
Dual-Task-Based Drum Playing with Rhythmic Cueing on Motor and Attention Control in Patients with Parkinson’s Disease: A Preliminary Randomized Study


Abstract
:1. Introduction
2. Materials and Methods
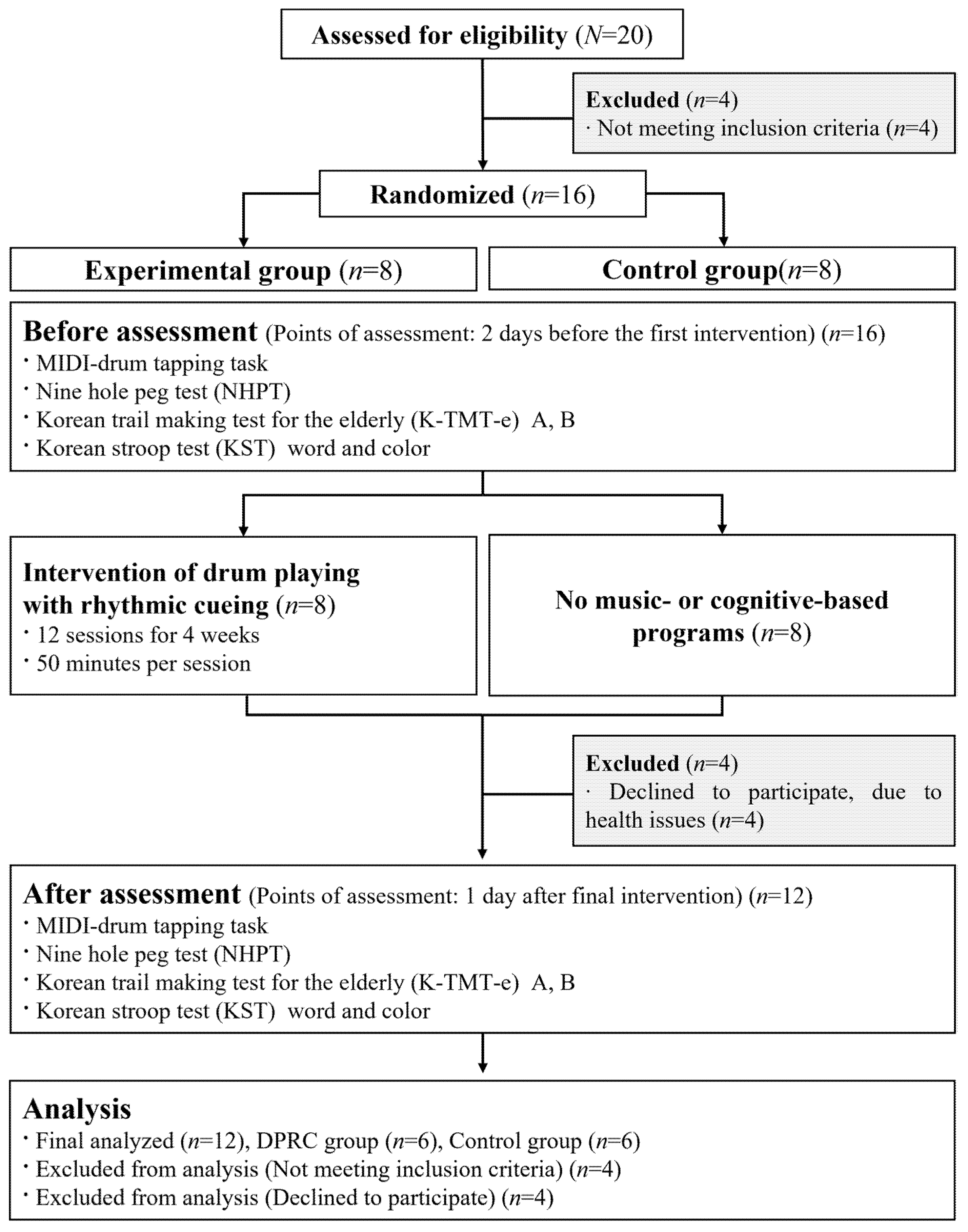
2.1. Participants
2.2. Procedure
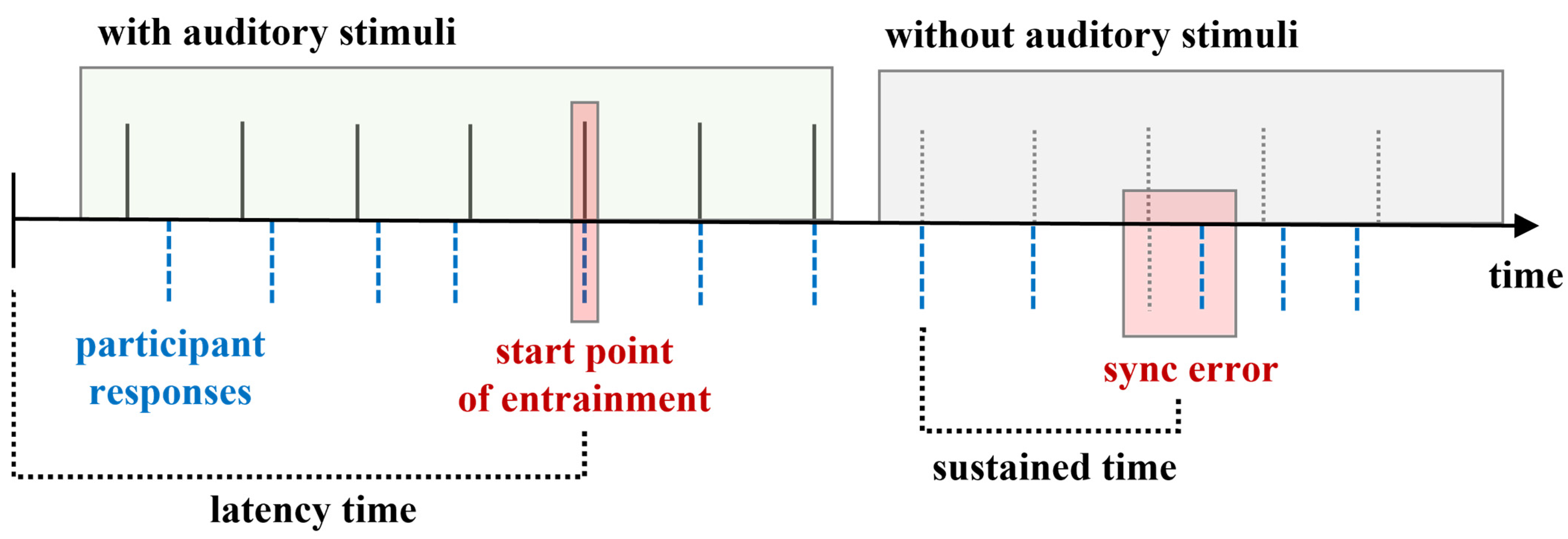
2.3. Measurements
2.4. Intervention of Drum Playing with Rhythmic Cueing
2.5. Data Collection and Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Crowley, E.; Nolan, Y.; Sullivan, A. Exercise as a therapeutic intervention for motor and non-motor symptoms in Parkinson’s disease: Evidence from rodent models. Prog. Neurobiol. 2019, 172, 2–22. [Google Scholar] [CrossRef]
- Braak, H.; Del Tredici, K.; Rüb, U.; De Vos, R.A.; Steur, E.N.J.; Braak, E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol. Aging 2003, 24, 197–211. [Google Scholar] [CrossRef]
- Remz, M.; Salinas, M. Psychosis in Parkinson’s Disease. Psychiatr. Ann. 2020, 50, 113–120. [Google Scholar] [CrossRef]
- Rodriguez-Oroz, M.C.; Jahanshahi, M.; Krack, P.; Litvan, I.; Macias, R.; Bezard, E.; Obeso, J.A. Initial clinical manifestations of Parkinson’s disease: Features and pathophysiological mechanisms. Lancet Neurol. 2009, 8, 1128–1139. [Google Scholar] [CrossRef] [Green Version]
- Robbins, T.W.; Cools, R. Cognitive deficits in Parkinson’s disease: A cognitive neuroscience perspective. Mov. Disord. 2014, 29, 597–607. [Google Scholar] [CrossRef] [PubMed]
- Venderova, K.; Park, D.S. Programmed cell death in Parkinson’s disease. Cold Spring Harb. Perspect. Med. 2012, 2, a009365. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.-C.; Hsieh, Y.-W.; Wu, C.-Y.; Chen, C.-L.; Jang, Y.; Liu, J.-S. Minimal detectable change and clinically important difference of the Wolf Motor Function Test in stroke patients. Neurorehabilit. Neural Repair 2009, 23, 429–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moustafa, A.A.; Chakravarthy, S.; Phillips, J.R.; Gupta, A.; Keri, S.; Polner, B.; Frank, M.J.; Jahanshahi, M. Motor symptoms in Parkinson’s disease: A unified framework. Neurosci. Biobehav. Rev. 2016, 68, 727–740. [Google Scholar] [CrossRef] [PubMed]
- Almeida, Q.J.; Wishart, L.R.; Lee, T.D. Disruptive influences of a cued voluntary shift on coordinated movement in Parkinson’s disease. Neuropsychologia 2003, 41, 442–452. [Google Scholar] [CrossRef]
