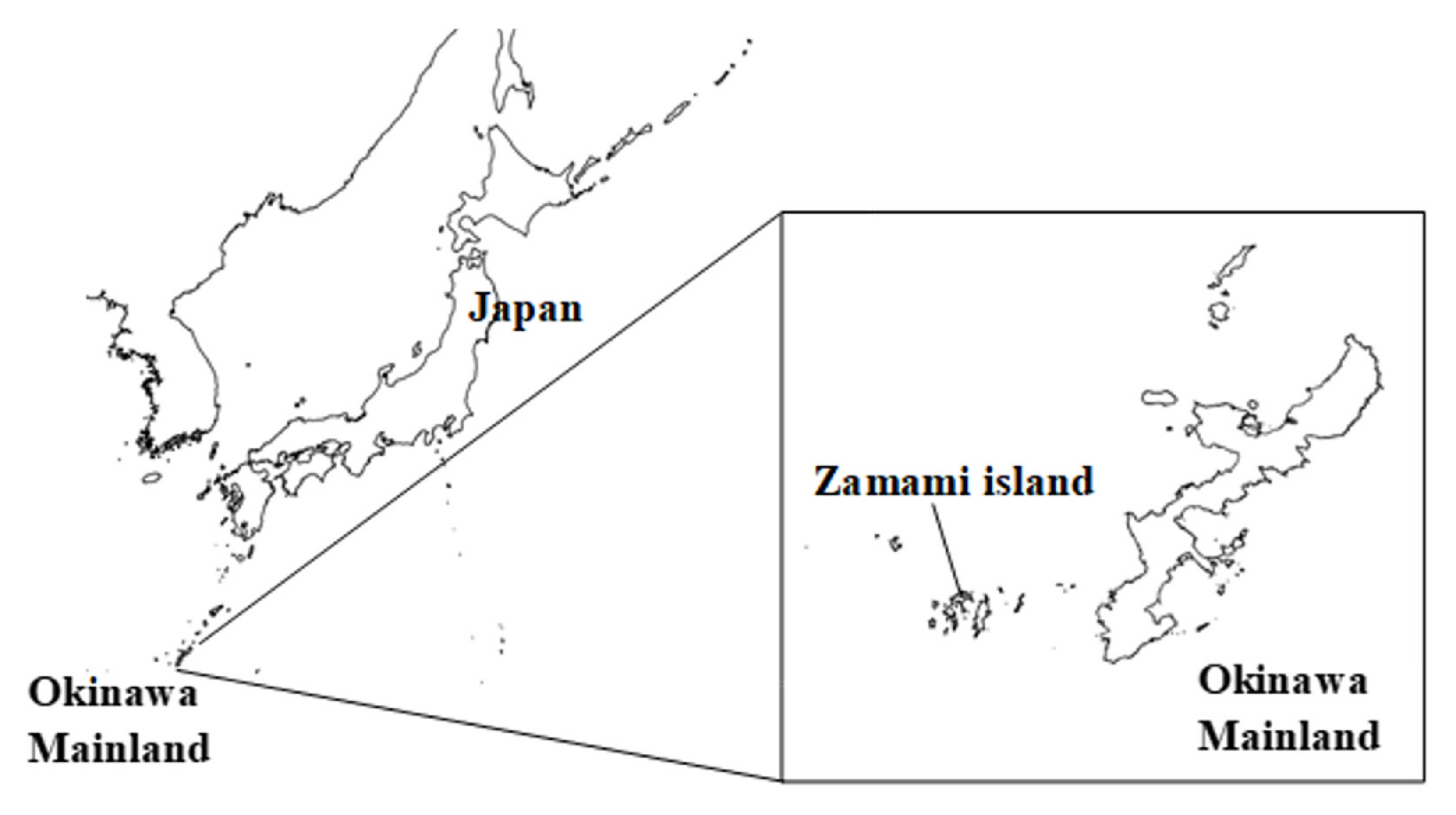
2.1. Setting
2.2. Participants
2.3. Data Collection Method
2.4. Data Analysis
2.5. Ethical Considerations
3. Results
3.1. Collection and Communication of Information between Residents
3.1.1. Watching and Taking Care of Each Other Based on Close Relationships
“We look out for each other, asking questions such as ‘How is that old man?’ We have concern for one another because we have lived in the same island.”
“There tends to be a lot of people who get sick without us becoming aware, and at times, the community residents tend to know more about one another. The community is small enough for each person to know each other well, and quite often, islanders notice changes in the islanders’ conditions faster than we (HCPs) do.”
