
Sleep Bruxism in Children: Etiology, Diagnosis, and Treatment—A Literature Review

 ,
,  ,
,
Abstract
:1. Introduction
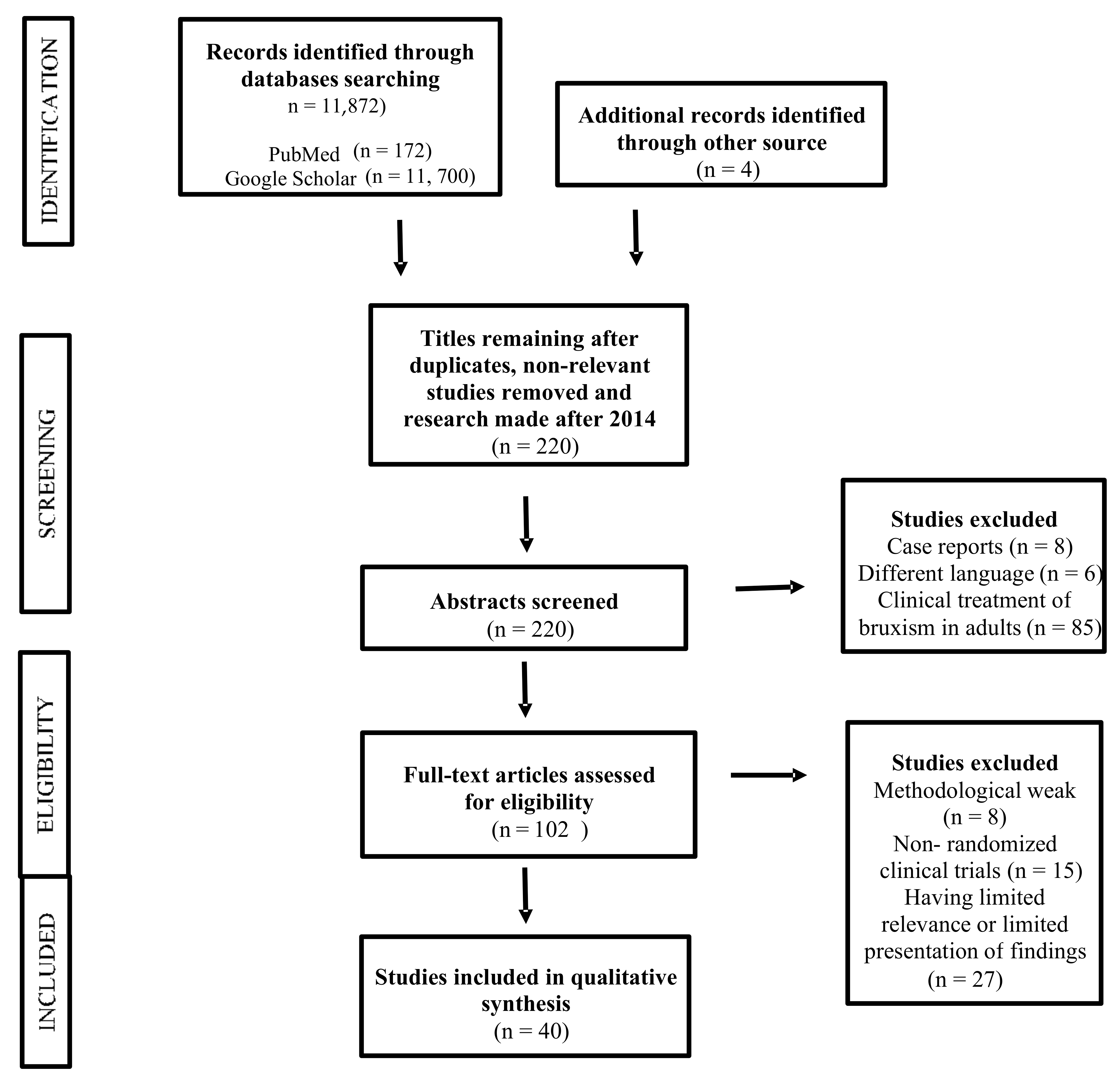
2. Materials and Methods
- (1)
- Randomized clinical trials (RCTs) and observational studies evaluating the association between risk factors and bruxism;
- (2)
- RCTs and observational studies evaluating the diagnosis of bruxism; and
- (3)
- RCTs and observational studies examining the treatment of patients with SB.
- (1)
- Case reports;
- (2)
- Articles published in other languages than English and;
- (3)
- Articles describing the methods used for clinical treatment in adult bruxers.
3. Results
4. Discussion
4.1. Etiology of Bruxism in Children
4.2. Diagnosis of Bruxism in Children
- Tooth grinding or clenching while sleeping and;
- One or more of the following:
- -
- Abnormally worn teeth;
- -
- Bruxism-related sounds; and;
- -
- Mandible muscle discomfort [4].