- Yarnall, A.J.; Breen, D.P.; Duncan, G.W.; Khoo, T.K.; Coleman, S.Y.; Firbank, M.J.; Nombela, C.; Winder-Rhodes, S.; Evans, J.R.; Rowe, J.B. Characterizing mild cognitive impairment in incident Parkinson disease: The ICICLE-PD study. Neurology 2014, 82, 308–316. [Google Scholar] [CrossRef] [Green Version]
- Amboni, M.; Barone, P.; Hausdorff, J.M. Cognitive contributions to gait and falls: Evidence and implications. Mov. Disord. 2013, 28, 1520–1533. [Google Scholar] [CrossRef]
- Derejko, M.; Slawek, J.; Wieczorek, D.; Brockhuis, B.; Dubaniewicz, M.; Lass, P. Regional cerebral blood flow in Parkinson’s disease as an indicator of cognitive impairment. Nucl. Med. Commun. 2006, 27, 945–951. [Google Scholar] [CrossRef] [PubMed]
- Lawson, R.A.; Yarnall, A.J.; Duncan, G.W.; Breen, D.P.; Khoo, T.K.; Williams-Gray, C.H.; Barker, R.A.; Collerton, D.; Taylor, J.-P.; ICICLE-PD Study Group. Cognitive decline and quality of life in incident Parkinson’s disease: The role of attention. Parkinsonism Relat. Disord. 2016, 27, 47–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shipley, B.A.; Der, G.; Taylor, M.D.; Deary, I.J. Cognition and mortality from the major causes of death: The Health and Lifestyle Survey. J. Psychosom. Res. 2008, 65, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Chen, X.; Wang, C.; Yin, C.; Hu, P.; Wang, K. Selective attention deficits in early and moderate stage Parkinson’s disease. Neurosci. Lett. 2012, 509, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Willis, A.W.; Schootman, M.; Kung, N.; Evanoff, B.A.; Perlmutter, J.S.; Racette, B.A. Predictors of survival in patients with Parkinson disease. Arch. Neurol. 2012, 69, 601–607. [Google Scholar] [PubMed] [Green Version]
- Yogev, G.; Giladi, N.; Peretz, C.; Springer, S.; Simon, E.S.; Hausdorff, J.M. Dual tasking, gait rhythmicity, and Parkinson’s disease: Which aspects of gait are attention demanding? Eur. J. Neurosci. 2005, 22, 1248–1256. [Google Scholar] [CrossRef]
- Jankovic, J. Parkinson’s disease: Clinical features and diagnosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 368–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, T.; Hallett, M. A functional MRI study of automatic movements in patients with Parkinson’s disease. Brain 2005, 128, 2250–2259. [Google Scholar] [CrossRef] [Green Version]
- Plummer-D’Amato, P.; Altmann, L.J.; Behrman, A.L.; Marsiske, M. Interference between cognition, double-limb support, and swing during gait in community-dwelling individuals poststroke. Neurorehabilit. Neural Repair 2010, 24, 542–549. [Google Scholar] [CrossRef]