3.1.2. Residents Consulting Local Leaders
“The head of districts have to distribute local works for people who have lost their jobs and need money. So, they naturally step in-to a private situation.”
“She worked as the head of a district for more than 10 years. Thus, lots of residents trust and rely on her, and they still tell her some essential information.”
3.1.3. Presence of Potential Healthcare Human Resources
“All of us took care worker courses together back in the day. Even if it was not used for work, it helped in providing caregiving for our parents. I think it is also useful that there are some people with nursing qualifications.”
3.2. Communication of Information from Non-HCPs to HCPs
3.2.1. Limitations of Communication between Non-HCPs
“The relationship (between islanders) may be too close. There might be a bit of hesitation since knowing too much about one another might affect the existing relationship.”
3.2.2. Ambiguous Boundaries between the Work and Private Lives of Professionals with a High Affinity to the Region
“I’ve lived here 20 years and have been working as a care worker for 15 of those years. Because of this, I know who to turn to when I need to ask something. You become familiar in 5 to 10 years, but not in 2 to 3 years.”
“I heard about Mr. A from the girl at the supermarket. I went to visit him at home after the girl said that he was acting unusual because he didn’t look at her and didn’t seem to be eating either.”
“A lot of islanders know that I take care of elderly, such as Mr. B and C. Thus, people told me wherever I was; not only at my office but also at the street or the post office, when their condition seemed to be bad.”
3.2.3. Preparation for the Collection of Information by HCPs
“When a guy told me that the light of an old lady’s house continued turning on at midnight these days, I felt that the guy was taking care of and watching over the neighbor. I told him to let me know immediately if anything happened to the old lady.”
“We always exchange greetings, whether or not there is a problem. For example, there was an older man who cared deeply for his goat. He wasn’t very friendly with people, but he was open to showing his goat when I asked to see it. This sort of everyday connection might be important. This could help avoid rejection. Being acquainted with one another before any problem occurs is much better than meeting for the first time after the problem occurs.”
3.2.4. History of Public Health Nurses
“’Ko-kan san (original public health nurses in Okinawa)’ used to go around changing bandages for bedsores and changing diapers. There were public health nurses even at a time when there were no caregiving insurance and no doctors on the island. The current situation might be a remnant of that. I think this is why islanders rely on modern-day public health nurses during times of trouble.”
3.3. Sharing of Information between HCPs
3.3.1. Conducting Regular Meetings
“I tend to look through the minutes of the meetings even if I cannot go to the meetings themselves.”
3.3.2. The Connection between HCPs as Residents
“We always share information. We always speak out if we notice something and speak to one another on the streets. If I am close by, I tend to stop by their workplaces when I am worried or even call them if the situation is urgent.”
3.3.3. Public Health Nurses as an Information Hub
“The public health nurse is the go-to person when something happens. The information always goes through them.”
3.3.4. Ingenuity and Consideration in Sharing Information among HCPs
“We tend to share it once. There is a lot of information about older adults. If the person in charge is already handling the situation, we leave it as it is. I tend to make visits personally if I know the person well. We share information in that manner and start getting involved.”
“We don’t discuss every single piece of information together. We manage the information with the individual’s permission if we judge that it is necessary.”
3.4. HCPs Taking Action to Initiate Their Approach
3.4.1. Division of Roles through Various Meetings
“The public health nurse calls for meetings and formulates care plans, and the nurses at the clinic administer medications. I think it is a good example of interprofessional collaboration.”
3.4.2. Efforts for Better Collaboration with Facilities Outside the Island
“The hospital staff in the mainland may not be aware of the situation on the island, such as the lack of resources. Sometimes, they send patients back to the island without enough preparation.”
“Care managers exchange information with the hospital outside the island when our patients need admission. This is done because it is difficult when they are sent back to the island without calling in advance even though we don’t have enough facilities. Thus, we call and write to the hospital frequently.”