4.3. Treatment of Bruxism in Children
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lobbezoo, F.; Ahlberg, J.; Raphael, K.G.; Wetselaar, P.; Glaros, A.G.; Kato, T.; Santiago, V.; Winocur, E.; De Laat, A.; De Leeuw, R.; et al. International consensus on the assessment of bruxism: Report of a work in progress. J. Oral Rehabil. 2018, 45, 837–844. [Google Scholar] [CrossRef]
- Alves, C.L.; Fagundes, D.M.; Soares, P.B.F.; Ferreira, M.C. Knowledge of parents/caregivers about bruxism in children treated at the pediatric dentistry clinic. Sleep Sci. 2019, 12, 185–189. [Google Scholar] [CrossRef]
- Castroflorio, T.; Bargellini, A.; Rossini, G.; Cugliari, G.; Rainoldi, A.; Deregibus, A. Risk factors related to sleep bruxism in children: A systematic literature review. Arch. Oral Biol. 2015, 60, 1618–1624. [Google Scholar] [CrossRef]
- Sateia, M.J. International classification of sleep disorders-third edition: Highlights and modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef]
- Zieliński, G.; Ginszt, M.; Suwała, M.; Szkutnik, J.; Majcher, P. Influence of sleep bruxism on primary headaches in children: A 2013–2018 literature review. Pediatr. Med. Rodz. 2019, 15, 374–377. [Google Scholar] [CrossRef]
- Firmani, M.; Reyes, M.; Becerra, N.; Flores, G.; Weitzman, M.; Espinosa, P. Sleep bruxism in children and adolescents. Rev. Chil. Pediatr. 2015, 86, 373–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dharmadhikari, S.; Romito, L.M.; Dzemidzic, M.; Dydak, U.; Xu, J.; Bodkin, C.L.; Manchanda, S.; Byrd, K.E. GABA and glutamate levels in occlusal splint-wearing males with possible bruxism. Arch. Oral Biol. 2015, 60, 1021–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saczuk, K.; Wilmont, P.; Pawlak, Ł.; Łukomska-Szymańska, M. Bruxism: Aetiology and diagnostics. A literature review. Prosthodontics 2018, 68, 456–463. [Google Scholar] [CrossRef]
- Oliveira, M.T.; Bittencourt, S.T.; Marcon, K.; Destro, S.; Pereira, J.R. Sleep bruxism and anxiety level in children. Braz. Oral Res. 2015, 29, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Beddis, H.; Pemberton, M.; Davies, S. Sleep bruxism: An overview for clinicians. Br. Dent. J. 2018, 225, 497–501. [Google Scholar] [CrossRef]
- Alfano, C.A.; Bower, J.L.; Meers, J.M. Polysomnography-Detected Bruxism in Children is Associated With Somatic Complaints But Not Anxiety. J. Clin. Sleep Med. 2018, 14, 23–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sousa, H.C.S.; Lima, M.D.M.; Neta, N.B.D.; Tobias, R.Q.; Moura, M.S.; Moura, L.F.A. Prevalence and associated factors to sleep bruxism in adolescents from Teresina, Piauí. Rev. Bras. Epidemiol. 2018, 21, e180002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manfredini, D.; Ahlberg, J.; Winocur, E.; Lobbezoo, F. Management of sleep bruxism in adults: A qualitative systematic literature review. J. Oral Rehabil. 2015, 42, 862–874. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Statistics; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Gomes, A.A.; Parchao, C.; Almeida, A.; Clemente, V.; Azevedo, M.H.P. Sleep-wake patterns reported by parents in hyperactive children diagnosed according to ICD-10, as compared to paired controls. Child Psychiatry Hum. Dev. 2014, 45, 533–543. [Google Scholar] [CrossRef] [Green Version]
- Gomes, M.C.; Neves, E.T.; Perazzo, M.F.; Souza, E.G.C.; Serra-Negra, J.M.; Paiva, S.M.; Granville-Garcia, A.F. Evaluation of the association of bruxism, psychosocial and sociodemographic factors in preschoolers. Braz. Oral Res. 2018, 32, e009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chinthakanan, S.; Laosuwan, K.; Boonyawong, P.; Kumfu, S.; Chattipakorn, N.; Chattipakorn, S.C. Reduced heart rate variability and increased saliva cortisol in patients with TMD. Arch. Oral Biol. 2018, 90, 125–129. [Google Scholar] [CrossRef]