- Silsupadol, P.; Siu, K.-C.; Shumway-Cook, A.; Woollacott, M.H. Training of balance under single-and dual-task conditions in older adults with balance impairment. Phys. Ther. 2006, 86, 269–281. [Google Scholar] [CrossRef] [Green Version]
- Yogev-Seligmann, G.; Hausdorff, J.M.; Giladi, N. The role of executive function and attention in gait. Mov. Disord. Off. J. Mov. Disord. Soc. 2008, 23, 329–342. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.; Hallett, M. The cerebellum in Parkinson’s disease. Brain 2013, 136, 696–709. [Google Scholar] [CrossRef] [Green Version]
- Fritz, N.E.; Cheek, F.M.; Nichols-Larsen, D.S. Motor-cognitive dual-task training in neurologic disorders: A systematic review. J. Neurol. Phys. Ther. 2015, 39, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.J.; Cho, S.-R.; Yoo, G.E. The applicability of rhythm-motor tasks to a new dual task paradigm for older adults. Front. Neurol. 2017, 8, 671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terrier, P.; Reynard, F. Effect of age on the variability and stability of gait: A cross-sectional treadmill study in healthy individuals between 20 and 69 years of age. Gait Posture 2015, 41, 170–174. [Google Scholar] [CrossRef] [Green Version]
- Herman, T.; Mirelman, A.; Giladi, N.; Schweiger, A.; Hausdorff, J.M. Executive control deficits as a prodrome to falls in healthy older adults: A prospective study linking thinking, walking, and falling. Biomed. Sci. Med. Sci. 2010, 65, 1086–1092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.L.; Zatorre, R.J.; Penhune, V.B. Interactions between auditory and dorsal premotor cortex during synchronization to musical rhythms. Neuroimage 2006, 32, 1771–1781. [Google Scholar] [CrossRef] [PubMed]
- Haslinger, B.; Erhard, P.; Altenmüller, E.; Schroeder, U.; Boecker, H.; Ceballos-Baumann, A.O. Transmodal sensorimotor networks during action observation in professional pianists. J. Cogn. Neurosci. 2005, 17, 282–293. [Google Scholar] [CrossRef] [PubMed]
- LaGasse, A.B.; Knight, A. Rhythm and music in rehabilitation: A critical review of current research. Crit. Rev. Phys. Rehabil. Med. 2011, 23, 49–67. [Google Scholar] [CrossRef]
- Thaut, M.H.; Stephan, K.M.; Wunderlich, G.; Schicks, W.; Tellmann, L.; Herzog, H.; McIntosh, G.C.; Seitz, R.J.; Hömberg, V. Distinct cortico-cerebellar activations in rhythmic auditory motor synchronization. Cortex 2009, 45, 44–53. [Google Scholar] [CrossRef]
- Molinari, M.; Leggio, M.G.; De Martin, M.; Cerasa, A.; Thaut, M. Neurobiology of rhythmic motor entrainment. Ann. N. Y. Acad. Sci. 2003, 999, 313–321. [Google Scholar] [CrossRef]