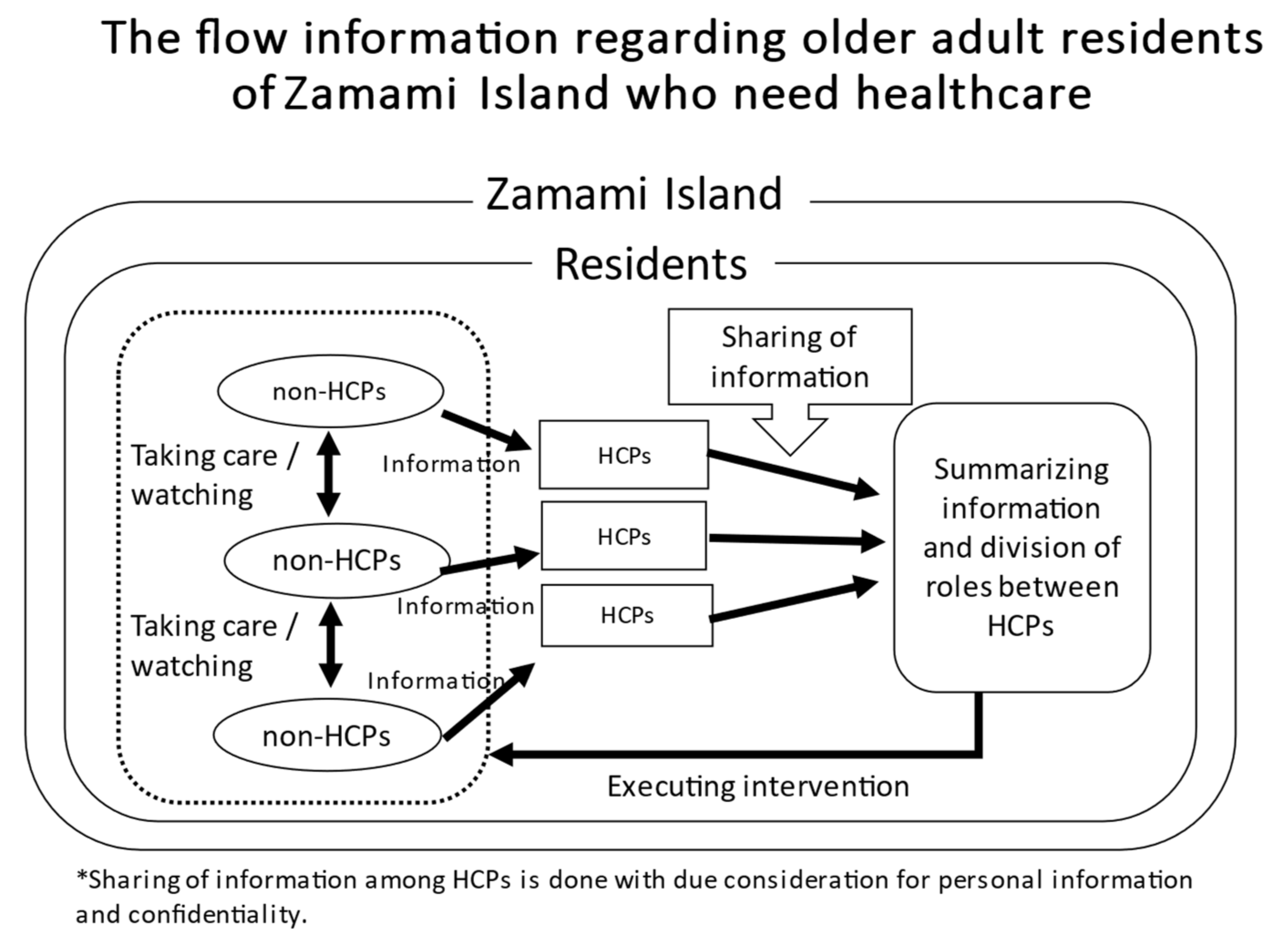
3.5. The Conceptual Diagram of This Study
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministry of Health, Labor and Welfare. About Comprehensive Care. Available online: https://www.mhlw.go.jp/seisakunitsuite/bunya/hukushi_kaigo/kaigo_koureisha/chiiki-houkatsu/dl/link4-1.pdf (accessed on 15 June 2021).
- Ohta, R.; Ueno, A.; Kitayuguchi, J.; Moriwaki, Y.; Otani, J.; Sano, C. Comprehensive care through family medicine: Improving the sustainability of aging societies. Geriatrics 2021, 6, 59. [Google Scholar] [CrossRef] [PubMed]
- Swensen, S.J.; Meyer, G.S.; Nelson, E.C.; Hunt, G.C., Jr.; Pryor, D.B.; Weissberg, J.I.; Kaplan, G.S.; Daley, J.; Yates, G.R.; Chassin, M.R.; et al. Cottage industry to postindustrial care—The revolution in health care delivery. N. Engl. J. Med. 2010, 362, e12. [Google Scholar] [CrossRef] [PubMed]
- Larsen, A.; Broberger, E.; Petersson, P. Complex caring needs without simple solutions: The experience of interprofessional collaboration among staff caring for older persons with multimorbidity at home care settings. Scand. J. Caring Sci. 2017, 31, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Ryu, Y.; Katsube, T. Care managers in rural Japan: Challenges to interprofessional collaboration. Home Health Care Serv. Q. 2019, 38, 270–285. [Google Scholar] [CrossRef]
- Australian Government Productivity Commission. Australia’s Health Workforce Research Report. Available online: https://www.pc.gov.au/inquiries/completed/health-workforce/report/healthworkforce.pdf (accessed on 11 July 2021).