- Tsitadze, T.; Puturidze, S.; Lomidze, T.; Margvelashvili, V.; Kalandadze, M. Prevalence and risk-factors of bruxism in children and adolescent population and its impact on quality of life (review). Georgian Med. News 2021, 310, 36–39. [Google Scholar]
- Ferreira, N.M.; Santos, J.F.; Santos, M.B.; Marchini, L. Sleep bruxism associated with obstructive sleep apnea syndrome in children. Cranio 2014, 33, 251–255. [Google Scholar] [CrossRef]
- Serra-Negra, J.M.; Paiva, S.M.; Fulgêncio, L.B.; Chavez, B.A.; Lage, C.F.; Pordeus, I.A. Environmental factors, sleep duration, and sleep bruxism in Brazilian schoolchildren: A case-control study. Sleep Med. 2014, 15, 236–239. [Google Scholar] [CrossRef]
- Khoury, S.; Rouleau, G.A.; Rompré, P.H.; Mayer, P.; Montplaisir, J.; Lavigne, G. A significant increase in breathing amplitude precedes sleep bruxism. Chest 2008, 134, 332–337. [Google Scholar] [CrossRef]
- Więckiewicz, M.; Bogunia-Kubik, K.; Mazur, G.; Danel, D.; Smardz, J.; Wojakowska, A.; Poreba, R.; Dratwa, M.; Chaszczewska-Markowska, M.; Winocur, E.; et al. Genetic basis of sleep bruxism and sleep apnea—Response to a medical puzzle. Sci. Rep. 2020, 10, 7497. [Google Scholar] [CrossRef]
- Carra, M.C.; Huynh, N.; Lavigne, G. Sleep Bruxism: A Comprehensive Overview for the Dental Clinician Interested in Sleep Medicine. Dent. Clin. N. Am. 2012, 56, 387–413. [Google Scholar] [CrossRef]
- Da Silva, C.G.; Pachêco-Pereira, C.; Porporatti, A.L.; Savi, M.G.; Peres, M.A.; Flores-Mir, C.; Canto Gde, L. Prevalence of clinical signs of intra-articular temporomandibular disorders in children and adolescents: A systematic review and meta-analysis. J. Am. Dent. Assoc. 2016, 147, 10–18.e8. [Google Scholar] [CrossRef]
- Kobayashi, F.Y.; Gavião, M.B.D.; Marquezin, M.C.S.; Fonseca, F.L.A.; Montes, A.B.M.; de Souza Barbosa, T.; Castelo, P.M. Salivary stress biomarkers and anxiety symptoms in children with and without temporomandibular disorders. Braz. Oral Res. 2017, 31, e78. [Google Scholar] [CrossRef] [Green Version]
- Raphael, K.G.; Janal, M.N.; Sirois, D.A.; Dubrovsky, B.; Klausner, J.J.; Krieger, A.C.; Levigne, G.J. Validity of self-reported sleep bruxism among myofascial temporomandibular disorder patients and controls. J. Oral Reahabil. 2015, 42, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Deregibus, A.; Castroflorio, T.; Bargellini, A. Reliability of a portable device for the detection of sleep bruxism. Clin. Oral Investig. 2014, 18, 2037–2043. [Google Scholar] [CrossRef]
- Castroflorio, T.; Bargellini, A.; Rossini, G.; Cugliari, G.; Deregibus, A. Agreement between clinical and portable EMG/ECG diagnosis of sleep bruxism. J. Oral Rehabil. 2015, 42, 759–764. [Google Scholar] [CrossRef]
- Veiga, N.; Ângelo, T.; Ribeiro, O.; Baptista, A. Bruxism—Literature review. Int. J. Dent. Oral Health 2015, 1. [Google Scholar] [CrossRef] [Green Version]
- Guaita, M.; Högl, B. Current Treatments of Bruxism. Curr. Treat. Options Neurol. 2016, 18, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Consolação Canuto Salgueiro, M.; Bortoletto, C.C.; Ratto Tempestini Horliana, A.C.; Costa Mota, A.C.; Jansiski Motta, L.; de Barros Motta, P.; Mesquita Ferrari, R.A.; Porta Santos Fernandes, K.; Kalil Bussadoricorresponding, S. Evaluation of muscle activity, bite force and salivary cortisol in children with bruxism before and after low level laser applied to acupoints: Study protocol for a randomized controlled trial. BMC Complement. Altern. Med. 2017, 17, 391. [Google Scholar]
- Pihut, M.; Ferendiuk, E.; Szewczyk, M.; Kasprzyk, K.; Wieckiewicz, M. The efficiency of botulinum toxin type A for the treatment of masseter muscle pain in patients with temporomandibular joint dysfunction and tension-type headache. J. Headache Pain 2016, 17, 29. [Google Scholar] [CrossRef] [Green Version]
- Bellerive, A.; Montpetit, A.; El-Khatib, H. The effect of rapid palatal expansion on sleep bruxism in children. Sleep Breath. 2015, 19, 1265–1271. [Google Scholar] [CrossRef] [PubMed]