- Alexander, J.S.; Fachner, J.; Magee, W.L. Upper limb rehabilitation in chronic stroke using neurologic music therapy: Two contrasting case studies to inform on treatment delivery and patient suitability. Nord. J. Music Ther. 2019, 28, 382–404. [Google Scholar]
- Malcolm, M.P.; Massie, C.; Thaut, M. Rhythmic auditory-motor entrainment improves hemiparetic arm kinematics during reaching movements: A pilot study. Top. Stroke Rehabil. 2009, 16, 69–79. [Google Scholar] [CrossRef]
- Vervoort, G.; Heremans, E.; Bengevoord, A.; Strouwen, C.; Nackaerts, E.; Vandenberghe, W.; Nieuwboer, A. Dual-task-related neural connectivity changes in patients with Parkinson’s disease. Neuroscience 2016, 317, 36–46. [Google Scholar] [CrossRef]
- Schroeder, C.E.; Lakatos, P. Low-frequency neuronal oscillations as instruments of sensory selection. Trends Neurosci. 2009, 32, 9–18. [Google Scholar] [CrossRef] [Green Version]
- Bella, S.D.; Benoit, C.E.; Farrugia, N.; Schwartze, M.; Kotz, S.A. Effects of musically cued gait training in Parkinson’s disease: Beyond a motor benefit. Ann. N. Y. Acad. Sci. 2015, 1337, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Galletly, R.; Brauer, S.G. Does the type of concurrent task affect perferred and cued gait in people with Parkinson’s disease? Aust. J. Physiother. 2005, 51, 175–180. [Google Scholar] [CrossRef] [Green Version]
- Braunlich, K.; Seger, C.A.; Jentink, K.G.; Buard, I.; Kluger, B.M.; Thaut, M.H. Rhythmic auditory cues shape neural network recruitment in Parkinson’s disease during repetitive motor behavior. Eur. J. Neurosci. 2019, 49, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Alberts, J.L.; Saling, M.; Adler, C.H.; Stelmach, G.E. Disruptions in the reach-to-grasp actions of Parkinson’s patients. Exp. Brain Res. 2000, 134, 353–362. [Google Scholar] [CrossRef]
- Pelton, T.; van Vliet, P.; Hollands, K. Interventions for improving coordination of reach to grasp following stroke: A systematic review. Int. J. Evid. Based Healthc. 2012, 10, 89–102. [Google Scholar] [CrossRef]
- Ma, H.I.; Hwang, W.J.; Lin, K.C. The effects of two different auditory stimuli on functional arm movement in persons with Parkinson’s disease: A dual-task paradigm. Clin. Rehabil. 2009, 23, 229–237. [Google Scholar] [CrossRef]
- Wu, T.; Hallett, M.; Chan, P. Motor automaticity in Parkinson’s disease. Neurobiol. Aging. 2015, 82, 226–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression, and mortality. Neurology. 1998, 50, 318. [Google Scholar] [CrossRef] [PubMed]