- Gardiner, F.W.; Richardson, A.M.; Bishop, L.; Harwood, A.; Gardiner, E.; Gale, L.; Teoh, N.; Lucas, R.M.; Laverty, M. Health care for older people in rural and remote Australia: Challenges for service provision. Med. J. Aust. 2019, 211, 363–364. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y.; Katsube, T. Challenges for Japanese rural home care workers in interprofessional collaboration: A qualitative study. Home Health Care Serv. Q. 2018, 37, 313–324. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Ryu, Y.; Kitayuguchi, J.; Gomi, T.; Katsube, T. Challenges and solutions in the continuity of home care for rural older people: A thematic analysis. Home Health Care Serv. Q. 2020, 39, 126–139. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y.; Katsube, T.; Sano, C. Rural Homecare Nurses’ Challenges in Providing Seamless Patient Care in Rural Japan. Int. J. Environ. Res. Public Health 2020, 17, 9330. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y.; Kataoka, D.; Sano, C. Effectiveness and Challenges in Local Self-Governance: Multifunctional Autonomy in Japan. Int. J. Environ. Res. Public Health 2021, 18, 574. [Google Scholar] [CrossRef]
- Motomura, K. Reflective practice and situated learning in remote medicine. An. Off. J. Jpn. Prim. Care Assoc. 2012, 35, 165–167. [Google Scholar]
- Kaneko, M.; Aoki, T.; Mori, H.; Ohta, R.; Matsuzawa, H.; Shimabukuro, A.; Motomura, K.; Inoue, M. Associations of patient experience in primary care with hospitalizations and emergency department visits on isolated islands: A prospective cohort study. J. Rural Health 2019, 35, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Yun, K.; Paul, P.; Subedi, P.; Kuikel, L.; Nguyen, G.T.; Barg, F.K. Help-seeking behavior and health care navigation by Bhutanese refugees. J. Community Health 2016, 41, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, R.C.; Manikandan, P.A.; Samuel, A.; Singh, Z. Determinants of health care seeking behavior among rural population of a coastal area in South India. Int. J. Sci. Rep. 2015, 1, 118–122. [Google Scholar] [CrossRef] [Green Version]
- Ohta, R.; Ryu, Y.; Kitayuguchi, J.; Sano, C.; Könings, K.D. Educational intervention to improve citizen’s healthcare participation perception in rural Japanese communities: A pilot study. Int. J. Environ. Res. Public Health 2021, 18, 1782. [Google Scholar] [CrossRef] [PubMed]
- Lauckner, H.M.; Hutchinson, S.L. Peer support for people with chronic conditions in rural areas: A scoping review. Rural Remote Health 2016, 16, 3601. [Google Scholar]
- Ohta, R.; Kamiyama, Y.; Makishi, T. Inquiry into short-term learning on Japanese rural islands: A qualitative study. Educ. Prim. Care 2019, 30, 88–95. [Google Scholar] [CrossRef]
- Horikoshi, N.; Kuwahara, Y.; Taguchi, A.; Nagata, T.; Murashima, S. Home care and place of death for elderly people living in the remote islands of Japan. An examination on the presence of inpatient facilities. Nihon Koshu Eisei Zasshi 2013, 60, 412–421. (In Japanese) [Google Scholar]
- Ohwan, A.; Miyagi, S.; Sakugawa, M.; Okawa, M. Municipal and Geographical Classification of the Remote Islands in Okinawa Prefecture and the Direction of the Development of Community Care System for Elderly. J. Okinawa Prefect. Coll. Nurs. 2005, 6, 40–49. [Google Scholar]
- Zamami Village Office. Zamami Village. Available online: https://www.vill.zamami.okinawa.jp/info/zamami.html (accessed on 21 July 2021).