- Nitecka-Buchta, A.; Walczynska-Dragon, K.; Batko-Kapustecka, J.; Wieckiewicz, M. Comparison between Collagen and Lidocaine Intramuscular Injections in Terms of Their Efficiency in Decreasing Myofascial Pain within Masseter Muscles: A Randomized, Single-Blind Controlled Trial. Pain Res. Manag. 2018, 2018, 8261090. [Google Scholar] [CrossRef] [Green Version]
- Mostafavi, S.M.; Jafari, A.; Hoseini, S.G.; Khademian, M.; Kelishadi, R. The efficacy of low and moderate dosage of diazepam on sleep bruxism in children: A randomized placebo-controlled clinical trial. J. Res. Med. Sci. 2019, 31, 24–28. [Google Scholar]
- Ghanizadeh, A. Treatment of bruxism with hydroxyzine. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 839–841. [Google Scholar] [PubMed]
- Salgueiro, M.C.C.; Silva, T.; Jansiski Motta, L.; Ratto Tempestini Horliana, A.C.; Leal Gonçalves, C.L.; Gomes, A.O.; Pinto, M.M.; Carvalho Bortoletto, C.; Altavista, O.M.; Melo Deana, A. Effects of Photobiomodulation in Children with Down Syndrome and Possible Sleep Bruxism: Protocol For A Randomized, Controlled, Blind, Clinical Trial. Medicine 2020, 99, e19904. [Google Scholar] [CrossRef]
- Salgueiro, M.C.C.; Kobayashi, F.Y.; Jansiski Motta, L.; Leal Gonçalves, M.L.; Ratto Tempestini Horliana, A.C.; Mesquita-Ferrari, R.A.; Porta Santos Fernandes, K.; Gomes, A.O.; Brugnera Junior, A.; Kalil Bussadori, S. Effect of Photobiomodulation on Salivary Cortisol, Masticatory Muscle Strength, and Clinical Signs in Children with Sleep Bruxism: A Randomized Controlled Trial. Photobiomodul. Photomed. Laser Surg. 2021, 39, 23–29. [Google Scholar] [CrossRef]
- Valiente López, M.; van Selms, M.K.A.; van der Zaag, J.; Hamburger, H.L.; Lobbezoo, F. Do sleep hygiene measures and progressive muscle relaxation influence sleep bruxism? Report of a randomized controlled trial. J. Oral Rehabil. 2015, 42, 259–265. [Google Scholar] [CrossRef]
- Kün-Darbois, J.D.; Libouban, H.; Chappard, D. Botulinum toxin in masticatory muscles of the adult rat induces bone loss at the condyle and alveolar regions of the mandible associated with a bone proliferation at a muscle enthesis. Bone 2015, 77, 75–82. [Google Scholar] [CrossRef]
- Bahali, K.; Yalcin, O.; Avci, A. Atomoxetine-induced wake-time teeth clenching and sleep bruxism in a child patient. Eur. Child Adolesc. Psychiatry 2014, 23, 1233–1235. [Google Scholar] [CrossRef]


{kind=link}
| Patient History | Clinical Evaluation |
|---|---|
|
|
| Treatment Method | Authors |
|---|---|
| Use of low and moderate doses of diazepam | S.N. Mostafavi et al. [35] |
| Oral administration of hydroxyzine | A. Ghanizadeh [36] |
| Photobiomodulation | M.C.C. Salgueiro et al. [37] |
| Orthodontic treatment (rapid palatal expansion) | A. Bellerive et al. [33] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bulanda, S.; Ilczuk-Rypuła, D.; Nitecka-Buchta, A.; Nowak, Z.; Baron, S.; Postek-Stefańska, L. Sleep Bruxism in Children: Etiology, Diagnosis, and Treatment—A Literature Review. Int. J. Environ. Res. Public Health 2021, 18, 9544. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189544
Bulanda S, Ilczuk-Rypuła D, Nitecka-Buchta A, Nowak Z, Baron S, Postek-Stefańska L. Sleep Bruxism in Children: Etiology, Diagnosis, and Treatment—A Literature Review. International Journal of Environmental Research and Public Health. 2021; 18(18):9544. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189544
Chicago/Turabian StyleBulanda, Sylwia, Danuta Ilczuk-Rypuła, Aleksandra Nitecka-Buchta, Zuzanna Nowak, Stefan Baron, and Lidia Postek-Stefańska. 2021. "Sleep Bruxism in Children: Etiology, Diagnosis, and Treatment—A Literature Review" International Journal of Environmental Research and Public Health 18, no. 18: 9544. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189544