- Shin, M.H.; Lee, Y.M.; Park, J.M.; Kang, C.J.; Lee, B.D.; Moon, E.; Chung, Y.I. A combination of the Korean version of the mini-mental state examination and Korean dementia screening questionnaire is a good screening tool for dementia in the elderly. Psychiatry Investig. 2011, 8, 348. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Cho, S.R.; Yoo, G.E. Age-Related Changes in Bimanual Instrument Playing with Rhythmic Cueing. Front. Psychol. 2017, 8, 1569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathiowetz, V.; Weber, K.; Kashman, N.; Volland, G. Adult norms for the nine hole peg test of finger dexterity. Occup. Ther. J. Res. 1985, 5, 24–38. [Google Scholar] [CrossRef]
- Jang, J.W.; Kim, K.; Baek, M.J.; Kim, S.Y. A comparison of five types of trail making test in Korean elderly. Dement. Neurocognitive Disord. 2016, 15, 135–141. [Google Scholar] [CrossRef] [Green Version]
- Seo, E.H.; Lee, D.Y.; Choo, I.H.; Kim, S.G.; Kim, K.W.; Youn, J.C.; Jhoo, J.H.; Woo, J.I. Normative study of the stroop color and word test in an educationally diverse elderly population. Int. J. Geriatr. Psychiatry 2008, 23, 1020–1027. [Google Scholar] [CrossRef]
- Ludwig, C.; Borella, E.; Tettamanti, M.; De Ribaupierre, A. Adult age differences in the Color Stroop Test: A comparison between an Item-by-item and a Blocked version. Arch. Gerontol. Geriatr. 2010, 51, 135–142. [Google Scholar] [CrossRef]
- Jones, C.R.; Jahanshahi, M. Motor and Perceptual Timing in Parkinson’s Disease. In Neurobiology of Interval Timing; Springer: New York, NY, USA, 2014; pp. 265–290. [Google Scholar]
- Rohenkohl, G.; Coull, J.T.; Nobre, A.C. Behavioural dissociation between exogenous and endogenous temporal orienting of attention. PLoS ONE 2011, 6, e14620. [Google Scholar] [CrossRef] [Green Version]
- Bangert, A.S.; Balota, D.A. Keep up the pace: Declines in simple repetitive timing differentiate healthy aging from the earliest stages of Alzheimer’s disease. J. Int. Neuropsychol. Soc. JINS 2012, 18, 1052. [Google Scholar] [CrossRef] [Green Version]
- McAuley, J.D.; Jones, M.R.; Holub, S.; Johnston, H.M.; Miller, N.S. The time of our lives: Life span development of timing and event tracking. J. Exp. Psychol. Gen. 2006, 135, 348. [Google Scholar] [CrossRef]