- Otani, N. SCAT: Steps for coding and theorization—A qualitative data analysis method that is easy to undertake with explicit procedures and can be applied to small-scale data. Kansei Eng. 2011, 10, 155–160. [Google Scholar]
- Motomura, K. Protecting Health Services in the Remote Islands of Okinawa. J. Healthc. Med. Community 2019, 29, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Iha, S. Remote islands and public health nurses Current status and challenges in the Okinawa Prefecture. Jpn. J. Public Health 1986, 50, 535–544. [Google Scholar]
- Ministry of Health, Labour and Welfare. The Role of Community Care Meeting in the Setting of Community-Based Comprehensive Care System. Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-12600000-Seisakutoukatsukan/0000114063_4.pdf (accessed on 21 July 2021).
- Aida, J.; Kondo, K. Social capital and health gap. J. Healthc. Med. Community 2014, 24, 57–74. [Google Scholar]
- Putnam, R. Making Democracy Work: Civic Traditions in Modern Italy; Princeton University Press: Princeton, NJ, USA, 1994; pp. 167–180. [Google Scholar]
- Ohta, R.; Kaneko, M. Effects of practicing in remote Japanese islands on physicians’ control of negative emotions: A qualitative study. J. Rural Med. 2017, 12, 91–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawachi, I. Social capital and community effects on population and individual health. Ann. N. Y. Acad. Sci. 1999, 896, 120–130. [Google Scholar] [CrossRef]
- Onyx, J.; Bullen, P. Measuring social capital in five communities. J. Appl. Behav. Sci. 2000, 36, 23–42. [Google Scholar] [CrossRef]
- Sadler, E.; Wolfe, C.D.; McKevitt, C. Lay and health care professional understandings of self-management: A systematic review and narrative synthesis. SAGE Open Med. 2014, 2. [Google Scholar] [CrossRef] [PubMed]
- Parker, V.; McNeil, K.; Higgins, I.; Mitchell, R.; Paliadelis, P.; Giles, M.; Parmenter, G. How health professionals conceive and construct interprofessional practice in rural settings: A qualitative study. BMC Health Serv. Res. 2013, 13, 500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohta, R.; Ryu, Y.; Katsube, T. Home care workers’ judgments about users’ acute conditions: A qualitative study on interprofessional collaboration. Home Health Care Serv. Q. 2020, 39, 184–195. [Google Scholar] [CrossRef] [PubMed]
- Bahrami, M.A.; Montazeralfaraj, R.; Gazar, S.H.; Tafti, A.D. Relationship between organizational perceived justice and organizational citizenship behavior among an Iranian hospital’s employees, 2013. Electron. Physician 2014, 6, 838–844. [Google Scholar] [PubMed]
- McNeil, K.; Mitchell, R.; Parker, V. The paradoxical effects of workforce shortages on rural interprofessional practice. Scand. J. Caring Sci. 2015, 29, 73–82. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Themes | Concepts |
|---|---|
| Collection and communication of information between residents | Watching and taking care of each other based on close relationships Residents consulting local leaders Presence of potential healthcare human resources |
| Communication of information from non-HCPs to HCPs | Limitations of communication between non-HCPs Ambiguous boundaries between the work and private lives of professionals with a high affinity to the region Preparation for the collection of information by HCPs History of public health nurses |
| Sharing of information between HCPs | Conducting regular meetings The connection between HCPs as residents Public health nurses as an information hub Ingenuity and consideration in sharing information among HCPs |
| HCPs taking action to initiate their approach | Division of roles through various meetings Efforts for better collaboration with facilities outside the island |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuroda, M.; Ohta, R.; Kuroda, K.; Yamashiro, S.; Kita, K. The Seamless Communication on a Rural Island in Japan: A Qualitative Study from the Perspective of Healthcare Professionals. Int. J. Environ. Res. Public Health 2021, 18, 9479. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189479
Kuroda M, Ohta R, Kuroda K, Yamashiro S, Kita K. The Seamless Communication on a Rural Island in Japan: A Qualitative Study from the Perspective of Healthcare Professionals. International Journal of Environmental Research and Public Health. 2021; 18(18):9479. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189479
Chicago/Turabian StyleKuroda, Moe, Ryuichi Ohta, Kaku Kuroda, Seiji Yamashiro, and Keiichiro Kita. 2021. "The Seamless Communication on a Rural Island in Japan: A Qualitative Study from the Perspective of Healthcare Professionals" International Journal of Environmental Research and Public Health 18, no. 18: 9479. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189479