- McAuley, J.D.; Henry, M.J.; Tkach, J. Tempo mediates the involvement of motor areas in beat perception. Ann. N. Y. Acad. Sci. 2012, 1252, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Loehrer, P.A.; Nettersheim, F.S.; Jung, F.; Weber, I.; Huber, C.; Dembek, T.A.; Pelzer, E.A.; Fink, G.R.; Tittgemeyer, M.; Timmermann, L. Ageing changes effective connectivity of motor networks during bimanual finger coordination. NeuroImage 2016, 143, 325–342. [Google Scholar] [CrossRef]
- Thaut, M.H.; Abiru, M. Rhythmic auditory stimulation in rehabilitation of movement disorders: A review of current research. Music Percept. 2010, 27, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Trapp, S.; Lepsien, J.; Sehm, B.; Villringer, A.; Ragert, P. Changes of hand switching costs during bimanual sequential learning. PLoS ONE 2012, 7, e45857. [Google Scholar] [CrossRef] [PubMed]
- Serrien, D.J.; Swinnen, S.P.; Stelmach, G.E. Age-related deterioration of coordinated interlimb behavior. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2000, 55, P295–P303. [Google Scholar] [CrossRef] [Green Version]
- Shetty, A.K.; Vinutha Shankar, M.; Annamalai, N. Bimanual coordination: Influence of age and gender. J. Clin. Diagn. Res. JCDR 2014, 8, 15. [Google Scholar] [CrossRef]
- Morillon, B.; Hackett, T.A.; Kajikawa, Y.; Schroeder, C.E. Predictive motor control of sensory dynamics in auditory active sensing. Curr. Opin. Neurobiol. 2015, 31, 230–238. [Google Scholar] [CrossRef] [Green Version]
- Alonso, C.C.; de Freitas, P.B.; Pires, R.S.; de Oliveira, D.L.; Freitas, S.M.F. Accuracy, sensitivity and specificity of different tests to detect impaired hand function in Parkinsons disease. medRxiv 2020. [Google Scholar] [CrossRef]
- Galvan, A.; Devergnas, A.; Wichmann, T. Alterations in neuronal activity in basal ganglia-thalamocortical circuits in the parkinsonian state. Front. Neuroanat. 2015, 9, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, D.J. Automaticity of walking: Functional significance, mechanisms, measurement and rehabilitation strategies. Front. Hum. Neurosci. 2015, 9, 246. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Tapping Task | Cueing | Condition of Cueing | |
|---|---|---|---|
| Without rhythmic cueing | Tapping to own pace | No | - |
| With rhythmic cueing | Tapping to follow regular rhythmic cueing | Yes | Providing regular rhythmic cueing for 15 s |
| Shifting tapping to match slow and fast tempo | Yes | Changing tempo of regular rhythmic cueing after 15 s | |
| Sustained tapping to regular intervals with cueing removed | Y→N | Removing regular rhythmic cueing after 15 s | |
| Stage Intervention Task | Regular Cueing | Interrupted Cueing | Content | |
|---|---|---|---|---|
| 1 | Drum playing with regular rhythmic cueing | Y | N | Tracking rhythmic cueing of regular interval of metronome beats |
| 2 | Drum playing with alternating tempo | Y | N | Tracking rhythmic cueing according to changes in tempo of 45 and 105 BPM |
| 3 | Drum playing with regular rhythm and unexpected stimulus interruption | Y | Y | Sustained regular interval of rhythmic cueing with unpredicted melodic cueing |
| 4 | Task shifting between initiation and stop with rhythmic cueing of different rhythmic patterns | Y | Y | During tracking of rhythmic cueing for regular tempo, participants shift tasks from initiating to stopping when provided with cueing of different rhythmic patterns |
| 5 | Task shifting between playing and singing with different rhythmic patterns | Y | Y | During tracking of rhythmic cueing for regular tempo, participants shift tasks between playing and singing when provided with different rhythmic patterns |
| Characteristic | DPRC M ± SD | Control M ± SD | Z | p |
|---|---|---|---|---|
| Age (years) | 61.6 ± 4.9 | 63.1 ± 10.1 | −0.434 | 0.673 |
| Duration of disease (years) | 5.6 ± 3.1 | 4.8 ± 1.4 | 1.000 | 0.363 |
| Education (years) | 12.3 ± 1.2 | 12.3 ± 3.1 | −0.416 | 0.686 |
| H&Y scale | 2.3 ± 0.8 | 1.6 ± 0.5 | 0.455 | 0.660 |
| MMSE-K score | 28.3 ± 1.2 | 26.3 ± 1.9 | 1.570 | 0.132 |
| Parameter | DPRC Group (n = 6) | Control Group (n = 6) | ||||
|---|---|---|---|---|---|---|
| Pre M ± SD | Post M ± SD | Pre M ± SD | Post M ± SD | Effects Size | ||
| Motor control measures | ||||||
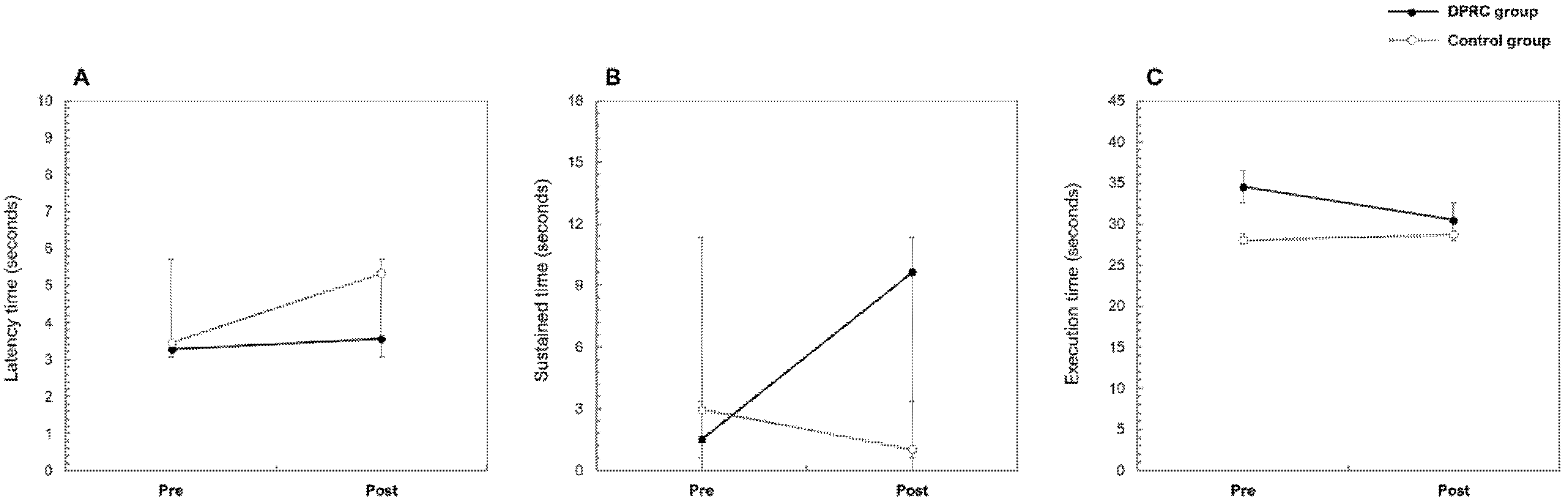
| Latency time until regularly self-paced tapping | Self-paced | 0.84 ± 0.37 | 0.55 ± 0.23 | 0.71 ± 0.52 | 0.96 ± 0.2 | 0.94 |
| Latency time until entrainment | 45 BPM | 4.05 ± 3.04 | 4.41 ± 2.78 | 3.87 ± 2.9 | 8.49 ± 4.31 | 0.53 |
| 105 BPM | 3.27 ± 0.65 | 3.56 ± 1.25 | 3.46 ± 3.14 | 5.33 ± 3.88 | 1.46 | |
| Latency time until entrainment for changes in tempo | 45→105 BPM | 4.01 ± 4.59 | 1.93 ± 0.4 | 4.75 ± 4.31 | 5.64 ± 4.32 | 0.84 |
| 105→45 BPM | 4.91 ± 2.78 | 3.59 ± 2.87 | 4.49 ± 1.03 | 7.03 ± 3.75 | 0.39 | |
| Sustained time of entrainment | 45 BPM | 1.52 ± 2.19 | 9.65 ± 5.56 | 2.96 ± 3.92 | 1.03 ± 1.73 | 0.9 |
| 105 BPM | 2.55 ± 1.3 | 7.12 ± 5.23 | 2.17 ± 1.18 | 3.11 ± 2.45 | 0.68 | |
| Execution time of NHPT | Right | 28.78 ± 6.14 | 27.64 ± 6.39 | 29.42 ± 5.45 | 39.60 ± 8.68 | 0.03 |
| Left | 34.51 ± 11.99 | 30.47 ± 8.84 | 28.00 ± 4.58 | 28.69 ± 1.71 | 0.87 | |
| Cognitive measures | ||||||
| K-TMT-e_A | 19.16 ± 5.41 | 19.18 ± 4.92 | 21.12 ± 5.07 | 21.94 ± 5.65 | 0.16 | |
| K-TMT-e_B | 42.67 ± 18.06 | 33.68 ± 13.40 | 41.06 ± 15.79 | 33.43 ± 8.56 | 0.07 | |
| KST_WR_Time | 65.55 ± 8.46 | 65.88 ± 15.71 | 63.51 ± 10.46 | 65.27 ± 10.58 | 0.14 | |
| KST_CR_Time | 121.69 ± 34.13 | 109.73 ± 26.86 | 119.08 ± 21.38 | 129.70 ± 27.25 | 1.04 | |
| Parameter | Repeated Measures Results | |||
|---|---|---|---|---|
| Time Effect | Group Effect | Time * Group | ||
| (t, p) | (t, p) | (t, p) | ||
| Motor control measures | ||||
| Latency time until regularly self-paced tapping | Self-paced | 0.011, 0.917 | 0.764, 0.403 | 2.704, 0.131 |
| Latency time until the entrainment | 45 BPM | 2.686, 0.132 | 0.178, 0.682 | 0.873, 0.372 |
| 105 BPM | 6.231, 0.032 ** | 5.407, 0.042 ** | 6.469, 0.029 ** | |
| Latency time until the entrainment in changes tempo | 45→105 BPM | 1.214, 0.296 | 0.939, 0.355 | 0.477, 0.505 |
| 105→45 BPM | 1.094, 0.320 | 0.990, 0.343 | 2.124, 0.176 | |
| Sustained time of entrainment | 45 BPM | 8.926, 0.014 ** | 0.017, 0.900 | 2.448, 0.149 |
| 105 BPM | 3.130, 0.107 | 0.031, 0.864 | 1.414, 0.262 | |
| Execution time of NHPT | Right | 0.284, 0.606 | 0.035, 0.856 | 0.004, 0.954 |
| Left | 10.994, 0.008 *** | 0.110, 0.747 | 2.327, 0.158 | |
| Cognitive measures | ||||
| K-TMT-e_A | 0.083, 0.779 | 0.616, 0.451 | 0.078, 0.786 | |
| K-TMT-e_B | 2.302, 0.160 | 0.016, 0.901 | 0.015, 0.903 | |
| KST_WR_Time | 0.132, 0.724 | 0.038, 0.849 | 0.062, 0.808 | |
| KST_CR_Time | 0.011, 0.917 | 0.279, 0.609 | 3.295, 0.100 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.-K.; Kim, S.J. Dual-Task-Based Drum Playing with Rhythmic Cueing on Motor and Attention Control in Patients with Parkinson’s Disease: A Preliminary Randomized Study. Int. J. Environ. Res. Public Health 2021, 18, 10095. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910095
Park J-K, Kim SJ. Dual-Task-Based Drum Playing with Rhythmic Cueing on Motor and Attention Control in Patients with Parkinson’s Disease: A Preliminary Randomized Study. International Journal of Environmental Research and Public Health. 2021; 18(19):10095. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910095
Chicago/Turabian StylePark, Jin-Kyoung, and Soo Ji Kim. 2021. "Dual-Task-Based Drum Playing with Rhythmic Cueing on Motor and Attention Control in Patients with Parkinson’s Disease: A Preliminary Randomized Study" International Journal of Environmental Research and Public Health 18, no. 19: 10095. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910095